AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Xiaolei Hu, MD, PhD, Associate Professor, Senior consultant physiatrist Department of Community Medicine and Rehabilitation Umeå University, 901 85 Umeå, Sweden
Citation: Eva Elgh and Xiaolei Hu (2023). Premorbid Employment and Education as Predictors of Recovery in General Cognition ten Years After Stroke Onset - A Longitudinal Cohort Study. J. Neuroscience and Neurological Surgery. 13(1); DOI:10.31579/2578-8868/260
Copyright: © 2023 Xiaolei Hu, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 13 February 2023 | Accepted: 28 February 2023 | Published: 06 March 2023
Keywords: cognitive improvement; cognitive reserve; education; employment; longitudinal study; stroke
Background: We have recently demonstrated significant general cognitive recovery with delayed improvement of working memory 10 years after stroke in a unique longitudinal cohort.Aim: This study investigated demographic and clinical characteristics relevant to improved cognitive functions 10-year after a first-ever stroke.
Materials and Methods: A prospective longitudinal cohort study was carried out in 38 middle-aged (mean age =54 at stroke onset) stroke survivors. Cognition was assessed thrice at one week, seven months, and ten years after the stroke. Working memory and visuospatial function were assessed with the Digit Span and Block Design subtests, respectively. General cognition was evaluated with the Mini-Mental State Examination at the two later time points. Multivariate linear regression was used to identify the variables that may significantly predict improved cognitive functions at 10-year follow-up.
Results: We found that having a full-time job prior to the stroke, suffering an ischemic (as opposed to a hemorrhagic) stroke, and having a university education predicted significantly superior general cognitive function 10 years after stroke (R2 of 0.77, p <0.001), while working memory and visuospatial function at 1 week after stroke significantly predicted their respective functions at 10-year follow-up (R2 of 0.41, p = 0.003).
Conclusions: Our results indicate that premorbid employment status and higher education as well as having suffered from an ischemic rather than a hemorrhagic stroke might predict superior cognitive recovery among middle-aged individuals 10 years after stroke.
Cognitive impairment is frequent among stroke survivors and contributes significantly to their disabilities [1, 2]. Various cognitive impairments – including in orientation, memory, abstract reasoning, visuospatial ability, verbal fluency, attention, processing speed, and language [3-5] – have been reported in both the acute [4] and chronic phase [2] after stroke. Stroke is also associated with the development of dementia [6]. A recent systematic review and meta-analysis demonstrated that greater cognitive impairment among individuals after stroke onset results in more severe limitations in their ability to complete both basic and complex activities of daily living and participate in work, social, and leisure activities [7]. These associations have been observed not only for general cognitive impairment, but also for various cognitive domains [7].
The severity of cognitive impairment and extent of recovery after stroke depend on each patient’s premorbid capacity, as well as on the characteristics of the stroke. In addition to common vascular risk factors [8, 9], a recent study has demonstrated that having obtained higher education and having an occupation are associated with less cognitive impairment and a more rapid recovery of cognitive function after stroke [10]. This is consistent with a meta-analysis that found that having fewer years of formal education was positively associated with post-stroke cognitive decline [11]. The effects of education and occupation on post-stroke cognitive improvements might be explained by the notion of cognitive reserve [12], the brain’s capacity to minimize the clinical manifestations of brain pathology [13, 14].
The results of studies on the effect of stroke subtype on post-stroke cognitive impairment have been inconsistent [15, 16]. A study that included 2847 patients showed that cognitive impairments are more common after lacunar infarct [17] and that a similar proportion of patients with lacunar and non-lacunar stroke have mild cognitive impairment or dementia up to four years after stroke [18]. Further, a recent Nor-COAST study demonstrated that cognitive impairments are common in all stroke subtypes, with impairment of attention being dominant among the subgroup of individuals with large artery disease and cardioembolic stroke [15]. Hemorrhagic strokes are less common than ischemic strokes and are associated with high mortality [19], which may explain the scarcity of cognitive data from hemorrhagic stroke patients.
We have recently demonstrated significant general cognitive recovery with delayed improvement of working memory 10 years after stroke in a unique longitudinal cohort comprising 38 middle-aged individuals (aged 18–65 at stroke onset) [20, 21]. Visuospatial function recovered earlier than working memory, with evidence of recovery already observed at 7 months, and remained stable at 10-year follow-up. Language disorder, as assessed with D-KEFS-FAS, showed no significant alteration over the 10-year follow-up [20]. However, such very long-term follow-up studies are rare, and alterations in cognitive impairment after stroke remain overlooked [2]. Our data on improvement in working memory among persons with stroke is consistent with the recent Nor-COAST study [15], which demonstrated improvements in working memory among both middle-aged and elderly stroke patients despite the fact that age-related decline in working memory has been well demonstrated [22]. Interestingly, a higher level of education and having an occupation were associated with more cognitive recovery after stroke in a KOSCO study [10]. Together with other studies, the results of our previous study [20, 21] suggested that full long-term cognitive recovery is possible in individuals after stroke. To our knowledge, no organized cognitive rehabilitation was provided after the initial hospitalization in the current cohort; thus, participants’ struggle to be active and/or live independently in their daily lives may be a crucial element in their cognitive improvements. This is reason why we hypothesize various demographic and clinical characteristics in this unique cohort may play some roles in the cognitive improvements.
The current study aimed to investigate which demographic and clinical characteristics are important for cognitive recoveries in middle-aged first-ever stroke survivors. Based on the results of previous studies, the null hypotheses were that length of education, employment status before and after stroke, stroke subtype, and demographic data would have no predictive value on cognitive improvements at 10-year follow-up in this cohort.
Materials and Methods
Study design
This single-center study was a prospective, longitudinal cohort study of stroke survivors with three consecutive follow-ups over a 10-year period after a first-ever stroke. The cognitive functions of stroke survivors were assessed prospectively at 10-year follow-up, then compared retrospectively with data collected one week and seven months after the time of stroke.
Ethical approval was obtained from the regional Ethical Review Board in Umeå, Sweden, D-nr 2015/144-31.
Recruitment and participants
The study was conducted at the Department of Neuro-Rehabilitation, University Hospital of Umeå. All middle-aged patients (18 to 65 years of age at the time of stroke) who had suffered a first-ever stroke between January 2004 and December 2007 and undergone neuropsychological assessments (NPA) at one- and 7-month after stroke. These data were collected from the medical journal. Only 10-year assessments were carried out prospectively. The participants were informed about the study and provided with written consent forms via letter, and research staff made contact with all eligible patients via telephone to improve the recruitment rate. Patients with severe dementia, severe aphasia, severe comorbidity, recurrence of stroke or transient ischemic attack, or other physical or psychiatric disease after first-ever stroke, along with those who were not community dwelling adults, were excluded [20]. After a thorough recruitment process taking place from 2015 to 2016, 49 of the total 102 middle-aged first-ever stroke patients with acute NPAs declined to participate and 15 others were excluded for a variety of reasons (Figure 1). Thus, our study included 38 stroke survivors with previous NPAs, all of whom provided their written, informed consent to participate in the 10-year follow-up. All were native Swedish citizens.
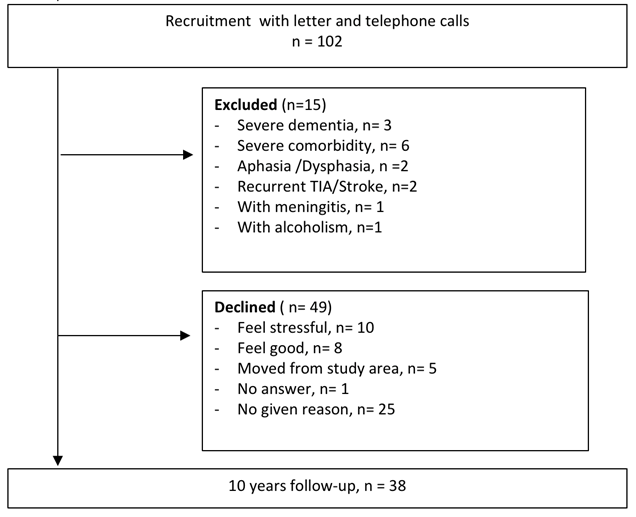
Figure 1: Flowchart showing inclusion process
Basic demographic and clinical characteristics
Baseline data were collected from the Riksstroke registry and patients’ medical records. The clinical data, premorbid education level, and employment, as well as patients’ status of fatigue, depression, and anxiety, were prospectively collected using various questionnaires one month prior to the scheduled appointment for NPAs at 10-year follow-up. Premorbid education level was collected, and higher education was predefined as more than or equal to 12 years of education and lower education was defined as less than or between 9 and 12 years of education. Employment status prior to stroke and at one year and ten years after stroke was also collected [20] (Figure 2). The questionnaires used in the study are described in detail below.
The Fatigue Assessment Scale (FAS) is a self-report questionnaire used to identify symptoms of chronic fatigue [23] affecting a patient’s daily activity. It consists of 10 questions addressing both physical and mental problems associated with fatigue and has a maximum score of 50 points, with higher scores indicating greater degrees of fatigue. The cutoff for post-stroke fatigue was set at 24 points [24]: scores of 24 and higher indicated that the patient had fatigue.
Depression was assessed with the Beck Depression Inventory-II (BDI-II) [25], a self-rating scale that measures depression in adults and adolescents. The test contains 21 questions, each of which is answered with a single score on a 0–3 scale. Higher total scores indicate more severe depressive symptoms. The standardized cutoffs of the BDI-II are ≤13 for minimal depression, 14–19 for mild depression, 20–28 for moderate depression, and 29–63 for severe depression.
Anxiety was assessed with the Beck Anxiety Inventory (BAI) [26], a 21-item multiple-choice self-report assessment. Each answer is given as a score describing how much the patient has suffered from a particular symptom, with the scale ranging from 0 (not at all) to 3 (severely). Higher total scores indicate more severe anxiety symptoms. The standardized cutoffs are ≤7 for minimal anxiety, 8–15 for mild anxiety, 16–25 for moderate anxiety, and 26–63 for severe anxiety.
The simplified modified Rankin Scale questionnaire (mRS) is a standardized, practical, and validated questionnaire for the reliable assessment of a person’s functional and disability status [27, 28]. The assessed patient answers five questions with either ‘yes’ or ‘no’; by following their answers on the associated decision tree–like flowchart, a value on a scale from 0 (no symptoms) to 5 (total physical dependence) is arrived at. Scores of 2 or less are considered to indicate total independence [28].
Cognitive function assessments
To assess general cognitive functioning, the Mini-Mental State Examination (MMSE) was carried out for each patient immediately prior to administering the NPA. The MMSE was used at the 7-month post-stroke assessment as a clinical routine more than 10 years prior to the current study (Figure 2). Although it has limitations [29] and the total score of the Wechsler Adult Intelligence Scale (WAIS) can be used as a global cognitive composite score, we chose to use the MMSE because it is considered the gold standard for assessment of global cognitive function.
Domain-specific cognition was assessed by NPA thrice, at one week, seven months, and ten years after stroke (Figure 2). NPA data collected at one week and seven months after stroke onset were retrospectively gathered from the medical records. Working memory and visuospatial function were assessed with the Digit Span and Block Design subtests from the WAIS, respectively. The reasons for the initial NPA at the earlier time points were unknown to us. However, the assessments were performed for clinical reasons and may have been determined by the patients’ ability to be assessed and access to a psychologist at that time. NPAs were often carried out within one week after stroke debut. Some of the participants were assessed again at approximately 7 months (IQR 2–10) after stroke. Four assessors who were blinded to the results of the assessments that had been performed 10 years ago were involved in the study. The full test battery took approximately 2–3 hours, with a 30-minute break and refreshments in the middle of the assessment. To ensure comparability, the tests administered at the 10-year follow-up were selected based on the tests that had been used at the initial assessment in the year of the stroke. It should be noted that the revised WAIS (WAIS-R) and WAIS-III were replaced by the WAIS-IV at the 10-year follow-up. This is because the previous version of WAIS was no longer available to us. Previous validation studies have shown that the WAIS-IV follows the same structure as both the WAIS-III and WAIS-R [30], with a very high correlation between subscales (r = .82–94) [31]. Swedish norms for the WAIS-IV were used as a control [31].
Changes in cognitive functions over the 10 years after a stroke have previously been presented in detail [20]. The following cognitive domains that were found to show significant improvement in our previous study were selected for analysis in the current study: visuospatial function (as measured by the Block Design subtest of the WAIS), working memory (measured using the Digit Span subtest of the WAIS), and general cognitive functioning (measured via the MMSE). 
Figure 2: Study design and process. Data from neuropsychological assessment (NPA) and Mini-Mental State Examination (MMSE) at approximately 1 week and 7 months after stroke onset were retrospectively collected from the patients' medical records. The clinical data, premorbid education level, and employment, as well as patients’ status of fatigue, depression, and anxiety, were prospectively collected using various questionnaires one month prior to the scheduled appointment for MMSE and NPA at 10-year follow-up.
Data presentation and statistical analysis
Demographic characteristics and NPA data are presented as mean (SD), number and percentage of cases (%), range, or median (25%–75% interquartile ranges [IQR]), as appropriate. No adjustment was made for missing values. A mixed linear model was used as a hierarchical linear model in SPSS to analyze the cognitive differences over time. Each p-value in the post hoc analyses was adjusted to account for multiple comparisons with Bonferroni correction.
Multivariate linear regression with a stepwise method was used to investigate whether the length of education, employment status before and after stroke, stroke subtype, demographic data, and clinical variables could significantly predict improvement in the three cognitive functions assessed at 10-year follow-up: general cognitive functioning, visuospatial function, and working memory. The independent variables included in the model were age, gender, residential status (i.e., whether an individual lived alone), premorbid education, employment prior to stroke onset, employment at one year and ten years after stroke, stroke subtype, functional status, general cognitive functioning at one-week follow-up, visuospatial function at one-week follow-up, and working memory at one-week follow-up. Employment was coded as 1 = full-time job, 2 = part-time job, 3 = sick leave, and 4 = retired; stroke subtype was coded as 1 = ischemic stroke and 2 = hemorrhagic stroke; and length of education was coded as 1 = 9 years, 2 = 12 years, and 3 = >12 years.
Values for tolerance and variance inflation factor (VIF) were calculated to assess the presence of collinearity. Standardized coefficients were used to determine the strength of each independent variable’s correlation with improved cognitive function. R2 was examined to determine how much variation in the cognitive functions could be explained by the modeled variables. Linearity and homoscedasticity were examined with Fred’s super scatterplot. Independence of errors was tested with the Durbin–Watson test. Normal distribution of the data was assessed with a normal P–P plot.
The software package IBM Statistical Package for the Social Sciences (SPSS) Statistics version 28.0 (SPSS, Chicago, IL, USA) was used to perform the multivariate linear regressions. Figure 2 was generated using GraphPad Prism 9 (San Diego, CA, USA). P-values < 0>
Basic demographic and clinical characteristics
Table 1 presents the baseline demographic and clinical characteristics of the 38 participants. The participants’ mean age was 53.9 years (SD 9.1) at stroke onset. All participants were living in the community, and nearly half (n = 18, 47%) had more than 12 years of education. The dominant stroke subtype was ischemia (79%). At 10-year follow-up, participants’ mean age was 63.8 years (SD 10.6). Participants exhibited good independence in daily activities at this time, with a median score of 1 on the mRS.
Employment status was collected at three time points. Thirty-three (87%) participants had a full-time or part-time job prior to stroke onset. One year after stroke, 16 (43%) participants had returned to either full-time or part-time work. Almost one third of the participants were employed full- or part-time; another two third were either retired or unemployed. Fatigue was a prevalent problem 10 years after the time of stroke: nearly three-quarters of the participants suffered from fatigue (FAS ≥ 24), with a median score of 25 and a 25%–75% IQR of 21–27. Fewer than one-third of the participants (n = 12) were depressed (BDI-II score > 13), but the median score was 9, with a 25%–75% IQR of 4–14 for the entire group. Approximately one-third (n = 13) had anxiety (BAI score > 8); however, the group’s median score of 6 (25%–75% IQR of 2–11) was relatively low. Although information on fatigue, depression, and anxiety was collected at the 10-year follow-up, it provided no predictive value on cognitive function recovery.
| Patient Characteristics at stroke onset (n = 38) | |
| Age [mean (SD)] | 54.2 (10.1) |
| Number of patients (age <30> | 3 |
| Number of patients (age between 30-60) | 11 |
| Number of patients (age >60) | 24 |
| Gender (Men/Women) | 19/19 |
| Residential status (live alone/live with somebody/unknown) | 7/30/1 |
| Stroke subtype (Ischemia/Hemorrhage/Unknown) | 30 /6/2 |
| Education [number of cases (%)] | |
| Lower education (9–12 years) | 19 (50%) |
| Higher education (> 12 years) | 18 (47%) |
| Unknown | 1 (3%) |
| Employment [number of cases (%)] | |
| Full-time job | 29 (76%) |
| Part-time job | 4 (11%) |
| Retired/Unemployed | 5 (13%) |
Employment at 1 year after stroke [number of cases (%)] | |
| Full-time job | 12 (32%) |
| Part-time job | 4 (11%) |
| Retired/Unemployed | 18 (47%) |
| Unknown | 4 (11%) |
| Characteristics at 10-year follow-up | |
| Age [mean (SD)] | 63.8 (10.6) |
| Years between stroke onset and follow-up [mean (SD)] | 10.5 (0.9) |
| mRS [Median (25%-75% IQR)] | 1 (0-2) |
Fatigue assessment score [Median (25%-75% IQR)] | 25 (21-27) |
| BDI-II [Median (25%-75% IQR)] | 9 (4-14) |
| BAI [Median (25%-75% IQR)] | 6 (2-11) |
| Employment [number of cases (%)] | |
| Full-time job | 4 (11%) |
| Part-time job | 6 (16%) |
| Retired/Unemployed | 27 (71%) |
| Unknown | 1 (3%) |
Abbreviations: standard deviation (SD); modified Rankin Scale (mRS); interquartile range (IQR); Beck Depression Inventory-II (BDI-II); Beck Anxiety Inventory (BAI)
Table 1: Demographic and clinical characteristics of all participants
Improved cognition
Mean (SD), range, or median (25%–75% IQR) are provided (Table 2) to present the detailed raw data on the cognitive improvements; notably, these cognitive improvements were previously reported in a 2019 study by Elgh and Hu [20]. At 10-year follow-up, the entire group collectively demonstrated a weak but significant improvement in general cognitive functioning as assessed by MMSE compared to the results at 7-month follow-up (from 27 to 29 points, p = 0.02). No significant difference was observed when comparing the MMSE scores between the subgroup with a higher independence level (mRS 0–1) and the subgroup with a lower independence level (mRS 2–3).
Median visuospatial function at both 7 months post-stroke and the 10-year follow-up (Table 2) was significantly improved compared to the results at 1 week after stroke (p = 0.001 and p = 0.007, respectively). However, there was no significant difference between visuospatial function at 7 months and at 10 years after stroke. A median total Digit Span raw score of 17 (25%–75% IQR of 14–19) signaled significant improvements in working memory at 10-year follow-up in comparison with the results at 1 week and 7 months post-stroke (p < 0.0001). There were no significant differences in cognitive processing speed or executive function between the follow-up time points.
Domain
| Assessment
| 1 week after stroke Raw score Mean (SD) Range Median (25%-75% IQR) N | 7 months after stroke Raw score Mean (SD) Range Median (25%-75%IQR) N | 10 years after stroke Raw score Mean (SD) Range Median (25%-75%IQR) N |
| General cognitive functioning | MMSE | - | 27 (3) 11 27 (25-29) 27 | 28 (2) 8 29 (27-30) † 38 |
| Visuospatial function | WAIS-Block Design | 25 (12) 40 27 (15-35) 27 | 41 (12) 48 39 (34-51) * 19 | 36 (12) 53 36 (29-48)* 38 |
| Working memory | WAIS-Digit Span (F + B) | 12 (4) 19 12 (11-14) 29 | 15 (5) 18 13 (11-18) 26 | 16 (3) 13 17 (14-19)*† 38 |
* Indicates significant difference vs. the data at 1 week after stroke. † Indicates significant difference vs. the data at 7 months after stroke. SD: standard deviation; IQR: interquartile range; MMSE: Mini-Mental State Examination; WAIS: Wechsler Adult Intelligence Scale; F: Forward; B: Backward.
Table 2:Scores of neuropsychological assessments over 10-year follow-up after stroke onset
Predictors of cognitive functional recovery
Most of the variables, including age, gender, residential status, employment after stroke, and functional status (mRS score), did not demonstrate any significant predictive value for cognitive recovery.
However, employment prior to stroke, stroke subtype, and length of premorbid education were significant predictors of general cognition, as assessed by MMSE, at 10-year follow-up. A significant regression equation was found [F(3,15) = 16.95, p <0 F(1,17) = 11.64, >p = 0.003], with an R2 of 0.41. Participants’ predicted working memory at 10-year follow-up was equal to 9.14 + 0.55*x (“x” refer to the score on the Digit Span test at 1 week after stroke) – that is, participants’ working memory at 10-year follow-up was 0.55 raw scores higher for each Digit Span score received at 1 week after stroke (Table 3B).
Visuospatial function (WAIS-Block Design) at 1 week after stroke was a significant predictor of visuospatial function 10 years after stroke. A significant regression equation was found [F(1,15) = 19.12, p < 0.001], with an R2 of 0.56. Participants’ predicted visuospatial function at 10-year follow-up was equal to 19.12 + 0.66 *y (“y” refer to the score on WAIS-Block Design test at 1 week after stroke) – that is, participants’ visuospatial function at 10-year follow-up was 0.66 raw scores higher for each Block Design score received at 1 week after stroke (Table 3C).

Table 3: Results of multiple linear regression
In the current study, we evaluated whether years of education, employment status before and after stroke, stroke subtype, and various demographic characteristics had any correlation with cognitive recoveries among 38 middle-aged stroke survivors whose cognitive functions had improved 10 years after stroke onset. The primary finding in the current study was that having a full-time job prior to stroke, having an ischemic (as opposed to hemorrhagic) stroke, and having ≥ 12 years of education predicted significantly superior general cognitive function 10 years after a stroke. In addition, working memory and visuospatial function at 1 week after stroke were significantly correlated with their respective functions at 10 years after stroke.
Premorbid employment status was found to be the strongest predictor for better general cognitive recovery, with an MMSE score 1.09 higher for participants with a job before stroke onset in the current study. This is consistent with a recent finding in the KOSCO study, in which occupation was demonstrated to be one of the important buffers against cognitive impairment and found to promote rapid cognitive recovery after stroke [10]. Meanwhile, the participants had good independence in their daily lives based on the lower mRS score demonstrated at 10-year follow-up in the study. However, this late higher independence in daily life was not statistically significantly correlated with the improvement in general
cognition in this cohort. These current data suggest that having a job prior to stroke may provide a more advanced challenge in daily life that enhances neuroplasticity and cognitive reserve, which has been
demonstrated in individuals with Alzheimer’s disease [32, 33]. However, employment status 1 and 10 years after stroke onset did not show any predictive value on the improvement in general cognition in this cohort. This may partly be explained by the fact that we collected only employment status (full-time/part-time/no job) without collecting details on the level/complexity of the job, as well as the small sample size in the current study [10]. Nonetheless, our data suggest that having a job prior to stroke is beneficial for general cognitive recovery after stroke.
Having received more than 12 years of education prior to stroke was another significant predictor of general cognitive improvement, which is consistent with our finding that the mean MMSE score among the participants who received exactly 9 years of education was significantly lower than the score for participants with university education. This outcome is in line with recent findings that high levels of education, as a protective factor against cognitive decline, also promote rapid cognitive recovery after stroke [10, 34]. The effects of education on cognitive improvements after stroke might be explained by the concept of cognitive reserve [12-14], which is defined as the cumulative brain capacity to mitigate cognitive decline due to various brain pathologies, such as stroke, aging, or age-related disease [14, 35]. It is believed that superior cognitive capacity among more highly educated individuals may confer more complex architecture of neuronal networks and an enhanced ability to effectively recruit these networks [14]. This, in turn, may produce better preconditions for activity-derived neuroplasticity after the brain has been damaged, such as in the case of a stroke. Meanwhile, higher education is also associated with better lifestyle choices, better socioeconomic status, less stress, etc., which may influence cognitive function [36]. Consistent with our finding is the association between low education and higher prevalence of cognitive impairment and the development of dementia after a stroke [1, 37]. Thus, together with premorbid employment, premorbid education appears to be one of the best preventive measures for preserving cognitive function in persons with stroke [9, 11, 38]. Moreover, the results of the present study suggest that higher levels of education might be important for cognitive recovery after stroke.
In this cohort, having an ischemic (as opposed to a hemorrhagic) stroke predicted better improvements in general cognition. This is substantiated by findings that hemorrhagic stroke is more strongly associated with cognitive impairment and the development of dementia [16, 39, 40]; however, this was not observed in all studies [15]. However, it remains largely unknown why ischemic and not hemorrhagic stroke is associated with superior general cognitive function. One possible explanation is that hemorrhage may lead to more diffused damage due to widespread intracranial pressure effects and underlying cerebral amyloid angiopathy [16, 39]. It has also been suggested that the difference is attributable to persistent (continuous) underlying cognitive impairment that is induced by the hemorrhagic stroke itself [16].
However, these significant predictors for general cognitive recovery did not predict the improvements in working memory and visuospatial function at 10-year follow-up. Instead, working memory and visuospatial function at 1 week after stroke significantly predicted their respective functions at 10 years after stroke. The reason for these discrepancies in the predictors for general cognitive function and domain-specific functions remains largely unknown. However, it is not difficult to understand why domain-specific functions at the acute stage after stroke may be associated with their respective functions at the chronic stage [41].
This study has several unique strengths. Cognition was assessed at the acute, sub-acute, and chronic phases over a 10-year period after stroke onset, which allowed us to investigate the long-term trajectory of cognitive alterations over the decade after stroke. Moreover, both general and domain-specific outcomes were assessed in this cohort. Although most of the sociodemographic variables, including age, gender, and residential status, did not show any predictive effect on cognitive improvement in the study, our data provide a distinct opportunity to enhance our understanding of the mechanisms of cognitive recovery after stroke.
Our study has some methodological biases, the first of which is that stroke location and stroke severity at onset – factors that can affect the degree of cognitive impairment [42] – were not collected in the study. Another challenge is that different versions of the WAIS cognitive battery were used: at the time of first assessment, participants were tested with the WAIS-III, whereas WAIS-IV was used at the 10-year mark due to the loss of access to WAIS-III. Though studies have shown that the two versions are closely correlated and measure the same constructs, the possibility that the difference in tests could have affected the results should not be discounted. An additional limitation concerns the length and nature of the study, which was longitudinal and took place over a full decade. One of the major methodological problems affecting longitudinal studies is attrition, which can deteriorate the generalizability of findings if participants who stay in a study differ meaningfully from those who drop out. Of the 102 middle-aged first-ever stroke patients with acute NPAs who were recruited for the study, only 38 were both qualified and willing to participate in the 10-year follow-up. We recognize that these 38 participants are not fully representative of patients in the literature on long-term cognitive recovery post-stroke [1-4]. The results are therefore not generalizable to the entire population of middle-aged stroke survivors; moreover, the small sample size confers limited statistical power. Nonetheless, our results demonstrated that premorbid employment and higher education may have played important roles in the patients who were able to ameliorate their post-stroke cognitive dysfunctions, although the mechanisms governing these recoveries are not yet fully understood.
We found that having a job prior to stroke, suffering from an ischemic rather than a hemorrhagic stroke, and having obtained higher levels of education were strong predictors of high levels of general cognitive functioning 10 years after stroke onset among 38 middle-aged individuals. Our data provided some hypotheses; namely, that premorbid employment and higher education as well as having an ischemic stroke might be crucial for post-stroke cognitive recovery. A large-scale study is necessary to confirm the veracity and generalizability of these findings.
The authors would like to thank each participant and assessor for their patience and time. We also wish to acknowledge rehabilitation coordinator Catharina Elback for her excellent recruitment work.
This study was supported by the Västerbotten County Council and Umeå University (ALF Foundation), the Swedish Stroke Foundation (Stroke a förbundet), and the Northern Swedish Stroke Fund (Strokeforskning i Norrland Insamlingsstiftelse).
The authors report there are no competing interests to declare.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
