AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Camille Elliott, Department of Para- Clinical Sciences. (Pathology and Microbiology Unit). University of the West Indies. Eric Williams Medical Complex, Mt. Hope Hospital, Champs Fleurs, Trinidad and Tobago, West Indies.
Citation: Camille Elliott, A Justiz-Vaillant. (2020) Nosocomial Infections at Three Regional Tertiary Hospitals in Trinidad and Tobago. Biomedical Research and Clinical Reviews. 1(1); DOI: 10.31579/2692-9406/001
Copyright: ©2020 Camille Elliott, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 February 2020 | Accepted: 16 March 2020 | Published: 20 March 2020
Keywords: Antibiotic resistance; cross sectional study; incidence; mortality; Nosocomial Infections (NI) and susceptibility pattern.
Objective: The main objectives of this research were to conduct and provide accurate and original findings related to the epidemiological study of nosocomial infections at three regional tertiary hospitals in Trinidad and Tobago. Specifically, the researcher determined; the frequency of nosocomial infections (NI), the frequency of multiple drug resistance among bacterial organisms associated with NI, infection control measures practiced at the research hospitals and the cost of such NI in terms of morbidity and mortality
Synopsis: This study estimated the rate of nosocomial infections (NI) among patients at three major regional hospitals in Trinidad and Tobago and evaluated the frequency of pathogens associated with nosocomial infections. Approximately 450 of 126, 668 patients had nosocomial infections and the most frequent type of nosocomial pathogens were: Staphylococcus sp. (22.5%), Pseudomonas aeruginosa sp.
(12.7%), Acinetobacter (11.8%) and Klebsiella sp. (11.6%).
Methods: A one-year prospective cross-sectional study was carried out. The nosocomial pathogens were retrieved from the microbiology laboratory. Antimicrobial susceptibility test by the disk diffusion method were done on all bacterial isolates. Data was analysed using SPSS version 20.0.
Results: This research revealed that 450 inpatients suffered nosocomial infections, with thirty (30) mortalities during the twelve (12) months that the study lasted (June 2013 to May 2014) at three regional hospitals of Trinidad and Tobago. The incidence of nosocomial infections was 5.8% and the nosocomial infection rate was 3.6 per 1000 (450/126,668). The highest rate (30.1%) was observed in the Intensive Care Unit (82/272 admissions). The most frequent type of nosocomial infection was Skin and Soft
Tissue Infections 168 (37.3%). Staphylococcus sp. (22.5%), Pseudomonas aeruginosa sp. (12.7%), Acinetobacter (11.8%) and Klebsiella sp. (11.6%) were the most frequently occurring nosocomial pathogens.
Conclusion: Consistency in performing good hygiene practices is vital for reducing the high nosocomial rate found at the research sites. Prediction of these infections is very important as a part of clinical surveillance programs to take preventive measures in advance. The antimicrobial susceptibility pattern rate (ASPR) showed that only 8.3 % (5/60) of the isolates were antibiotic-susceptible strains.
Limited studies have been done on nosocomial infections in Trinidad and Tobago. Nosocomial infection is important to study so as to reduce the incidence, mortality and morbidity associated with nosocomial infections. Neonatal and elderly admitted patients are mostly at risk due to their weak immune. Orrett, 2002 indicated in his research in Trinidad and Tobago that 139 NI were identified from 629 admissions to ICU. The main NI was from respiratory tract, 41 (29.5%) followed by surgical wounds, 35 (25.2%), urinary tract, 28 (20.1%) then bloodstream, 24 (17.3%). From the 165 bacterial organisms, 80% of these organisms were gram negative bacilli, with Pseudomonas aeruginosa, 48 (36.6%), being the most common isolate followed by Klebsiella pneumoniae, 27 (20.6%) then Enterobacter sp. 22 (16.8%). The major gram positive isolates were Staphylococcus aureus, 23 (41.8%), coagulase-negative Staphylococci, 17 (30.9%) and Enterococci, 11 (20.0%) [9]. In Europe, incidences varied from 1% for all types of nosocomial infections and up to 23.6% in paediatric ICUs [16]. In the United States of America (USA), the Centre for Disease Control and Prevention (CDC) calculated approximately 1.7 million nosocomial infections from all types of microorganisms resulting in 99,000 deaths annually [17]. The American Thoracic Society/Infectious Disease Society of America (ATS/IDSA) introduced the concept of healthcare-associated pneumonia (HCAP) in 2005 and among its guidelines includes the recommended broad-spectrum antibiotics therapy as the treatment of hospital-acquired pneumonia [18]. These nosocomial pathogens affect other organs and tissues including the urinary tract [3, 5, 10, 19], bloodstream [20], brain [15, 21], and digestive tract [22] and the skin and soft tissues [23]. Prevalence of other multidrug-resistant bacteria are also rising, example vancomycin-resistant Enterococci (VRE) [1, 24] and Clostridium difficile that is an etiological agent of hospital acquired antibiotic-associated diarrhoea, causing an estimated 453,000 cases with 29,000 deaths yearly in the USA [11, 25].
According to World Health Organization (WHO), health care associated infection (HCAI) is defined as “an infection acquired in hospital by a patient, who was admitted for a reason other than that infection [29]. An infection occurring in a patient in a hospital or other health care facility in whom the infection was not present or incubating at the time of admission. This includes infections acquired in the hospital, but appearing after discharge, and occupational infections among staff of the facility” [30].
The standard criteria that were used along with WHO’s definition to confirm nosocomial cases were: the patient had no growth of organism from laboratory culture present at day one of their admission and no signs and symptoms present the same day including temperature spikes, worsening coughing or dyspnea, tachypnea, bronchial rates, breath sounds, vomiting, leukopenia <4000, low white blood cell (WBC) counts or leukocytosis, sloppiness at wound, redness, swelling, warmth, hotness around wound area, septicemia, hypotension, dysuria, urgency and tenderness. [31].
The aims of this study were to carry out a hospital microbiological survey for detecting the most prevalent pathogens that were causing nosocomial infections and to study their antimicrobial susceptibility patterns to prevent and control existing outbreaks and to insight in control measures to prevent nosocomial infection in Trinidad and Tobago. The research was a Cross Sectional Study conducted at three major hospitals in Trinidad and Tobago namely; Eric Williams Medical Science Complex, San Fernando General Hospital and Port of Spain General Hospital.
The study population was all patients hospitalized on the following wards: Medical, Surgical, Paediatrics, Intensive Care Unit (ICU) and Obstetrics & Gynaecology in three public hospitals in Trinidad during the period June 1, 2013 to May 31, 2014.
Inclusion and Exclusion Criteria:
All patients with features suggestive of nosocomial infections, who were willing to participate and gave their written or verbal consents on ward, were included in the study. Out-patients from accident & emergency wards and nephrology wards were excluded from this study, if suspected infections were considered community-acquired infections.
This research was a cross-sectional study conducted at three major hospitals in Trinidad and Tobago.
These medical facilities were: Eric Williams Medical Sciences Complex (EWMSC), San Fernando General Hospital (SFGH) and Port of Spain General Hospital (POSGH). Ethics approvals were granted by the University Campus Ethics Committee and the three Regional Health Authorities.
Clinical symptoms and laboratory diagnosis of nosocomial infections were noted and reviewed by the attending physician. Each week, prospective cases of nosocomial infections were reviewed from
Doctor’s notes in patient’s dockets for any clinical signs of nosocomial infections three days (72hrs) following patient admission for all types of nosocomial infections, except for nosocomial bloodstream infections (BSI) of which was observed two days (48hrs) after admission.
A total of 2600 patient dockets for the duration of the research period were obtained at each of the research hospitals and reviewed for prospective cases of nosocomial infections. Codes were assigned
for the nosocomial patient’s names on the data collection sheets. In addition, the patient’s names, their laboratory registration numbers, dates of samples collection and dates of sending samples to the laboratory by doctor or nurses were extremely useful to trace in the log book for their sample number, which helped to distinguish their respective nosocomial isolates from the others. The type of pathogen was confirmed by standard laboratory and biochemical tests. Samples were sent day one of patient’s admission to confirm that the patients had no growth of organism on admission.
Laboratory Diagnosis
Manual antimicrobial susceptibility testing was performed using agar disk diffusion method for all bacterial isolates on Mueller Hinton agar as recommended by Clinical and Laboratory Standards [32]. Assessment of the infection control measures practiced at the research hospitals and mortality figures were reviewed and assessed from patient’s dockets. In addition, total admission figures for all inpatients admitted on all researched wards were retrieved each month from the medical record unit at each of the regional hospitals, which was used to calculate the nosocomial rate. All samples were prepared and examined on at least three separate occasions and similar results were obtained. The antibiotics tested for resistance were amikacin (AK), amoxicillin/clavulanic acid (AMC), amoxicillin (AML), ampicillin (AMP), aztreonam (ATM), ceftazidime (CAZ), cefaclor (CEF), ciprofloxacin (CIP), clindamycin (CN), cefuroxime (CXM), clindamycin (DA), ertapenem (ETP), nitrofurantoin (F), cefepime (FEP), gentamicin (GN), imipenem (IMP), levofloxacin (LEV), linezolid (LZD), meropenem (MEM), norfloxacin (NOR), piperacillin (PIP), trimethoprine/sulphamethazole (SXT), tetracycline (TE), tigercycline (TGC), tobramycin (TOB) and piperacillin/tazobactam (TZP).
Descriptive statistics was used to calculate the sample size, incidence and rate of nosocomial infections and the percentage of nosocomial infections by age, months, research wards and nosocomial pathogens involved. Data related to patients and nosocomial infections were entered in a Microsoft® Access 2010 data bank and statistically processed using IBM SPSS® Statistics (version 20). The statistical review of the study was done by a biomedical statistician.
Sample Size Calculation:
The sample size was calculated via a cluster sampling method by wards and patient's files [33]. The most practical sampling approach, and via the WHO and standard criteria for prospective nosocomial cases were selected from the defined population. Surveillance was conducted on a weekly basis for fifty-two (52) weeks, for prospective nosocomial cases and pathogen isolates that were obtained from the laboratory during the research period. The average confirmed number of nosocomial cases by WHO’s definition was two per week. Therefore, via cluster sample size calculation equals number of wards multiplied by number of surveillance days and multiplied again by average number of patients with nosocomial infection confirmed during each week’s surveillance. That is 5 wards x 52 surveillance days x 2 = 520 patients were expected to acquire nosocomial infection during the data collection period. Hence, 520 patients from clustered sample size calculation were expected to have been associated with nosocomial infections with confidence interval of 95% and relative precision of 10% within the research period.
Measurements
In calculating the incidence of nosocomial infections in Trinidad and Tobago (2013 – 2014), the number of surveillance days (52) was multiplied by fifty (50) that was the average number of dockets reviewed each surveillance day from all the research wards: surgical, medical, paediatrics, ICU and Obstetrics & Gynaecology. Therefore, fifty-two (52) multiplied by 50 equals 2600 cases reviewed at each research site. If this product is multiplied by three (3) equals 7800 files reviewed during the research period. Four hundred and fifty (450) nosocomial cases were recovered during the research period. The incidence of all three (3) regional hospitals was calculated by dividing number of confirmed cases over total number of reviewed files and multiplied by one hundred: (450/7800) X 100 = 5.8% and this was the incidence for inpatients associated with nosocomial infections at all major regional hospitals of Trinidad and Tobago during the specified period.
The incidence at site A was calculated by dividing the number of cases with nosocomial infection (265) divided by the total files reviewed (2600) and multiplied by 100, which equaled to 10.2%. Similarly, the incidence at site B was calculated by dividing the number of cases with nosocomial infection (63) divided by the total files reviewed (2600) and multiplied by 100, which equaled to 2.4%. The incidence at site C was calculated by dividing the number of hospital associated cases (122) divided by the total files reviewed (2600) and multiplied by 100, which equaled to 4.7%.
The nosocomial rate was calculated by dividing the number of nosocomial cases recovered during the research period, divided by the total number of patients admitted on the research wards and multiplied by 100. The number of patients admitted on research wards for all three regional hospitals was 126,668 and the total number of nosocomial cases recovered for the research period was 450. Hence, nosocomial rate for research period was; 450/126,668 x 100 = 0.36%; 3.6 per 1000 patients. The nosocomial rate for research site A was 265/48057 = 0.55% (5.5 per 1000), whereas the nosocomial rate for research site B was 63/39950 = 0.16%; 1.6 per 1000 and the nosocomial rate for research site C was 122/38,661= 0.32%; 3.2 per 1000 patients.
Calculation of the antimicrobial susceptibility pattern rate (ASPR) for each pathogen strain was done as follows:
Number of antibiotics with susceptibility for a specific strain
ASPR= _________________________________________ x 100
Total number of antibiotic tested for that specific strain
From out of 126668 admissions 450 nosocomial infections were recorded.
Table 1 reflects the frequency distribution of gender cases. Male patients (56%) were predominantly more associated with nosocomial infections than female (44%).
Table 1:- Frequency Distribution of Demographic Variables
__________________________________________________________________
Gender Number of Nosocomial Cases (n) % P- Value
__________________________________________________________________
Male 251 56 1.960
Female 199 4 1.960
Total 450 100
__________________________________________________________________
Table 2 depicts frequency distribution of nosocomial infections by age groups. The age group 60 and over accounted for the highest percentage of nosocomial infections (26.7%), followed by the age group 50-59 (14.2%) and 40-49 (11.8%) respectively.
Table 2:- Age distribution of the Patients with Nosocomial Infections (NI) ________________________________________________________________________
Age Group Total NI (n) %
________________________________________________________________________
0-9 108 24
10-19 16 3.6
20-29 40 8.8
30-39 49 10.9
40-49 53 11.8
50-59 64 14.2
60 and above 120 26.7
Total 450 100 __________________________________________________________________
Table 3 represents the distribution of nosocomial infection in each month of the research period. The month of August had the highest percentage of nosocomial infections (12%), followed by the months of March (10.7%) and November (10%). The month of June (21) had the least percentage of nosocomial infections (4.7%) and followed very closely by July (4.9%).
Table 3:- Distribution of Nosocomial Infections (NI) in Trinidad and Tobago by Month 2013 - 2014
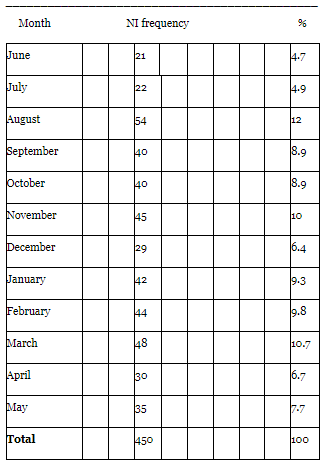
Table 4 depicts the frequency of microorganisms that were associated with nosocomial infections during the study period. Staphylococcus sp. (22.4%) followed by Pseudomonas aeruginosa (12.7%) accounted for the most frequent causative organism that were associated with nosocomial infections. These organisms were the most common multidrug resistant organisms producing many strains. Multiple pathogens (859) were mostly identified in each of the nosocomial cases of hospital-acquired infections.
Table 4:- Distribution of Identified Organisms associated with HAI in Trinidad and Tobago 2013 -2014
___________________________________________________
Identified Organisms Frequency %
___________________________________________________
Staphylococcus sp. 193 22.4
Pseudomonas aeruginosa 109 12.7
Acinetobacter sp. 101 11.8
Klebsiella sp. 100 11.6
Enterobacter sp. 74 8.6
Enterococcus sp. 64 7.4
Escherichia coli 58 6.8
Candida albicans 58 6.8
Proteus sp. 22 2.6
Serratia sp. 21 2.4
Providencia stuartii 14 1.6
Stenotrophomonas maltophilia 14 1.6
Streptococcus sp. 10 1.2
Citrobacter koseri 6 0.7
Alcaligenes sp. 6 0.7
Morganella morgannii 4 0.5
Burkholderia (P) cepacia 4 0.5
Achromobacter xylosidans 1 0.1
Total 859 100
__________________________________________________
Footnote: HAI – Hospital Acquired Infections
Table 5 shows susceptibility patterns of Staphylococcus sp. These microorganisms showed 15 patterns of susceptibility, which indicate that 15 strains of Staphylococci exist as nosocomial pathogens in the hospital setting. At least, all strains were resistant to nine antibiotics including AML and CN.
Table 5: - Susceptibility Pattern of Staphylococcus spp. in Trinidad and Tobago
2013- 2014
__________________________________________________________________
Staphylococcus spp. (193/859)Antibiotics
RD TGC VA CXM E OX TOB SXT CN LZP CIP FOX AMC AML CEC GM CAZ TE
_______________________________________________________________
a) S S S R R R R R R R R R R R R R R R
b) S S S R R R R R S R R R R R R R R R
c) S R S R R R R R R R R R R R R R R R
d) S S S R R R R R R S R R R R R R R R
e) S R S S S R R R R R R R R R R R R R
f) S R S S R R R S R R S R R R R R R R
g) S R S R S R R S R R S R R R R R R R
h) R R R R S S S S R R R R R R R R R R
i) S R S S S R R S R R S S S R R R R R
j) S S S R R R R R R R R R R R R R R R
k) S S R R R R R R R R R R S R R R R R
l) S S S R R R R R R R R R R R R R R R
m) R R S R S S R S R R S R S R S S R R
n) R R R R S R R R R S R S S R S S S S
o) S R S R S R R S R R S S S R R S R S
______________________________________________________________
Footnote: RD-Rifampicin, TGC- Tigercycline, VA-Vancomycin, CXM-Cefuroxime, E-Erythromycin, Ox-Oxacillin, TOB-Tobramycin, SXT-Trimethoprine/Sulphamethazole, CN-Clindamycin, LZP-Linezolid, CIP-Ciprofloxacin, FOX-AMC-Amoxicillin/Clavulanic acid, AML-Amoxicillin, CEC-Cefaclor, GM-Gentamicin, CAZ-Ceftazidime, TE-Tetracycline.
Table 6 represents the susceptibility pattern of Pseudomonas aeruginosa organisms, which had four different patterns indicating that there are four different strains of the same organism. All strains were resistant to ATM, ETP and TOB. On the other hand, the four strains were sensitive to TZP and CAZ.
Table 6: - Susceptibility Pattern of Pseudomonas aeroginosa in Trinidad and Tobago 2013- 2014
____________________________________________
Pseudomonas aeroginosa (109/859)Antibiotics
IPM TZP CAZ CIP CN GM ATM ETP ATM TOB
____________________________________________
a) S S S S S R R R R R
b) S S S S R S R R S R
c) S S S S S R R S R R
d) R S S S R S S R R S
____________________________________________
Footnote: IPM-Imipenem, TZP-Zosyn, CAZ-Ceftazidime, CIP-Ciprofloxacin, CN-Clindamycin, GM-Gentamicin, ATM-Aztreonam, ETP-Ertapenem, FEP-Cefepime and TOB-Tobramycin.
Table 7 depicts the antibiogram profile of Acinetobacter sp. indicating that five distinct strains of the same organism existed. The following antibiotics were observed to be most frequently resistant to Acinetobacter sp.: AML, AMC, ATM, CEC, ETP, CXM, GM and TE.
Table 7: - Susceptibility Pattern of Acinetobacter in Trinidad and Tobago 2013- 2014
__________________________________________________________________
Acinetobacter (101/859)Antibiotics
CAZ CIP ETP SXT TZP IMP TGC TOB AK CT TGC FEP CN AML AMC ATM CEC ETP CXM GM TE
_________________________________________________________________________
a) S S S S S S R R R R R R R R R R R R R R R
b) S R R R S R S S R R R R R R R R R R R R R
c) R R R R R S R S S S S R R R R R R R R R R
d) R S R S S S R R R R R S S R R R R R R R R
e) S S S S S R R R R R R R R R R R R R R R R ________________________________________________________________________
Footnote: CAZ-Ceftazidime, CIP-Ciprofloxacin, ETP-Ertapenem, SXT-Trimethoprine/Sulphamethaxole, TZP-Zosyn, IMP-Imipenem, TGC-Tigercycline, TOB-Tobramycin, AK-Amikacin, CT-Colistin, FEP- Cefepime, CN-Clindamycin, AML-Amoxycillin, AMC-Augmentin (Amoxicillin/Clavulanic acid), ATM-Aztreonam, CEC-Cefaclor, ETP-Ertapenem, CXM-Cefuroxime, GM-Gentamicin, TE-Tetracycline.
Table 8 shows the susceptibility of Klebsiella sp. indicating that there are six (6) different strains of the same organism. The table depicted the presence of multidrug resistant strains of this pathogen.
Table 8: - Susceptibility Pattern of Klebsiella spp. in Trinidad and Tobago 2013- 2014
__________________________________________________________________
Klebsiella spp. (100/859)Antibiotics
CN IPM TZP AMC FEP CAZ CXM TOB CIP LEV TE ETP F NOR GM SXT AML CEC GM ATM TGC _________________________________________________________________________
a) S S S S S S S S S S R R R R R R R R R R R
b) R S R R R R R R R S S R R R R R R R R R R
c) R S S R R R R R S R R S S S R R R R R R R
d) R S S S R R R R S R R S R S R S R R S R R
e) S S S R R R R R S R R R R R R R R R R R R
f) S R S S S S R R S R R R R R R R R S R S S
__________________________________________________________________
Footnote: CN-Clindamycin, IPM-Imipenem, TZP-Zosyn, AMC-Augmentin (Amoxicillin/Clavulanic acid), FEP-Cefepime, CAZ-Ceftazidime, CXM-Cefuroxime, TOB-Tobramycin, CIP-Ciprofloxacin, LEV-Levofloxacin, TE-Tetracycline, ETP-Ertapenem, F-Nitrofurantoin, NOR-Norfloxacin, GM-Gentamicin, SXT-Trimethoprine/Sulphamethaxole, AML-Amoxycillin, CEC-Cefaclor, ATM-Aztreonam, TGC-Tigercycline.
Table 9 represents the susceptibility of Enterobacter sp. indicating that five different strains of the same organism existed. This microorganism’s strains were resistant to AK, FEP and TE; and mostly susceptible to CAZ, CIP and TZP.
Table 9: - Susceptibility Pattern of Enterobacter in Trinidad and Tobago 2013- 2014
__________________________________________________________________
Enterobacter (74/859)Antibiotics
CAZ CIP ETP SXT TZP TOB IMP GM ATM CXM AK FEP CN TE
__________________________________________________________________
a) S S S S S R S R R R R R R R
b) S S S S S S S R R R R R R R
c) S S S S S R S S S S R R R R
d) S S R R S S R S R R S S R R
e) S S R R S R R R S R R S S S __________________________________________________________________
Footnote: CAZ-Ceftazidime, CIP-Ciprofloxacin, ETP-Ertapenem, SXT-Trimethoprine/Sulphamethaxole, TZP-Zosyn, TOB-Tobramycin, IMP-Imipenem, GM-Gentamicin, ATM-Aztreonam, CXM-Cefuroxime, AK-Amikacin, FEP-Cefepime,CN-Clindamycin, TE-Tetracycline.
Table 10 features the susceptibility of Enterococcus sp. This pathogen had three different susceptibility patterns inferring that three different strains of the same organism existed.
Table 10: - Susceptibility Pattern of Enterococcus spp. in Trinidad and Tobago 2013- 2014
__________________________________________________________________
Enterococcus spp. (64/859)Antibiotic
CEC CXM AMC ETP TZP IPM CAZ CIP CT CN AK
__________________________________________________________________
a) S S S R R R R R R R R
b) R R R S S S R R R R R
c) R S R R R S S S S S S
_________________________________________________________________
Footnote: CEC-Cefaclor, CXM-Cefuroxime, AMC-Augmentin (Amoxicillin/Clavulanic acid), ETP-Ertapenem,TZP-Zosyn,IPM-Imipenem,CAZ-Ceftazidime,CIP-Ciprofloxacin,CT-Colistin,CN-Clindamycin, AK-Amikacin.
Table 11 depicts three susceptibility patterns of Escherichia coli inferring that there is three different strains of the same organism. Two of the strains were multi-resistant to ten or more antibiotics.
Table 11: - Susceptibility Pattern of Escherichia coli in Trinidad and Tobago 2013- 2014
________________________________________________________
Escherichia coli (58/859)Antibiotics
CF CN SXT AMP AMC AML ATM CEC CAZ CIP E ETP GM IPM TZP FEP TGC
________________________________________________________
a) S S S S S R R R R R R R R R R R R
b) R R S R S S S S S S S S S S S R R
c) R R R R R S S R R R R R R R S S S
_______________________________________________________
Footnote: CF/KF-Cephalothin, CN-Clindamycin, SXT-Trimethoprine/Sulphamethaxole, AMP-Ampicillin, AMC-Augmentin (Amoxillin/Clavulanic acid), AML-Amoxycillin, ATM-Aztreonam, CEC-Cefaclor, CAZ-Ceftazidime, CIP-Ciprofloxacin, E-Erythromycin, ETP-Ertapenem, GM-Gentamicin, IPM-Imipenem, TZP-Zosyn, FEP –Cefepime, TGC-Tigercycline.
Table 12 shows two susceptibility patterns for Proteus sp. indicating that two strains of the same organism existed. The two strains were resistant to F and SXT and sensitive to TZP.
Table 12: - Susceptibility Pattern of Proteus spp. in Trinidad and Tobago 2013- 2014
_____________________________________________
Antibiotic Profile of Proteus spp. (22/859) Antibiotic
CAZ CIP CN TZP AMC CEC GM IPM NOR F SXT
____________________________________________
a) S S S S R R R R R R R
b) R R R S S S S S S R R
____________________________________________
Footnote: CAZ-Ceftazidime, CIP-Ciprofloxacin, CN-Clindamycin, TZP-Zosyn, AMC-Augmentin (Amoxicillin/Clavulanic acid), CEC-Cefaclor, GM-Gentamicin, IPM-Imipenem, NOR-Norfloxacin, F/M-Nitrofurantoin, SXT-Trimethoprine/Sulphamethaxole.
Table 13 represents seven (7) distinct susceptibility patterns of Serratia marcescens, indicating that seven (7) different strains of the same organism existed. All strains were resistant to AML, AMC and CEC. Most strains were sensitive to ATM, CAZ, TZP and CIP. Six of Seven (6/7) strains were resistant to TGC, CEC, CT, LEV, IMP and PIP.
Table 13: - Susceptibility Pattern of Serratia spp. in Trinidad and Tobago 2013- 2014
__________________________________________________________________
Serratia spp. (21/859) Antibiotic
ATM CAZ FEP CIP CN TZP TE AK TOB AML AMC CEC SXT GM TGC CT LEV IMP PIP ETP
________________________________________________________________
a) S S S S S S S R R R R R R R R R R R R R
b) S S S S R S S S S R R R R S R R R R R R
c) S S R S R S R R R R R R S S R R R R R R
d) S R R R R R R S R R R R R R R R R R R R
e) S S S S R S S R R R R R R S S R R R R R
f) S S R S R S R R R R R R S S R S R R R S
g) R R S R R R R R S R R R S R R R S S S R _____________________________________________________________
Footnote: ATM-Aztreonam, CAZ-Ceftazidime, FEP-Cefepime, CIP-Ciprofloxacin, CN-Clindamycin, TZP(PIP/TAXO)-Zosyn, TE-Tetracycline, AK-Amikacin, TOB-Tobramycin, AML-Amoxycillin, AMC-Augmentin (Amoxicillin/Clavulanic acid), CEC-Cefaclor, SXT-Trimethoprine/Sulphamethaxole, GM-Gentamicin, TGC-Tigercycline, CT-Colistin, LEV-Levofloxacin, IMP-Imipenem, ETP-Ertapenem.
Table 14 depicts one susceptibility pattern for Providencia stuartii sp. indicating that one strain of the organism existed. This pathogen was sensitive to the three antibiotics (AK, TGC and MEM) tested.
Table 14: - Susceptibility Pattern of Providencia Stuartii (14/859) in Trinidad and Tobago 2013- 2014
_______________________
AK TGC MEM
_______________________
a) S S S
_______________________
Footnote: AK-Amikacin, TGC-Tigercycline, MEM-Meropenem
Table 15 features two (2) different susceptibility patterns of the Stenotrophomonas maltophilia inferring that two (2) different strains of the same organism existed.
Table 15: - Susceptibility Pattern of Stenotrophomonas maltophilia (14/859) in Trinidad
and Tobago 2013- 2014.
_____________________________
AK TGC MEM CAZ LEV SXT
_____________________________
____________________________
Footnote: AK-Amikacin,TGC-Tigercycline,MEM-Meropenem,CAZ-Ceftazidime,LEV-Levofloxacin,SXT-Trimethoprine/Sulphamethaxole.
Table 16 shows one susceptibility pattern for Streptococcus sp. inferring that one strain of the organism was present.
Table 16: - Susceptibility Pattern of Streptococcus spp. (10/859) in Trinidad and
Tobago 2013- 2014.
____________________________
GM TZP MEM CAZ FEP
____________________________
a) S S S S S
____________________________
Footnote: GM-Gentamicin, TZP-Zosyn, MEM-Meropenem, CAZ-Ceftazidime, FEP-Cefepime.
Table 17 depicts two (2) susceptibility patterns of the Citrobacter koseri indicating that there are two (2) strains of this organism circulating at regional hospital in Trinidad and Tobago. Both strains were resistant to AMP and TE and sensitive to TZP and CIP.
Table 17: - Susceptibility Pattern of Citrobacter koseri (6/859) in Trinidad and Tobago 2013- 2014.
_____________________________________________________________
SXT TZP F NOR AMC CEC CXM CN CIP ATM CAZ GM TOB AMP TE
____________________________________________________________
Footnote: SXT-Trimethoprine/Sulphamethaxole, TZP-Zosyn, Nitrofurantoin, NOR-Norfloxacin, AMC-Augmentin (Amoxicillin/Clavulanicacid), CEC-Cefaclor, CXM Cefuroxime, CNClindamycin, CIP-Ciprofloxacin, ATM-Aztreonam, CAZ-Ceftazidime, GM-Gentamicin, TOB-Tobramycin, AMP-Ampicillin, TE-Tetracycline
Table 18 features two (2) susceptibility patterns of Alcaligenes sp. indicating that two strains of the same organism were present. This pathogen was sensitive to CAZ, CIP and TZP.
Table 18: - Susceptibility Pattern of Alcaligenes (6/859) in Trinidad and Tobago 2013- 2014.
______________________
CAZ CIP TZP SXT TOB CN TE
______________________
a) S S S S R R R
b) S S S R S S S
_____________________
Footnote: CAZ- Ceftazidime, CIP-Ciprofloxacin, TZP-Zosyn, SXT-Trimethoprine/Sulphamethaxole, TOB-Tobramycin, CN-Clindamycin, TE-Tetracycline.
Table 19 represents one (1) susceptible pattern inferring that only one (1) strain of the Morganella morgannii organism was present. This strain was sensitive to all antibiotics tested.
Table 19: - Susceptibility Pattern of Morganella morgannii (4/859) in Trinidad and
Tobago 2013- 2014.
_____________________
ATM FEP CIP GM IPM TZP
_____________________
a) S S S S S S
_____________________
Footnote: ATM- Aztreonam, FEP-Cefepime, CIP-Ciprofloxacin, GM-Gentamicin, IPM-Imipenem and TZP-Zosyn.
Table 20 depicts one (1) susceptibility pattern inferring that Burkholderia (P) cepacia has only one strain present at the research sites. It was resistant to AK, CIP, GM and TE and sensitive to many antibiotics.
Table 20: - Susceptibility Pattern of Burkholderia (P) cepacia (4/859) in Trinidad and
Tobago 2013- 2014.
__________________________________________________________________
CAZ FEP TZP TGC TOB SXT AK CIP GM TE
____________________________________________________________
a) S S S S S S R R R R
________________________________________________________________
Footnote: CAZ-Ceftazidime, FEP-Cefepime, TZP-Zosyn, TGC-Tigercycline, TOB-Tobramycin, SXT-Trimethoprine/Sulphamethaxole, AK-Amikacin, CIP-Ciprofloxacin, GM-Gentamicin, TE-Tetracycline.
Table 21 shows the simplified criteria for surveillance of nosocomial infections. It serves as a practical guide for diagnosis and management of different types of nosocomial infections [61].
Table 21: Simplified Criteria for Surveillance of Nosocomial Infections by World Health Organization (WHO).
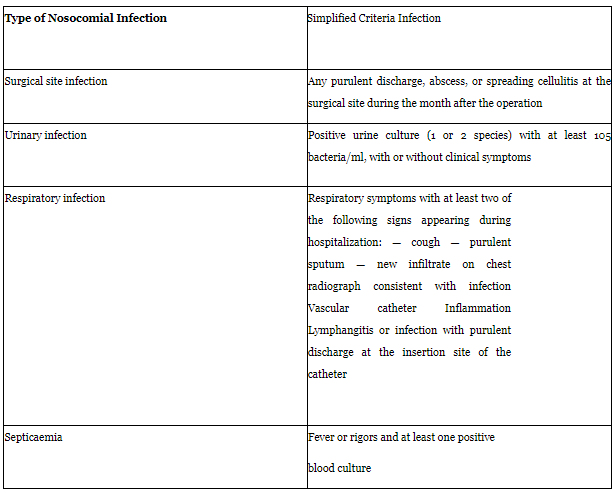
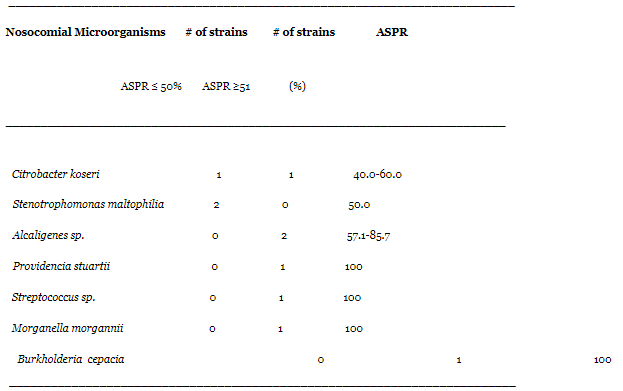
Table 22 features the different antimicrobial susceptibility pattern rates (ASPR) for each pathogen. Strains of Staphylococcus sp. showed low susceptibility pattern that range between 5.6% and 50% indicating the presence of multidrug resistance. Most strains isolated have an ASPR below 50% and this is worrisome for the management of hospital-acquired infections. This stresses the necessity of good hygiene practices and caution in the misuse of broad-spectrum antibiotics and new generation antimicrobials for the treatment of minor bacterial infections. All strains of Acinetobacter sp. (15.0%-40.0%), Serratia marcescens (10.0%-45.0%) and Klebsiella sp. (10.0%-45.0%), as shown in the table have an ASPR below 50%, which is the cut-off point established based on the availability of antimicrobials. On the other hand, Providencia stuartii, Streptococcus sp., Morganella morganii and Burkholderia cepacia were susceptible to the 100% of antibiotics used in the antibiogram. It is good news that these pathogens have yet not develop antibiotic resistance, since they have started becoming more prevalent in the hospital facilities. Multidrug resistant strains of Providencia stuartii [77], Streptococcus sp. [78], Morganella morganii [79] and Burkholderia cepacia [80] have been reported. Antibiotic resistance can be acquired by horizontal transfer of a resistance gene or mutation and generally an acquired mechanism results in a predictable increase in phenotypic resistance [78]. A surveillance programme is in place at the 3 regional hospitals to monitor susceptibility patterns of these microorganisms, to delay antibiotic resistance in the future. The fact that antibiotic resistance has not been developed for these four (4) pathogens represents a success of the institutional antimicrobial stewardship.
Table 22: Antimicrobial Susceptibility Pattern Rates (ASPR) for Nosocomial Pathogens
Isolated at Three (3) Regional Hospitals in Trinidad and Tobago during the Period June 1st, 2013 to May 31st, 2014.
In Trinidad and Tobago information on nosocomial infections are lacking. Orrett, 2002 documented that 7,158 hospital acquired infections were observed from 72,532 patients. High nosocomial rates were observed in the intensive care unit (ICU) (67/100), urology (30/100), neurosurgery (29.5/100) and new-born nursery (28.4/100) wards. Nosocomial urinary tract infections (4.1/100) accounted for the majority of nosocomial infections (42%), followed by post-operative nosocomial wound infections (26.8%) having a nosocomial rate of 2.6/100 [9]. The researcher observed from the research that the incidence of nosocomial infections was 5.8% which was lesser when compared to Benin, another developing country, whose incidence was 19.1% [6, 26]. There were other nations (developing countries) with higher incidences when compared to the researcher’s findings [27].
The age of patients who had nosocomial infections ranged from eight (8) days old to ninety- six (96) years old. Neonates were more susceptible of acquiring nosocomial infections (108/450; 24%) and this was due to their weak immune system. It was reported in the literature that children, who developed nosocomial infections had a three-fold increase in hospital stay (27 days versus 9 days, p<0.001) compared to those who did not [14]. An increased expression of cytokine genes (IL1B and IL10) was observed in patients, who developed nosocomial infections, in addition to a pro-apoptosis pattern due to a lower expression of BCL2. CD3D, a key TCR co-factor that was found significantly down-modulated in children, which developed nosocomial infections [34]. Frequency of nosocomial cases amongst elderly inpatients were higher than other age group, and this was supported by several studies [35-42], which reported that it may be due to risk factors such as impaired immunity, chronic diseases, medications, malnutrition, and functional impairments, among others.
This study showed that surgical wards had the highest nosocomial infection rate (33.8%). But in a surgical emergency department was verified or suspected aspiration as the most important risk factor for the development of nosocomial infection [43] and we agreed with that. Another research showed that the highest surgical site infection (SSI) incidence was after dirty surgery and was 17.8% (102 out of 574) in patients living in high human development index (HDI) countries. Patients in middle-HDI countries had an incidence of 31.4% (74 out of 236), and the poorest countries had an incidence of approximately 40% (72 out of 181) [44]. The use of prophylactic antibiotics for the prevention of SSI has been cited but it may not be available for third world countries [45]. This data indicate that poverty and hospital environment are also risk factors for nosocomial infections and we stressed the need of measures to control and prevent infections from pathogens that live in the hospital microbiota. In addition, a high incidence of nosocomial infection (28.15%) was seen in intensive care units in a study carried out in Ethiopia, where the risk of nosocomial infection was found to be higher in patients with chest tube, on mechanical ventilation or underlying diseases [2, 46].
Skin and soft tissue infection was the most frequent type of nosocomial infection shown in this study, accounting for 37.3% (168 out of 450). It was reported that the most frequent clinical syndromesin 174 infection episodes in patients ≥65 years old were osteoarticular (40%) and skin and soft-tissue infections(30%) in a research aiming to study the frequency distribution of syndromes in the elderly, where bacteraemia was found in 46% of the skin and soft tissue nosocomial infections [47]. Despite the considerable effort devoted to observing each ward, it is of vital importance that key focus be placed on the surgical, medical and paediatric facilities, where the nosocomial cases were highest. Another aspect of great interest is to put special attention in sterilizing surgical tools, frequent hand washing and changing of gloves as often as possible. ReichmannDE &GreenbergJA, 2009 reported that patient skin preparation in the operating room, usage of chlorhexidine- based preparations, pre-operative hand/forearm antisepsis, hair removal, etc. should be considered for safe procedures, when carried out on the surgical wards to reduce the nosocomial rate [48].
In this investigation Staphylococcus sp. (22.4%; 193/859) and Pseudomonas aeruginosa (12.6%; 109/859) organisms were one of the principal gram-positive and gram-negative nosocomial pathogens respectively connected with hospital acquired infections during the research period. The cumulative occurrence of multi-drug-resistant Staphylococcus sp. and Pseudomonas aeruginosa strains were alarming as effective antibiotic choices were severely limited. Other frequently associated multidrug resistant nosocomial organisms included Acinetobacter sp. (11.8%; 101/859) and Klebsiella sp. (11.6%; 100/859). In addition, Klebsiella and Staphylococcus sp. were the most frequently observed causative organisms in nosocomial bloodstream infections in our investigation. Several scientists studied nosocomial bloodstream infections caused by Pseudomonas sp. in new-borns and concluded that they were very frequent in neonates and a cause of bacteraemia and mortality, which may be due to low birth weight, underlying disorders and invasive procedures as predisposing factors [49-50]. Other authors published the most commonly isolated microorganisms in new-born ICU in another research. It was Klebsiella sp. (39.6%) followed by Pseudomonas aeruginosa (11.3%) and coagulase-negative staphylococci (9.4%) [7-8, 51]. Our results along with what has been previously reported in the literature suggest that gram-negative bacteria (especially P. aeruginosa and Klebsiella sp.) play an important role in the pathogenesis of nosocomial infections in neonates admitted in ICU. The neonate’s immune system is not mature enough to fight off these infections caused by these organisms and thus linked to their virulence factors create a perfect scenario for bacteraemia, septic shock and other complications [4, 15].
Nosocomial skin and soft tissue infections (SSTI) and bloodstream infections (BSI) were the most common types of nosocomial infections with occurrences of 37.3% and 28.4% respectively, but their incidence can be dropped by good hygiene practices, and this has been observed by other authors [72-75]. These infections were commonly transmitted via direct contact. Respiratory tract infections (RTI) and bloodstream infections (BSI) were observed to be most frequently associated on the medical wards. Also, BSI was mostly observed on the paediatric medical wards, whereas skin and soft tissue infection (SSTI) was most frequently observed on the surgical wards. Nosocomial central nervous system infections and nosocomial urinary tract infections were more commonly observed on the medical facilities followed by surgical wards. Nosocomial urinary tract infection was least observed on the gynaecology wards. Candida albicans, Enterobacter and Escherichia coli isolates were most commonly observed in urinary tract infections. Of the susceptibility test results, Amoxicillin (AML), Amoxicillin/Clavulanic acid (AMC), Cefaclor (CEC), Cefuroxime (CXM), Ampicillin (AMP) and Trimethoprine/Sulphamethazole (SXT) were observed of being the most frequently resistant antibiotics in this study. Resistance of these antibiotics were commonly observed for the following nosocomial pathogens: Acinetobacter, Klebsiella,
Staphylococcus, Enterobacter, Escherichia coli, Serratia sp. and Citrobacter koserii organisms. In the literature has been published that the highest resistance rate was against Ciprofloxacin and Imipenem in Iran [52]. A total of eight multi-resistant strains of gram-negative bacteria with ESBL-production were detected in five E. coli and three K. pneumoniae strains at the Albert Schweitzer hospital in Gabon. However, four were resistant to the whole spectrum of antibiotics available [27]. Van der Zee Aet al (2014) reported that the resistance to Carbapenem antibiotics is emerging worldwide among Enterobacteriaceae and they developed a PCR technique for identification of carbapenemase genes: blaOXA-48, blaVIM, blaIMP, blaNDM and blaKPC in cultures of broth rectal swabs [53]. Lin et al (2014) reported that Tigecycline non-susceptible K. pneumoniae bacteraemia may suggest a critical problem that caused high mortality of patients at a medical centre in Taiwan over a 3-year period. It was divulged that resistance to commonly used antibiotics was observed in up to 80% of the isolates in Malawi [54].
However, Pseudomonas aeruginosa, Acinetobacter and Klebsiella were observed to be most frequently susceptible to Imipenem, Amikacin, Ciprofloxacin, Gentamicin and Cefepime. Quinupristin (QD) was observed to be most commonly susceptible for methicillin-resistant coagulase negative Staphylococcus (MRCNS) organisms and Clindamycin, Rifamficin, Tigercycline, Vancomycin and Linezolid were also commonly observed to be effective for methicillin-resistant coagulase negative Staphylococcus (MRCNS) isolates. Sulphamethazole was frequently observed to be susceptible for Citrobacter koserii, Stenotrophomonas maltophilia and Alcaligenes sp. In contrast Sulphamethazole was least susceptible for Burkholderia (P) cepacia isolates. Piroth Let al, 2014 reported that E. coli were susceptible to third-generation Cephalosporins and amoxicillin-clavulanate in 89.5% and 62.5% of cases, respectively. No single antibiotic allowed antimicrobial coverage of more than 60% in 190 cirrhotic patients in France [55]. Natoli Set al, 2009 reported that bacteraemia caused by Coagulase negative Staphylococci remained susceptible to Linezolid, Daptomycin and Tigecycline in Italy [56].
In this study inpatients were more likely of being associated with nosocomial infections due to inconsistency in sanitizing work areas, lack of proper ventilation on some wards, irregularity in changing long term use of invasive devices such as urinary and central venous catheters, long term stays in hospitals and previous hospitalization exposure. Patients acquired nosocomial infections either endogenously or from external environment (exogenously). Endogenous nosocomial infections were because of opportunistic pathogens residing in or on external surfaces of patients and brought on by conditions present at or as a direct outcome of events on the wards. In contrast, exogenous hospital acquired infections were the result of pathogens being transmitted by patients as they are shed from numerous thresholds of exit while the patients were hospitalized. Zilberberg MDet al, 2014 reported several risk factors that predispose to recurrent Clostridium difficile infection including use of certain antimicrobial such as Fluoroquinolones and IV Vancomycin after completion of C. difficile treatment, community-onset healthcare associated infection, ≥2 hospitalizations within prior 60 days, age and gastric acid suppression [11, 57].
Among the reported risk factors for colonization by extensively drug-resistant P. aeruginosa in immunocompromised patients, the unnecessary use of antibiotics, particularly ciprofloxacin was reported; and when using medical devices, it was suggested that a high standard of infection control measures must be achieved [28, 58, 76]. YamakawaKet al, 2011 reported that Healthcare-associated methicillin resistant Staphylococcus aureus infection in ICU patients causes high mortality, which is associated to risk factors such as intubation, treatment with antibiotics, open wound, and steroid administration, all occurring within 24 hours of ICU admission [12-13, 59].Vasudevan Aet al, 2014 agreed with previous authors that the global increase of resistant gram-negative bacilli infections in ICU are due to various risk factors and the most important one is the widespread use of empiric broad spectrum antibiotics [1, 60].
In this study the infection control measures practiced at the health care facilities as recorded from patient’s dockets during weekly surveillance included: isolation of MRSA patients. These individuals were separated from others to avoid non-affected inpatients becoming contaminated. It was observed wearing gloves and face masks by the barrier nurses when attending to MRSA patients. Other infection control measures that were observed at the health care facilities included strict observance of contact precautions, ventilatory support, and use of antibiotics, analgesia, fluid resuscitation and frequent cleaning of infected wounds with Lysol. All were part of the management of the sick documented by health care professionals. In addition, it was advised that indwelling catheters be changed frequently to prevent persistence and reoccurrence of infections.
Nosocomial Infections pose serious health problems or challenges to patient well-being. Therefore, CDC provides world-wide guidance in close watch, outbreak surveys, laboratory research and prevention of nosocomial infections. CDC uses awareness acquired through these campaigns to spot infections and develop and implement new plans to prevent and reduce nosocomial infections. Public health action by CDC and other healthcare partners demonstrated great improvements in clinical practice, medical methods and the continuing growth of infection control guidance and prevention accomplishments.
Hospitals should comply with all sanitization protocols comprising uniforms, fumigating equipments, washing and other pre-emptive procedures. Proper hand washing along with usage of alcohol rubs by all health care staff prior to and after each patient contact is one of the most effective ways of fighting hospital-acquired infections. These measures have been observed by other researchers [62-68]. Furthermore, some health personnel have challenged the idea that the stethoscope, may essentially be a path for transmission of nosocomial infections. In a research of a hundred and fifty (150) health care staffs, fifty (50) paramedics, fifty (50) nurses, and fifty (50) doctors, Staphylococcus sp., mostly coagulase negative were cultured from 89% of the participant’s stethoscopes with the average amount of colony forming units increased, when the stethoscopes were not sanitized [5, 69]. In general, 48% of health care workers cleaned their stethoscopes each day or week, 37% each month, 7% annually and 7% had never cleaned them. Cleaning the stethoscope caused an immediate decline in the bacterial count by 94% with alcohol swabs, 90% with a non-ionic detergent, and 75% with antibacterial soap [69]. With regards to ventilators, which may be an aid to prevent the risk of hospital-acquired pneumonia infections by controlling hospital internal air quality must be a fulfilled requirement at the most suitable areas. To an extent nosocomial infection can be lessened to strengthen this point as reported by [70].
Cautious use of antibiotics is crucial. Despite sanitation guidelines, patients can become susceptible of acquiring hospital-acquired infections and they are often given alternative antibiotics in controlling infections that may amplify the range for the appearance of resistant strains. In addition, sterilization is further than sanitizing; it destroys all pathogens on medical devices and surfaces via contact with chemicals, ionizing radiation, dry heat or steam under pressure. Safety measures must be implemented to avoid spread of pathogens by regular paths in health care facilities.
Practicing of hand washing is the solitary way of minimizing the hazards of spreading skin pathogens between patients or from one spot to another on the same patient. Frequent hand washing as often between contacts with patients and after contact with blood, body fluids, secretions, excretions, and equipment or items infected by these pathogens is a vital constituent of infection management and isolation preventative measures. The transmission of hospital-acquired infections, among immunocompromised patients is linked with health care staff’s hand infectivity in nearly 40% of cases and it is a difficult predicament in the modern health care facilities. The most appropriate application for staffs to conquer this challenge is performing proper hand-hygiene actions.
Therefore, the World Health Organization (WHO) initiated in 2005, the Global Patient Safety Challenge. The objective of hand sanitation is to eradicate the transitory flora with proper act of hand washing, with various types of soap; customary and antibacterial and alcohol-based gels. The major challenges observed in the performance of hand sanitation are associated with the inadequacy of sinks, lengthy time and act of hand washing procedures. A simple way in resolving this issue can be using alcohol-based hand rubs, since, it is a quicker process in contrast to accurate hand washing [71].
Consistency in performing good hygiene practices is vital for reducing the high nosocomial rate found at the research sites. Prediction of these infections is very important as a part of clinical surveillance programs to take preventive measures in advance. ASPR showed that only 8.3 % (5/60) of the isolates were antibiotic-susceptible strains.
This study was self-sponsored. I would like to thank Alexander Elliott for the financial support making this project a reality and God for His sustaining grace throughout the successful completion of this research.
COMPETING INTERESTS
All authors declare that they have no competing interests.
CE made contributions to the study design, data acquisition, analysis and interpretation of data. She also drafted the manuscript. AJV took part in analysis, writing up and revision of the manuscript. All authors read and approved the final manuscript.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
