AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Jose A. Pinto Tasende, MD, PhD, Department of Rheumatology-INIBIC, Complexo Hospitalario Universitario de A Coruña, 84 Xubias de Arriba Road, 15006 A Coruña, Spain.
Citation: Jose A. Pinto Tasende Jose M. Lorenzo Alvarez, Carlota Iñiguez Ubiaga, Luis Fernández Dominguez, Carlos García Porrúa, Francisco J. Maceiras Pan, Jose L. Guerra Vázquez and Jose A. Mosquera Martínez (2021) Obesity and Clinical Activity in Psoriatic Arthritis Patients Treated with Synthetic Disease-Modifying Antirheumatic Drugs. J, Clinical Medical Reviews and Reports. 3(9); DOI: 10.31579/2690-8794/099
Copyright: © 2021, Jose A. Pinto Tasende, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 August 2021 | Accepted: 13 September 2021 | Published: 30 September 2021
Keywords: corticosteroid; csDMARD; DAPSA score; enthesitis; metabolic syndrome; obesity; psoriatic arthritis
Introduction: Comorbidities are prevalent in psoriatic arthritis (PsA) and which may affect disease activity and response to therapy.
Aims: To evaluate comorbidities among patients with PsA naïve to biologics, and their association with basal inflammatory activity status, before starting them.
Methods: We performed a retrospective cross-sectional a study of cohort of patients with PsA (CASPAR criteria), treated with synthetic disease-modifying antirheumatic drugs. Patients were managed according to EULAR/GRAPPA recommendations, and the collected variables included demographics, clinical, serological, classical CV risk factors, and treatment. Disease activity was assessed using the Disease Activity Score for Psoriatic Arthritis and clinical DAPSA scores. The tests were two-tailed, with a significance level of <0.05.
Results: A total of 416 patients were included in the study: 222 maintained remission or low disease activity being treated without biologics, and 194 who needed to be treated with bDMARD because they did not response well to csDMARD. From patients who were waiting to start biologics, 38.1% had obesity and had increased risk of MetS for age > 50 years old (OR 3.287 [95%CI: 1.258-8.591], p 0.015) and CRP > 0.5 mgr/dL (OR 2.684 [95%CI: 1.141-6.313], p 0.024) but not for cDAPSA>13 (OR 1.539 [95%CI: 0.695-3.409], p 0.288).
DAPSA score was higher in patients with obesity, 20.3 (14.4) vs 13.8 (8.5), p0.010 and these patients had an OR for cDAPSA>13 of 3.15 [95%CI: 1.07-9.25], p 0.037). Patients with obesity had a higher frequency of DAPSA and cDAPSA MoDA-HDA (p = 0.022; p = 0.032). In the linear logistic regression analysis, a high-moderate DAPSA score was associated with obesity (p = 0.017), CRP (p <0.0001), and cDAPSA score with obesity (0.029) but not with CRP (p = 0.748). Obesity and corticosteroid treatment were independent factors for cDAPSA>13 and the presence of enthesitis for cDAPSA≤13.
Conclusion: PsA patients who did not respond well to csDMARD had a higher prevalence of MetS, associated with age > 50 years and CRP higher than normal values. The DAPSA score was higher in patients with obesity and corticosteroid treatment. Enthesitis was more frequent in patients with low disease activity by DAPSA score.
Psoriatic arthritis (PsA) is a chronic inflammatory skeletal and dermatological disease with heterogeneous clinical features and a strong relationship with the spondyloarthritis group, sharing several genetic, clinical, and radiographic characteristics [1] and with a prevalence in the western country populations around 0.07-0.42 [2]. Therapeutic options for both skin and joint diseases have dramatically improved, allowing efficient control of inflammatory activity in patients, including control of comorbidities such as metabolic and cardiovascular diseases (CVD) [3]. Inflammatory charge of psoriatic disease seems to be an independent risk factor for CVD in those patients with severe joint or skin disease [4], even in patients without traditional CVD risk factors and having a higher frequency of subclinical atherosclerosis than matched controls [5, 6].
PsA patients have multiple comorbidities such as obesity, hypertension, and hyperlipidemia [4, 7] and a higher prevalence of cardiovascular comorbidities compared to patients with psoriasis without PsA [8] and compared to the general population [9]. More than 50% of patients with PsA have at least one comorbidity and approximately 40% of patients can have three or more comorbidities [10, 11]. However, patients with PsA are at a higher risk of cardiovascular disease, including myocardial infarction and major adverse cardiovascular events (MACE) after accounting for traditional cardiovascular risk factors [12].
Obesity is a prevalent comorbidity in PsA, and this may be particularly important as adipose tissue plays a role in metabolism and immune-inflammatory processes affecting disease activity and response to therapy [13]. A higher body mass index (BMI) affects disease activity and response to therapy and has an impact on cardiovascular and metabolic morbidity [14]. It has been shown that metabolic syndrome (MetS) is associated with a state of chronic, low-grade inflammation [15] and Haroon et al [16] confirmed the high prevalence of MetS in patients with PsA compared to a control group probably reflecting the increasing burden of inflammation.
The Disease Activity Psoriatic Arthritis Index (DAPSA) is one of the main recommended targets for PsA treatment following EULAR recommendations, with a treat-to-target strategy [17]. Obese patients were found to have higher joint counts, C-reactive protein (CRP), Health Assessment Quality-Disability Index (HAQ-DI), and composite measures, including Clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) [18]. Dietary intervention showed significant improvement in disease activity measures like DAS28-CRP, DAPSA, and HAQ-DI.
Therefore, we hypothesize that a higher body mass index and the presence metabolic syndrome are a risk factor for development much disease activity and worse response to therapy.
The aim of this study was to evaluate obesity and MetS among patients with PsA treated with synthetic disease-modifying antirheumatic drugs (csDMARD), naïve to biologics and its association with inflammatory activity status.
Study population
We performed a retrospective cross-sectional multicenter study of a cohort of patients with following inclusion criteria: ≥18 years of age, all patients with a diagnosis of PsA who met the CASPAR criteria [19], included in the “Sueiro Cohort” (20), treated with csDMARD without good response and waiting to start biologic treatment. As a control group, we used a previously described cohort of patients with PsA naïve to biologics and low disease activity or remission treated with csDMARD [21]. Key exclusion criteria were immune-mediated disease other than PsA, pregnancy, cancer or serious infection in the moment of evaluation.
All patients gave their informed consent to participate in the study, and the rules of good clinical practice (Helsinki declaration) were followed. The study was approved by the local clinical research ethics committee (reference no. 2015/671). Patient anonymity and confidentiality were preserved throughout the study.
Study design and variables
Patients were managed according to a standard protocol adopted at Rheumatology outpatient clinic of six hospitals and were followed up for at least 6 months. The study period spanned from 2017 to 2019.
Collected variables included age, sex, blood biochemistry, blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), HLA-B27, rheumatoid factor, glucocorticoid, NSAID and csDMARD, smoking habit, hyperuricemia, type 2 diabetes mellitus, obesity (BMI≥ 30 kg/m2), liver involvement (NAFLD, not including infectious or alcoholic liver disease) and the diagnosis of anxiety and depressive syndrome performed by the Health Mental Unit.
Metabolic syndrome (MetS) was defined as a combination of abdominal obesity, impaired fasting glucose, atherogenic dyslipidemia, and elevated blood pressure. Revised NCEP ATP III criteria [22] require at least three of the following components: abdominal obesity (waist circumference ≥90 cm for men, or ≥85 cm for women); triglycerides ≥150 mg/dL, and/or drug treatment for elevated triglycerides; high-density lipoprotein (HDL)-cholesterol <40>
Evaluation procedures for activity disease
The clinician´s criteria determined whether patients had a good response to DMARD. Disease activity status was supported by tender and swollen joint counts (TJC68 and SJC66) from patients before they started treatment with biologics. At the same time, patient-reported outcome measures were collected with Patient Global Assessment (PtGA 0-10 cm) and Patient Pain Assessment (Pain 0-10 cm). DAPSA and cDAPSA scores were calculated. Very low (VLDA), low (LDA), moderate (MoDA), and high disease activity (HDA) status were obtained by DAPSA and cDAPSA scores with their defined cut-offs elsewhere [23], when data were present in the records.
Statistical analysis
A descriptive statistical analysis of all the variables was performed, including central tendency and dispersion measures for continuous variables, and absolute and relative frequencies for categorical variables. The differences between quantitative variables with normal distribution according to the Kolmogorov–Smirnoff test were analyzed using Student’s t-test, or ANOVA test. Differences between quantitative non-normal variables were studied using non-parametric tests (Mann–Whitney U test or Kruskal–Wallis H test). Pearson’s chi-square or Fisher’s exact test was used for qualitative variables. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated using binary logistic regression analysis. Initially, univariate analysis was performed to examine the unadjusted associations of DAPSA and cDAPSA with its potential risk factors. The factors introduced in the univariate model were age, sex, disease duration, patterns of arthritis, nail involvement, dactylitis, enthesitis, use of NSAIDs, use of glucocorticoids, use of csDMARD, duration of systemic treatment, CVRF, and CRP. Significant variables in the univariate analysis (P<.10) were then introduced in a multivariate analysis with a backward stepwise approach. Tests were two-tailed with a significance level of 5%. Data were analyzed using SPSS version V21.0 statistical software (IBM Corp. NY, USA).
All patients: CVRF
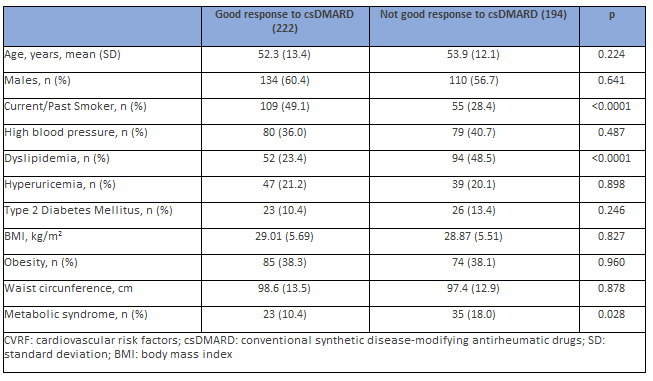
A total of 416 PsA patients were included in the study: 222 PsA patients kept on remission or low disease activity being treated without biologics (DAPSA score 8.3±4.5), and 194 who needed to be treated with bDMARD because they did not respond well to csDMARD. Both groups showed no differences with respect to age or sex. Dyslipidemia and MetS were more prevalent, and smoking habits (current/past) were less frequent in PsA patients who did not respond well to csDMARD (Table 1).
PsA patients who needed to be treated with bDMARD
Patients with a good response to csDMARD (in remission/LDA disease) were not included in the association analysis for inflammation because their clinical and biological activity indices were not elevated.
The frequency of traditional CVRF was more prevalent in men than in women: active smokers, diabetes mellitus, and hyperuricemia, but not hypertension, dyslipidemia, and obesity. NAFLD was also more frequent in men than in women. Women had less CVE than men (12 [4.4%] vs. 30 [9.2%], p = 0.021), but this difference was only in relation to angina and MI, but not in relation to stroke/TIA. Hyperuricemia (25.3% vs. 4.8%, p <0 xss=removed>
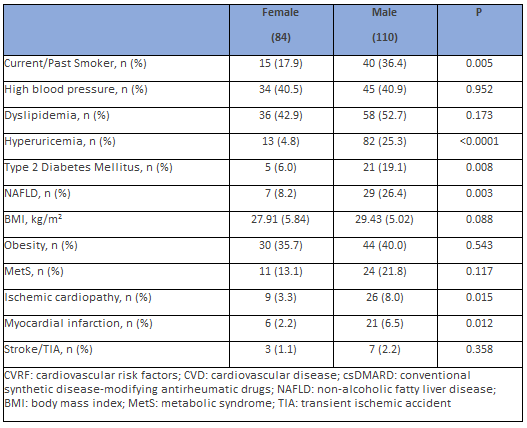
Patients with CVE had more nail psoriasis (41.7% vs. 20.8%, p=0.09), but there were no significant differences with regard enthesitis (p=0.562), dactylitis (p=0.780), or uveitis (p=0.553). Clinical patterns of PsA, treatment with NSAIDs, corticosteroids, or the positivity for HLA-B27 did not imply differences among genders.
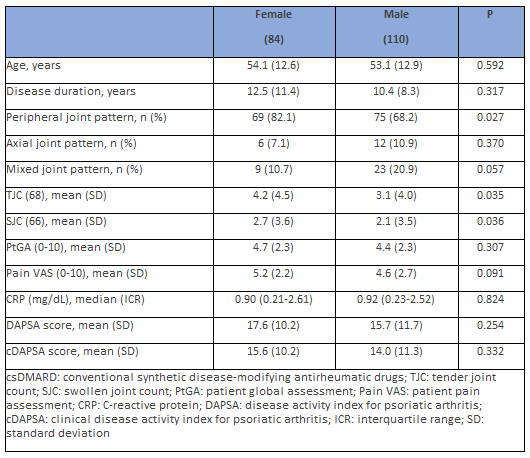
Most peripheral joint involvement was observed in women and axial affection in men (p = 0.027), but there were not significant differences between women and men in nail disease (17.1% vs. 25.4%), enthesitis (23.5% vs. 21.1%), dactylitis (12.7% vs. 12.9%), or uveitis (2.4% vs. 2.9%). Anxiety and depressive disorders were more prevalent in women (31% vs. 15.5%, p = 0.010).
Furthermore, women had joint counts much higher than men (TJC p =
0.035 and SJC p = 0.036), but there were no differences in the PtGA and levels of C-reactive protein. Patient pain VAS scores were higher in women but did not reach statistical significance. There was no difference between males and females with regard DAPSA or cDAPSA scores (Table 3), neither according to age (p = 0.622). The DAPSA and cDAPSA scores had a high positive correlation between both (rho = 0.972, p < 0>
A statistically significant difference was not observed between the DAPSA score and treatment with NSAIDs but was detected in relation to corticoids. The proportion of patients who received corticosteroids was significantly higher among patients with DAPSA>14 (28.8% vs. 11.5%; p = 0.006).
Metabolic syndrome and inflammatory activity
Patients with MetS were older than those without MetS, 59.6 (9.8) vs. 52.2 (13.1) years (p = 0.002). MetS was present in 18.0% of men and 13.1% of women (p = 0.117). MetS was not associated with clinical patterns (p = 0.782), serum levels of CRP (p = 0.681), DAPSA (p = 0.252), or cDAPSA score (p = 0.215). A higher frequency of enthesitis (p = 0.012) and lower of dactylitis (p 0.030) was observed.
In the linear logistic regression analysis (adjusted for age and sex), a high DAPSA score was not associated with MetS (p = 0.350). Binary regression analysis showed increased risk of MetS for age > 50 years old (OR 3.287 [95%CI: 1.258-8.591], p 0.015) and CRP > 0.5 mgr/dL (OR 2.684 [95%CI: 1.141-6.313], p 0.024) but not in relation to gender (OR 2.136 [95%CI: 0.932-4.893], p 0.073) neither to cDAPSA>13 (OR 1.539 [95%CI: 0.695-3.409], p 0.288).
Obesity and inflammatory activity
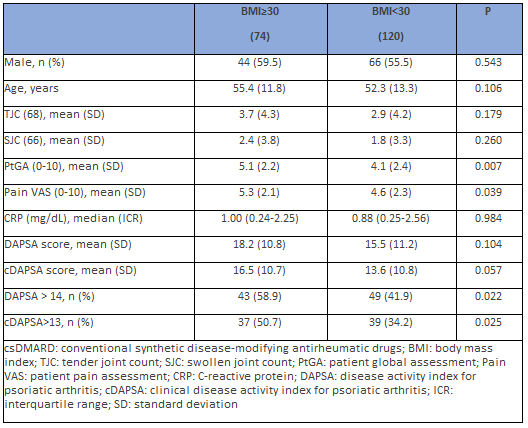
Patients with obesity were not significantly older than those without obesity (p = 0.106) and there were no differences in relation to sex (p = 0.543).
Obesity was not associated with clinical patterns (p = 0.322), onychopathy, or other clinical features. There was no observed correlation with frequency of enthesitis (p = 0.293) or dactylitis (p = 0.493). The intake of NSAIDs (33.6%) and corticosteroids (18.9%) implied no difference in relation to obesity (p = 0.666 and 0.371, respectively).
PtGA and pain VAS scores were higher in patients with obesity (p 0.007 and 0.044), but TJC, SJC, serum levels of CRP, DAPSA, or cDAPSA scores remained unchanged (Table 4). When the cut-off points of DAPSA were taken, patients with obesity had a higher frequency of DAPSA MoDA-HDA (p = 0.022) and the same was observed with cDAPSA (p = 0.025).
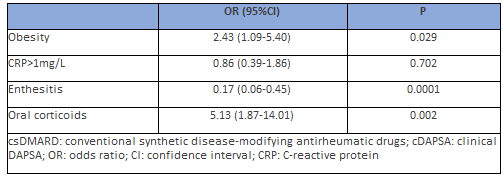
In the linear logistic regression analysis (adjusted for age and sex), a high DAPSA score was associated with obesity (p = 0.017) and CRP (p <0 xss=removed xss=removed> 50 years and sex) instead of DAPSA to include CRP as an independent variable, together with obesity, MetS, and other dichotomous variables. When it was taken “cDAPSA MoDA-HDA” as a dependent variable, it was observed that the presence of obesity and treatment with corticosteroids were independent factors for cDAPSA>13, and the presence of enthesitis for cDAPSA≤13 (Table 5).
Psoriatic arthritis is associated with increased cardiovascular comorbidity compared to control populations, including the risk of high blood pressure, dyslipidemia, diabetes mellitus, obesity, and metabolic syndrome, which results in increased cardiovascular events [8]. Likewise, several observational studies [24-26] have shown that the occurrence of cardiovascular events is directly associated with the severity of psoriasis, understanding the correlation between systemic inflammation and this increased risk. However, in a cohort study in which neither psoriasis nor severe psoriasis were associated with an increased risk of major cardiovascular events over a period of 3–5 years, after adjusting the parameters in relation to known cardiovascular disease risk factors [27], the risk of a major cardiovascular event was 36% higher in patients with psoriasis who also had inflammatory arthritis. Husted et al. [8] observed that the prevalence of hypertension, obesity, hyperlipidemia, type 2 diabetes mellitus, and at least one cardiovascular event in PsA patients was 37.1%, 30.0%, 20.7%, 12.0%, and 8.2%, respectively. This was significantly higher than in patients with psoriasis without arthritis, with unadjusted ORs ranging from 1.54 to 2.59. In multivariate analyses, hypertension remained significantly elevated (adjusted OR 2.17).
In our study, dyslipidemia and MetS were more prevalent in PsA patients who were going to start therapy with biologics when we compared them to patients with low charge of activity who were treated with csDMARDs, and with good response to them.
When we analyzed more in dept the most frequent CVRF, we found high percentages of hypertension, dyslipidemia, hyperuricemia, and diabetes among patients who experienced cardiovascular events, and these factors were directly related to male sex. The results obtained closely resemble those presented by Shah et al. [28], after analyzing the most frequent comorbidities associated with psoriatic arthritis in a cohort of US patients using real-life data. In this study, the authors observed that comorbidities in relation to the metabolic syndrome were higher in the population affected by this pathology than in the healthy population, with exception of obesity, which in the USA has a prevalence of 36.5%.
Given the strong link between PsA, systemic inflammation, metabolic syndrome and cardiovascular events, control of the inflammation associated with PsA may be applied beyond the skin and joint disease to prevent cardiovascular diseases. Limited data exist regarding the impact of csDMARD on cardiovascular outcomes. An association between methotrexate treatment and reduced cardiovascular risk has been found among patients with PsA using DMARDs who have been reported to have a lower cardiovascular risk than those who were not using them [4]. A meta-analysis of ten cohort studies including patients with rheumatoid arthritis, psoriasis, and PsA found that MTX therapy was associated with a 21% reduction in overall cardiovascular risk and 18% reduction in myocardial infarction risk [29].
The serum level of C-reactive protein is considered a marker of inflammation in several conditions, including psoriasis and rheumatoid arthritis, and high baseline levels of CRP have been found in some patients with psoriasis with or without PsA [30]. However, the clinical usefulness of C-reactive protein determination in cardiovascular disease in the general population has been questioned in relation to patients with pre-existing inflammatory conditions such as psoriasis [31]. In the present study, there were no differences between men and women or patients with or without CVD. Patients with obesity neither had higher levels of CRP when they were compared to no obese.
Recently, Gerdes et al. [32] suggested a neutral to favorable long‐term trend in metabolic and liver parameters under secukinumab treatment, and metabolic comorbidities were associated with increased hsCRP levels. In this exploratory post hoc analysis of pooled data from three phase 3
studies in patients with plaque psoriasis, psoriatic arthritis, metabolic syndrome, obesity, impaired glucose metabolism, and hyperuricemia, each were associated with increased hsCRP levels at baseline. Concomitant obesity attenuated the decline in hsCRP levels under treatment, which could reflect the role of systemic inflammatory processes in their pathophysiology.
The role of Th17-derived cytokines in the pathogenesis of obesity and related inflammatory diseases has been increasingly recognized [33]. Obesity has been shown to promote the expansion of IL-17-producing T cells in adipose tissue (especially visceral fat) and peripheral tissues [34, 35]. Accordingly, a significant increase in circulating IL-17 and IL-23 cytokines has also been observed in obese individuals compared with lean individuals in humans [36]. Supporting the implication of IL-17 in metabolic syndrome, the levels of IL-17R expression in the liver or muscle have been shown to correlate with insulin resistance [37], and IL-17 blocking results in a decrease in hepatic inflammation in non-alcoholic steatohepatitis syndrome [38].
Frequently, obese patients with PsA also have a higher disease severity. Mok et al. [39] observed that among 314 patients with PsA, obese patients tended to have a longer time to diagnosis compared to patients with a normal BMI, which leads to greater persistence over time of a systemic inflammatory state. The presence of arthritis may indicate an increased underlying systemic inflammation that may worsen comorbidities and cardiovascular outcomes. Obesity and its related metabolic abnormalities are more prevalent in patients with PsO and PsA than in those with other types of arthritis [39-41]. We could not observe any association between BMI>30 and tender or swollen joint counts but patients with BMI>35 (morbid obesity) had higher joint counts. Enthesitis was higher in obese patients, conversely to reported by Eder et al. [42]. We believe that patients with active enthesitis did not respond to csDMARD for this reason, requiring start treatment with bDMARD despite having a cDAPSA score in low activity, which is a consequence of not including an assessment of enthesitis in this score. Although systemic corticosteroids are not included in any guidelines, their prescription for PsA is still common in real life [43]. In the present study, patients with DAPSA>14 had a higher proportion of treatment with corticoids as a result a higher inflammatory activity. Patients using long-term low-dose prednisolone have hepatic insulin resistance and reduced peripheral nonoxidative glucose disposal indicating that low-dose prednisolone also exerts a deleterious effect on carbohydrate metabolism and abdominal adiposity [44].
In other reports [45-46], obese patients were found to have higher joint counts, C-reactive protein, Health Assessment Quality-Disability Index, and composite measures including cDAPSA. In our study, obesity was associated with higher DAPSA and cDAPSA scores, but the difference was not statistically significant. However, obese patients had a higher prevalence of DAPSA>14 (moderate-to-high activity) than patients without obesity. Both DAPSA and cDAPSA scores were had higher in patients with morbid obesity.
The study has some strengths and limitations. It was design as a cross-sectional study, and to evaluate the role of some specific comorbidities, such as cardiovascular, a longitudinal study could provide more data. It would be of interest to provide the MDA (minimal disease activity) status of our patients to evaluate disease activity status, including more domains of psoriatic disease than DAPSA score, like enthesitis or skin activity, since in other reports it has published those patients with a higher body mass index are less likely to achieve MDA and further studies are needed to answer these questions. The chronic inflammation in patients with high body mass index may be responsible for the increased risk for cardiovascular disease in PsA patients, and poor response to therapy.
Psoriatic arthritis has an increase in classic risk factors and cardiovascular events, especially in men and it also increases with age. There is abundant evidence of the association between chronic inflammation and cardiovascular risk factors, such as obesity or metabolic syndrome, but population studies are required to better understand the underlying mechanisms.
Some manifestations of PsA, such as enthesitis that are not included in the DAPSA score, have a significant inflammatory activity and must be considered when evaluating disease activity. Similarly, treatment with corticosteroids indicates that they have been established due to the inflammatory activity of PsA.
Early management of comorbidities, using the reference guidelines as well as a close control of disease activity, can contribute to the global improvement of these patients.
Take home messages:
The authors thank Mrs. Alba Pinto-Alonso for her grammatical support.
Conceptualization, JAPT, JMLV, CGP, FJMP and JAMM; Methodology, JAPT, JMLA, CIU, LFD, CGP, FJMP, JLGV and JAMM; validation, JAPT, JMLV, CGP, FJMP and JAMM; formal analysis, JAPT, JMLV, CGP, FJMP and JAMM; investigation, E.F., L.D., A.S., F.M., G.C., M.P. and F.P.; data curation, JAPT, JMLV, CGP, FJMP and JAMM; writing—original draft preparation, JAPT, JMLV and CGP; writing—review and editing, JAPT, JMLA, CIU, LFD, CGP, FJMP, JLGV and JAMM. All authors have read and agreed to the published version of the manuscript.
All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee (Ethical Committee of Santiago-Lugo, n. 2015/671) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all subjects involved in the study.
The data presented in this study are available upon request from the corresponding author. The data are not publicly available because of privacy restrictions.
None.
The authors declare no conflict of interest.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
