AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Carlos Valencia Calderón, MD, PhD, Department of Neurosurgery, Central University Hospital of Oviedo, Oviedo-Spain.
Citation: Valencia-Calderón C, Calderón-Valdiviezo A, Alvarez-Fernandez B, Rial-Basalo JC, Bernal-Carrillo R, (2019) Neuronavigation as a tool for Pre-surgical Planning in Refractory Epilepsy Surgery. J. Neuroscience and Neurological Surgery.5(1);DOI:10.31579/2578-8868/095
Copyright: © 2019 Carlos Valencia Calderón, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 October 2019 | Accepted: 18 October 2019 | Published: 24 October 2019
Keywords: epilepsy surgery; neuronavigation; pre-surgical planning
Summary
Epilepsy is one of the most frequent chronic neurological pathologies, with high incidence and prevalence worldwide. A third of these patients are resistant to treatment, which is known as refractory epilepsy. Most of these patients suffer epilepsy secondary to epileptogenic lesions, where the surgery is the only treatment that could cure epilepsy. The goal of epilepsy surgery is to remove the epileptogenic area with preservation of eloquent areas, and here the surgical experience, the neuroimaging technology and the availability of image-guided surgery systems known as a neuronavigator plays a key role.
Objectives: To demonstrate the usefulness of neuronavigation in pre-surgical planning and in the surgery of refractory epilepsy.
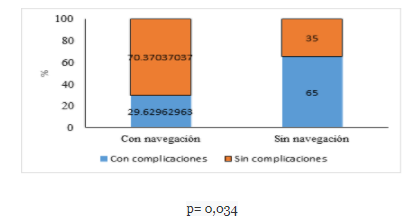
Method: A cross-sectional and analytical descriptive study was conducted based on 47 surgeries performed (12 resective, 32 palliative and 3 diagnostic) in patients with refractory epilepsy and mean age of 9.93 years (SD 4.1). In 27 patients (57.44%) the neuronavigator was used. In the group of patients operated with neuronavigation, the surgical time decreased by 47.17 minutes (p = 0.022), the amount of bleeding by 111.41 milliliters (p = 0.011) and the days of hospitalization by 6.68 days (p = 0.005), compared with the group operated without neuronavigation. Complications in the neuronavigation group were 29.63% compared to 65% in the group operated without neuronavigation (p = 0.034).
Conclusions: In our series, the use of the neuronavigator in the planning and development of the surgery had a significant impact by reducing the amount of bleeding lost, the surgical time, the days of hospitalization, and the post-surgical complications.
Epilepsy is one of the most frequent chronic neurological pathologies, with an incidence of 50 / 100,000 / year and a prevalence between 0.5 and 2% worldwide [1,2]. A third of these patients are resistant to treatment with antiepileptic drugs [3]. ILAE defines refractory epilepsy as “one in which there has been a failure to 2 trials of antiepileptic drugs (FAE), in monotherapy or in combination, tolerated, appropriately chosen and appropriately used, to achieve the sustained absence of crisis” [4,5].
Most of these patients suffer from focal epilepsy secondary to epileptogenic lesions, increasingly evidenced in direct correlation with the new brain neuroimaging techniques [6]. Epilepsy surgery is the only treatment that could cure epilepsy in patients with refractory epilepsy. This option should be considered as soon as drug resistance is evident, as several studies have shown that patients with active epilepsy have a mortality three times higher than the general population (7). In well-selected patients, epilepsy surgery is highly effective, obtaining freedom of crisis of up to 84%, depending on the experience of surgeons and the technology available in their centers (8). The aim of epilepsy surgery is to remove the epileptogenic area with preservation of eloquent areas, and it is here that surgical experience and neuroimaging technology play a key role [9].
Images in the Preoperative Evaluation of Refractory Epilepsy.
The basic protocols for the acquisition of images in epilepsy were defined by the International League against epilepsy (ILAE) [4]. In the last 20 years there has been an important technological development in the area of epilepsy imaging, especially in the field of nuclear magnetic resonance, such as improvements in the equipment of 3 teslas and even 7 teslas, which have revolutionized the approach of these patients finding injuries that went unnoticed with 1.5 tesla equipment [10]. Magnetic resonance, both structural and functional, is the imaging modality of choice to determine and delimit the epileptogenic zone, as well as to define the surrounding structures.
These studies obtained in DICOM format allow the analysis of the images in the workstations of the neuronavigation teams.
Neuronavigation
In the last two decades, the evolution of neuroimaging techniques, both structural, functional and neuronavigation, have proven useful in pre-surgical planning of refractory epilepsy [11]. Neuronavigation consist of a sophisticated computer technology concerning software and hardware, that processes digitized neurorradiological images in DICOM format (process called planning), interacting and matching point by point imaging data with the real anatomical structures of the patient obtaining a neuroanatomic imaging map in 3D through a process called registration.
Accuracy and safety when locating the lesion, choosing the best route or path to address it without damaging adjacent tissues, reducing surgical instrumentation time and radical removal of the lesion are some of the advantages of this technique.[11].
Stereotactic location is a neurosurgical technique capable of achieving the location and approach of any intracranial point or target through a system of x, y, z coordinates, through a device that is attached to the patient's head and guided by tomography images Axial computational (CT), magnetic resonance image (MRI), angiography, or positron emission tomography (PET).
The main disadvantage of navigation systems is the well-known brain shift or cerebral movement that is caused by cerebral edema, secondary to cerebral decompression or after cerebrospinal fluid drainage, which produces a calculation error due to this displacement, which can be corrected with the acquisition of intraoperative images of Ultrasound, CT or MRI, with systems that are compatible with neuronavigation equipment, which would allow visualizing changes in real time [12].
For intraoperative use, neuronavigation systems must relate the physical location of a patient to the preoperative models through a transformation that relates the two paradigms through patient-to-image mapping [12]. The main components of any neuronavigation system are a location device which will track the position of the patient and the surgical tools, a computer console that will present the information of the acquired images and finally accessories such as navigation probes and Frameworks.
The use of neuronavigation in lesion refractory epilepsy has not yet been adequately standardized. The objective of this work is to demonstrate the usefulness of neuronavigation in the pre-surgical planning of refractory epilepsy based on the experience acquired in the five years of use of neuronavigation in epileptic patients in our center.
Materials and Methods
A descriptive cross-sectional and analytical study that reviewed the data of patients with refractory epilepsy who were operated in our hospital with or without neuronavigation was conducted. Our hospital is a national reference pediatric center located in a city with a population of 2,576,287 inhabitants, and 723,073 inhabitants under 15 years. Since 2013 the hospital has an epilepsy surgery program and a multidisciplinary committee made up of specialists in neurology, neurosurgery, neurorradiology, neuropsychology, nutrition and neuroendocrinology. During the committee meetings, compliance with the refractoriness criteria, the frequency of the crises, the impact on the quality of life in relation to the crises, the indication of the type of medical and / or surgical, curative or palliative treatment were verified. Likewise, family members were informed of the recommendations issued by the committee and informed consent was obtained.
All patients with refractory epilepsy discussed by the epilepsy committee between January 2013 and December 2016, in total 55 patients, who met the inclusion criteria were included.
Pre-surgical planning was reviewed through neuronavigation, medical records and operative protocols for all cases.
Technology used MRI of the Brain:
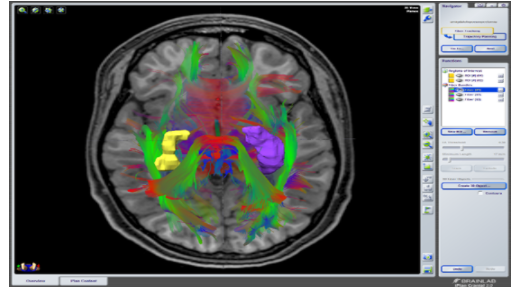
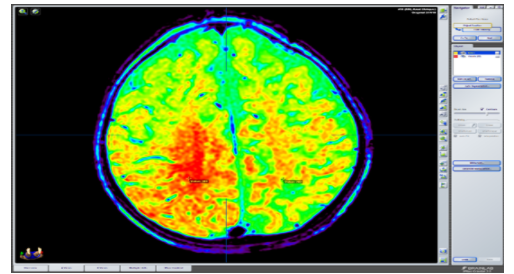
Brain MRI study conducted with a team of 3.0 Phillips brand teslas (Medical Systems, DA Best, The Netherlands), which followed an epilepsy protocol that included simple volumetric T1 and T1 sequences and contrasted contrast with axial, coronal and sagittal cuts of up to a minimum of 0.4 mm thick, T2 and FLAIR; images by diffusion tensor were obtained with a minimum of 16 addresses and were assigned by agreement the colors red, green and blue to the right-left, anterior-posterior and superior-inferior orientations respectively; multivoxel spectroscopy and arterial and venous angio-MRI in all cases. The images were acquired in DICOM format and subsequently transferred to a workstation where the three-dimensional analysis of the study was performed, as well as the pre-surgical planning of each case.
Neuronavigator:
We use a neuronavigator consisting of:
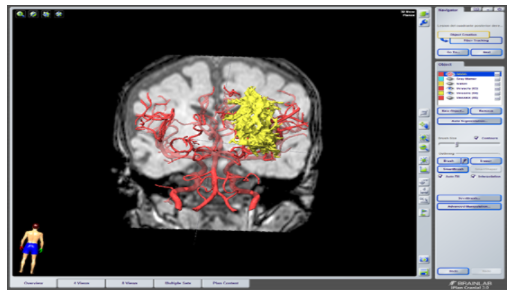
a) a BrainLab Z800 workstation, with the iPlan version 3.0.5 program where images acquired on magnetic resonance were loaded. The trajectories that were to be followed during the surgery were planned and the paths of the cutaneous flap opening, as well as the craniotomy and durotomy were delimited. Objects of images of interest were created, both normal and structural injuries; Vascularization was reconstructed by angio-MRI studies, and tractography of fascicles of interest.
b) In the volumetric analysis we used the function called Automatic Segmentation, which uses a knowledge-based segmentation approach that is capable of identifying brain structures by comparing the patient's images with a set of images from an atlas included in the iPlan, which contains defined anatomical structures. The application finds the direct correspondence between the set of images of the patient and the set of images of the atlas and transfers all the delimited structures of the anatomical atlas to the images of the patient.
c) A function called Fiber tracking of the iPlan 3.0 program was used to study the tractography. This function is based on the measure of diffusion anisotropy in the brain calculated from images of the diffusion tensor (DTI) acquired in several directions. The diffusion direction of the water along the potential fibers of the white substance was calculated for the entire volume explored.
d) The information planned in BrainLab Z800 workstation was transferred to a BrainLab Curve system with dual screen, where the facial and cranial anatomy points of the patient already anesthetized and fixed in the craniostat were registered. Registration was made using an infrared camera and a pointer.
Surgical Planning.
Once the images were presented on the screen of the planning station of the neuronavigator, the lesion, epileptogenic zone, corpus callosum, tonsil, hippocampus were drawn and colored, as well as eloquent or vascular structures of importance. Then the three-dimensional reconstruction was performed, as well as, triplanar (sagittal and coronal sections).
Upon this reconstruction, the desired entry points, target, and trajectories were drawn, immediately visualizing some of the eloquent or vascular structures near the trajectories.
Intraoperative Registration.
Once in the operating room, the patients were placed in a surgical position, with head fixation with a 3-point head (craniostat) (in the hospital they have the Mayfield Modified Skull). Next, a reference star (not sterile) was fixed, on one side or the other depending on the distribution of the operating room and the craniotomy as well. The recording chamber was usually located at the patient's feet usually on the right side. The calibration was performed by moving the cameras until observing the 3 reflective spheres of the star and those of the pointer, by using the camera's own laser. And then the patient's facial and / or cephalic surface was recorded.
Registration was always carried out under non-sterile conditions; the patient's face was placed as far as possible in front of the camera. Through the facial recognition pointer, multiple points of the malar area, orbital flange, superciliary flange, and nose were acquired, since these structures were the least mobile. In this way, a facial scan was performed, which the neuronavigation system used to calculate and obtain a three-dimensional model of the patient's facial anatomy.
Then, this model, which represented the position of the patient's head already in the operating room, was correlated with the diagnostic radiological data, and the registration was completed. To verify the correct registration, the anatomical reference test was performed as a control of the accuracy of the system. The pointer was placed on non-movable structures such as the nasion, tip of the nose and swallow.
Next, we proceeded to locate the point of entry, and delimitation of the cutaneous surface of the region to be resected, to define the limits of the surgical incision and craniotomy. Next, the non-sterile star was removed, aseptic and antiseptic, sterile star placement and sterile fields were performed. And the surgical procedure was continued, using the registration tips or calibrated instruments to be recognized by the navigation system.
Source of data Collection
For the evaluation of the cases, medical records data were used, as well as the external consultation and hospitalization files, as well as data of the patients that were selected by the epilepsy committee, all the imaging studies that were found in the neuronavigator database.
Data Collection Instruments
Data collection sheets created for specific research purposes were made, data were collected from the statistical archives, the medical records and photographic archives available from the patients who were recorded in the Neuronavigator of patients with refractory epilepsy that were discussed in the epilepsy committee of the Baca Ortiz Pediatric Hospital between January 2013 and December2016 and processed in the neurosurgical department of the Central University Hospital of Oviedo.
Statistical analysis of the data: To describe the results of the study variables, descriptive statistics methods were used: for numerical variables the mean and standard deviation were used, for the categorical variables percentages were used. For the analysis of the relationship between variables, non-parametric statistics were used, specifically the comparison of dependent means of numerical variables (crisis frequency and quality of life scale score) was performed using the Wilcoxon test, and the comparison of variables. categorical through the X2 test. Data analysis was performed with the SPSS (Statistical Package for the Social Sciences) version 22.0 (SPSS, Inc., Chicago, IL, USA). Ethical and legal aspects: Since this is a descriptive study and therefore without intervention, it did not require approval by a bioethics committee, although it was approved by the Department of Teaching and Research of the hospital. In collecting data, the physical and emotional integrity of each patient was preserved, as well as their confidentiality. This work has no conflicts of interest with the company BrainLab.
Results
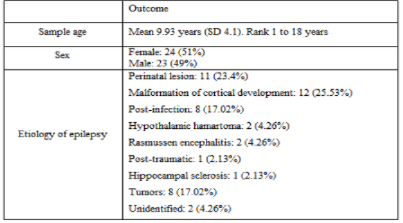
During the years 2013 – 2016, 55 cases of patients with refractory epilepsy were presented in the “Multidisciplinary Committee of Epilepsy” (table 1). For the study, inclusion and exclusion criteria were applied (table 2), obtaining a sample of 47 cases (2 patients were excluded because they had lesions in eloquent areas and 6 requested voluntary discharge) (figure 1-3).
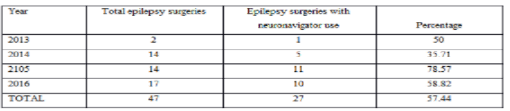
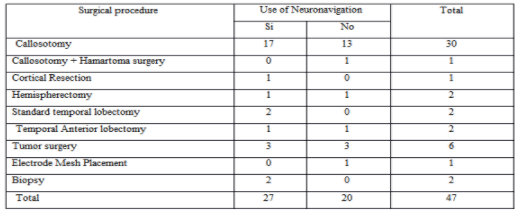
Of the 47 epilepsy surgeries, 57.44% (n 27) were performed with the use of neuronavigation (21 of them were performed in the last two years – 77.78%) (table 3-5).
When comparing the results of surgical time, bleeding during the surgical procedure and days of hospitalization obtained from surgeries performed with and without the use of neuronavigation, we observed that with the use of the neuronavigator, the surgical time decreased by 47.7 minutes (p = 0.022), bleeding in 111.41 milliliters (p = 0.011) and days of hospitalization in 6.68 days (p = 0.05) (table 6).
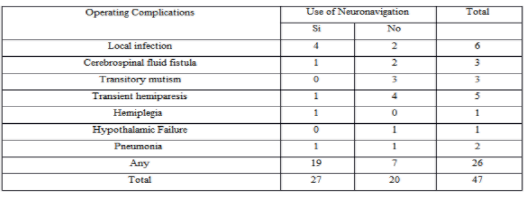
The complications in the neuronavigation group were 29.63% (eight patients) compared with 65% in the group operated without neuronavigation (p = 0.034) (table 7). The complications described were surgical site infection, hemiplegia, transient hemiparesis. Without the use of neuronavigation, 13 patients presented complications (65%). The complications described were motor deficits (hemiplegia, transient hemiparesis, mutism) (Figure 4).
The table 8 describes the absolute frequency of mortality in both groups, being higher in the group operated without neuronavigator. These two deaths were not related to the neuronavigation process (one death due to pneumonia and another due to severe hyponatremia).




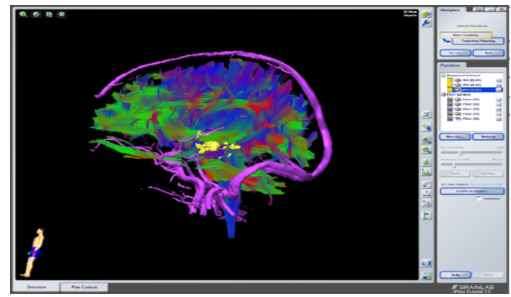
The study of this image has several connotations, such as the location in the space of this lesion, as well as its proximity to the vascular structures and its relationship with the language pathways.


For the performance of any surgical procedure, a sense of three-dimensional spatial perception of the anatomy of each patient is required; Intracranial location is a challenge for all neurosurgeons as they face each patient's own anatomical variations caused by the distortion caused by the underlying pathology, by the limited visual field product of the type of approach, the same location of the lesion, the anatomical complexity of the deeper areas of the brain, vascular relationships, proximity to eloquent areas, etc.
Diagnostic imaging methods based on a three-dimensional (3D) model, greatly facilitated the spatial location of all types of injuries, especially those that are more difficult to access and delimit by their location or distribution. The main link between imaging studies and the anatomy of each patient is due to the integration provided by navigation systems during surgery.
However, not all centers have neuronavigation equipment. In Argentina, in 2016, a series of 43 surgeries were reported without the use of neuronavigation in 10 years [13]. In our center, 20 patients were operated without a browser for computer processes related to the equipment.
In 2014, Valencia et al., Performed 10 callosotomies assisted with neuronavigation; In no case were intraoperative complications reported, concluding that callosotomy guided by frameless neuronavigation is an accurate and safe technique [11].
In Germany, in a series of 28 patients with lesional epilepsy, non-lesion and temporal epilepsy underwent surgery, 11 of them (39.3%) used intraoperative MRI and neuronavigation; better results were obtained in the group that used neuronavigation as an aid in the development of surgery [14].
If we compare the aforementioned studies with our research, in our series a greater number of surgeries were performed in less time (47 surgeries in 4 years), with a higher percentage of neuronavigator utilization (57.44% vs. 39.3% reported by Sommer) [14]. Amandeep Kumar, Sarat Chandra, et al. in 2014 they mention that the use of multimodal neuronavigation (with functional resonance and tractography) together with cerebral mapping with cortical stimulator for resection of lesions on eloquent cortical areas (motor, sensory, language) can reduce the risk of leaving the patient with permanent neurological sequelae and improving the percentage of resection of the affected area [15]. Björn Sommer, et al. In 2015, they describe how the use of intraoperative functional resonance and neuronavigation in ganglioglioma excision, (responsible for causing refractory epilepsy), improves the percentage of tumor resection, and therefore the number of seizures is significantly reduced [16]. In 2016, the same author Björn Sommer, et al, described how resection based on magnetoelectroencephalography with the use of neuronavigation and intraoperative MRI promises to be very useful in the complete resection of epileptogenic areas [17]. Karl Roessler et al. They report in 2016 that neuronavigation along with intraoperative MRI proved to be very useful in performing epilepsy surgery since it was associated with better resection of compromised cortical areas, with fewer complications and with better crisis control [18]. A systematic review carried out in Brazil in 2015 by Sovenso mentions that only one of the 28 studies analyzed reports that there was no significant difference in surgical time compared to the use or not of neuronavigation (239 vs 208 minutes). Four other studies analyzed only describe the mean surgical times with the use of neuronavigation (212 min, 213.3 min, 243 min and 213 min) [19]. If we compare our study where the average surgical time was 198 minutes for the group that used neuronavigation, we see that the surgery time was shorter than the studies analyzed.
The Department of Neurosurgery of the School of Medicine of the University of Osaka Japan, Haruhiko Kishima et al. published in 2017 the utility of neuronavigation in the performance of selective amygdalohippocampectomy via infratemporal cortex, with excellent results in crisis control and memory preservation because the lobe is not damaged by the guidance of the neuronavigator during the surgical procedure temporary [20].
Regarding postoperative complications, in the Aberastury series of 43 patients operated without navigation, it reports 19 patients with new postsurgical neurological deficits of which 14 were permanent, 4 cases of post-surgical hydrocephalus, 7 cases of surgical site infections [13]. In our series, with the use of a neuronavigator, 9 patients presented neurological deficits, of which 8 were transient, 4 infections of the surgical site, no hydrocephalus was reported.
Roessler from Germany, in his study based on a series of patients operated with the use of neuronavigation does not report deaths, and a low percentage of hemiparesis and pneumonia [18].
In Germany, Delev and colleagues studied 40 patients in whom the use of neuronavigator was used in the planning of patients with apparently non-lesion epilepsy. It was shown that with the correct use of the neuronavigator tools, lesions were identified that were not initially seen on the MRI, and their use during the surgical procedure helped to perform more extensive resections, with better crisis control [21].
In summary, the refractory epilepsy in children is a debilitating condition, which impacts approximately 20 or 30% of the pediatric population that suffers from epilepsy. Epilepsy surgery improves not only the quality of life with crisis control, but it has been shown to improve cognition and behavior in patients undergoing surgery.
The challenge for the neurosurgeon is to translate the data from neuroimaging and neurophysiology recordings into a 3D space for surgical resection. The generation of a planned resection area clarifies the surgical strategy and gives the surgeon confidence that the proposed resection is complete [22].
Conclusions
We can conclude that since 2013 there has been a gradual increase in surgery for the control of refractory epilepsy with the use of neuronavigation as an aid in the development of surgeries; The use of this resource in pre and trans surgery is useful since it reduces the risk of the presence of trans and post-surgical complications associated with the procedure, decreases the surgical time, the amount of bleeding and even the days of hospitalization. Although the performance of epilepsy surgery with the use of neuronavigation has increased, it continues to be underutilized for the treatment of refractory epilepsy.
Recommendations
It is necessary to conduct training in the use of neuronavigation for the planning and development of surgeries for the control of refractory epilepsy. It is essential to establish protocols for diagnosis, evaluation and management of patients with refractory epilepsy, as well as to design a protocol for the use of neuronavigation in pre-surgical planning and its use during the development of epilepsy surgery. Surgery with the use of neuronavigation as a treatment for refractory epilepsy should be considered within the initial management to achieve better control of epileptic seizures.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
