AUCTORES
Globalize your Research

Review
*Corresponding Author: Anthony Kodzo-grey Venyo, Department of Urology, North Manchester General Hospital, Retired Clinician, United Kingdom.
Citation: Anthony Kodzo-grey Venyo, (2024), Myointimoma Of The Penis: Review And Update,Clinical Medical Reviews and Reports; 6(7): DOI: 10.31579/2690-8794/231
Copyright: © 2024 Anthony Kodzo-grey Venyo, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 September 2024 | Accepted: 13 September 2024 | Published: 20 September 2024
Keywords: Myointimoma of the penis; angiocentric myofibroblastic tumour of the penis; penile mass; glans penis; corpus spongiosum; biopsy;
Myointimoma, which is also referred to angiocentric myofibroblastic tumour, is an uncommon benign soft tissue neoplasm which is derived from intimal cells of the vascular spaces of the corpora cavernosa of the penis, histologically typified by multinodular/plexiform myofibroblastic proliferation within the vascular spaces of cavernous bodies of the penis. Myointimoma could afflict children as well as adult males and it does tend to present as a lump or mass upon the penis that had been noticed recently over a few weeks and which recently had been increasing in size or getting larger within the glans penis. Generally, patients who are afflicted by myointimoma tend to be asymptomatic apart from having noticed a lump in the penis. Diagnosis of myointimoma can be confirmed via pathology examination and immunohistochemistry staining studies and molecular and cytogenetics studies of biopsy specimens or excised specimens of the penile tumour. Total excision alone is stated to be sufficient for the management of myointimoma of the glans penis in view of the fact that the tumour tends to portend a benign indolent cause. Less than 30 cases of myointimoma of the penis had so far been reported in the global literature and for this reason, it would be envisaged that most clinicians in the world have never encountered a case of myointimoma of the penis before and they would tend not to be familiar with the presentation, diagnostic features, treatment, and outcome of the tumour ensuing its treatment. The important thing that needs to be appreciated is the fact that myointimoma of the penis which mimics more common lesions of the penis does require careful pathology examination and a high-index of suspicion by the clinician and the pathologist in order to differentiate myointimoma of the penis from its simulants including: plexiform fibrohistiocytic tumour of penis, epithelioid haemangioendothelioma of penis, myofibroma of the penis, intravascular fasciitis of penis, nerve sheath tumour of penis, leiomyoma of penis as well as various other types of lesions afflicting the penis.
Myointimoma, which is also referred to as angiocentric myofibroblastic tumour, is an uncommon benign soft tissue tumour which is derived from intimal cells of the vascular spaces of the corpora cavernosa of the penis, histologically typified by multinodular / plexiform myofibroblastic proliferation within the vascular spaces of cavernous bodies. [1] The terminology of myointimoma was stated to be first introduced by Fetsch et al. [2]in 2000 and it was recognized as a distinctive histological entity in the World Health Organization Classification of the Tumours of the Urinary System and Male Genital Organs in 2016 [3]. It has been iterated that up to Nobember 2022, only 22 cases had been reported in the literature, of which only 10 had been reported in children and adolescents. Except of two small series [2] [4] of cases that had based upon a retrospective re-evaluation of few decades stored slides of tumours, these myointimoma tumours had been stated to be based upon isolated case reports. [1] It has been pointed out that in view of the rarity of myointimoma of the penis, the main importance is to be able to differentiate myointimoma from other tumours of variable biological behaviour. In view of the rarity of myointimoma of the penis, it would be envisaged that majority of clinicians all over the world would not have encountered a case of myointimoma of the penis before. The ensuing article on myointimoma of the penis is divided into two parts: (A) Overview which has discussed general aspects of myointimoma and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to myointimoma of the penis.
AIM
To review and update the literature on myointimoma of the penis.
METHOD
Internet data bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Myointimoma of the penis; Penile myointimoma; Myointimoma of glans penis. Twenty references were identified which were used to write the article which has been divided into two parts: (A) Overview which has discussed general aspects of myointimoma and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to myointimoma of the penis.
RESULTS
[A] OVERVIEW
Top of Form
Bottom of Form
Definition / general statement
Essential features
The essential features of myointimoma had been summated as follows: [5]
Terminology
Some of the terminologies that tend to be used for myointimoma had been summated to include the ensuing: [5]
Epidemiology
The epidemiology of myointimoma had been summated as follows: [5]
Sites
Pathophysiology
Aetiology
Clinical features
The clinical features of myointimoma of the penis had been summated as follows: [5]
Diagnosis
Prognostic factors
Treatment
Gross description
Frozen section description
Microscopic (histologic) description
The microscopy pathology examination features of specimens of myointimoma of the penis had been summated as follows: [5]
Positive stains
It has been iterated that immunohistochemistry staining studies tend to demonstrate positive staining for the ensuing tumour markers: [5]
Negative stains
It has been iterated that immunohistochemistry staining studies tend to demonstrate negative staining for the ensuing tumour markers: [5]
Differential diagnoses
The differential diagnoses of myointimoma of the penis has been summated to include the ensuing: [5]
Cito et al. [15] reported a 49-year-old Caucasian man who had presented with a 12-month history of a palpable, firm, solitary lesion involving his glans penis. During his clinical examination, there was a 1 cm palpable, endophytic well-circumscribed nodule, that was located to the left side of his glans penis, close to his coronal sulcus, with disease-free external urethral orifice. The patient underwent complete excisional biopsy. A skin rhombus that measured 1.1 cm × 0.8 cm × 0.3 cm was removed and the biopsy sample, was fixed in 10% formaldehyde, sent to the pathology department. During his 18-month follow-up visit, he was clinically disease free. Histopathology examination of his excised penile lesion demonstrated a multi-nodular intra-vascular proliferation of the corpus spongiosum. The myointimal proliferation had comprised of bland predominantly spindle cells in an abundant fibromyxoid stroma. Immunohistochemistry staining for smooth muscle actin (1A4), cytokeratins (AE1/AE3, CAM5.2), and CD34 were undertaken utilising the avidin-biotin complex (ABC) immunoperoxidase method. The lesional cells had exhibited positive staining for smooth muscle actin and negative staining for cytokeratins and CD34. Cito et al. [15] made the ensuing concluding iterations:
Casa et al. [6] made the ensuing iterations:
Casa et al. [6] reported four additional tumours of this unique myointimal proliferation. Casa et al. [6] summated the results as follows:
Casa et al. [6] made the ensuing concluding iterations:
Tanriverdi et al. [13] reported an 11-year-old boy, who was referred to Manisa Celal Bayar University Hospital with a nodule upon the left side of his glans penis. The nodule was detected two weeks preceding his assessment and the patient had not had any symptom except for the finding of the penile mass. The mass was located within the left side of his glans and it had measured 10 mm in size (see figure 1). The penile mass was also immobile and painless. The patient had been circumcised when he was 6 years-old. He did not have any history of any trauma or infection. The results of his laboratory tests were within their normal limits. He had ultrasound scan of his abdomen, urinary tract as well as scrotum which was also normal. The tumour was completely excised totally and his glans penis was sutured primarily. It had an irregular border (see figure 2).
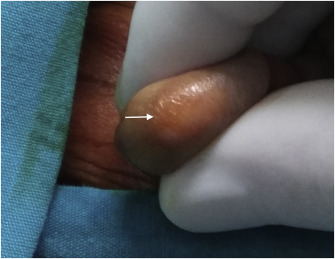
Fig. 1. The nodule in the left side of glans penis (white arrow). Reproduced from: [13] under the Creative Commons Attribution License.

Fig. 2. The nodule excised totally. Reproduced from: [13] under the Creative Commons Attribution License.
Upon histopathology examination, the mass was found to consist of thick, smooth muscle fibres (see figure 3). There were focal fibrotic/fibromyxoid areas and spindle cell proliferation among them (see figure 4). The neoplastic cells had exhibited strongly positive staining with actin and weakly stained with desmin upon immunohistochemistry staining studies. (see figure 5). All of these aforementioned pathological findings were evaluated as myointimoma. In the first year of follow-up, the patient did not have any problem regarding his penis or other urinary tract organs.
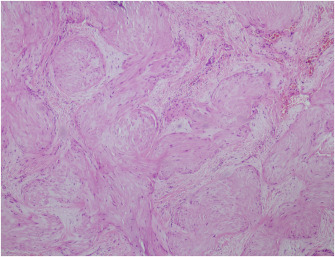
Fig. 3. Thick, smooth muscle bundles (HE, x100). Reproduced from: [13] under the Creative Commons Attribution License.
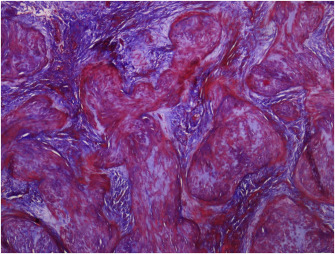
Fig. 4. Focal fibrotic/fibromyxoid areas among smooth muscle fibers (Masson-trichrome, x100). Reproduced from: [13] under the Creative Commons Attribution License.
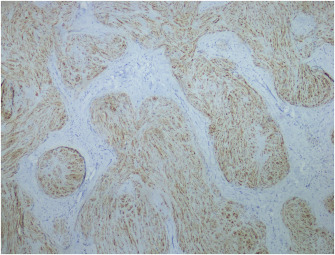
Fig. 5. Strongly staining with actin (Actin, x100). Reproduced from: [13] under the Creative Commons Attribution License.
Tanriverdi et al. [13] made the ensuing educative discussion:
Tanriverdi et al. [13] made the ensuing conclusions:
Turner et al. [14] reported a case of myointimoma of the penis in a healthy 14-year-old male, who had manifested to the paediatric surgery unit of university of Florida with a firm, non-mobile 1 cm nodule upon the right side of his glans penis, which had been evident over about the preceding one month. His clinical examination was noted to be otherwise normal. An excisional biopsy of the penile lesion was undertaken. Histopathology examination of specimens of the excised penile lesion demonstrated an occlusive myointimal proliferation with complex multi-nodular / plexiform architecture which had involved the vasculature of his glans penis, and which had extended into the tissue margins. The nodular proliferations had comprised of medium to large spindle, and / or stellate cells that had long tapered cytoplasmic process, fine nuclear chromatin, inconspicuous nucleoli, and based upon additional pathology examination features of the lesion, a diagnosis of myointimoma of the penis was made.
Drlík et al. [1] reported a 15-year-old Caucasian boy, who had manifested with a 6-months history of a slowly growing, palpable firm nodule within his glans penis. Clinically he was completely asymptomatic and had voided freely. He did not report any history of trauma, systemic connective tissue diseases or other autoimmune disorders. During his clinical examination, there was evidence of a palpable, well circumscribed, firm, whitish painless mass, about 1 cm in diameter within his glans penis (see figure 6). His overlying skin was of a normal structure without signs of inflammation. No palpable inguinal lymphadenopathy was identified. The stage of puberty was Tanner III.

Figure 6: Whitish nodule visible under normal overlying skin. Reproduced from: [1] under the Creative Commons Attribution License.
In view of the fact that there were no guidelines concerning penile tumours in his age, the authors [1] adhered to the EAU guidelines for penile cancer in adults and they undertook a penile Doppler Ultrasound scan and MRI (Magnetic Resonance Imaging). The ultrasound scan demonstrated hypoechogenic, hypo-perfused poorly defined area within his glans penis. (see figure 7). The MRI scan did not confirm any other pathology mass inside his glans penis and corpora cavernosa (see figure 8). An excisional biopsy under general anaesthesia with intra-operative pathological evaluation was decided upon. The formation was noted not to have been clearly demarcated from the encompassing glans penis tissues and had reached close to the urethra, without interfering with its wall. The procedure was undertaken at optical magnification, utilising magnifying glasses with particular attention to prevent the injury of the neighbouring urethra (see figure 9). In view of the fact that the intra-operative pathology evaluation had demonstrated a benign nature of the tumour, Drlik et al. [1] simply closed the wound and did not proceed with any more extensive surgery (see figure 10).
Figure 7.
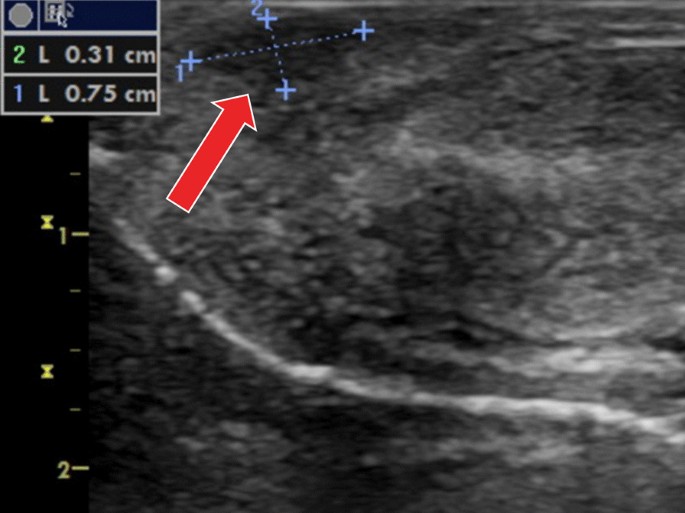
Figure 7. Ultrasound finding—a hypoechogenic, hypo-perfused non-well-defined area inside the glans (arrow). Reproduced from: [1] under the Creative Commons Attribution License.
Figure 8.
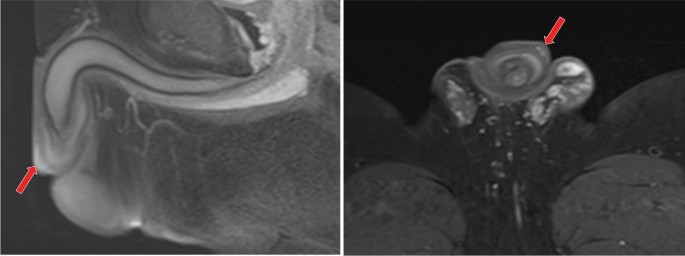
Figure 8.
MRI finding—a single hyperintense mass inside glans (arrow), corpora cavernosa, are normal, sagittal (A) and coronal (B) cut. Reproduced from: [1] under the Creative Commons Attribution License.
Figure 9.

Figure 9. Careful excisional biopsy with special attention to protection of the urethra. Reproduced from: [1] under the Creative Commons Attribution License.
Figure 10.

Figure 10. Simple wound closure. Reproduced from: [1] under the Creative Commons Attribution License.
Drlik et al. [1] found the lesion to be a macroscopically pale tissue sample which had measured 10 mm × 8 mm × 5 mm (see figure 11). On the cut surface, the lesion was noted to be light red in colour and had solid consistency. Subsequent detailed histopathology examination of specimens of the lesion demonstrated changes that were diagnostic for myointimoma - nodular intravascular myofibroblastic proliferation involving multiple cavernous spaces (see figure 12). At low power magnification, a complex multinodular architecture was visualised. At higher magnification the myofibroblasts were observed to be uniform, elongated spindle shaped cells with no significant hyperchromasia or pleomorphism, nor any mitotic figures or necrosis. Immunohistochemistry staining studies staining for alpha-smooth muscle actin (αSMA) was noted to be positive within the lesion (see figure 12), the proliferative activity (Ki-67) was low (beneath 1%) (see figure 13). Immunohistochemistry staining for desmin was negative within myofibroblasts, while positive in the pre-existing vessel wall only (see figure 15). No reactivity was visualised for other performed immunohistochemistry staining markers (S100 protein, CD34 and ERG). Microphotographs were taken with Olympus BX41 microscope and processed by QuickPHOTO Software.
Figure 11.
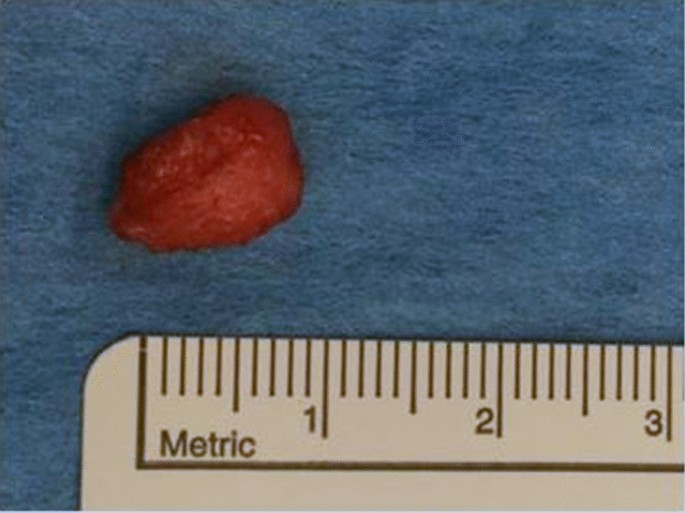
Figure 11: Macroscopic appearance of myointimoma. Reproduced from: [1] under the Creative Commons Attribution License.
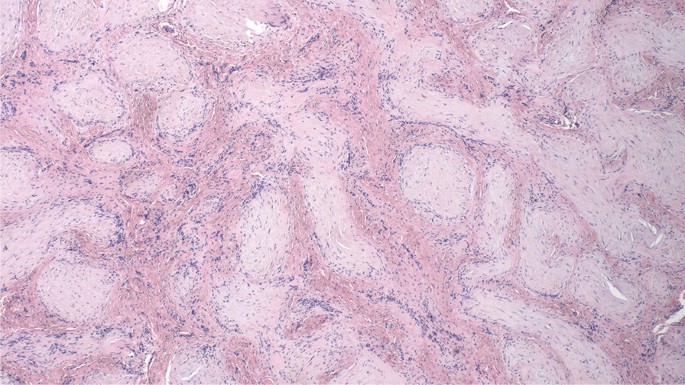
Figure 12: Nodular intravascular proliferation of spindle myofibroblastic cells presenting typical morphology for myointimoma (hematoxylin-eosin, 100x). Reproduced from: [1] under the Creative Commons Attribution License.
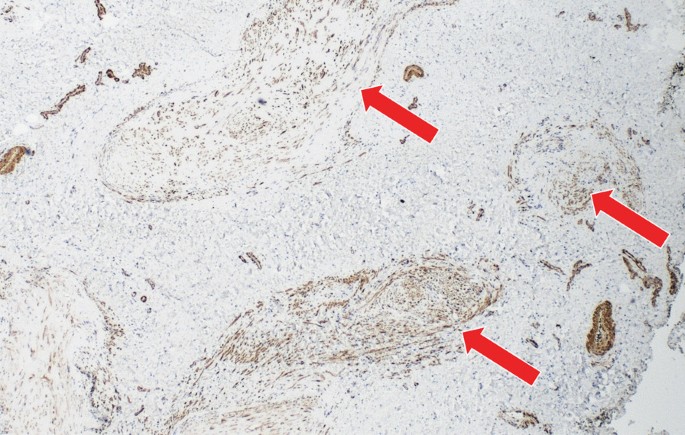
Figure 13: Immunohistochemical expression of alpha-smooth muscle actin (SMA) shows diffuse positivity in intravascular myofibroblastic population (arrow) (200x). Reproduced from: [1] under the Creative Commons Attribution License.
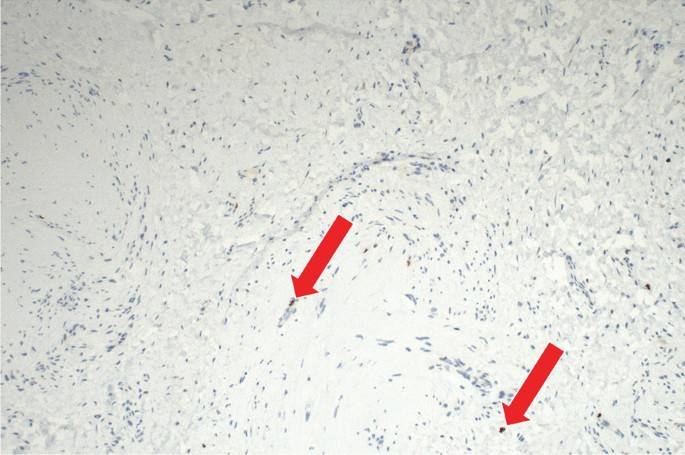
Figure 14: Immunohistochemical expression of Ki-67 (proliferative antigen MIB-1), labelling cells beyond G0 phase of the mitotic cycle, shows expression of sporadic cells (beneath 1%, arrow) (400x). Reproduced from: [1] under the Creative Commons Attribution License.
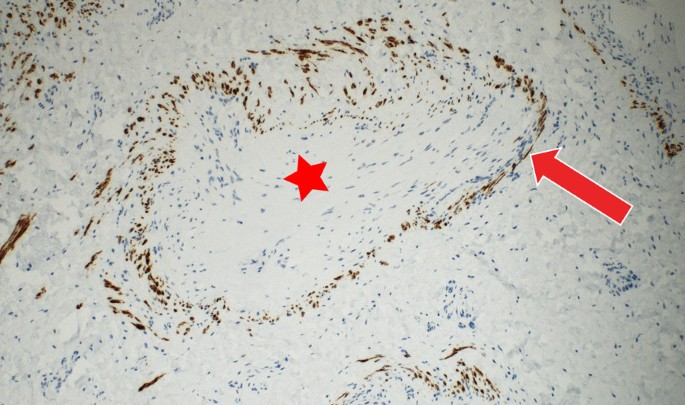
Figure 15: Immunohistochemical expression of desmin showing positivity in the smooth muscle cells of the pre-existing vessel walls (arrow), tumorous myofibroblastic cells are negative (star) (400x). Reproduced from: [1] under the Creative Commons Attribution License.
In view of the nature of the benign nature of the lesion, Drlik et al. [1] did not undertake staging for distant metastases and simply undertook an outpatient follow-up. Three years pursuant to the excision of the lesion, there was no evidence of local recurrence, no urethral stricture and a cosmetic appearance is good (see figure 16).

Figure 16: Favourable cosmetic outcome 3 years later. Reproduced from: [1] under the Creative Commons Attribution License.
Drlik et al. [1] made the ensuing educative discussion and conclusion:
Cito et al. [15] reported a 49-year-old Caucasian man who had presented with a 12-month history of a palpable, firm, solitary lesion involving his glans penis. During his clinical examination, there was a 1 cm palpable, endophytic well-circumscribed nodule, that was located to the left side of his glans penis, close to his coronal sulcus, with disease-free external urethral orifice. The patient underwent complete excisional biopsy. A skin rhombus that measured 1.1 cm × 0.8 cm × 0.3 cm was removed and the biopsy sample, was fixed in 10% formaldehyde, sent to the pathology department. During his 18-month follow-up visit, he was clinically disease free. Histopathology examination of his excised penile lesion demonstrated a multi-nodular intra-vascular proliferation of the corpus spongiosum. The myointimal proliferation had comprised of bland predominantly spindle cells in an abundant fibromyxoid stroma. Immunohistochemistry staining for smooth muscle actin (1A4), cytokeratins (AE1/AE3, CAM5.2), and CD34 were undertaken utilising the avidin-biotin complex (ABC) immunoperoxidase method. The lesional cells had exhibited positive staining for smooth muscle actin and negative staining for cytokeratins and CD34. Cito et al. [15] made the ensuing concluding iterations:
Casa et al. [6] made the ensuing iterations:
Casa et al. [6] reported four additional tumours of this unique myointimal proliferation. Casa et al. [6] summated the results as follows:
Casa et al. [6] made the ensuing concluding iterations:
Tanriverdi et al. [13] reported an 11-year-old boy, who was referred to Manisa Celal Bayar University Hospital with a nodule upon the left side of his glans penis. The nodule was detected two weeks preceding his assessment and the patient had not had any symptom except for the finding of the penile mass. The mass was located within the left side of his glans and it had measured 10 mm in size (see figure 1). The penile mass was also immobile and painless. The patient had been circumcised when he was 6 years-old. He did not have any history of any trauma or infection. The results of his laboratory tests were within their normal limits. He had ultrasound scan of his abdomen, urinary tract as well as scrotum which was also normal. The tumour was completely excised totally and his glans penis was sutured primarily. It had an irregular border (see figure 2).
Fig. 1. The nodule in the left side of glans penis (white arrow). Reproduced from: [13] under the Creative Commons Attribution License.
Fig. 2. The nodule excised totally. Reproduced from: [13] under the Creative Commons Attribution License.
Upon histopathology examination, the mass was found to consist of thick, smooth muscle fibres (see figure 3). There were focal fibrotic/fibromyxoid areas and spindle cell proliferation among them (see figure 4). The neoplastic cells had exhibited strongly positive staining with actin and weakly stained with desmin upon immunohistochemistry staining studies. (see figure 5). All of these aforementioned pathological findings were evaluated as myointimoma. In the first year of follow-up, the patient did not have any problem regarding his penis or other urinary tract organs.
Fig. 3. Thick, smooth muscle bundles (HE, x100). Reproduced from: [13] under the Creative Commons Attribution License.
Fig. 4. Focal fibrotic/fibromyxoid areas among smooth muscle fibers (Masson-trichrome, x100). Reproduced from: [13] under the Creative Commons Attribution License.
Fig. 5. Strongly staining with actin (Actin, x100). Reproduced from: [13] under the Creative Commons Attribution License.
Tanriverdi et al. [13] made the ensuing educative discussion:
Tanriverdi et al. [13] made the ensuing conclusions:
Turner et al. [14] reported a case of myointimoma of the penis in a healthy 14-year-old male, who had manifested to the paediatric surgery unit of university of Florida with a firm, non-mobile 1 cm nodule upon the right side of his glans penis, which had been evident over about the preceding one month. His clinical examination was noted to be otherwise normal. An excisional biopsy of the penile lesion was undertaken. Histopathology examination of specimens of the excised penile lesion demonstrated an occlusive myointimal proliferation with complex multi-nodular / plexiform architecture which had involved the vasculature of his glans penis, and which had extended into the tissue margins. The nodular proliferations had comprised of medium to large spindle, and / or stellate cells that had long tapered cytoplasmic process, fine nuclear chromatin, inconspicuous nucleoli, and based upon additional pathology examination features of the lesion, a diagnosis of myointimoma of the penis was made.
Drlík et al. [1] reported a 15-year-old Caucasian boy, who had manifested with a 6-months history of a slowly growing, palpable firm nodule within his glans penis. Clinically he was completely asymptomatic and had voided freely. He did not report any history of trauma, systemic connective tissue diseases or other autoimmune disorders. During his clinical examination, there was evidence of a palpable, well circumscribed, firm, whitish painless mass, about 1 cm in diameter within his glans penis (see figure 6). His overlying skin was of a normal structure without signs of inflammation. No palpable inguinal lymphadenopathy was identified. The stage of puberty was Tanner III.
Figure 6: Whitish nodule visible under normal overlying skin. Reproduced from: [1] under the Creative Commons Attribution License.
In view of the fact that there were no guidelines concerning penile tumours in his age, the authors [1] adhered to the EAU guidelines for penile cancer in adults and they undertook a penile Doppler Ultrasound scan and MRI (Magnetic Resonance Imaging). The ultrasound scan demonstrated hypoechogenic, hypo-perfused poorly defined area within his glans penis. (see figure 7). The MRI scan did not confirm any other pathology mass inside his glans penis and corpora cavernosa (see figure 8). An excisional biopsy under general anaesthesia with intra-operative pathological evaluation was decided upon. The formation was noted not to have been clearly demarcated from the encompassing glans penis tissues and had reached close to the urethra, without interfering with its wall. The procedure was undertaken at optical magnification, utilising magnifying glasses with particular attention to prevent the injury of the neighbouring urethra (see figure 9). In view of the fact that the intra-operative pathology evaluation had demonstrated a benign nature of the tumour, Drlik et al. [1] simply closed the wound and did not proceed with any more extensive surgery (see figure 10).
Figure 7.
Figure 7. Ultrasound finding—a hypoechogenic, hypo-perfused non-well-defined area inside the glans (arrow). Reproduced from: [1] under the Creative Commons Attribution License.
Figure 8.
Figure 8.
MRI finding—a single hyperintense mass inside glans (arrow), corpora cavernosa, are normal, sagittal (A) and coronal (B) cut. Reproduced from: [1] under the Creative Commons Attribution License.
Figure 9.
Figure 9. Careful excisional biopsy with special attention to protection of the urethra. Reproduced from: [1] under the Creative Commons Attribution License.
Figure 10.
Figure 10. Simple wound closure. Reproduced from: [1] under the Creative Commons Attribution License.
Drlik et al. [1] found the lesion to be a macroscopically pale tissue sample which had measured 10 mm × 8 mm × 5 mm (see figure 11). On the cut surface, the lesion was noted to be light red in colour and had solid consistency. Subsequent detailed histopathology examination of specimens of the lesion demonstrated changes that were diagnostic for myointimoma - nodular intravascular myofibroblastic proliferation involving multiple cavernous spaces (see figure 12). At low power magnification, a complex multinodular architecture was visualised. At higher magnification the myofibroblasts were observed to be uniform, elongated spindle shaped cells with no significant hyperchromasia or pleomorphism, nor any mitotic figures or necrosis. Immunohistochemistry staining studies staining for alpha-smooth muscle actin (αSMA) was noted to be positive within the lesion (see figure 12), the proliferative activity (Ki-67) was low (beneath 1%) (see figure 13). Immunohistochemistry staining for desmin was negative within myofibroblasts, while positive in the pre-existing vessel wall only (see figure 15). No reactivity was visualised for other performed immunohistochemistry staining markers (S100 protein, CD34 and ERG). Microphotographs were taken with Olympus BX41 microscope and processed by QuickPHOTO Software.
Figure 11.
Figure 11: Macroscopic appearance of myointimoma. Reproduced from: [1] under the Creative Commons Attribution License.
Figure 12: Nodular intravascular proliferation of spindle myofibroblastic cells presenting typical morphology for myointimoma (hematoxylin-eosin, 100x). Reproduced from: [1] under the Creative Commons Attribution License.
Figure 13: Immunohistochemical expression of alpha-smooth muscle actin (SMA) shows diffuse positivity in intravascular myofibroblastic population (arrow) (200x). Reproduced from: [1] under the Creative Commons Attribution License.
Figure 14: Immunohistochemical expression of Ki-67 (proliferative antigen MIB-1), labelling cells beyond G0 phase of the mitotic cycle, shows expression of sporadic cells (beneath 1%, arrow) (400x). Reproduced from: [1] under the Creative Commons Attribution License.
Figure 15: Immunohistochemical expression of desmin showing positivity in the smooth muscle cells of the pre-existing vessel walls (arrow), tumorous myofibroblastic cells are negative (star) (400x). Reproduced from: [1] under the Creative Commons Attribution License.
In view of the nature of the benign nature of the lesion, Drlik et al. [1] did not undertake staging for distant metastases and simply undertook an outpatient follow-up. Three years pursuant to the excision of the lesion, there was no evidence of local recurrence, no urethral stricture and a cosmetic appearance is good (see figure 16).
Figure 16: Favourable cosmetic outcome 3 years later. Reproduced from: [1] under the Creative Commons Attribution License.
Drlik et al. [1] made the ensuing educative discussion and conclusion:
Acknowledgement to:
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
