AUCTORES
Globalize your Research

Case Report
*Corresponding Author: Lynnette Mazur, Emeritus Professor, McGovern Medical School, 6431 Fannin Houston, Texas.
Citation: Catherine Yang, Rajan Patel and Lynnette Mazur (2021). Neonatal Gallstones. J Clinical Research and Reports, 8(4); DOI:10.31579/2690-1919/181
Copyright: © 2021 Lynnette Mazur. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 June 2021 | Accepted: 25 June 2021 | Published: 05 July 2021
Keywords: spontaneous vaginal delivery; gestational diabetes; cholelithiasis; transcutaneous bilirubin; down syndrome
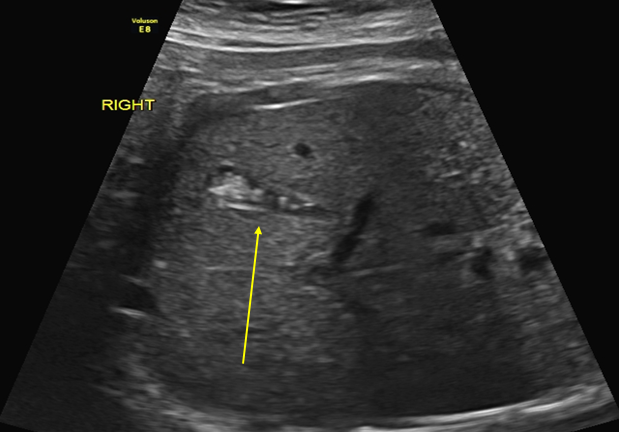
A term male infant was born by spontaneous vaginal delivery to a 23 year old gravida 2 para 2 mother. His weight, length, and head circumference were 2720g (8%), 47cm (6%) and 31.5cm (1%) respectively; the remainder of his physical examination was unremarkable. The pregnancy was complicated by intra-uterine growth retardation, gestational diabetes controlled with glyburide, and gestational thrombocytopenia. The mother had a past medical history of obesity, BMI of 32 (>95%), HPV infection, and atypical squamous cells of the cervix. A fetal ultrasound at 38 weeks gestational age showed echogenic foci consistent with cholelithiasis (Figure 1); a previous US at 37 weeks gestational age was normal. On routine laboratory testing the mother’s blood type was O positive and the infant’s was A+ (positive). His transcutaneous bilirubin was 4.3 mg/dL at 36 hours of life. Both mother and son were discharged after two days without problem.
A term male infant was born by spontaneous vaginal delivery to a 23 year old gravida 2 para 2 mother. His weight, length, and head circumference were 2720g (8%), 47cm (6%) and 31.5cm (1%) respectively; the remainder of his physical examination was unremarkable. The pregnancy was complicated by intra-uterine growth retardation, gestational diabetes controlled with glyburide, and gestational thrombocytopenia. The mother had a past medical history of obesity, BMI of 32 (>95%), HPV infection, and atypical squamous cells of the cervix. A fetal ultrasound at 38 weeks gestational age showed echogenic foci consistent with cholelithiasis (Figure 1); a previous US at 37 weeks gestational age was normal. On routine laboratory testing the mother’s blood type was O positive and the infant’s was A+ (positive). His transcutaneous bilirubin was 4.3 mg/dL at 36 hours of life. Both mother and son were discharged after two days without problem. Figure 1 shows, prenatal ultrasound of fetus at 38 weeks. Arrow indicating gallstones.
At seven days of age the infant was brought to the clinic for jaundice. A transcutaneous bilirubin measured 14.9 mg/dL; the total serum bilirubin was 15.6 mg/dL with a direct measurement of 0.2 mg/dL. He was diagnosed with breast milk jaundice and no intervention was indicated. At a one month follow-up his total serum bilirubin was 12.7 mg/dL with a direct measurement of 0.3 mg/dL. An abdominal US showed no evidence of cholelithiasis or sludge.
At five months of age he presented to the emergency department with vomiting. An abdominal US showed ‘mobile echogenic material consistent with biliary sludge’. (Figure 2) No stones were seen. He was diagnosed with ileus and discharged home. Figure 2 shows, postnatal abdominal ultrasound at 5 months old. Arrow indicates biliary sludge.

With the routine use of ultrasound (US) examinations in obstetric practice, fetal gallstones are occasionally found. In a study of almost 4,000 consecutive third-trimester US studies, 19 (0.42%) fetuses had echogenic material in the gallbladder. Eleven had echogenic foci and eight had biliary sludge [1]. Although the etiology of fetal gallstones and sludge is unknown, increased bilirubin levels may be a factor. Unconjugated bilirubin is insoluble and at higher concentrations forms calcium salt precipitates. Estrogen also plays a role by stimulating cholesterol production and reducing the synthesis of biliary acids [3]. Stone formation can occur once the concentration of cholesterol overtakes the ability of bile to maintain it in solution [4,5]. As bile becomes saturated, cholesterol vesicles form and interact with surrounding proteins such as mucin and crystallize [6,7]. Other risk factors include certain medications and maternal conditions (Table 1) [8,9]. Additionally, children with Down Syndrome are at increased risk [10].

Gallbladder sludge, thought to be the precursor of stones, is composed of calcium, pigment and cholesterol elements (calcium bilirubinate and cholesterol crystals) [11]. Sonographically it presents as diffuse homogeneous echogenic material filling the gallbladder. However, unlike stones that usually cause ‘acoustic shadowing’ or ‘comet tail artifacts’, sludge lacks this sonographic finding. This may be due to small, undetectable stones that are less than 3mm or stones that escape detection because they do not lie in the center of, or in the focal range of, the US beam. Therefore, it is difficult to distinguish sludge from small non-shadowing stones [12]. Additionally, the development of crystals that ultimately become stones is not a uniform process [6,7]. After birth, when the infant begins to feed, increasing plasma levels of cholecystokinin cause the gallbladder to contract and release the viscous material into the duodenum. This resolution may be associated with a colic pain [1].
The short-term prognosis of fetal gallstones is good. More than 70% of patients have spontaneous resolution within two months after birth and more than 90% within six months [1,8]. The prognosis for the resolution of sludge is less clear as not all infants with sludge have a follow-up US. Pharmacologic treatment with ursodeoxycholic acid and laparoscopic surgery have been reported [2,13]. However, the risks of adverse events with medications and surgery and anesthesia in the infant population need to be considered. The long-term prognosis in older children is unclear but there are reports of older children requiring a cholecystectomy for persistent gallstones [14].
Although spontaneous resolution of neonatal gallstones is common in the first year of life, our patient’s US at five months of age showed that the sludge had reappeared. Knowing that sludge may progress to stone formation or that it may represent small ‘non-shadowing’ stones, periodic US will be done until complete resolution is demonstrated. Future studies are needed to determine if this neonatal finding is a risk factor for the development of gallstones in childhood.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.









































