AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals, Department of Pharmacy. University of Karachi, Pakistan.
Citation: Rehan Haider, (2023), Peripheral Vascular Disease, Cardiology Research and Reports, 5(4); DOI:10.31579/2692-9759/104
Copyright: © 2023, Rehan Haider. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 July 2023 | Accepted: 02 August 2023 | Published: 14 August 2023
Keywords: peripheral arterial disease; atherosclerosis; vascular surgery; ankle-brachial index
Peripheral vascular disease comprises diseases of the arteries and veins outside the thoracic region.: peripheral arterial disease (PAD), carotid artery disease (CAD), and aortic aneurysmatic disorder (AAA). Other rare manifestations of atherosclerotic disorders (e.g., renovascular high blood pressure, abdominal angina, and ischemia of the top extremity) were briefly noted. Special concerns in patients with diabetes are addressed in relevant sections; for instance, infection in an ischemic foot in an affected person with diabetes is described within the phase of critical limb ischemia. Atherosclerosis is the primary cause of peripheral arterial vascular ailments. It is vital to appreciate that the pathogenic mechanisms of clinical atherosclerosis are dual: chronic obstruction and biotic. The chronic obstructive mechanism is the primary purpose of lower limb ischemia, and in patients with diabetes, it is far more regularly preceded by a thrombotic occasion. An affected person with moderate clay diction abruptly studies significantly shortening of walking distance or surprising onset of rest ache. Alternatively, the seemingly wholesome character develops claudication. A coronary period heart attack or stroke in an affected person with claudication is also a thrombotic event in a patient with chronic obstructive disorder. In general, patients with diabetes greater frequently develop symptoms of atherosclerotic headaches, they do it at a younger age and it may be greater difficult to treat and feature greater headaches with treatment (in particular with invasive treatment.
Peripheral arterial disease
Peripheral arterial disease is a persistent condition that, like atherosclerosis in other vascular beds, develops over a long benefit. The International Health Enterprise (WHO) definition consists of exercising-related pain and/or an ankle-brachial index (ABI) < 0>
PAD is traditionally divided into four ranges (Fontaine).
Occurrence
In most current population-based studies in Western Europe, the occurrence of symptomatic PAD is three – 4% among 60 - 65 -year-old, increasing to 15 – 20% in individuals eighty-five – 90 years [1 – 3]. Comparable findings have been reported in the United States. When looking at asymptomatic instances where the ABI is < zero>
Pathophysiology
It is outside the scope of this chapter to describe the pathophysiology of PAD however, in brief, the pathophysiology of PAD in patients with diabetes is similar to that in the non-diabetic population. The abnormal metabolic state that accompanies diabetes directly contributes to the development of atherosclerosis. Pro atherogenic changes include increases in vascular inflammation and alterations in multiple cell types. Both mechanisms of atherosclerotic complications are of importance in PAD (gradual narrowing resulting in stenosis and an acute form of existing atherosclerotic lesions). The long-term accumulation of lipids in the vessel wall is important and sudden Local thrombosis can occur at any time, although in most cases, it occurs after the development of symptoms (claudication). To reach the stage of critical limb-threatening ischemia, advanced atherosclerosis has developed. Multiple segments of the arterial tree from the aorta to the foot are often affected (stenotic and/or occluded). Other sclerotic lesions are more peripherally located in people with diabetes than in people without diabetes. While the iliac and femoral arteries are most commonly stenotic and/or occluded in individuals without diabetes, in those with diabetes, the crural arteries are most often severely affected by atherosclerosis. This poses a challenge for revascularization because the results in general are better the more proximal reconstruction. To develop ischemic non-healing ulcers, perfusion has to be very poor. Pressure measurement is the most reliable method for assessing peripheral perfusion in patients with diabetes. A toe pressure below 20 – 25 mmHg signals a poor Possibility of healing a peripherally located ulcer. Special considerations related to the potentially dramatic course of infection in diabetic foot are addressed.
Asymptomatic stage
The asymptomatic level of PAD is mainly interesting because it is associated with approximately threefold improved mortality compared to matched controls [7,8]. This extra mortality is the result of an accompanying cardiovascular disorder (CVD). Asymptomatic PAD may be identified via a completely simple take-look at the measurement of ankle blood pressure. This check takes only a few minutes and is expressed as the ABI, in which ankle stress is divided using the highest of the two arms BP (BPs). In this way, variations in BP between measurements do not influence the test result. now not only is an ABI < 0>
Claudication
Claudication is experienced by the patient as pain in the lower limb muscles appearing after walking, most often in the calf and thigh, and more rarely in the buttocks. The walking distance that elicits the pain is very variable, beginning after 10 – 15 m in severe cases, whereas other patients will report pain only when walking fast uphill for more than 500 m. It is important for both the patient and the treating physician to understand that claudication, although it may be incapacitating for a few and troublesome for many, signals severe vascular disease systemically, and cardiovascular morbidity and mortality are high (elevated 3 – 4 times compared to matched controls).
Rest pain
Rest pain generally starts off evolving at night when the patient is in a horizontal position. The superb effect of gravity on the lower limb, consistent with fusion, was abolished. The affected person typically complains of pain in the ft or toes for the duration of the night and the maximum experiences that standing or sitting up relieves the ache. Many patients sleep while sitting on a chair. In patients with diabetes, symptomatology may additionally vary because of coincidental peripheral neuropathy. much like myocardial ischemia may be masked, signs and symptoms from the lower extremity can be missing even though peripheral ischemia exists. that is in particular critical whilst an affected person with diabetes presents with a small ulcer or wound on the lower limb, although the affected person thinks there is a great reason for growing the ulcer, which includes an applicable trauma. the lack of signs to signal peripheral ischemia combined with the risk of escalating infection in a diabetic foot has brought about many Diabetologist to endorse the habitual assessment of peripheral movement at everyday durations in anyone with diabetes.
Non-healing ulcers
Non-healing ulcers often begin after minor trauma (e.g., hitting the toe against a chair or using shoes that are too small). In some cases, the ulcers develop without any trauma and those will often progress to gangrene if not treated. Ischemic ulcers develop on or on the foot, typically at points where shoes are in firm contact. Thus, they are usually easy to discriminate from venous ulcers located at the level of the ankles or lower calf. Rest pain, non-healing ulcers, and/or gangrene are often referred to as critical ischemia.
Diagnosis
Most often the history and objective findings will ensure the diagnosis, but measurement of ankle blood pressure will quantify the ischemia and can be used to monitor changes in the disease. In some patients with diabetes, the media of the smaller arteries becomes calcified, making them compressible. Thus, very high ankle pressures resulting in elevated ABI (> 1.3) signals media sclerosis and should be recognized as a falsely elevated measurement. ABI > 1.3 is associated with a marked increase in mortality because media sclerosis is found in patients with diabetes and those with renal failure. Because small arteries are rarely affected by media sclerosis, the measurement of pressure is an alternative for the assessment of PAD. The strain gauge technique was the most commonly used. Pressure is also useful in predicting the healing of ulcers and amputation wounds.
Prognosis
The risk of amputation is only 1 – 2% at 5 years.25% of patients with claudication will experience worsening of their symptoms in the lower legs; however, 75% will remain unchanged or improve without revascularization [9]. In contrast, " systemic " risk is huge. Mortality in 5 years will be 15 – 25%, and many more patients will have non-fatal myocardial infarction (MI) or stroke. The risk of a patient with diabetes and PAD is much higher than that of an average patient with PAD. Patients with diabetes have an 8 times greater risk of amputation at the level of the trans metatarsal bones or above than the non-diabetic population [10]. In addition to the already severely increased mortality of PAD, patients who additionally have diabetes have a further doubling of their risk of death [10 – 12].
Treatment
Therefore, the treatment of patients with lower limb symptoms involves two aspects:
The former includes lifestyle modification, medical therapy, and interventional therapy by either percutaneous trans luminal angioplasty (PTA) or open surgery, whereas the latter includes lifestyle modification and preventive medical therapy. It is beyond the scope of this chapter to detail all aspects of lifestyle modification and preventive medical therapy; however, the reader needs to understand that patients with PAD derive as much or greater benefit from lifestyle modification and aggressive preventive medical therapy as any other group of patients (see Chapter 40). Most lifestyle changes that are beneficial to patients with diabetes will benefit the PAD aspect as well, especially smoking cessation, regular exercise, weight loss, and dietary changes. Medical prevention follows the same guidelines as that of other clinical atherosclerotic manifestations, such as ischemic heart disease, and can be summarized as follows: aggressive statin treatment meant almost irrespective of cholesterol levels (Heart Protection Study and American Heart Association guidelines), antiplatelet therapy, and BP control. In this chapter, only details of lifestyle modification and medical therapy relevant to PTA and surgery are discussed.
Treatment of symptoms from the lower l limb
The vast majority of patients should be managed without invasive PTA (and/or surgery). Because the risk of cardiovascular complications (cardiac and cerebral) is much higher than that of amputation, the main focus should be on preventive measures to halt the atherosclerotic process. A conservative approach concerning revascularization is especially important for patients with diabetes because of the increased risk of surgical complications and poorer results of revascularization. One exception was patients with critical limb ischemia. Early revascularization before widespread infection can be considered limb-saving. Exercise therapy has proven effective for improving walking distance, and regular exercise for 3 months can be expected to improve walking distance by 200 – 250% [13]. Because exercise also reduces cardiovascular morbidity and mortality, it cannot be stressed enough (for both the patient and physician) that this is extremely important. Because the effect on walking distance is very good and because it is important for survival, exercise therapy should always be tried before considering interventional treatment. There are only a few exceptions in which interventional treatment may be considered early.
Patients with very short walking distance, not able to carry out important daily responsibilities such as their work; and Two Patients at risk of amputation (rest pain and non-healing ulcers). The dilemma of explaining to patients that the symptoms they experience from the lower limb signal high cardiovascular risk rather than lower limb risk is challenging. First of all, there is (or has been) a general perception that atherosclerosis in the limb is less dangerous than in other locations. The author hopes that the introductory remarks in this chapter have changed potential misperception of the reader. Medical therapies for claudication include cilostazol and statins. Treatment with both may be expected to improve walking distance by 30 – 50% and the latter further reduces cardiovascular risk. Other drugs have not proven useful in significantly improving walking distance [14].
Interventional treatment
Interventional remedies (endovascular or open surgical treatment) for PAD are as follows:
• Exercise and other ways of life modification have failed to enhance signs in an appropriate country.
• Claudication is incapacitating or limb ischemia is present (rest ache, non-restoration ulcers, and/or gangrene). Again, for patients with diabetes, the indication for revascularization must be considered very cautiously in the sufferer's best with claudication. The choice between PTA and open surgical control depends on the location and extent of the disease. In fashionable, endovascular treatment can be anticipated to perform well in cases of shorter lesions, whereas open surgery is preferred in cases of good-sized occlusive sickness. Obviously, on every occasion comparable effect can be achieved, PTA is preferred because it is much less invasive and is associated with fewer complications than open arterial reconstructions. In sufferers with extreme comorbidity that might complicate the final results of open surgical treatment, PTA would be desired even though theoretical surgical treatment could be the treatment of desire if the simplest potency of the revascularization of the technique is taken into consideration.
The arterial lesions obstructing blood supply to the lower limb are most often located in the distal stomach aorta simply proximally to the aorta–iliac bifurcation, within the iliac arteries, in the common and superficial femoral arteries, respectively. The arteries in the calf, anterior and posterior tibial arteries, and perineal artery are regularly involved in people with important ischemia and diabetes. In popular, whilst sufferers with diabetes gift with symptoms, they have got an extra distal involvement with open vessels to the level of the popliteal artery and then the occlusive disease of calf vessels and, occasionally, arteries in the foot. The outcomes of revascularization for patients with diabetes with toe or foot ulcers are worse than those of the general population, partially because reconstructions yield higher consequences with recognition of potency, while the lesions are more centrally positioned. Percutaneous t trans luminal an angioplasty In principle, PTA can be performed anywhere between the heart and feet. The more centrally located the lesions being treated, the better the results, particularly with PTA. Also, the shorter the stenosis or occlusion, the better the results, and stenting improves potency in most cases. Endo-vascular-treated common iliac arteries, for example, remain patent in 60 – 80% of cases after 5 years, and thereafter they may be reinstated. Primary stenting is the preferred treatment in most cases. Because complications are rare and this procedure is associated with the best results, the tendency to offer PTA for iliac artery obstruction is greater than that for occlusive disease more peripherally located.
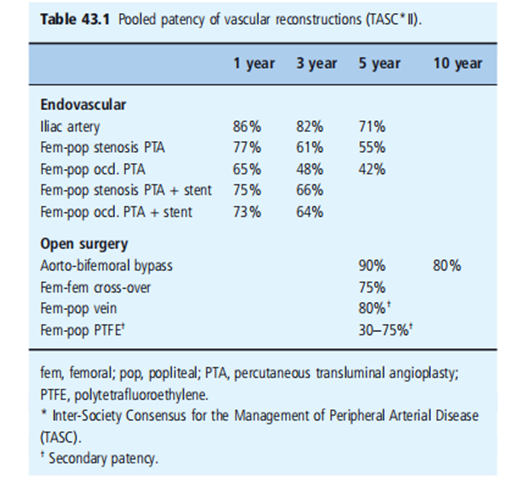
PTA of the superficial femoral artery may relieve symptoms; however, the results depend on the extent of the disease. The longer the lesion, the greater the risk of early re-occlusion. Stenting appeared to improve potency, at least for longer lesions (Table 43.1) [15]. When the indication for PTA is claudication, potency is better than when the indication is critical ischemia. This difference is related to the more extensive nature of the disease in cases of critical limb ischemia and may also be related to poor run-off vessels. The 3-year potency was 48%, which could be improved to 64% with the addition of stenting. In the case of critical limb ischemia, the results at 3 years showed a potency of 30% without stenting and 63% with stenting (Table 43.1) [15]. PTA of the crural vessels is also feasible; however, long-term results are not good. Data on limb salvage with PTA of the crural vessels alone are scarce. Adjunctive medical therapy to improve potency following PTA and stenting, with anticoagulation and/or antiplatelet therapy, has been tested in only a few trials. Antiplatelet drugs improve potency, and the combination of aspirin and clopidogrel may be beneficial [16].
Open surgical revascularization
Open surgical revascularization still dominates as the treatment of choice in cases of critical limb ischemia because of the extensive nature of atherosclerotic lesions in these patients. For claudication, open surgical treatment is rarely performed, while for the extensive disease of the distal aorta and iliac arteries, the aorta-bi femoral bypass remains the procedure with the best long -term outcome. In addition, a femoral–femoral cross-over bypass may be performed for unilateral iliac artery occlusion. Additionally, endarterectomy, as described below, may be an option for claudication treatment. Only one trial compared open surgery with endovascular treatment of critical limb ischemia, the bypass versus angioplasty in severe ischemia of the leg (BASIL) trial [17]. The primary efficacy outcome measure was amputation-free survival; however, because approximately two-thirds of the endpoints were deaths, only one-third of the endpoints determined which procedure was best. Within 6 months postoperatively, there was no difference in the primary endpoint, but thereafter, bypass patients seemed to perform better [17].
In general, two surgical techniques are used: endarterectomy and bypass. Endarterectomy is performed by separating the intima from the media, and in this manner, the atherosclerotic lesion can be removed. Endarterectomy can be used in cases with severe occlusive lesions of limited anatomical extension in the external iliac or common femoral artery. The advantage of this technique can often be performed without the use of artificial graft materials, and its patency is excellent. Bypass is preferred when the obstructive and/or occlusive lesions are extensive (e.g., total superficial femoral artery occlusion or multiple serial lesions warranting a femoral–crural bypass) (Figure 43.4).
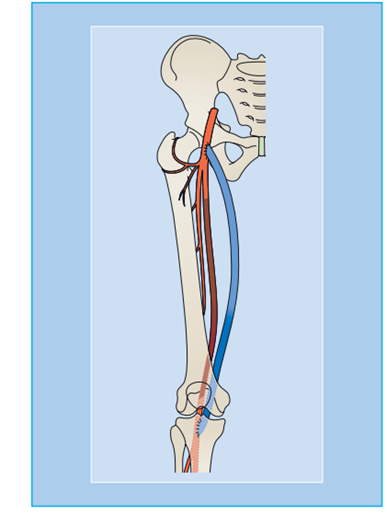
Figure 43.4: Long superficial femoral artery occlusion treated with femoropopliteal bypass.
Bypass surgery can be performed by using artificial materials or autologous veins. Artificial grafts are almost always used for bypass of the aortic or iliac artery origin. This is because there are no easily removable veins with similar dimensions that can be used in these locations. Additionally, Dacron or polytetrafluoroethylene (PTFE) grafts perform very well in the aortoiliac–femoral region. For peripheral bypasses, typically originating from the common femoral artery, autologous vein grafts are preferred for two reasons: they last longer (much better patency) (Table 43.1) and carry less risk of infection. For longer bypasses, such as those from the common femoral artery to the popliteal artery below the knee, a saphenous bypass is performed, leaving the vein in situ. This means that the vein is left in its original anatomic location; however, the proximal and distal ends are anatomized to the arterial system. The venous valves are cut with a knife mounted on a catheter and side branches are occluded. In this manner, the vein retains its nervous innervations and native vascularization. - Complications of endovascular treatment.
However Complications are mainly related to the puncture site and the risk of peripheral embolization, systemic " cardiovascular complications are rare. Hematoma in the groin access point is common; however, it rarely requires any action. Iatrogenic pseudo aneurysms develop in 0.5 – 1% of cases and can easily be treated with ultrasound-guided compression or ultrasound-guided thrombin injection.
Complications of open surgical treatment
They can be divided into local and systemic categories. The former relates to actual incisions and dissections, including wound healing and infections. Although complications from accidental damage to other organs and/or structures are rare, wound healing problems and infections are quite common. In particular, surgery on the lower limb involving the groin and peripheral incisions causes wound complications in 10 – 20% of cases (e.g., hematoma, lymph oozing, or necrosis of the wound) [18]. Infections are seen in 3 – 5% of cases, approximately one-third of which involve vascular reconstruction. Infection of vascular reconstruction is more frequent when using artificial graft material [18]. Systemic complications associated with open surgical revascularization are related to surgical trauma and the stress response. The rate of cardiopulmonary complications is considerable in vascular reconstructions involving the aorta and other central arteries. Implantation of an auto-bi femoral bypass graft is associated with A 30-day mortality of 2 – 5% and a rate of " general " complications of 10 – 15% (e.g., pulmonary, cardiac, renal, prolonged stay at the intensive care unit, stroke, and deep venous thrombosis) [18]. Systemic complications associated with peripheral revascularization occur less frequently, but are considerable. When the indication is claudication, the morbidity concerning general complications is low, 2 – 4%; however, in cases of critical ischemia and peripheral bypass surgery, the morbidity increases to 10% with a 30-day mortality of 3 – 5%. This difference in morbidity reflects the more advanced level of generalized atherosclerotic disease in patients with critical ischemia. Complications are more common in patients with diabetes, especially in those who undergo open surgery. A doubling of the risk should be expected.
Results of endovascular and o pen surgical reconstructions
The results of endovascular and op-pen surgical reconstruction are summarized in Table 43.1. In general, when treating more centrally located arterial obstructions, the long-term results are better. In addition, treating patients with claudication results in better long-term outcomes than treating patients with limb-threatening ischemia. This difference relates to the generally poorer condition of the peripheral circulation in cases of critical ischemia with better run-off vessels in the patient with claudication.
In peripheral reconstructions, the vein grafts performed better. It may seem unrewarding to treat patients with critical limb ischemia with a peripheral bypass using an artificial graft when there is only a 50% chance of being patented in 1 year; however, if the alternative is amputation and/or a very poor quality of life (i.e., severe rest pain), 1 year with a functioning graft may be worthwhile for both the patient and the surgeon. Limb salvage as a result is almost always better than the patency of the reconstruction because in many cases, once the ischemic limbs with tissue loss have healed, the " need " for amputation has decreased. Patients with diabetes typically have poorer outcomes of vascular reconstructions, with patency rates that are inferior to those without diabetes. Patients with diabetes have more complications to treatment, not only infections but also systemic complications are more common.
Acute lower limb ischemia
This condition is most often caused by thrombosis in patients with existing atherosclerosis (i.e., a patient with previous symptoms of chronic PAD). Another common cause is thrombosis of popliteal aneurysms. Embolism remains a common cause, although not as often as in the past, because of better anticoagulant therapy in patients with atrial fibrillation. Eighty percent of emboli are cardiac origin However, aortic or peripheral aneurysms may give rise to peripheral emboli. Other causes include trauma and iatrogenic lesions (e.g., arteriography with puncture of the femoral artery). Aortic dissection may cause lower limb ischemia as well as acute deep venous Thrombosis (phlegm a copulae dozens). Its incidence in Western Europe is 300 – 400 million per year.
Pathophysiology
Thrombosis is caused by plaque rupture and the subsequent thrombosis. Distal to acute occlusion, arterial flow is slow and, when combined with a hypercoagulable condition, may lead to further thrombosis. The degree of ischemia depends on the location and the degree of collateral development. Therefore, it is often better tolerated than embolism because patients with existing atherosclerosis often develop collaterals. Emboli typically occlude an artery at a bifurcation, in the lower limbs, at the aortic bifurcation (saddle embolus), iliac artery, and femoral artery bifurcation. Sixty percent of cardiac emboli end in the lower limbs, 15% in the arms, and the rest end in the brain and other organs. Micro emboli, typically from systems, affect small peripheral arteries and are thus the cause of the "blue toe" syndrome.
Symptoms
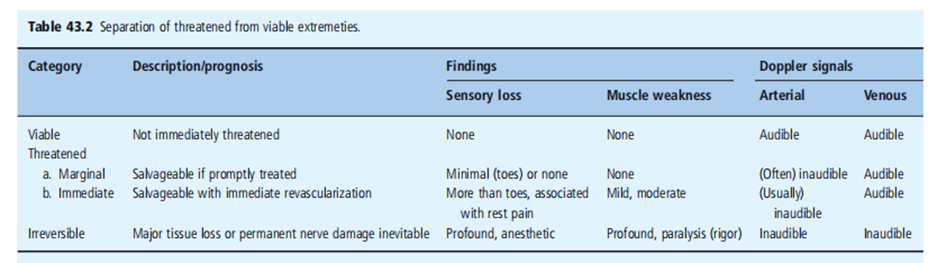
Acute ischemia is characterized by pallor, pain, pulselessness, paresthesia, and paresis (5Ps). Symptoms may begin dramatically and, in some cases, the late signs of ischemia, paresthesia, and paresis can occur within a few hours. More often, symptoms begin with pain, paresthesia, and, later, sensory and muscular paresis. Acute ischemia is traditionally divided into three classes (Table 43.2).
Diagnosis
The diagnosis is often easy with typical clinical signs. ABI will be low if measurable. Imaging with duplex ultrasound, magnetic resonance angiography (MRA), or digital subtraction angiography (DSA) is possible, but may delay treatment. In cases of thrombosis, it is often desirable to perform arteriography with subsequent thrombolysis to visualize the underlying pathology causing thrombosis.
Prognosis
If revascularization is possible before irreversible ischemia occurs, the limb can be salvaged and normal function is regained. Comorbidity is high in cases of acute ischemia; when acute
Revascularization requires a procedure-related mortality rate of 10 – 20
within the dialogue section of a research paper on peripheral vascular ailment, the findings of the observation are interpreted and contextualized. Researchers regularly compare their effects with present literature and discuss the consequences and ability mechanisms in the back of the found outcomes. here are a few feasible factors that could be discussed: occurrence and chance factors: The study may display the prevalence of PVD inside the studied populace and become aware of the important thing hazard factors related to the sickness. those risk elements can consist of smoking, high blood pressure, diabetes, hyperlipidemia, obesity, and a sedentary lifestyle. The discussion may also highlight the significance of those hazard factors within the development and progression of PVD. sickness Severity and Scientific Manifestations: Researchers can also talk about the distribution of ailment severity a number have a look at participants and the associated medical manifestations. this could vary from asymptomatic instances to intermittent claudication (pain during workout), vital limb ischemia (extreme limb pain at relaxation), and tissue necrosis. The discussion may additionally explore the effect of disorder severity on a patient's pleasant existence and useful status. treatment and management: The dialogue may additionally cover numerous remedy alternatives for PVD, which include way-of-life changes (e.g., smoking cessation, workout), pharmacotherapy (e.g., antiplatelet dealers, statins), and invasive interventions (e.g., angioplasty, skip surgery). Researchers may additionally speak about the effectiveness of various remedy modalities, capability complications, and the need for a multidisciplinary method concerning vascular surgeons, interventional radiologists, and different healthcare specialists.
The belief segment of a research paper on peripheral vascular disease summarizes the principal findings of the examination and gives a concise precis of the implications. It has to mirror the objectives mentioned within the advent and the effects received thru the studies techniques. here are some key factors that may be blanketed within the conclusion: summary of Findings: the belief should in brief recapitulate the primary findings of the study. this may consist of the prevalence of PVD, diagnosed threat elements, sickness severity distribution, and treatment consequences.
scientific significance: Researchers must highlight the medical importance of their findings. this can include the potential effect on patient management, the significance of early detection and intervention, and the want for centered prevention techniques.
obstacles: it's miles crucial to renowned the constraints of the observation. this can include pattern length constraints, ability biases, or another factor that could have stimulated the effects. Acknowledging barriers enables providing context for interpreting the findings.
future guidelines: Researchers may also suggest ability avenues for future research based totally on the gaps recognized for the duration of the have-a-look. this may consist of investigating novel remedy procedures, exploring particular subgroups of patients, or assessing long-time period outcomes in PVD management.
By following those preferred recommendations for research strategies, result discussion, and end, researchers can correctly contribute to the understanding of peripheral vascular disease and tell medical exercise and decision-making.
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project We would also like to thank My Mentor [Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout the research. Their insights and expertise were instrumental in shaping the direction of this project
I at this moment declare that:
I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
The authors declare that they have no conflicts of interest.
No Funding was received to assist with the preparation of this manuscript
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
