AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester, M8 5RB. United Kingdom.
Citation: Anthony Kodzo-Grey Venyo. (2021) Prostatic Abscess: A Review and Update. Archives of Medical Case Reports and Case Study, 4(6); DOI:10.31579/2692-9392/090
Copyright: © 2021 Anthony Kodzo-Grey Venyo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 October 2021 | Accepted: 29 October 2021 | Published: 08 November 2021
Keywords: prostate abscess; aspiration, drainage; trans-urethral resection of prostate; insertion of prostatic drain
Prostate abscess (PA) is a complication that ensues an acute infectious purulent process within the prostate gland which is typified by accumulation of purulent material within the prostate gland and this purulent material could be unilocular or multi-septated within the prostate gland. PA is a rare disease especially in the developed world where PA tends to be more commonly associated with patients who have diabetes mellitus, chronic kidney disease, chronic liver disease, immunosuppressive disease, HIV Infection, renal transplantation, and long-term urethral catheterisation. PA tends to be more commonly encountered in the developing world. PA could be an acute abscess or chronic abscess especially in association with chronic inflammatory conditions including tuberculosis or intravesical instillations of Bacillus Calmette Guerin (BCG). PA tends to constitute 0.5% of all urology disease and 6% of all acute cases of bacterial prostatitis. The mortality rate associated with PA has tended to be between 1% and 16% of all cases of prostate abscess. PA tends to be most commonly encountered in individuals who are in their fifth to sixth decade and could occur at any age. PAs that are due to sexually transmitted organisms tend to be more commonly encountered in younger males. PA tends to affect the central zone as well as the peripheral zones of the prostate gland. Haematogenous dissemination from a primary source of infection from a primary infection elsewhere have been reported and some of the reported sources included respiratory tract, digestive tract, urinary tracts, skin, and soft tissue are very rare. PA has also been reported to be associated with staghorn calculus. Some of the reported bacterial organisms that have caused acute prostate abscess (APA) include: Escherichia Coli, Klebsiella, Pseudomonas, Proteus, Enterobacter, Enterococcus, and staphylococcus. Other causes of prostate abscess have included other bacteria and fungal infection including: Brucellosis, Salmonella, Nocardia, Mycobacterium tuberculosis. Prostate abscess has also been reported in association with malignancy of the prostate gland. Manifestations of prostate abscess could include: (a) systemic symptoms including pyrexia, chills, headache, general malaise, low back ache and in some rare cases of prostate abscess, a history of treatment for tuberculosis or contact with a person who has tuberculosis, or travel to a salmonella endemic area may be obtained and in cases of Brucellosis PAs drinking of raw milk / contact with animals may be elicited and or rare occasions treatment of superficial urothelial carcinoma with Bacillus Calmette Guerin may be elicited. (b) perineal pain, dysuria, urinary frequency, urinary urgency, retention of urine, recent prostate biopsy, visible haematuria, urethral discharge of pus, lower urinary tract obstructive symptoms with poor flow, intermittent flow, hesitancy, and sensation of incomplete emptying of the urinary bladder, retention of urine, and tenderness over the prostate gland with a feeling of bogginess and soft fluctuation. The symptoms tend to be non-specific. Diagnosis of PAs tends to be established based upon a good clinical history taking, good clinical examination, urinalysis and urine culture, routine haematology and biochemistry blood tests with evidence of raised white blood cell count and CRP and at times lymphocytosis in cases of tuberculous prostate abscess, blood culture, urine culture, PCR detection of sexually transmitted organisms, radiology imaging including trans-rectal ultra-sound scan of the prostate, or CT) scan of abdomen and pelvis including the prostate, or MRI scan of the prostate. Treatment of PA depending upon the size of the abscess has been undertaken with various options including: Appropriate antibiotic treatment alone for small abscesses based upon the antibiotic sensitivity pattern of the cultured organism, Antibiotic treatment and radiology image-guided aspiration of the abscess. Antibiotic treatment plus radiology image-guided insertion of a drain into the prostate abscess, trans-urethral incision / resection / modified resection of the prostate gland to deroof and drain the abscess, open drainage of the abscess is only undertaken on rare occasions. Within remote district hospitals in developing countries in the absence of radiology imaging, the clinician would have no choice but to undertake finger guided aspiration / drainage of the prostate abscess plus antibiotic treatment. It is important to obtain the culture and sensitivity result of the aspirated and drained pus so that if there are fungi cultured or rare organisms cultured the choice of antibacterial / antifungal treatment would depend upon the microbiology results. It is important to treat all complications urgently and appropriately including provision of intensive care. Careful clinical follow-up, laboratory investigations and radiology imaging are necessitated to ensure good recovery and to quickly identify as well as appropriately treat any recurrent abscess and on rare occasions if there is an associated prostate cancer it would be detected. The prognosis associated with the treatment of PA depends upon a number of factors including:
Reddivari and Mehta [1] made the ensuing summations related to an abscess and prostate abscess:
Considering that prostate abscess is a rare condition especially in the developed world as well radiology imaging facilities including ultrasound scan, magnetic resonance imaging (MRI) scans tend not to be readily available in remote district hospitals in some developing countries, there is the possibility that some clinicians may not be familiar with the diagnostic features and management options that are utilised to treat prostate abscesses. The ensuing article on prostate abscess is divided into two parts including: (A) Overview of general aspects of acute and chronic prostate abscess and (B) Miscellaneous narrations and discussions from some case reports, case series, and some studies related to prostate abscess including documentation of some of the organisms and conditions that have been related to the development of acute and chronic prostate abscess.
Internet data search engines were searched including Google, Google Scholar, Yahoo, and PUBMED to obtain information on prostate abscess. The search words that were used included: Prostate abscess, prostatic abscess, abscess of the prostate, abscess of prostate gland, and prostate gland abscess, acute prostate abscess, chronic prostate abscess, candida prostate abscess, bacterial prostate abscess, fungal prostate abscess, Salmonella prostate abscess, and conditions associated with prostate abscess. Seventy two (72) references were obtained which were used to write the article in two parts including: (A) Overview of general aspects of acute and chronic prostate abscess and (B) Miscellaneous narrations and discussions from some case reports, case series, and some studies related to prostate abscess including documentation of some of the organisms and conditions that have been related to the development of acute and chronic prostate abscess.
[(A)] Overview
Some of the summations related to the overview of prostate abscess include: [17]
Definition / general statements
Essential features
Terminology
Epidemiology
Pathophysiology
Aetiology
Clinical Manifestations of acute prostatic abscess.
The clinical presentations of acute prostatic abscess could divided into systemic symptoms and localised prostatic symptoms as follows: [17]
Some of the localised symptoms of acute prostatic abscess include:
Diagnosis
Laboratory
Radiology description
Differential Diagnoses
Some of the differential diagnoses of prostate abscess include:
[(B)] Miscellaneous narrations and discussions from case reports, case series, and studies related to acute prostatic abscess, and chronic prostatic abscess.
Elshal et al. [35] assessed the outcome of the drainage procedure that was used for the treatment of a prostatic abscess, in order to propose a treatment algorithm to reduce the morbidity and the need for re-treatment of prostate abscess. With regard to the patients and methods, Elshal et al. [35] retrospectively reviewed patients who had been admitted and who had undergone an interventional treatment for a prostate abscess. Elshal et al. [35] reviewed all baseline relevant variables. Elshal et al. [35] recorded details of the intervention, laboratory data, duration of hospital stay, follow-up data as well as re-admissions of the patients. Elshal et al. [35] summarised the results as follows:
Elshal et al. [35] concluded that:
Lee et al. [3] undertook a study in order to ascertain the risk factors that tend to be associated with the formation of abscess in acute bacterial prostatitis, as well as to compare the outcomes of treatment between abscess group and non-abscess group. Lee et al. [3] undertook a multi-centre retrospective cohort study in which all patients who were suspected to have an acute infection of the prostate gland underwent computed tomography (CT) scan or trans-rectal ultrasound scan of the prostate gland to differentiate acute abscess of the prostate gland from acute prostatitis without abscess formation. Lee et al. [3] summarised the results as follows:
Lee et al. [3] made the ensuing conclusions:
Abdelmoteleb et al. [4] iterated the following:
Barozzi et al. [11] stated that prostatic abscesses tend to be uncommon within clinical practice in view of the fact that utilisation of early antibiotic treatment has led to the reduction of complications of prostatitis. Barozzi et al. [11] also stated that prostatic abscess does mainly affect diabetic and immunosuppressed patients and that the organisms which most frequently tend to be involved in acute prostatic abscess tend to include: Escherichia coli and Staphylococcus, whereas gonococcus rarely tends to be encountered. Barozzii et al. [11] reported that the results in eight men with prostatic abscess they had managed showed that five of the men were treated with ultrasound-scan-guided percutaneous drainage of the abscess. They also reported that the diagnosis of prostatic abscess was clinically suspected in only three patients, and the diagnosis of prostatic abscess was confirmed by trans-rectal ultrasound scan of the prostate gland. All patients experienced complete resolution of their prostatic abscess. Barozzi et al. [11] made the following conclusions:
Tiwari et al. [28] undertook a retrospective study which was aimed to ascertain the clinical findings as well as treatment strategies in 24 patients who had been admitted due to prostatic abscess from 1999 to 2008. Tiwari et al. [28] reported that the diagnosis of prostate abscess was established clinically based upon digital rectal examination that demonstrated presence of positive fluctuation and tenderness within the prostate gland. Tiwari et al. [28] additionally stated that all cases were confirmed based upon trans-rectal ultrasound (TRUS) of the prostate gland and only positive cases were included in the study. Tiwari et al. [28] undertook the following diagnostic work-up assessment of the patients: analysis of mid-stream specimens of urine of the patients as well as analysis abscess fluid culture for pathogens. The treatment options that were used included: (a) endoscopic trans-urethral incision of the prostate (TUIP), or (b) trans-perineal aspiration of the abscess under ultrasound scan-guidance or (c) conservative treatment. With regard to the results, Tiwari et al. [28] stated the following:
Tiwari et al. [28] made the ensuing iterations:
Brede et al. [29] made the ensuing iterations about acute prostatitis, prostatic abscess, and prostatic fistula:
Susaníbar Napurí et al. [30] reported two cases of prostate abscess that had difficult management. They reported two patients who had prostatic abscess as follows: The first patient was a 73-year-old diabetic man, who was treated with utilization of a more passive approach with per-cutaneous trans-rectal drainage of the abscess fluid and after a slow response, the patient died as a result of developing sepsis. The second patient was a 59-year-old man who did experience a negative clinical response to antibiotic treatment of his prostate abscess. While he was undergoing antibiotic ambulatory care, the patient underwent trans-urethral resection of his prostate gland which did yield a successful outcome. Susaníbar Napurí et al. [30] made the following conclusions:
Schneider et al. [31] stated the following:
Schneider et al. [31] undertook a study to compare the inflammatory and infectious status of men who have prostatitis syndrome with results from their study cohort from 1992. A total of 168 symptomatic men, whose ages had ranged between 18 years and 79 years whose mean age was 43.2 years that attended the Giessen prostatitis outpatient department were included in the study. All men had undergone a standard four-glass-test including leucocyte analysis in all specimens. A routine search for Ureaplasma urealyticum and Chlamydia trachomatis was undertaken. Ejaculate analysis following World Health Organization (WHO) criteria was undertaken including the evaluation of increased number of peroxidase-positive leucocytes (PPL). The men were classified according to the National Institutes of Health (NIH) prostatitis classification. The distribution of patients according to NIH criteria was as follows: NIH II (4.2%), NIH IIIA (31.5%), NIH IIIB (50.0%) and urethra-prostatitis (14.3%). Chlamydial infection was present in one man (0.6%). Only two men with increased leucocytes within prostate secretions demonstrated greater than or equal to 106 million ml-1 PPL in semen. As compared with the cohort study 10 years earlier,, the proportion of the different subtypes of the prostatitis syndrome had remained stable. The aetiological spectrum of chronic bacterial prostatitis had not changed, however, in contrast, the prevalence of C. trachomatis was then found to be strikingly reduced. Using the WHO cut-points for leucocytospermia the inclusion of seminal leucocytes to the diagnostic process had not influenced the distribution between inflammatory (type NIH IIIA) and noninflammatory (type NIH IIIB) chronic pelvic pain syndrome. The lesson learnt from this summation is that some rare organisms could also be involved in prostatitis syndrome and prostatic abscess that emanate from the prostatitis syndrome and clinicians need to be aware that on rare occasions they may need to treat chlamydia abscesses of the prostate gland with an appropriate antibiotics pursuant to drainage or surgical treatment of prostatic abscesses.
Jang et al. [14] stated that prostate abscess is an uncommon urological disease but it does tend to have a high mortality rate if it is not treated properly. They also stated that the diagnosis and proper treatment of prostatic abscesses had remained a challenge for physicians. Jang et al. [14] compared data on conservative treatments, transurethral resection of prostatic abscess, and transrectal ultrasound (TRUS)-guided needle aspiration in 52 cases over a period of 10 years. With regard to materials and methods, Lang et al. [14] reported that the records of 52 patients who were diagnosed as having prostate abscess based upon computed tomography at Gangnam Severance Hospital between January 2000 and September 2010 were retrospectively reviewed. All of the patients were discharged when their leucocytosis had normalized and the patients had been free of fever for 2 days. Multivariate regression analysis was undertaken to ascertain independent risk factors for the length of hospitalization. Jang et al. [14] summarised the results as follows:
At the time of the diagnosis of prostatic abscess, the ages of the 52 patients had ranged between 33 years and 81 years and the mean age was 56.3 years. The average volume of the prostate was 56.3 ml and the volume of the prostate gland had ranged between 21 and 223 ml), the average prostate-specific antigen level was 18.54 ng/ml which ranged between 2.0 ng/ml and 57.0 ng/ml, and the average size of the abscess was 3.8 cm as well as the size of the prostate abscess had ranged between 2.1 and 5.5 cm.. All patients were treated by means of parenteral antibiotics during their hospital stay with intravenous antibiotics that entailed fluoroquinolone monotherapy or 3rd-generation cephalosporin in combination with an aminoglycoside. Out of the 52 patients, 22 had diabetes mellitus that amounted to 42.3%, 19 of the patients had hypertension that amounted to 36.5% of the patients, and 7 patients that amounted to 13.5%, had paraplegia due to spinal cord injury. The most common manifestations were fever in 47, 90.4% of the patients, perineal discomfort in 43, 82.7% of the patients, dysuria in 40, 76.9% of the patients, and urinary retention in 29, 55.8% of the patients. The prostate abscesses were treated by means of conservative treatment in 11 cases, transurethral resection of prostatic abscess in 23 cases, and TRUS-guided needle aspiration of the abscess in 18 cases.. The average hospitalization stay was 17.5 days and this did range from 6 days to 39 days. The average hospitalization stay of conservative treatment patients was 19.1 days and did range from 9 days to 39 days. Patients who underwent treatment by transurethral resection of prostatic abscess and TRUS-guided needle aspiration stayed for an average of 10.2 days but this did range between 6 days and 15 days; and an average stay of 23.25 days which did range, from 18 to 34 days, respectively. Of the 18 cases who had undergone needle aspiration, the prostate abscesses recurred in 4 cases that amounted to 22.2% within 1 month pursuant to the discharge of the patients. The 2 patients who had conservative treatment died due to sepsis. Jang et al. [14] did not find any independent factors that affected the average hospitalization period. Jang et al. [14] concluded that:
Thornhill et al. [33] studied the value of computed tomography (CT) scan of the prostate and pelvis as well as ultrasound scan of the prostate gland with regard to the diagnosis and follow-up of prostate abscesses that they had studied in 6 patients who had prostate abscess. With regard to the results, Thornhill et al. [33] reported that five patients had CT scan alone, one patient had had CT scan and ultrasound scan and one patient had ultrasound scan only. Thornhill et al. [33] also reported that the CT scan findings did include an enlarged prostate gland with non-enhancing fluid density collections which sometimes were multiseptated or which had enhancing rims. The ultrasound scan findings were reported to be similar in that they demonstrated a hypo-echoic mass that had thick walls. Follow-up examinations pursuant to antibiotic treatment in which one CT scan and one ultrasound scan were undertaken showed improvement or resolution. Thornhill et al. [33] concluded that:
Singh et al. [34] stated that DIFFUSION: weighted MRI (DWI) is a novel technique which is utilised to analyse the diffusion of water molecules in vivo. And that DWI has been utilised extensively in the central nervous system. As well as they stated that Its use in body imaging is on the rise and that with regard to the prostate gland, it has been utilised in the evaluation of prostatic carcinoma. Singh et al. [34] reported the DWI findings in two patients of prostate abscess and they pointed out the usefulness of MRI scan in the assessment and diagnosis of prostate abscess.
Jana et al. [36] stated that abscesses of the prostate gland usually tend to be related to gram negative bacilli. Nevertheless, methicillin-resistant Staphylococcus aureus (MRSA) had emerged as a substantial cause of prostate abscesses over recent years. Jana et al. [35] reported the case of a 31-year-old man who had a history of orthotopic liver transplantation 10 years preceding the report of the case, who had manifested with acute onset of dysuria and abdominal pain and who was diagnosed as having an MRSA prostate abscess. They stated that to their knowledge, the reported case was the first case that had described a prostate abscess in a liver transplant recipient and the first case that reported MRSA as the causative organism of a prostate abscess in a solid organ transplant recipient. A lesson learnt from this short summation is the fact that even though rare, methicillin resistant staphylococcus aureus could cause prostate abscess and therefore clinicians who treat patients who have prostate abscess should ensure that they see the culture and sensitivity results of all cases of prostate abscess fluid they send for microbiology examination to ensure they are aware of the causative organism of the abscess and the sensitivity pattern of the cultured organism to enable them treat their patients with the most appropriate antibiotics to ensure complete resolution of the abscess and to avoid or reduce the incidence of recurrent prostate abscess.
Carroll et al. [36] stated that prostate abscess is an uncommon complication of acute bacterial prostatitis and it is most commonly caused by Enterobacteriaceae. Carroll et al. [36] reported on a case of prostate abscess which was caused by Staphylococcus aureus that was successfully treated by means of a combination of antibiotic and surgical treatment. The isolate was non–multidrug-resistant, methicillin-resistant Staphylococcus aureus and which was genotyped as clonal complex 5, an emerging regional clone that tends to be trimethoprim resistant and Panton-Valentine leukocidin positive. Carroll iterated that their current reported case was the first case to report the use of clindamycin step-down treatment. Carroll et al. [36] iterated that their review of the literature had identified a further 39 cases of Staphylococcus. aureus prostate abscesses, of which 26 were methicillin resistant. Carroll et al. [36] made the following conclusions:
Liao et al. [37] stated the following: (a) Prostate abscess usually tends to be a complication of acute urinary tract infection. (b) Invasive liver abscess syndrome is characterized with Klebsiella pneumoniae related multiple organ metastasis. (c) Concomitant pyogenic liver abscess and prostate abscess had rarely been reported in the literature. (d) Recurrent episode of liver abscess is even rarer. Liao et al. [37] reported a 71-year-old man who developed acute bacterial prostate abscess and urinary tract infection that was caused by Klebsiella. pneumoniae which was associated with multiple liver abscess, psoas muscle abscess and osteomyelitis. The patient’s blood culture and urine culture yielded Klebsiella. pneumoniae, that confirmed the diagnosis of invasive liver abscess syndrome which was caused by Klebsiella. pneumoniae. The patient was successfully treated with empirical antibiotics for 6 weeks. Liao et al. [37] concluded that their reported case had emphasized the importance of timely and accurate diagnosis which should be ensued by appropriate treatment in disseminated Klebsiella. pneumoniae infection in order to prevent significant morbidity and mortality.
Bastide et al. [38] stated that fungal urinary tract infection does represent a high-risk event in severely ill patients. Bastide et al. [38] reported a case of a prostate abscess due to Candida tropicalis which was not associated with any systemic manifestations. They reported that on the first occasion, a conservative treatment with antifungal treatment and transrectal ultrasound-guided drainage was performed without success. In view of this transurethral resection of the prostate was required for drainage with a favourable course.
Somuncu et al. [39] stated prostatic abscess is uncommon but; however, serious disease and that prostatic abscess should be diagnosed at an early stage by the combination of clinical examination and transrectal ultrasound, as well as drained. Somuncu et al. [39] treated a 79-year-old man who had multiple prostate abscesses (PAs) by utilising lavage of the saline and antibiotic (cefoxitin) pursuant to transrectal ultrasound-guided transrectal puncture and aspiration of the abscess. Somuncu et al. [39] reported that that at his 12 months follow-up there was no evidence of recurrence of his prostate abscess based upon his clinical examinations and ultrasound scan follow-up assessments over the period of one year. .
Chou et al [40] undertook a study to analyse the trans-rectal ultrasound (US), or TRUS and colour Doppler ultrasonography (CDU) findings as well as treatment strategies with TRUS-guided procedures in 13 patients who had prostate abscess. They reported that over a period of 6 years, 18 prostate abscesses had been diagnosed in 13 patients whose mean age was 59 years. They reported that the diagnostic work up of the patients did include TRUS, analysis of mid-stream specimens of urine, as well as analysis, as well as analysis and culture of the prostate abscess fluid for leucocytes and pathogens. With regard to the treatment of the patients, the patients were treated either by a conservative treatment option with regard to abscesses that were less than 1 cm in diameter, or by means of aspiration of the prostate abscess or drainage of the prostate abscess of the abscesses were either 1 cm or greater than 1 cm in diameter. Chou et al. [40] corelated the CDU findings to the treatment effects. Chou et al. [40] also reviewed the predisposing factors for the development of the prostate abscess. They reported that with regard to the 13 patients, the commonest clinical manifestations were urinary frequency in 77% of the patients, and pus cells within the mid-stream urine in 92% of the patients. Predisposing factors were found in 11 men, and 5 of the men had diabetes mellitus. With regard to 10 patients, the definitive peri-interventional diagnosed was based upon trans rectal ultrasound scan (TRUS) findings. TRUS with probe palpation did demonstrate tiny floating echogenic speckles within the abscess cavity with regard to 4 patients. CDU had demonstrated increased colour-flow signals at the margin and encompassing tissue of the abscess pockets. Abscesses that had poorly defined boundaries did have more prominent surrounding colour-flow signals and had achieved, with relative difficulty, a satisfactory aspiration procedure. Aspiration was undertaken for all 11 abscesses that measured between 1 cm and 3 cm. A total of 4 larger abscesses that measured more than 3.0 cm were treated with aspiration or drainage utilizing a 5-French pigtail catheter. No surgical drainage was undertaken. Chou et al. [40] made the ensuing iterations:
Trans-rectal CDU could help in the evaluation of maturity of an abscess pocket. US-guided aspiration with an 18-gauge needle or drainage with a 5-French pigtail catheter significantly shortened the hospital stay.
Varkarakis et al [41] undertook a study to evaluate the feasibility and effectiveness of three-dimensional ultrasound-guided trans-perineal puncture and drainage of prostate abscesses. They reported that between 1985 and 2003, a prostate abscess was diagnosed in 22 men. One of the treatment options used to drain the abscesses was trans-perineal puncture under three-dimensional ultrasound scan-guidance. They compared the post-operative results with the outcomes of other modalities. With regard to the results, Varkarakis et al. [41] reported that the average age of the patients was 52 years and predisposing factors were found in 12 patients. Trans-perineal puncture of the prostate abscess was undertaken in 7 patients under general anaesthesia. In addition to antibiotic treatment, a nephrostomy tube was left in place in all of the patients for a mean period of 3 days to drain the prostate abscess. All of the patients were treated effectively without any additional treatment or complications. Varkarakis et al. [41] concluded that three-dimensional ultrasound scan-guided trans-perineal puncture was a minimally invasive and effective technique to be utilized for the treatment of prostate abscesses.
Basiri eand Jayaherforooshzadeh [42] stated that prostate abscess is an uncommon infection which can be treated by antibiotic administration and drainage and the reported mortality rate of the prostate abscess is between 3% and 16%. They also stated that with regard to patients who are refractory to medical treatment, surgical interventions are advocated. They reported a patient with the prostate abscess who was treated with percutaneous drainage. Basiri et al. [42] reported a 67-year-old man who had obstructive lower urinary symptoms and prostate-specific antigen level of 8.9 ng/mL who had undergone trans-perineal prostate biopsy. Three days subsequently, the patient manifested as an the emergency with fever, chills, and poor general condition. His clinical examination demonstrated that his blood pressure, pulse rate, and temperature were 130/80 mmHg, 105 per minute, and 39°C, respectively. He had a digital rectal examination which demonstrated that he had a huge enlarged prostate with a prominent left lobe. He had urine and blood cultures, preceding the commencement of his antibiotic treatment and both cultures exhibited Escherichia coli. He had trans-abdominal ultrasound scan of the prostate gland which demonstrated a hypo-echoic mass that contained abundant debris within his left lobe of the prostate gland. He had computed tomography (CT) scan which showed a 5 cm × 8 cm homogenous mass that had a low density upon the same region of his prostate gland. He received vancomycin, metronidazole, and ceftazidime intravenously. He subsequently underwent percutaneous drainage of the prostate abscess in view of his unresponsiveness to his medical treatment. His prostate abscess was drained transperineally with utilization of trans-rectal ultrasonography (TRUS) guidance and a suprapubic cystostomy was undertaken. A Pigtail catheter was inserted into the abscess cavity and irrigation of the abscess cavity was undertaken twice per day with utilization of saline and antibiotics. On the 5th day, following discontinuation / stoppage of discharge of pus from his drainage catheter, the Pigtail catheter and the cystostomy were removed. One month subsequently, his symptoms had resolved and the abscess had diminished in size based upon the features of his follow-up assessment computed tomography (CT) scan. He was referred to the clinic of the authors again with obstructive lower urinary tract symptoms and medical treatment was commenced anew. In view of failed medical treatments, open prostatectomy was undertaken 5 months later. The patient was completely symptom-free at the time of the publication of the case report. Basiri et al. [42] made the ensuing summations related to prostate abscess:
El-Shazly et al. [49] stated that the incidence of prostate abscess (PA) has markedly decreased with the widespread utilization of antibiotics and the decreasing incidence of urethral gonococcal infections. El-Shazly et al. [50] evaluated different treatment options for prostate abscess in order to describe technical points which would improve the outcome of transurethral (TUR) drainage of prostate abscess. El-Shazly et al. [49] undertook a retrospective study of a series of 11 patients who were diagnosed as having prostate abscess, who had been admitted and treated within Farwaniya Hospital, Kuwait, between February 2008 and November 2010. Drainage of the prostate was indicated when antibiotic treatment was not ensued by clinical improvement and after the diagnosis of prostate abscess was confirmed by TRUS (Transrectal ultrasonography) and/or CT computed Tomography scan. TUR drainage was undertaken in 7 cases, ultrasound-guided trans-rectal drainage was undertaken in 2 cases, and ultrasound-guided perineal drainage was undertaken in 2 cases. With regard to the results, El-Shazly et al. [49] reported that all of the patients had undergone Trans-urethral-drainage (TUR-drainage) of the prostate and they all had successful outcomes without the need to undergo secondary treatment or further surgery. El-Shazly et al. [49] made the ensuing conclusions:
Granados et al. [6] reported a series of 25 men who had prostate abscesses that they had studied during an 11-year interval in whom prostate fluctuation upon digital rectal examination was the most characteristic sign. Transrectal ultrasound was the most reliable method for diagnosis and transurethral drainage under antibiotic coverage was the ideal treatment for this disease.
Baral et al. [50] stated that tuberculosis of the prostate gland is one of the rarest findings within clinical practice and abscess of prostate associated with tuberculosis of the prostate gland is even scarce in the reported literature. Baral et al. [50] reported a case of tuberculosis of the prostate gland which was complicated by huge prostate abscess. Baral et al. [50] reported a 68-year-old man who did not have any comorbidity who had manifested with a history of increased frequency of voiding that was associated with poor urinary flow, urinary urgency as well as nocturia over the preceding 17 days. He had been undergoing medical treatment for benign enlargement of his prostate gland for a period of 2 years. He had digital rectal examination which demonstrated a boggy cystic swelling anteriorly and enlarged prostate gland with mild tenderness. He had ultrasound scan of his abdomen and pelvis which demonstrated massive enlargement of his prostate gland with central avascular necrotic area with moving internal echoes. He had contrast-enhanced computed tomography (CECT) scan which demonstrated a 230 grams of prostate gland with central liquefaction of about 101 cubic mm3. He underwent trans-urethral loop drainage of the prostatic abscess together with trans-urethral resection of the prostate gland (TURP). Histopathology examination of the specimen demonstrated granulomatous prostatitis which was highly suggestive tuberculosis of the prostate gland. His prostatic abscess culture was negative. At the time of the case report, the patient was undergoing category 1 anti-tuberculosis treatment.. Baral et al. [50] stated the following:
.Baral et al. [50] concluded that trans-urethral loop drainage of prostatic abscess is a safe treatment option for patients who manifest with tuberculous prostatic abscess which is then followed by anti-tuberculosis treatment if the histopathology examination features of the specimen are suggestive of granulomatous lesions of the prostate gland.
Kim et al. [51] stated that Klebsiella pneumonia (KP) is related to a metastatic phenomenon from the originally affected primary organ and that approximately 28% of patients who have pyogenic liver abscess arising from KP do suffer from metastatic complications. Kim et al. [51] undertook a study I order to define the clinical features of KP-induced prostatic abscess. Kim et al. [51] reported that a total of 14 patients were diagnosed as having prostate abscess based upon clinical, laboratory examination and abdominopelvic computed tomography (CT) scan from 2007 to 2013. Kim et al. [51] summarised the results as follows: Out of the 14 patients, KP was the dominant causative microorganism in 6 patients that amounted to 42.9% of the patients, which was followed by Escherichia coli in 2 patient, Pseudomonas aeroginosa in 1 patient, methicillin-resistant Staphyolcoccus aureus in 1 patient, and no growth in either the urine or blood culture in 4 patients. Four patients that amounted to 66.7% of the 6 KP induced-prostate abscess had other concurrent abscess sites besides the prostate that included the liver in 3 patients, the kidney in 1 patient, and the perianal area with endogenous endophthalmitis that ended in loss of vision in 1 patient. Kim et al. [51] made the following conclusions:
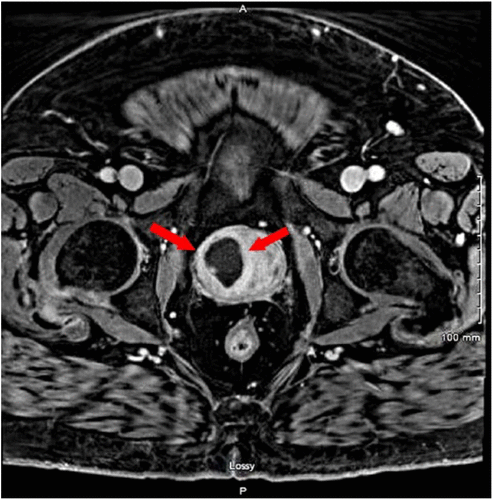
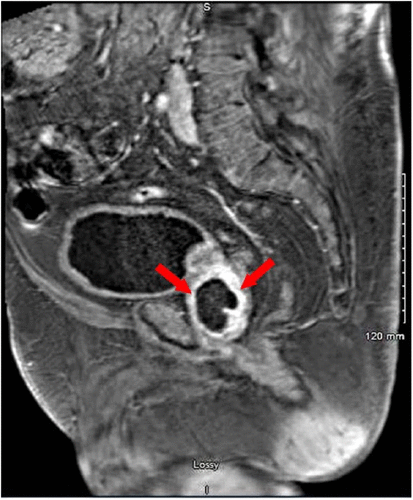
Ullah et al. [52] reported a 60-year-old man who manifested with fever, chills, cough, and shortness of breath. He denied having any abdominal pain, urinary urgency, dysuria, or haematuria. The results of his routine haematology and biochemistry laboratory tests demonstrated an elevated white blood cell count and lactic acid, and one set of blood culture stained positively for gram-positive cocci. He was empirically commenced on intravenous antibiotics. On the next hospital day, the patient complained of haematuria and lower abdominal discomfort. He had computed tomography scan of his abdomen and pelvis which demonstrated focal hypodensity relating to his prostate abscess, which was subsequently confirmed based upon magnetic resonance imaging (MRI) scan of the prostate (see figures 1 and 2). The final report of his blood cultures confirmed a growth of methicillin-resistant Staphylococcus aureus. He was treated by means of intravenous vancomycin and transurethral resection as well as deroofing of the prostate gland with drainage of the abscess fluid which resulted in complete resolution of his symptoms. Patient was reviewed within the hospital of the authors by the Urology team about 3 weeks later, and he did not have any urological issues. He had repeated blood and urine cultures which did not report any growth of an organism. He received a total of 1 month of antibiotic treatment
Deshpande et al. [53] made the ensuing iterations about prostate abscess:
Deshpande et al. [53] reported a 49-year-old man who manifested with 5 and tenderness of the scrotum and adjacent perineum. He had an elevated white blood cell count and his blood and urine days of fever and chills that was associated with scrotal pain and swelling. He was found upon examination to have a temperature of 100.7 degrees Fahrenheit cultures were negative. He had contrast-enhanced computed tomography (CT) scan which demonstrated an enlarged prostate gland which contained a 4 cm septated hypodense lesion that had contrast-enhancing walls as well as encompassing fatty inflammation. He was commenced upon ciprofloxacin antibiotic treatment. He underwent cystoscopy-guided trans-urethral drainage of the abscess together with resection of the prostate gland with removal of about 50 ml of purulent pus. Culture of the pus grew MRSA that was sensitive to vancomycin, tetracycline, ciprofloxacin, as well as trimethoprim/sulfamethoxazole. Histopathology examination of the resected specimens demonstrated benign prostate tissue and urothelial mucosa with evidence of acute and chronic inflammation. His antibiotic treatment was changed to intravenous vancomycin. He discharged himself against medical advice but he was discharged home on oral doxycycline which he continued for 6 weeks. He had a follow-up CT scan 8 weeks pursuant to his initial manifestation which demonstrated marked interval improvement.
Sakamati et al. [54] sated that Nocardia farcinica usually does infect the respiratory tract and it can sometimes cause central nervous system infections; nevertheless, Nocardia farcinia rarely infects the prostate gland. Sakamaki et al. [54] reported the first case of N. farcinica that was identified within the purulence specimen that was drained from a prostate abscess. A 70-year-old Japanese man who was receiving steroid and cyclosporine treatment presented with chief complaint of turbid urine. His urine microscopy demonstrated 100 white blood cells per high power field and bacteria. He had computed tomography (CT) scan of abdomen and pelvis which showed a low-density lesion within his prostate gland that measured 4.0 cm x 5.0 cm x 5.0 cm (see figure 3). Gram staining of his urine did demonstrate gram-positive, filamentous, branching rods (see figure 4a). Kinyoun staining of his urine demonstrated filamentous, branching rods (see figure 4b). His urine culture was positive for N. farcinica, and the presence of this organism was confirmed by mass spectrometric analysis. The antibiotic drug sensitivity analysis of the cultured organism is demonstrated in Table 1.



He received treatment by means of oral trimethoprim/sulfamethoxazole (TMP/SMX) 320/1600 mg/day (6.4/32 mg/kg/day). On the 6th day pursuant to commencement of his treatment, his serum creatinine level was raised at 1.53 mg/dL. Because of his acute kidney injury, his antimicrobial treatment was changed to imipenem/cilastatin (IPM/CS) 1.5 g/day (30 mg/kg/day). On the 11th day from the commencement of his treatment with TMP/SMX, trans-perineal prostatic drainage with percutaneous vesicostomy was undertaken. The culture of the drained pus was positive for N. farcinica. On the 18th day, the patient was recommenced on oral TMP/SMX 80/400 mg/day (1.6/8 mg/kg/day) that was increased gradually to 320/1600 mg/day following discontinuation of the intravenous IPM/CS administration. Nevertheless, his serum creatinine level was found to be raised again. The TMP/SMX dose was reduced to 160/800 mg/day (3.2/16 mg/kg/day), and clavulanate/amoxicillin (CVA/AMPC) 1500 mg/day (30 mg/kg/day) was added. After 60 days from the commencement treatment against nocardiosis, the patient was eventually discharged on TMX/SMX 160/800 mg/day and CVA/AMPC 2250 mg/day (45 mg/kg/day). He continued to take the medications for about 12 months in the outpatient setting. Sakamaki et al. [54] made the following conclusions:
Scorey and Daniel. [55] stated the following:
Scorey and Daniel. [55] reported what in their opinion was the first case of a prostate abscess that was caused by Nocardia farcinica in a man who had a history of severe psoriasis and psoriatic arthritis. The man had been on long term immunosuppression for his psoriasis and psoriatic arthritis with prednisolone and etanercept. Scorey and Daniel. [55] felt that the Nocardia was likely contracted via direct skin inoculation while the patient was gardening with haematological dissemination to the prostate. He did respond well to long term sulfamethoxazole and trimethoprim.
Scorey and Daniel. [55] reported a 68 year old man who had manifested in March 2015 with a one week history of intermittent dysuria as well as suprapubic pain. He had a two day history of hesitancy before voiding, fever, vomiting, diarrhoea and dyspnoea. Three weeks prior to his presentation he had cut his left middle finger when he was gardening and which became infected and for which he received a one week course of amoxicillin.
He had been immunosuppressed heavily for 30 years for severe psoriasis and psoriatic arthritis. He had been taking prednisolone 10 mg daily and etanercept 50 mg weekly for the preceding 5 years. Two days into his admission he developed retention of urine for which he was catheterised. He had a digital rectal examination which demonstrated a tender prostate gland. He had computed tomography (CT) scan of abdomen and pelvis which demonstrated a 3.6 cm × 3 cm × 3.4 cm left prostate abscess as well as a possible sub-centimetre abscess which had involved his right lobe of prostate (see figure 5). His antibiotics were next changed to 500 mg twice per day of intravenous ciprofloxacin.

On the 6th day his blood culture specimens that were taken prior to commencement of his antibiotics on the first grew N. farcinica. The identification was undertaken by 16 s rRNA gene sequencing. Trimethoprim and sulfamethoxazole (TMP-SMX) treatment were next started in addition. He furthermore had blood cultures taken on the 7th day as well as 10th day which did not grow any organism. He had a computed tomography (CT) scan of his thorax and brain which did not demonstrate any evidence of Nocardia seeding even though a 5 mm soft tissue nodule was demonstrated within his right lower lobe. He did respond to treatment and the levels of his inflammatory markers returned to within normal range. He was subsequently discharged home pursuant to 15 days of him being on oral ciprofloxacin and TMP-SMX. The etanercept was withheld indefinitely and prednisolone was weaned back onto his normal dose of treatment. He had at the time of publication of the article been on antibiotics for 8 months and he had had a repeat CT scan which demonstrated resolution of his prostate abscess. Scorey and Daniel. [55] Made the following conclusions:
Goyal et al. [56] reported their experience of prostate abscess management by the undertaking of modified transurethral resection (TUR) technique. With regard to the methods, Goyal et al. [56] reported that Seventeen men who had prostate abscess and had undergone TUR between 2003 and 2011 were retrospectively analysed. Goyal et al. [56] noted the details of demography, surgical procedures, complications, and follow-up. Goyal et al. [56] summarized the results as follows:
Goyal et al. [56] made the following conclusions:
Gilmore et al. [57] reported a healthy 6-year-old man who had rare case of a prostate abscess which he had developed following iodine-125 seed brachytherapy he had undergone as treatment for prostate adenocarcinoma. Gilmore et al. [57] iterated that the only other documented case of prostate abscess that developed after brachytherapy was reported in an HIV-positive man whose underlying pathology turned out to be squamous cell carcinoma of the prostate and rectum.
Bae et al. [58] stated that emphysematous prostatic abscess is a very uncommon form of prostatitis and that emphysematous prostate abscess due to Klebsiella pneumoniae could have a poor prognosis according to a few previous reports. Bae et al. [58] reported a rare case of successfully treated emphysematous prostate abscess with cystitis due to Klebsiella pneumoniae in a 50-yr-old man who had a 15-year history of diabetes mellitus, who was referred to the emergency room of their hospital. The KUB film demonstrated gas shadows within the lower pelvic area which was suggestive of emphysematous cystitis or emphysematous prostatic abscess. The gas had mainly occupied the prostate and was also observed in the bladder on computed tomography (CT) scan of pelvis. He was successfully treated with long-term antibiotic utilisation and additional percutaneous drainage of the abscess. Bae et al. [58] made the ensuing iterations:
Share this article Share with email Share with twitter Share with linkedin Share with facebook
Chuang et al. [59] reported a young alcoholic and heavy smoker who was admitted because of Klebsiella pneumoniae bacteraemia. He had Contrast-enhanced Computed tomography (CT) scan of abdomen and pelvis which demonstrated an abscess within his the right lobe of his prostate gland. He did develop blurred vision of his left eye on the third day during his admission. His initial eye examination revealed mild reaction within his anterior chamber and vitreous as well as multiple Roth's spots within his retina. The administration of empirical antibiotics that included cefazolin and gentamicin intravenously was changed to ceftriaxone and amikacin following ophthalmologic consultation. After he had received parenteral antibiotics for 3 weeks, his systemic condition was controlled, and his vision did remain stable. Chuang et al. [59] stated that over the past decades, many cases of endogenous Klebsiella pneumoniae endophthalmitis that were associated with liver abscess had been reported in Taiwan. Nevertheless, documented reports of this condition associated with a prostate abscess were not common but rare. Chuang et al. [59] reported a case of Endogenous Klebsiella pneumoniae endophthalmitis that was associated with prostate abscess:, which was classified as posterior focal endogenous endophthalmitis, that had good prognosis under appropriate antibiotic treatment. Chuang et al. [59] iterated that early diagnosis and prompt treatment are important for the control of sepsis and restoration of vision.
Stafford and Prybys. [60] reported a 57-year-old African American male patient who had a past history of hypertension and long-standing end-stage renal disease (ESRD) who was on maintenance haemodialysis through a left upper extremity arteriovenous fistula who had manifested with penile pain and discharge for one day. He did report that he had been anuric for many years; nevertheless, on the day preceding his presentation, he had started experiencing a scanty amount of thick urethral discharge. His genitourinary examination demonstrated a scanty amount of urethral discharge and no other abnormality. He had a right-sided inguinal lymphadenopathy. His digital rectal examination demonstrated an enlarged and boggy as well as tender prostate gland upon palpation. A urethral swab of his discharge fluid was obtained for gram stain, culture, and polymerase chain reaction assay for gonorrhoea and chlamydia DNA. Resistance to swab passage within the distal urethra was noted. In view of concern for him having prostatitis and sexually transmitted infection, he was given a single-dose treatment regimen of ceftriaxone, azithromycin, and metronidazole, with a plan to prescribe for him ciprofloxacin as outpatient treatment of prostatitis. Nevertheless, about 60 minutes after the urethral swabbing was undertaken, he then developed a large amount of purulent drainage from his urethra, which was cultured. His repeat vital signs at that time showed a heart rate of 120, blood pressure 160/100, respiratory rate 22, and temperature 101.7 Fahrenheit which established a diagnosis of early sepsis, which was initially considered to be secondary to pyelonephritis in the setting of anuria. Following various routine laboratory investigations and blood culture specimens being sent to the laboratory he was commenced on vancomycin and piperacillin/tazobactam. He had contrast-enhanced computed tomography (CECT) of the abdomen and pelvis which demonstrated communication between the posterior bladder wall and the seminal vesicles and a large prostatic abscess (see figure 6). Following his admission to the hospital, the a Foley urethral catheter was inserted for further bladder irrigation and drainage. Following a successful drainage of the prostate abscess through a percutaneous drain that was inserted by an interventional radiologist, the Foley catheter was removed.

The results of cultures of the discharge fluid and of the prostate abscess after the drain was inserted both demonstrated Escherichia coli which was resistant to ampicillin, gentamicin, tetracycline, tobramycin, and trimethoprim/sulfamethoxazole, and sensitive to cephalosporins, carbapenems, fluoroquinolones, and piperacillin/tazobactam. His blood and stool cultures did not grow any organism. He recovered and was discharged on a two-week course of ciprofloxacin with urology follow up.
Liao et al. [37] stated the following:
Liao et al. [37] reported a 71-year-old man who had acute bacterial prostate abscess and urinary tract infection that was caused by Klebsiella pneumoniae that was associated with multiple liver abscess, psoas muscle abscess and osteomyelitis. His blood culture and urine culture grew Klebsiella. pneumoniae, which confirmed the diagnosis of invasive liver abscess syndrome that was caused by Klebsiella pneumoniae. He was successfully treated with empirical antibiotics for 6 weeks. Liao et al. [37] made the following conclusions:
Walker et al. [61] stated the following:
Walker et al. [61] undertook a retrospective review of adult patients who were admitted to a tertiary care hospital between 2008 and 2018 and who had a diagnosis of Staphylococcus. aureus Prostate Abscess. Walker et al. [61] summarised the results as follows:
Walker et al. [61] made the following conclusions:
Arrabal-Polo et al. [62] stated that the incidence of prostate abscess is 0.5% in relation to all prostate pathologies and that prostate abscess usually does occur in patients who have diabetes mellitus or with some degree of immunosuppression. Arrabal-Polo et al. [62] reported the case of an 84 years-old man who had a history of arterial hypertension and mild renal failure, who had manifested with high fever, prostate syndrome, genital oedema and constipation. He was diagnosed as having prostate abscess by means of trans-rectal ultrasonography (TRUS). His treatment was commenced with empirical meropenem and a puncture of the abscess was undertaken transperineally under TRUS guidance with insertion of an 8-Fr nephrostomy tube for 36 hours. He was discharged 48 hours pursuant to the puncture of the prostate abscess with a good prognosis. Arrabal-Polo et al. [62] made the following conclusions:
Quraishi et al. [63] stated the following:
Quraishi et al. [63] reported a case of a 70-year-old man who had manifested with sepsis, that was found to have originated from a complex prostate abscess. The patient did not have any history of urinary tract infections or risk factors. Quraishi et al. [63] believed that the incidentally identified staghorn calculi had promoted the growth of Proteus mirabilis which had led to the development of the prostate abscess. The patient underwent a transurethral resection of his prostate gland and drainage of the abscess following a failed course of antibiotic treatment. Quraishi et al. [] stated that their reported case also highlighted the paucity of guidelines that were available for the treatment of prostate abscesses.
Dakdouki et al. [64] stated that Brucellosis is a multi-system disease which tends to be endemic in many Mediterranean countries including Lebanon. Nevertheless, human Brucella prostate abscess had not been previously reported in the English medical literature. Dakdouki et al. [64] reported the case of a young man who had manifested with fever and urinary symptoms, and who subsequently was demonstrated to have culture confirmed Brucella prostate abscess. The culture of drained prostate pus grew Brucella melitensis.
Alenazi et al. [65] reported a 54-year-old man, who was a known diabetic patient and who had manifested with a chief complaint of dysuria, weak urine stream, suprapubic pain radiating to perineal area, urethral pus discharge, and fever for about a 2-week duration. His symptoms had not improved pursuant to receiving a 1 week course of antibiotics. He reported that he had ingested raw milk prior to the commencement of his presenting symptoms. Upon examination, he was found to have high-grade fever otherwise his vital sign examination findings were unremarkable. He had a digital rectal examination which revealed an enlarged and tender prostate gland. The results of his laboratory tests revealed mild leucocytosis and elevated lymphocytes as well as monocytes. His urine analysis demonstrated pus cells as well as red blood cells. He had trans-rectal ultrasonography and computed tomography (CT) scan which did confirm the diagnosis of prostate abscess. Trans-urethral drainage of the prostate abscess, was undertaken for the patient and foley's and suprapubic catheter were inserted to relieve the obstruction. The culture of his prostatic pus culture and titration were positive for Brucella Bactria. Postoperatively, he received intravenous (IV) fluids and antibiotics which included sulfamethoxazole/trimethoprim and gentamicin. One week following his surgery, he developed low-grade fever and his urine culture grew Staphylococcus species and he received ciprofloxacin. Two weeks later, he had improved and he was discharged home on Sulfamethoxazole/trimethoprim. During his follow-up assessment, CT scan, was undertaken and no further collection of abscess was identified with evidence of complete resolution of the prostate abscess.
Alenazi et al. [65] made the ensuing summing iterations:
Prostatic abscess is uncommon case in clinical practice especially with prevalent use of antibiotics. [66] There are different mechanisms exist regarding causation, which include acute or chronic prostatitis; retrograde stream of contaminated urine; or hematogenous spread of distant infection. [67] Predisposing factors for the incidence of prostatic abscess include diabetes, urinary catheter, bladder outlet blockade, chronic renal failure, and chronic liver disorder. [68] It has been stated that, prostatic abscess is mainly caused by Gram-negative enterobacteriaceae including E. coli (Barozzi et al., 1998). [11] Their patient was known to have diabetes as a predisposing risk factor with history of ingestion of raw milk. The patient was diagnosed as having brucellosis based upon serology test and thus was proposed to be the source for hematogenous spread of the infection into prostate. The obtained pus culture demonstrated that the prostate abscess contained Brucella organisms. The patient was treated by means of intravenous (IV) fluids and antibiotics that included sulfamethoxazole/trimethoprim, Gentamicin, and ciprofloxacin. Transurethral drainage of the prostate abscess was undertaken for the patient with foley's and suprapubic catheter insertion to obviate the obstruction.
Alenazi et al. [65] summated their case report by stating the following:
Alenazi et al. [65] made the following conclusions: (a) Their reported case was the first case of prostate abscess that was caused by Brucella bacteria in Saudi Arabia. (b) clinicians should consider Brucella infection in their history and management approach for patients who have clinically suspected prostate abscess.
Gupta et al. [69] stated the following:
Gupta et al. [69] reported a case of Candida glabrata prostate abscess which was successfully treated with utilisation of micafungin. Gupta et al. [69] also reported that adequate concentrations of micafungin were demonstrated during the treatment of the fungal prostate abscess.
Lin and Patel. [25] reported a 50-year-old immunocompetent man who had a past medical history that was significant for childhood malaria who had manifested with fevers and myalgias pursuant to his trip to Ghana one week preceding his presentation. He at first denied any focal infectious symptoms, including cough, chest pain, and shortness of breath, dysuria, nausea, abdominal pain, or diarrhoea. During his trip to Ghana, he stayed in a rural village that had indoor plumbing, and he ate home-cooked food, as well as he drank bottled water, and he was not aware of having had any contact with any individual or individuals who were sick or ill. His vital signs upon presentation were as follows: temperature 102˚F, heart rate 133 bpm, blood pressure 127/88 mmHg, and oxygen saturation 98% on ambient air. Upon his clinical examination he did appear to be fatigued with dry mucous membranes, he was tachycardic with a regular rhythm, apart from that no other significant findings were found upon his examination. The results of laboratory tests were summarised as follows: White blood cell count of 12,000/µL with 86.1% neutrophils and 70 bands/µL. The results of his first blood cultures, urinalysis, and chest X-ray were unremarkable. In view of his recent travel and concern for infection, a broad infectious work-up was undertaken to ascertain the cause of his symptoms. The results of his nasal influenza/respiratory syncytial viral swab, HIV-1/HIV-2, dengue IgM, Zika IgM, and blood smears for malaria were reported as negative. Considering his persistent high fevers and recent travel to an endemic area for malaria, he was empirically treated for malaria with atovaquone/proguanil which was not associated with any significant improvement in his symptoms. On the 2nd day of his admission to hospital 2, the patient had a temperature of 101.6˚F and developed dysuria as well as visible haematuria. He had a repeat urinalysis which showed pyuria and 2+ blood, and he was empirically commenced on ceftriaxone. The results of his urine culture subsequently demonstrated ceftriaxone-sensitive Salmonella non-typhi Group B serotype. He continued to have fevers and on his 4th day of admission to hospital, he did develop non-bloody diarrhoea. He had stool bacterial testing and this demonstrated the same strain of Salmonella. The results of his blood cultures continued to remain negative. In view of his persistent fevers, he had a contrast-enhanced computed tomography (CECT) scan of his abdomen and pelvis which demonstrated multi-focal prostate abscesses (see figure 7). He patient underwent trans-gluteal drainage of his prostate abscesses and the resultant cultures grew the same Salmonella pathogen. His fever curve subsequently improved, and following this, he was discharged on an extended course of trimethoprim-sulfamethoxazole. The lesson that needs to be learnt from this case report is that Salmonella prostate abscess though uncommon does exist and for this reason clinicians need to have a high index of suspicion for Salmonella prostate abscess especially in individuals who travel to and back from Salmonella endemic areas.

Reproduced from: [25] Lin C, Patel S. Salmonella Prostatic Abscess in an Immunocompetent Patient. Cureus. 2020 July 10; 12(7): e9122. doi:10.7759/cureus.9122 https://www.cureus.com/articles/34896-salmonella-prostatic-abscess-in-an-immunocompetent-patient under Creative Commons Attribution License which permits reproduction of contents and figures from the Cureus articles provided the original source is cited and credited.
Aust et al. [70] reported a case of tubercular prostatic abscess in a patient who had undergone intravesical bacillus Calmette-Guérin immunotherapy for bladder carcinoma in situ. His abscess did require surgical drainage and anti-tuberculous treatment.
Bour et al. [71] reported the diffusion and contrast-enhanced MRI appearance of five cases of granulomatous prostatitis (GP), non-specific (two cases) and infectious post-Bacillus Calmette-Guerin (BCG) therapy (three cases, with a tubercular abscess in two of them). All of the patients did have raising PSA levels and abnormal digital rectal examination (DRE) findings. Bour et al. [71] reported that a history of BCG treatment or acute prostatitis was present in four of the patients. Multiparametric MRI (T2W-MRI, DW-MRI and DCE-MRI) was undertaken before the biopsies were taken. The diagnosis of granulomatous prostatitis and tuberculous prostate abscess was confirmed by TRUS-guided biopsies in four cases and by transurethral resection in one case. MRI scan demonstrated a tumour-like appearance in three cases, an abscess-like appearance in one case and a combined tumour/abscess-like appearance in one case. Extra-prostatic fat was found to be infiltrated in three patients that simulated T3a disease. Histopathology examination of the specimens showed caseous necrosis when the MRI scan showed abcedation. Bour et al. [71] stated that the demonstration of occult tubercular abscesses in post-BCG GP could have therapeutic implications and MRI is useful prior to surgical or interventional drainage of large caseous abscesses.
Wang et al. [72] made the ensuing summating iterations about prostate abscess:
Wang et al. [72] reported a 67-year-old man who did not have any underlying diseases, who manifested with acute prostatitis. He underwent trans-rectal ultrasound (TRUS) scan 14 days after commencement of his antibiotic treatment which demonstrated a fluid-containing irregular mass. Doppler ultrasound scan demonstrated high vascularity encompassing the margin of the mass. Advanced prostate cancer with necrosis was found within tissue that was obtained from trans-urethral resection of the prostate (TURP). His symptoms did improve considerably pursuant to his undergoing TURP and he received androgen deprivation treatment in the outpatient clinic. Wang et al. [72] stated that even though ultrasound-guided needle aspiration of prostate abscess does remain the mainstream treatment for prostate abscess, TURP should be considered with regard to patients who have complicated prostate abscess or suspected carcinoma of the prostate gland.
None
Acknowledgements to:
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
