AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Chadia Haddad, Diana Malaeb, Hala Sacre, Sandrella Bou Malhab, Dalia Khachman. Psychiatric Hospital of the Cross, P.O. Box 60096, Jall-Eddib, Lebanon.
Citation: Chadia Haddad, Diana Malaeb, Hala Sacre, Sandrella Bou Malhab, Dalia Khachman (2023), Psychological Distress Among Lebanese Women During the COVID-19 Confinement: Any Mediating Effect of Violence. Single Center Study., J. Obstetrics Gynecology and Reproductive Sciences, 7(1) DOI:10.31579/2578-8965/150
Copyright: © 2023, Chadia Haddad. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 January 2023 | Accepted: 10 February 2023 | Published: 27 February 2023
Keywords: violence; women; anxiety; stress; depression; psychological distress
Background: Violence among women is associated with poor psychological health and increased internalizing symptoms, such as depression, stress, and anxiety. The primary objective was to evaluate the association of marital conflict, pregnancy status, socioeconomic status, and stressful life events with violence, depression, anxiety, and stress. The secondary objective was to evaluate the mediating effect of violence on psychological distress.
Methods: A cross-sectional study was conducted among 369 women between June 8 and August 1, 2020. The questionnaire was developed on Google Forms and distributed online, using the snowball technique.
Results: higher marital conflicts (Beta=0.199), financial difficulties (Beta=2.046), an abuse by a family member (Beta=2.292) and a history of child abuse (Beta=2.209) were significantly associated with higher depression scores. Higher marital conflicts (Beta=0.367) and financial difficulties (Beta=4.001) were significantly associated with higher anxiety scores. Higher marital conflicts (Beta=0.074) and financial difficulties (Beta=1.422) were significantly associated with higher perceived stress scores. Composite abuse scale partially mediated the association between pregnancy status, financial difficulties, history of child abuse by a family member and anxiety and depression. No mediation effect of the CASR-SF was found between the independent variables and perceived stress.
Conclusion: Our main findings suggest that violence mediated the association between pregnancy status, marital conflicts, financial difficulties, and depression and anxiety but did not mediate between these factors and stress. Further studies are needed to understand better the factors that mediate the relations between domestic violence and mental well-being among Lebanese women.
Depression, anxiety, and stress are now the leading mental health disorders causing disability, and having a high burden on the health care budget (Organization, 2003; Organization et al., 2004). Severe mental health problems are associated with emotional, cognitive, and social abilities that can lead to the vast majority of detrimental consequences (McLachlan et al., 2013; Slade et al., 2009). Depression is much more common in women than in men due to biological, environmental, and social factors (Kazi et al., 2006; Fu and Parahoo, 2009; Patel et al., 2008). Previous literature supported that other risk factors increased the propensity of depression among married women, such as marital conflicts, lack of social support, and marital dissatisfaction (Lorant et al., 2007; Berenson et al., 2003; Zuraida Zainal, 2008). In addition to the influence of the social environment, other potential risk factors also increased the risk of depression, including a low level of education and financial difficulties (Ting and Leong, 2014; Cheah et al., 2020). Women of low socioeconomic status continually fear that they will not be able to meet their daily needs and worry about the future, which limits their recreational activities (Watson et al., 2012). Hence, poverty, combined with a lack of social support, induce a higher risk of anxiety and depressive disorders in women. Married women with low income are more likely to encounter financial difficulties, relationship problems, unstable health, and unemployment, which can contribute to the onset of depression (Ali et al., 2010). A poor relationship with the partner causes intimate partner violence and stress in the marital life. Also, husbands who are busy with their professions or having extramarital affairs increase the risk for depression in women (Nisar et al., 2004; Chowdhary and Patel, 2008; Niaz, 2004; Fu and Parahoo, 2009). On the other hand, enhanced marital satisfaction has been associated with a lower propensity to develop depressive symptoms (Manaf et al., 2016). Married women undergoing domestic violence, work stress, traumatic experiences, and abused conditions had a higher risk of depression (Ferrari et al., 2016). Stress, another mental health disorder, is a highly prevalent condition in women, particularly during pregnancy (Shishehgar et al., 2014). Pregnant women are highly prone to stress due to the feeling of imbalance when they cannot cope with demands and worries (Ruiz and Fullerton, 1999). Other influential factors of increased risk of stress among women include low socioeconomic status, exposure to violence, stressful life events, lack of social support, and conflicts (McCormick et al., 1990; Lu and Chen, 2004; Marquis and Butler, 2001). Previous literature supports the fact that violence among women is related to several factors, including low socioeconomic level, previous violence in the family, pregnancy status, and social isolation (Ceballo et al., 2004). Furthermore, women exposed to violence had poor psychological health and increased internalizing symptoms, such as depression, stress, and anxiety (Fridh et al., 2014; Evans et al., 2008). Previous studies reported various mediating factors for violence. However, only a few examined the mediating effect of violence on psychological distress in women (Adams et al., 2012; Lelaurain et al., 2018). Our research uses a conceptual model based on a study done by Ceballo et al. (Figure 1) (Ceballo et al., 2004).
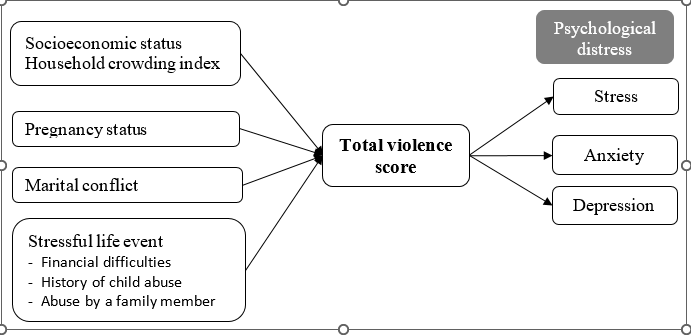
Figure 1. Conceptual model of risk factors associated with violence and the psychological effects among women
However, relatively little is known about how an epidemic outbreak impacts emotional well-being and even less is known about the factors that may worsen or protect emotional well-being during an outbreak (Lu et al., 2020; Zhang et al., 2020). It has been highlighted that during COVID-19 pandemic, disruptions of daily routines for individuals and families, compounded by the anxiety of the pandemic, lack of physical activity, absence of outside social outlets, lack of access to non-essential clinical care, and reduced physical contact may all contribute to increase in depression, anxiety, and other negative mental health outcomes among females (Luetke et al., 2020; Rosenberg et al., 2020; Lu et al., 2020). Furthermore, current unemployment, especially amongst those who are daily wage workers, increased responsibilities because of children being at home due to school closures and increased stress in the family, may make women more vulnerable for depression and anxiety (Joseph et al., 2020). Thus, identifying these factors is critically important, as they inform policies and interventions aimed at protecting people's psychological well-being in the age of pandemics. In Lebanon, there are no studies that evaluated the magnitude of depression, anxiety, and stress among Lebanese women in COVID-19. Therefore, our primary objective was to assess the association of marital conflict, pregnancy status, socioeconomic status, and stressful life events with violence, depression, anxiety, and stress. Our secondary objective was to evaluate the mediating effect of violence on psychological distress.
Study design and sampling: A cross-sectional online study conducted between June 8 and August 1, 2020, enrolled a total of 369 women. The questionnaire used was developed on Google Forms and distributed on social media and WhatsApp groups, using the snowball technique; it required 40 minutes to complete. Eligibility criteria were the following: married women aged between 18 and 51, currently living with their partner, and with internet access. Single, widowed, or divorced women, and those with a fertility problem, were excluded. The inclusion criteria were stated in the consent form at the beginning of the survey. Participation in this study was anonymous and voluntary, and participants received no compensation in return.
Sample size calculation:
The Epi info software (Centers for Disease Control and Prevention, Epi Info™) calculated a minimum sample of 233 participants, a prevalence of 10.9% women with depression, according to a previous study (El Asmar et al., 2014), a confidence level of 95%, and adding a 4% margin of error. A sample of 500 women was targeted to allow for missing values. The final sample size consisted of 369 participants.
Translation procedure:
A forward and backward translation was conducted for all the items of the questionnaire. One translator did the translation from English into Arabic, and a second one performed the back translation. Discrepancies between the two English versions were resolved by consensus.
Questionnaire:
The online questionnaire consisted of two sections, including closed-ended questions available in English and Arabic. The first one assessed the sociodemographic details of participants (age, educational level, the region of residence, religion, working status, monthly income, smoking and alcohol status, and physical activity). The monthly income was divided into four levels: no income, low less than 1,000USD intermediate1,000-2,000 USD, and high income greater than 2,000 USD.
The second section consisted of the following measures:
Household crowding index: The household crowding index was calculated by dividing the number of persons living in the household by the number of rooms, excluding bathrooms and kitchen, to assess socioeconomic status (Melki et al., 2004).
Stressful life events: Negative life events were assessed using three dichotomous questions (Yes/No) about financial difficulties, history of child abuse, and history of family member abuse.
Marital conflict: The Relationship Dynamics Scale was utilized to measure the frequency of conflicts in relationships (Forthofer et al., 1996). The scale consists of eight items scored on a 5-point Likert scale, (1 = Never or almost never to 5 = Always) (Forthofer et al., 1996). A higher score indicates a higher conflict between partners. In this study, Cronbach’s alpha value was 0.915.
Pregnancy status: The current pregnancy status was assessed using binary questions (Yes/No). The current pregnancy status reflects the ability of women to choose to reproduce or be coerced into an unwanted pregnancy.
Partner violence: Violence was assessed using the Composite Abuse Scale (Revised) – Short Form (CASR-SF). This 15-item scale evaluates the existence, extent, and severity of physical, sexual, or psychological abuse (Ford-Gilboe et al., 2016). The total score is calculated by summing the 15 responses. Items are graded on a Likert scale from 1 to 6, where a higher score indicates a higher intensity/occurrence of abuse. The total score was dichotomized as follows: presence of violence (scores of 1 or more) vs no violence (scores of 0). The author of the questionnaire, Professor Marilyn Ford-Gilboe, granted permission to use the scale. Cronbach’s alpha value was 0.902 for the full scale.
Psychological distress: Stress, anxiety, and depression were measured using three scales, reflecting psychological distress among women. The Perceived Stress Scale-4 (PSS-4) evaluated the occurrence and intensity of stress. It consists of four questions graded on a Likert scale from 1 to 5. The total score was calculated by summing the four items, ranging from 0 to 16, with higher scores indicating a higher intensity/occurrence of perceived stress (Cohen et al., 1983). In this study, Cronbach’s alpha value was 0.484. The Lebanese anxiety scale (LAS; developed and validated in Lebanon) is a 10-item tool graded on a Likert scale from 1 to 5. It assessed the occurrence and intensity of anxiety. The total score was obtained by summing all the responses, with higher scores indicating higher anxiety (Hallit et al., 2020). In this study, Cronbach’s alpha value was 0.890. The PHQ-9, validated in Lebanon (Sawaya et al., 2016), assesses the level of depression. It consists of 9 items graded on a Likert scale from 1 to 4. The PHQ-9 score can range from 0 to 27, with higher scores indicating a more severe depression (Kroenke and Spitzer, 2002). In this study, Cronbach’s alpha value was 0.893.
Data were analyzed on SPSS software version 25 (SPSS Inc., Chicago, IL, USA). A descriptive analysis was performed, using the absolute frequency and percentages for categorical variables and mean and standard deviation for quantitative measures. Student t-test and ANOVA F tests were used to assess the association of continuous variables with two or more levels, and Pearson correlation was used for linear correlation between continuous variables. In the multivariable analysis, four linear regressions were performed, taking stress, anxiety, depression, and violence as the dependent variables, meeting all the assumptions for normality and homoscedasticity. Regressions took into account the variables of interest selected based on the conceptual mode: household crowding index, marital conflict, pregnancy status, history of child abuse, history of family member abuse and financial difficulties and total violence score. Also, a multivariate General Linear Model was conducted, comparing mental health variables between presence and absence of violence among women, after adjusting for the following variables: woman’s age, pregnancy status, marital conflict, financial difficulties, abuse by a family member, history of child abuse and household crowding index.
The PROCESS SPSS Macro version 3.4 model four was used to evaluate the mediation of violence using the CASR-SF through three steps. Step 1 determined the regression coefficient for the effect of marital conflict, household crowding index, pregnancy status, financial difficulties, history of child abuse, and abuse by a family member. Step 2 examined the association between violence and psychological distress (stress, anxiety, and depression), and Step 3 estimated the direct effect of each of the marital conflict, household crowding index, pregnancy status, financial difficulties, history of child abuse, and abuse by a family member on psychological distress. Each independent variable was entered in a separate model since the variables were not highly correlated. The macro generated bias-corrected bootstrapped 95% confidence intervals (CI) to test the significance of the indirect effect (Yzerbyt et al., 2018; MacKinnon et al., 2007). Mediation was considered significant when the CI around the indirect effect did not include zero (MacKinnon et al., 2007). The mediation effect was calculated by dividing the indirect effect of X by the direct effect of Y. The covariates included in the mediation model were those that showed significant associations with psychological distress in the bivariate analysis. Statistical significance was set at a value of P less than0.005.
Sample description
TThe mean age of women was 32.5 ± 6.4 years. The majority (83.9%) had a university level of education, 59.9% were employed, 23.3% had no income, and 42.5% practiced physical activities. Only 31.2% of them were smokers, and 10.8% consumed alcohol. The mean duration of confinement was 71.0 ± 42.8 days, and the mean fear of poverty was 5.8 ± 3.2 (Table 1).
| Table 1: Sociodemographic and other characteristics of the studied sample (N=369) | |
| Frequency (%) | |
| Education level | |
| Primary | 3 (0.8%) |
| Complementary | 11 (3.0%) |
| Secondary | 32 (8.7%) |
| University | 323 (87.5%) |
| Religion | |
| Christian | 115 (31.2%) |
| Muslim | 155 (42.0%) |
| Druze | 81 (22.0%) |
| Atheist | 2 (0.5%) |
| Refused to answer | 16 (4.3%) |
| Working status | |
| Employed | 221 (59.9%) |
| Unemployed | 148 (40.1%) |
| Monthly income | |
| No income | 102 (27.6%) |
| Low | 94 (25.5%) |
| Intermediate | 112 (30.4%) |
| High | 61 (16.5%) |
| Smoking status | |
| Non smoker | 254 (68.8%) |
| Smoker | 115 (31.2%) |
| Alcohol consumption | |
| Yes | 40 (10.8%) |
| No | 329 (89.2%) |
| Physical activity | |
| Yes | 157 (42.5%) |
| No | 212 (57.5%) |
| Mean ± SD | |
| Age in years | 32.5 ± 6.4 |
| Duration of confinement (days) | 71.0 ± 42.8 |
| Fear of poverty | 5.8 ± 3.2 |
Bivariate analysis: correlates of psychological scales: A significantly higher mean violence score was found in non-pregnant as compared to pregnant women, those with a history of family member abuse or a history of child abuse. A significantly higher mean depression score was found in non-employed as compared to employed women, those with financial difficulties, history of child abuse, or history of family member abuse. A significantly higher mean anxiety score was found in non-pregnant as compared to pregnant women, those unemployed, with financial difficulties, history of child abuse, or abuse by a family member. A significantly higher mean stress score was found in those with financial difficulties (Table 2).
| Table 2: Bivariate analysis taking the psychological scales as the dependent variables | ||||
| Total violence score | Depression score | Anxiety score | Stress score | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Pregnancy status | ||||
| Yes | 0.39 ± 1.20 | 6.07 ± 6.03 | 12.12 ± 6.47 | 6.83±2.41 |
| No | 2.18 ± 6.14 | 7.15 ± 5.36 | 14.73 ± 7.45 | 7.42±2.65 |
| P-value | 0.025 | 0.050 | 0.034 | 0.233 |
| Financial difficulties | ||||
| Yes | 2.91±7.53 | 8.74±5.75 | 17.22±7.54 | 8.20±2.42 |
| No | 1.23±3.84 | 5.66±4.76 | 12.22±6.46 | 6.68±2.58 |
| P-value | 0.311 | <0> | <0> | <0> |
| Working status | ||||
| Yes | 1.45±4.44 | 6.41±4.91 | 13.39±6.59 | 7.20±2.53 |
| No | 2.76±7.39 | 7.95±6.05 | 16.01±8.21 | 7.58±2.75 |
| P-value | 0.320 | 0.031 | 0.004 | 0.292 |
| Monthly income | ||||
| No income | 2.04±5.19 | 7.53±5.69 | 16.58±8.06 | 7.73±2.45 |
| Low | 2.28±6.13 | 7.49±5.30 | 14.17±6.58 | 7.29±2.52 |
| Intermediate | 1.33±4.13 | 6.28±4.92 | 13.06±6.78 | 6.94±2.76 |
| High | 2.61±8.50 | 6.87±6.07 | 13.84±7.82 | 7.61±2.75 |
| P-value | 0.885 | 0.171 | 0.007 | 0.261 |
| History of child abuse | ||||
| Yes | 4.89±7.51 | 10.74±6.09 | 17.95±7.04 | 7.54±2.51 |
| No | 1.45±5.32 | 6.35±5.04 | 13.80±7.27 | 7.32±2.65 |
| P-value | <0> | <0> | <0> | 0.480 |
| History of family member abuse | ||||
| Yes | 8.15±11.74 | 12.54±6.81 | 19.19±8.61 | 7.85±2.69 |
| No | 1.51±4.84 | 6.61±5.10 | 14.08±7.17 | 7.32±2.62 |
| P-value | <0> | <0> | 0.003 | 0.331 |
The correlation analysis showed that older age, longer duration of marriage, higher marital conflict, stress, depression, and anxiety were significantly associated with higher violence. Additionally, higher marital conflict, higher stress, anxiety, and violence were significantly associated with higher depression. Moreover, higher marital conflict, stress, depression, and violence were significantly associated with higher anxiety. Also, higher marital conflict, depression, anxiety and violence were significantly associated with higher stress (Table 3).
| Table 3: Pearson correlation between quantitative variables and the psychological scales | ||||
| Total violence score | Depression score | Anxiety score | Stress score | |
| Correlation coefficient | Correlation coefficient | Correlation coefficient | Correlation coefficient | |
| Age | 0.149 | -0.066 | -0.038 | -0.037 |
| P-value | 0.004 | 0.209 | 0.466 | 0.473 |
| Household crowding index | -0.063 | 0.014 | 0.018 | 0.030 |
| P-value | 0.231 | 0.791 | 0.733 | 0.560 |
| Marital conflict | 0.510 | 0.353 | 0.338 | 0.211 |
| P-value | <0> | <0> | <0> | <0> |
| Duration of marriage | 0.127 | -0.068 | -0.046 | -0.017 |
| P-value | 0.014 | 0.192 | 0.380 | 0.741 |
| Duration of confinement (days) | -0.064 | 0.033 | -0.008 | -0.009 |
| P-value | 0.217 | 0.526 | 0.877 | 0.860 |
| Number of pregnancies | 0.074 | -0.051 | -0.023 | -0.011 |
| P-value | 0.158 | 0.332 | 0.666 | 0.831 |
| Number of children | 0.080 | 0.002 | 0.027 | 0.036 |
| P-value | 0.163 | 0.978 | 0.637 | 0.529 |
| Stress | 0.123 | 0.447 | 0.503 | - |
| P-value | 0.018 | <0> | <0> | |
| Depression | 0.259 | - | 0.785 | 0.447 |
| P-value | <0> | <0> | <0> | |
| Anxiety | 0.141 | 0.785 | - | 0.503 |
| P-value | 0.007 | <0> | <0> | |
| Total violence score | - | 0.259 | 0.141 | 0.123 |
| P-value | <0> | <0> | 0.018 | |
| *Values marked in bold are significant | ||||
Multivariable analysis: The first linear regression taking the violence score as the dependent variable showed that higher marital conflicts (Beta= 0.500) and higher household crowding index (Beta=3.598) were significantly associated with a higher violence score (Table 4, Model 1).
A second linear regression taking the depression score as the dependent variable showed that higher marital conflicts (Beta=0.199), financial difficulties (Beta=2.046), an abuse by a family member (Beta=2.292) and a history of child abuse (Beta=2.209) were significantly associated with a higher depression score (Table 4, Model 2).
A third linear regression taking the anxiety score as the dependent variable showed that higher marital conflicts (Beta=0.367) and financial difficulties (Beta=4.001) were significantly associated with higher anxiety scores (Table 4, Model 3).
A fourth linear regression taking the stress score as the dependent variable showed that higher marital conflicts (Beta=0.074) and financial difficulties (Beta=1.422) were significantly associated with higher perceived stress scores (Table 4, Model 4).
| Table 4: Multivariable analysis | |||||
| Model 1: Linear regression model taking the total violence score as the dependent variable | |||||
| Variable | Unstandardized Beta | Standardized Beta | P | 95% Confidence Interval | |
| Pregnancy status | -.206 | -.011 | .796 | -1.773 | 1.361 |
| Marital conflict | .500 | .526 | <.001 | .416 | .583 |
| Financial difficulties | .307 | .026 | .548 | -.697 | 1.311 |
| Abuse by a family member | .352 | .022 | .649 | -1.166 | 1.870 |
| History of child abuse | -.973 | -.075 | .081 | -2.068 | .122 |
| Household crowding index | 3.598 | .158 | .001 | 1.463 | 5.734 |
| Duration of confinement (days) | .352 | .022 | .649 | -1.166 | 1.870 |
| Model 2: Linear regression model taking the depression scale as the dependent variable and the total violence score as the independent variable | |||||
| Variable | Unstandardized Beta | Standardized Beta | P | 95% Confidence Interval | |
| Pregnancy status | -.025 | -.001 | .976 | -1.631 | 1.582 |
| Marital conflict | .199 | .224 | <.001 | .098 | .299 |
| Financial difficulties | 2.046 | .187 | <.001 | 1.017 | 3.076 |
| Abuse by a family member | 2.292 | .108 | .043 | .070 | 4.514 |
| History of child abuse | 2.209 | .147 | .006 | .652 | 3.765 |
| Household crowding index | .083 | .007 | .885 | -1.044 | 1.211 |
| Duration of confinement (days) | .002 | .016 | .730 | -.010 | .014 |
| Total violence score | 0.072 | 0.077 | 0.186 | -0.035 | 0.178 |
| Model 3: Linear regression model taking the anxiety scale as the dependent variable and the total violence score as the independent variable | |||||
| Variable | Unstandardized Beta | Standardized Beta | P | 95% Confidence Interval | |
| Pregnancy status | -1.188 | -.051 | .284 | -3.363 | .988 |
| Marital conflict | .367 | .305 | <.001 | .230 | .503 |
| Financial difficulties | 4.001 | .269 | <.001 | 2.606 | 5.395 |
| Abuse by a family member | .798 | .028 | .602 | -2.211 | 3.807 |
| History of child abuse | 1.653 | .081 | .124 | -.455 | 3.761 |
| Household crowding index | .574 | .035 | .460 | -.952 | 2.101 |
| Duration of confinement (days) | -.006 | -.033 | .483 | -.022 | .010 |
| Total violence score | -.014 | -.011 | .850 | -.158 | .130 |
| Model 4: Linear regression model taking the stress scale as the dependent variable and the total violencescore as the independent variable | |||||
| Variable | Unstandardized Beta | Standardized Beta | P | 95% Confidence Interval | |
| Pregnancy status | -.427 | -.051 | .313 | -1.258 | .404 |
| Marital conflict | .074 | .173 | .006 | .022 | .126 |
| Financial difficulties | 1.422 | .270 | <.001 | .889 | 1.954 |
| Abuse by a family member | -.095 | -.009 | .871 | -1.244 | 1.054 |
| History of child abuse | -.333 | -.046 | .416 | -1.138 | .472 |
| Household crowding index | -.028 | -.005 | .925 | -.611 | .555 |
| Duration of confinement (days) | -.002 | -.025 | .626 | -.008 | .005 |
| Total violence score | -.013 | -.029 | .645 | -.068 | .042 |
| Variables entered in all models: Pregnancy status, marital conflict, financial difficulties, abuse by a family member, history of child abuse, household crowding index, duration of confinement and total violence score | |||||
| Note: Values marked in bold are significant | |||||
Figure 2: displays the association of psychological variables with violence among women, adjusted for woman’s age, pregnancy status, marital conflict, financial difficulties, abuse by a family member, history of child abuse and household crowding index. The results showed no association between women being exposed or not to violence and psychological distress (p> 0.05 for all).
|
|
Figure 2. Adjusted means of psychological variables according to the presence/absence of violence
LAS=Lebanese Anxiety Scale; PHQ=Patient Health Questionnaire for depression measurement; PSS-4=Perceived Stress Scale
Mediation analysis: Table 5 presents the mediation analysis conducted anxiety and depression. The CASR-SF partially mediated the association between pregnancy status, financial difficulties, history of child abuse abuse by a family member and anxiety and depression. No mediation effect of the CASR-SF was found between the independent variables and perceived stress.
| Table 5. Mediation analyses | |||||||
| Model 1: Taking the anxiety scale as a dependent variable and the composite abuse scale as a mediation factor | |||||||
| Independent variables | Direct effect | Indirect effect | Mediating effect of composite abuse scale | ||||
| Beta | SE | p | Beta | Boot SE | Boot CI | ||
| Household crowding index | 1.37 | 0.82 | 0.09 | -0.18 | 0.16 | -0.52; 0.11 | - |
| marital conflict | 0.43 | 0.06 | <0> | 0.009 | 0.04 | -0.08; 0.09 | - |
| pregnancy status | -2.31 | 1.17 | 0.04 | -0.49 | 0.17 | -0.87; -0.18* | 21.21% |
| history of child abuse | 3.01 | 1.03 | 0.003 | 0.80 | 0.30 | 0.22; 1.42* | 26.57% |
| history of family member abuse | 2.99 | 1.50 | 0.04 | 1.56 | 0.80 | 0.37; 3.49* | 52.17% |
| financial difficulties | 4.21 | 0.73 | <0> | 0.36 | 0.17 | 0.05; 0.73* | 8.55% |
| Model 2: Taking the depression scale as a dependent variable and the composite abuse scale as a mediation factor | |||||||
| Independent variables | Direct effect | Indirect effect | Mediating effect of composite abuse scale | ||||
| Beta | SE | p | Beta | Boot SE | Boot CI | ||
| Household crowding index | 0.35 | 0.60 | 0.55 | -0.15 | 0.14 | -0.46; 0.12 | - |
| marital conflict | 0.24 | 0.05 | <0> | 0.06 | 0.03 | -0.003; 0.12 | - |
| pregnancy status | -0.68 | 0.86 | 0.43 | -0.49 | 0.14 | -0.78; -0.23* | 72.05% |
| history of child abuse | 3.53 | 0.74 | <0> | 0.73 | 0.24 | 0.27; 1.22* | 20.67% |
| history of family member abuse | 4.34 | 1.08 | 0.001 | 1.35 | 0.56 | 0.41; 2.64* | 31.10% |
| financial difficulties | 2.59 | 0.54 | <0> | 0.35 | 0.14 | 0.05; 0.64* | 13.51% |
| * Indicates significant mediation. | |||||||
To our knowledge, this study is the first to assess the factors related to psychological distress among Lebanese women during the COVID-19 confinement. The results showed that marital conflicts and financial difficulties were associated with high stress, anxiety, and depression, while higher violence was related to higher depression among women. Also, violence was a mediating factor between pregnancy status and anxiety and between marital conflict and depression. In this study, marital conflicts were related to higher depression, anxiety, and stress among women. Consistently, previous findings have also associated high levels of psychological distress with marital dissatisfaction (Perrin, 2008; Trudel and Goldfarb, 2010; Choi and Marks, 2008; Goldfarb et al., 2007). A recent study conducted in China during the COVID-19 pandemic showed that emotional well-being in married people was lower than in unmarried people (Yang and Ma, 2020). Evidence suggests that stressful or life-threatening events, such as natural disasters, can lead to a decline in the quality of relationships due to stress and conflict or, instead, improve the quality of relationships and intimacy (Cohan and Cole, 2002; Fredman et al., 2010; Marshall and Kuijer, 2017). Also, during the COVID-19 confinement, several factors can lead to increased tension between romantic partners confined together, such as disturbed everyday activities, the fear of the pandemic, loss of physical activity, loss of outside social networks, lack of access to non-essential health services, and reduced physical interaction in overcrowded households (Luetke et al., 2020). Previous studies have shown that the persistence of tense verbal or non-verbal exchanges between partners can lead to physiological and psychological changes, eventually progressing to disease states (Robles and Kiecolt-Glaser, 2003; McEwen, 1998). Once health conditions develop or intensify, they can be experienced as a traumatic life occurrence or persistent stress, resulting in adverse mental health consequences, such as depression and anxiety (Williamson et al., 2000). Our results also showed that marital conflicts were associated with higher violence, consistent with those of previous studies (Park et al., 2017; Burlaka et al., 2017; Garrison and Curtis, 2019). The severity of marital conflicts ranges from minor disagreements to disputes that partners cannot overcome, which harms their relationship and could lead to violence (Fincham, 2003).
This study showed that violence was associated with higher depression among women, in agreement with previous studies showing that women subject to behavioral, physical, and sexual violence by an intimate partner were more likely to exhibit signs of depression (Pico-Alfonso et al., 2006; Beydoun et al., 2012; Devries et al., 2013). The core mechanisms that explain why violence can cause subsequent depression in women are traumatic and psychological stress reactions (Organization, 2013). Sustained psychological stress due to social threats or rejection can affect women’s cognition, mood, and behavior, leading to symptoms of depression (Slavich and Irwin, 2014). Also, domestic environments have become a suitable place for intimate partner abuse because of lockdown restrictions (Joseph et al., 2020). Abusive individuals may use the confinement to exert power over the vulnerable ones, especially women (Joseph et al., 2020). Lockdown restrictions can contribute to increased stress and further lead to exacerbation of anxiety, depressive symptoms, and violence (Telles et al., 2020). Thus, the perpetrator disturbed psychological health could adversely affect that of abused individuals (Telles et al., 2020). The persistent exposure of vulnerable persons to abusive individuals constrains the victim to cope with the situation, which further aggravates depressive symptoms (Mechanic et al., 2008). Our findings revealed that financial difficulties were associated with higher depression, stress, and anxiety, consistent with those of a recent study showing a correlation between financial hardship and emotional impact due to the pandemic (Skapinakis et al., 2020). Other studies have also reported that financial difficulties due to the lockdown might impair mental health and increase the incidence of psychological stress (Hamadani et al., 2020; Dsouza et al., 2020; Bhuiyan et al., 2020). During times of crisis and confinement, women face plenty of problems, including high risks of economic poverty. Also, they are over-represented in health services, continue to do most unpaid household care jobs, and face increased risks of violence, assault, or harassment (Home). Additionally, their employment, businesses incomes, and living conditions could be more vulnerable than men to the predicted systemic economic effects of the pandemic, placing them at greater risk of financial instability. All these issues have a considerable impact on the health and psychological well-being of women (Home). Psychological difficulties expected by financial pressures include higher psychological distress and intensified issues and relations with family members, friends, and in the workplace (Kahn and Pearlin, 2006).
Our results showed that a higher number of pregnancies and abuse by a family member were related to higher violence against women. Similarly, other studies found that a large family is a risk factor for frequent domestic violence, empowered by lower socioeconomic status, deprivation of maternal care, neglect of children, lack of family planning, and parenteral conflict (Guler, 2010; Malta et al., 2012; Das et al., 2013; Kouyoumdjian et al., 2013). Furthermore, a history of child abuse was related to higher depression among women, consistently with other findings (Ouellet‐Morin et al., 2015; Howard et al., 2013; Fonseca-Machado et al., 2014; SAHİN et al.). Hence, the loss of attachment and the absence of a secure life were the main features for women to experience depression (Kwako et al., 2010; Whiffen and MacIntosh, 2005). Moreover, women victims of childhood abuse are more likely to endure violence later in their life (Zeglin et al., 2015; Till-Tentschert, 2017; Antoniou and Iatrakis, 2019). Identifying women with a history of childhood abuse and assaults would provide efficient maternal care and increase awareness against domestic violence.
Our results showed that violence mediated the association between pregnancy status, marital conflicts, financial difficulties, and depression and anxiety but did not mediate between these factors and stress. Contrary to our findings, a recent study conducted in Lebanon during the COVID-19 lockdown among 502 adults found that female gender and physical violence at home were associated with higher stress during the pandemic (Salameh et al., 2020). It also showed that a previous higher socioeconomic status was associated with higher stress, while current financial wellness was correlated with lower stress (Salameh et al., 2020). However, a previous study among 215 mothers found that stressful life events were directly linked to psychological distress, particularly depression through domestic violence, while marital and pregnancy statuses were not related to the presence of domestic violence (Ceballo et al., 2004). Several other studies found that dissatisfied married women would present a high risk of mental distress (Brock and Lawrence, 2011; Røsand et al., 2014; Lorenz et al., 1993). The sudden disruption of routine due to the COVID-19 outbreak has affected the populations globally, leading to exacerbation of stress in the majority of people. However, the Lebanese people exhibited psychological resilience during the confinement, as they had faced and continue to endure political instabilities, a decline of essential services, in addition to several types of violence (International Crisis Group, 2015 ); they adapt to abuse and work through it more than they oppose it (International Crisis Group, 2015 ). Regarding gender equality in Lebanese society, women continue to face discrimination at numerous levels, such as decision-making structures, socio-cultural values, and security issues. Men are raised in a manner that gives them a sense of authority over women and makes them expect women to recognize their superiority. Thus, unhappy marriages, marital conflicts, and economic insecurity make women more vulnerable to mental problems (Goldfarb et al., 2007; Fincham, 2003; Howard et al., 2013). Future studies are necessary to determine the psychological distress faced by Lebanese married women, particularly during confinement.
This study has several limitations. Its findings could not be generalized to the entire Lebanese female population due to the small sample size. Also, its cross-sectional design makes it difficult to find causal relations. The study relies on self-report data, which may be biased by memory recall and social desirability effects. The fact that the data was collected online via a self-reported questionnaire may have resulted in an information bias. We utilized odd-numbered answer categories with a neutral choice to eliminate this sort of bias, allowing participants to opt-out and provide an indifferent response, resulting in a non-differential measurement error rather than a differential information bias. A selection bias is also likely because the sample was not randomly chosen but rather obtained using the snowball sampling method. Residual confounding bias is also possible since there could be variables linked to psychological distress that were not measured. The violence scale was not validated in Arabic among women prior to our investigation.
Our main findings suggest that violence mediated the association between pregnancy status, marital conflicts, financial difficulties, and depression and anxiety but did not mediate between these factors and stress. During the COVID-19 pandemic, reducing the effect of stress in relationships and attempting to solve existing conflicts are essential steps to assist partners and families to adapt to new and challenging conditions. Further studies are needed to understand better the factors that mediate the relations between domestic violence and mental well-being among Lebanese women.
COVID-19: Coronavirus disease of 2019, USD: United States dollar, CASR-SF: The Composite Abuse Scale Revised – Short Form, PSS-4: Perceived stress scale short version, LAS: Lebanese Anxiety Scale, PHQ-9: Patient Health Questionnaire, SPSS: Statistical Package for Social Sciences, CI: Confidence Interval, SD: Standard deviation.
Ethics approval and consent to participate
The Psychiatric Hospital of the Cross-ethics committee approved the study protocol (HPC-018-2020). Online Informed consent was obtained from each participant involved in this study on the first page of the questionnaire.
Consent for publication
Not applicable.
Availability of data and materials
Data can be made available under reasonable request form the corresponding author.
Competing interests
The authors have nothing to disclose.
Funding
None.
Authors’ contribution:
CH designed the study; CH, DM, SBM, JA drafted the manuscript; CH and PS carried out the analysis and interpreted the results; PS, HS, DK, NL, JA assisted in drafting and reviewing the manuscript; CH, DM, DK, NL, JA, and SBM were responsible for data collection; HS edited the paper for English language, PS supervised the course of the article. All authors reviewed and approved the final version of the manuscript.
Acknowledgements:
The authors would like to thank all those who participated in this study, and Mrs. Mireille Awad Zeinoun for the research idea and for helping in data collection. Also, special thanks go to the Order of Midwives in Lebanon who helped in the data collection by filling up and spreading the web-based online survey.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

