AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Farid Gharagozloo, M.D., FACS, Center for Advanced thoracic Surgery. 400 celebration Place, Celebration, 34786, Florida.
Citation: Farid Gharagozloo and Mark Meyer. (2022). Proposed Pathogenesis for a Subgroup of Patients with Neurogenic Thoracic Outlet Syndrome. J Clinical Surgery and Research, 3(4); DOI:10.31579/2768-2757/045
Copyright: © 2022, Farid Gharagozloo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 March 2022 | Accepted: 16 March 2022 | Published: 24 March 2022
Keywords: : neurogenic; thoracic outlet syndrome (TOS); bony tubercle; first rib; robotic first rib resection
Most patients with Neurogenic Thoracic Outlet Syndrome (TOS) have upper extremity pain and paresthesia with normal neurologic examination and objective tests. The purpose of this study was to determine the pathologic nature of the resected first ribs in a subgroup of patients TOS who experienced resolution of symptoms postoperatively.
Methods: In a retrospective study, we compared normal human cadaver first ribs (control, C) with first ribs from patients with proven NTOS (N). Ribs were examined for anatomic features. Preoperative and postoperative dynamic Magnetic Resonance Angiograms (MRA) of the affected and contralateral upper extremities were examined.
Results: There were 41 first ribs from patients with DNTOS and 12 normal first ribs from human cadavers. In all patients (100%) with DNTOS there was a bony tubercle which corresponded to the area of subclavian vein groove in the normal ribs.
Conclusion: A bony tubercle at the site of the subclavian vein groove in patients with DNTOS may be the pathologic entity which causes extrinsic compression of the subclavian vein at rest. The neurologic symptoms resolve following disarticulation and resection of the medial aspect of the first rib. In a subgroup of patients, NTOS may be the manifestation of venous ischemia of the nerves of the upper extremity as opposed to nerve compression.
Type of Research: Single-center retrospective cohort study.
Key Findings: A bony tubercle at the site of the subclavian vein groove in a subgroup of patients affected with DNTOS is the pathologic entity which causes extrinsic compression of the subclavian vein at rest. In these patients the neurologic symptoms resolve following disarticulation and resection of the medial aspect of the first rib.
Take Home Message: A subgroup of patients with Disputed Neurogenic Thoracic Outlet Syndrome may have neurologic symptoms caused by venous ischemia of the upper extremity which is caused by extrinsic compression of the subclavian vein by a bony tubercle on the first rib at the costo-sternal joint.
Table of Content Summary: This retrospective study compared normal human cadaver first ribs with first ribs from patients with proven NTOS (N). Proof of NTOS was symptom resolution following resection of the medial aspect of the first rib. The study suggests that in a subgroup of patients with Disputed Neurogenic Thoracic Outlet Syndrome, neurologic symptoms caused by venous ischemia of the upper extremity which is caused by extrinsic compression of the subclavian vein by a bony tubercle on the first rib at the costo-sternal joint
In 1956, a group of diverse patients with symptoms in the shoulder, neck, and the upper extremity who presented with pain, numbness, tingling, and swelling, were placed under the umbrella of “thoracic outlet syndrome” (“TOS”) [1]. Since that publication, Thoracic Outlet Syndrome has been classified as Neurogenic, Venous (Paget Schroetter Syndrome), and Arterial varieties. In the past six decades TOS has been characterized by confusion about the actual pathophysiology of the disease, the appropriate diagnostic tests, and the appropriate therapeutic interventions [2, 3]. As a result, further subtypes have been proposed: True neurogenic TOS, Disputed Neurogenic TOS (DNTOS), Traumatic neurovascular TOS. It has been postulated that the common pathologic feature of these conditions is the compression of the brachial plexus and/ or subclavian vessels just above the first rib. Although the role of the first rib seems to be a unifying feature of TOS, the exact mechanism by which the first rib results in compression, and specifically what is compressed, has remained unclear. Furthermore, given the fact that in the absence of rarely seen cervical rib or cervical bands, anatomically the first rib is not in the vicinity of the brachial plexus, the exact role of the first rib in the majority of patients with “Neurogenic” TOS (Disputed Neurogenic TOS) has been an enigma.
Based on the comparison of the resected first ribs from patients with Venous TOS, or Paget Schroetter Syndrome (PSS) and normal first ribs, Gharagozloo et. al. proposed that an abnormal bony tubercle at the costo-sternal joint of the first rib is the pathologic entity [4]. The hypothesis was tested in 83 patients who underwent transthoracic robotic resection of the medial aspect of the rib and disarticulation of the costo-sternal joint with relief of the extrinsic compression of the subclavian vein [5,6]. Two years after robotic resection of the offending portion of the first rib and obtaining patency of the SV, all patients remained asymptomatic and had full function of the affected upper extremity. Unexpectedly, detailed preoperative assessment in these patients revealed a significant history of unrecognized upper extremity neurologic symptoms which predated the clotting of the subclavian vein and onset of Paget Schroetter Syndrome. The neurologic symptoms resolved after undergoing resection of the first rib for PSS. Therefore, it was hypothesized that in a subgroup of patients with DNTOS neurologic symptoms may be a manifestation of compression of the subclavian vein, venous congestion resulting in venous ischemia of the upper extremity nerves which lead to diffuse neurologic symptoms unrelated to nerve compression.
In order to test the above hypothesis, the present study compared the anatomic features of the first rib in normal individuals to the first ribs resected from a subgroup of patients with DNTOS who experienced postoperative symptom relief following the resection of the costo-sternal joint and the medial aspect of the first rib resection.
This study is a retrospective analysis comparing normal human cadaver first ribs (Control, C) with first ribs from a subset of patients affected with “Neurogenic” TOS (N).
First ribs from human cadavers were obtained from individuals without an ante-mortem history of upper extremity symptoms or pathology.
Neurogenic TOS was suspected in patients who had a clinical history of upper extremity, shoulder, and neck pain in whom cervical spine disease, shoulder disease, and other orthopedic conditions were ruled out. Preoperative diagnosis of DNTOS was made after all specific localizing diagnostic findings were ruled out. All patients underwent robotic transthoracic resection of the medial aspect of the first rib with disarticulation of the costo-sternal joint. Definitive diagnosis of DNTOS was made only after the patient experienced complete resolution of symptoms on postoperative follow-up. Only the rib specimens from patients who experienced complete resolution of their neurologic symptoms were included in this study.
The study included postmortem (C group) or postoperative (N group) pathologic anatomic observations, review of the preoperative and postoperative MRA, and review of video recording of the operation. For each rib, the following anatomic observation points were recorded: 1) width of the rib at the costo-sternal junction, 2) the presence of a groove for the subclavian vein, 3) the presence of a groove for the subclavian artery, and 4) the presence of tubercle at the medial aspect of the rib. The preoperative MRA study with maneuvers were examined for the presence of extrinsic compression of the subclavian vein. The area of extrinsic compression on the MRA was then correlated with the anatomic findings. The post-operative MRA study with maneuvers were examined for the presence of extrinsic compression of the subclavian vein. The relationship of the first rib to the subclavian vein was assessed at rest and with elevation of the extremity above the shoulder. The intraoperative videos from transthoracic robotic surgical resection of the first rib were examined for surgical observations in terms of the relationship of the medial aspect of the first rib to the subclavian vein. The anatomic features of the first rib in relation to the subclavian vein were recorded.
Data were exported from Excel (Microsoft Corp., Redmond, WA.). Information was obtained through hospital databases, medical records, and our prospective database. The data was prospectively accrued and retrospectively analyzed. Individual consent was waived for inclusion in this study; however, it was required and obtained to enter patient data in the prospective database. This study was reviewed institutional review board and determined to be exempt under 45 CFR 46.101 (b)
Control (C) Group: There were 12 first ribs obtained from human cadavers in the C group. There were 6 right first ribs and 6 left first ribs in the C group. The ribs in the C group had a thickness of 0.5 +/- 0.1cm at the midpoint of the rib and 1.0 +/- 0.08cm at the costo-sternal junction. All of the ribs in the C group exhibited a groove at the subclavian vein with a thickness of 0.2 +/- 0.04cm. In addition, in all ribs in the C group there was a groove at the subclavian artery with rib thickness 0.2 +/- 0.04cm.
Experimental (N) Group: There were 41 first ribs resected from patients who had the definitive postoperative diagnosis of Neurogenic TOS based on complete resolution of the preoperative neurologic symptoms. There were 29 right first ribs and 12 left first ribs in the N group. The ribs in the N group had a thickness of 0.6+/-0.1 cm at the midpoint of the rib and 1.3 +/-0.4cm at the costo-sternal junction. All of the first ribs in the N group demonstrated a bony protuberance at the site of the subclavian vein groove with a thickness of 1.4 +/- 0.1cm.
In all (100%) patients in the N group, the surgeon reported a bony tubercle just lateral to the costo-sternal joint.
Preoperative MRA with maneuvers of the ipsilateral side in all patients (100%) in the N group revealed extrinsic compression of the subclavian vein at its junction with the innominate vein by a bony protuberance on the underside of the vein. (Figure. 1)
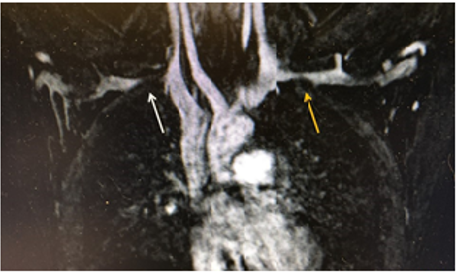
In all patients (100%), elevation of the arm above the shoulder resulted in greater compression of the subclavian vein by the bony protuberance. The postoperative MRA with maneuvers showed relief of extrinsic compression of the subclavian vein in all patients. There was no statistical difference between the C and N groups in terms of thickness of the rib at its midpoint. The thickness of the first rib at the subclavian vein groove and costo-sternal joint was significantly different between the C and N Groups (p less than 0.05).
In 1956 Peet, attempted to classify patients who presented with a variety of symptoms that affected the upper extremity, the ipsilateral neck and shoulder. Curiously, as a result of Peet’s classification which was based on symptoms rather than the underlying pathology, it was extrapolated that TOS represents a group of diverse disorders that result from compression of the neurovascular bundle exiting the thoracic outlet. Compression of this area has been thought to result in a constellation of distinct symptoms, which can include upper extremity pallor, paresthesia, weakness, muscle atrophy, pain, and swelling [8,9]. Historically, the subgroups of TOS have consisted of Neurogenic (NTOS), Venous (VTOS
or Paget Schroetter Syndrome, PSS), and Arterial (ATOS) (85). Neurogenic TOS accounts for over 95% of the cases, followed by venous (3–5%) and arterial (1–2%). (10) Neurogenic TOS (NTOS) has been further divided into True (TNTOS) and Disputed NTOS (DNTOS), with disputed reportedly representing 95–99% of all neurogenic cases [11]. The symptoms of TTOS and DNTOS are largely the same, although objective findings from nerve conduction studies and needle electromyography are notably absent in the DNTOS [12]. TNTOS most commonly affects a younger woman in their teenage years, is associated with cervical ribs or cervical bands, and is usually unilateral. Disputed NTOS is most commonly seen in women ranging from their 20s to 60s and is often bilateral [13]. One possible mechanism for the pathogenesis of a subgroup of patients with DNTOS who present with neurologic symptoms of the upper extremity who have negative nerve conduction studies and a normal neurologic exam is the subject of the present paper.
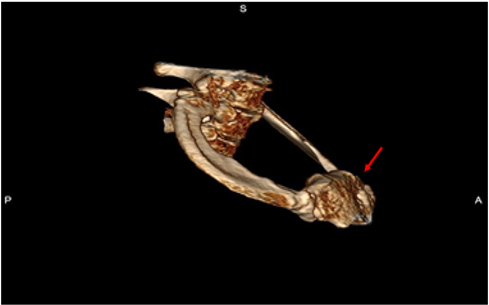
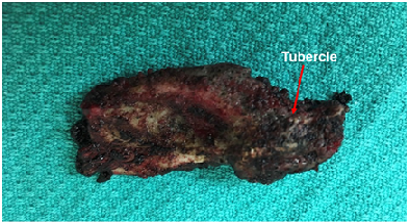
Recently, examination of the medial aspect of the resected first ribs in patients with Paget–Schroetter syndrome has demonstrated the presence of a congenitally malformed bony tubercle that forms a tighter and wider joint at the junction of the first rib and the sternum [4-6]. (Figure. 2)

It has been observed that the wider and less mobile cost-sternal joint “locks” the medial aspect of the first rib into place and results in extrinsic compression of the boney tubercle onto the subclavian vein at its junction with the innominate vein. It can be surmised that without the benefit of the sophisticated modern imaging, and relying only on intraoperative observations, it is likely that historically surgeons have erroneously referred to this tubercle as the hypertrophied costoclavicular ligament and the hypertrophied scaleneus anticus tubercle. This abnormal tubercle on the medial aspect of the first rib can be seen on 3-D reconstruction of computerized axial tomograms in patients with PSS. (Figure. 3) In addition, the extrinsic compression of the subclavian vein by the tubercle at the medial aspect of the first rib can be demonstrated on dynamic magnetic resonance angiography (MRA) with maneuvers and dynamic venography. (Figures. 4a, 4b)
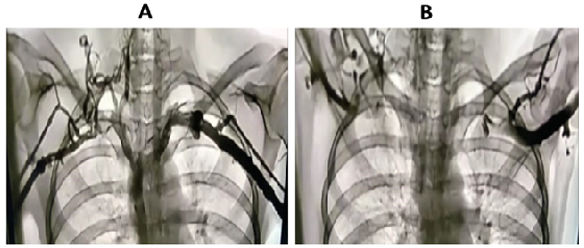
Furthermore, these studies clearly demonstrate that the subclavian vein compression increases with elevation of the arm above the shoulder. Prolonged compression stemming from activities that elevate the arm above the shoulder, result in thrombosis of the vein (PSS). As a definitive proof of the proposed pathogenesis of Paget Schroetter Syndrome, Gharagozloo et al. have demonstrated that disarticulation of the costo-sternal joint and resection of the medial aspect of the first rib results in decompression of the subclavian vein and complete resolution of symptoms [6].
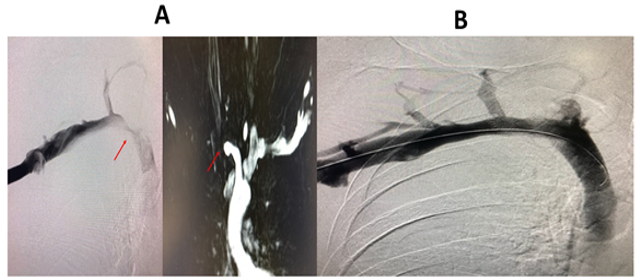
Observations in patients with a previous diagnosis of Neurogenic TOS who had persistent upper extremity neurologic symptoms following first rib resection by the transaxillary and supraclavicular approaches, revealed persistent extrinsic compression of the subclavian innominate junction on dynamic MRA. Disarticulation of the cost-sternal joint and removal of the remaining portion of the first rib, which bore a tubercle similar to that which was seen in patients with Paget Schroetter syndrome, resulted in relief of neurologic symptoms in all patients. In turn, Postoperative MRA and Venogram showed relief of extrinsic compression and decompression of the subclavian innominate junction. (Figures. 5a, 5b) This observation, in addition to the observation that patients with PSS have diffuse neurologic symptoms of the upper extremity prior to clotting of SV, led to the hypothesis that in a subgroup of patients with DNTOS, upper extremity neurologic symptoms may be due to venous compression and the resultant venous ischemia of the nerves in the upper extremity. This hypothesis is supported by the fact that the upper extremity is fed by a single artery and a single vein as an “end organ.” In such a setting, studies have demonstrated that the blood-nerve barrier in the nerve root was more easily broken by venous congestion than by arterial ischemia. Venous congestion may be an essential factor precipitating circulatory disturbance in nerve roots and inducing neurogenic intermittent claudication. This phenomenon is illustrated by the feeling of a leg “falling asleep” or pain and paresthesia which is experienced in the lower extremity after crossing the leg for a prolonged period of time. Of interest, patients with DNTOS liken their symptoms to their arms “falling asleep”.
In a proof-of-concept study, surgical outcomes in patients diagnosed with DNTOS who underwent robotic first rib resection were reviewed. Diagnosis was made by history, physical exam, MRI of C-spine, orthopedic and neurologic examination, nerve conduction studies, and MRA of the thoracic outlet with maneuvers. Patients with specific nerve compression, cervical ribs or cervical bands we excluded. Patients with compression of the subclavian vein by the medial aspect of the first rib underwent robotic resection of the first rib. Subjective symptoms were assessed by Disabilities of the Arm, Shoulder and Hand Questionnaire Score (Quick DASH), at 1 week, 1 month, and 6 months. With relief of extrinsic compression on the subclavian vein, 97% of patients with Disputed Neurogenic TOS experienced complete relief of symptoms [14, 15]. Significant relief of symptoms was reported in the remaining 3% of patients.
In this study we compared the resected ribs from patients with DNTOS who experienced complete postoperative relief of symptoms to normal ribs. In patients with Disputed Neurogenic TOS, the first rib exhibits an abnormal bony tubercle immediately lateral to the costo-sternal joint. The tubercle is found in the same location as the subclavian groove which is seen in normal first ribs. The tubercle results in a wider and tighter costo-sternal joint and traps the subclavian vein at its junction with the innominate vein. In this study, in normal individuals, the rib thickness at the subclavian groove was 0.2cm which represented an indentation of 0.8cm from the rib surface. It can be surmised that at the time of extension of the upper extremity above the shoulder and elevation of the first rib, the presence of this groove prevents compression of the subclavian vein by the rib. On the other hand, in patients with DNTOS the thickness of the first rib at the abnormal tubercle was 1.4 cm, which represents a differential elevation of 1.2 cm above the subclavian groove. Given the fact that the subclavian vein has an average diameter of approximately 1cm [16] in its position over the first rib, it can be concluded that the tubercle compresses the subclavian vein at rest, and significantly occludes the vein with extension of the arm above the shoulder.
These observations support the “ischemic” versus the “compressive” pathogenesis of a subgroup of patients with DNTOS. In these patients DNTOS appears to be the manifestation of a congenital malformation of the first rib. The congenital malformation is in the form of a pronounced tubercle, which results in an abnormal costo-sternal joint and the compression of the subclavian vein at its junction with the innominate vein. (Figure. 6) The compression of the subclavian vein in the thoracic outlet results in a spectrum of neurologic symptoms which are the result of venous ischemia of the upper extremity nerves. The ischemic pathogenesis of DNTOS is consistent with the normal neurologic exam and lack of objective evidence for nerve compression in these patients.
Magnetic Resonance Angiography clearly demonstrates the extrinsic compression at the subclavian innominate junction and can guide the decision for surgery. The most compelling evidence for ischemic pathogenesis of DNTOS is the relief of symptoms following disarticulation of the costo-sternal joint and removal of the medial aspect of the first rib.
A bony tubercle at the site of the subclavian vein groove in patients with DNTOS may be the pathologic entity which causes extrinsic compression of the subclavian vein at rest. The neurologic symptoms resolve following disarticulation and resection of the medial aspect of the first rib. In a subgroup of patients, NTOS may be the manifestation of venous ischemia of the nerves of the upper extremity as opposed to nerve compression.
None.
The author(s) declare that they have no competing interests
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
