AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Sangeeta Vivek Shetty, Department of Anaesthesia, Fortis Hospitals, Mulund Goregaon Link Road, Mulund, Mumbai.
Citation: Sangeeta V Shetty, Vijay L Shetty, Gita D Baria, Nishigandha G Sawant, Hitesh R Singhavi. (2021) Modifications in anesthesia techniques and safety protocols at the outset of the COVID-19 pandemic, in a tertiary care center. Journal of Clinical Surgery and Research. 2(2) DOI: 10.31579/2768-2757/006
Copyright: © 2021 Sangeeta Vivek Shetty, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 February 2021 | Accepted: 12 April 2021 | Published: 15 April 2021
Keywords: anesthesia; covid-19; sars-cov-2; operating rooms; safety management; aerosols; personal protective equipment
Background and Aims: Anaesthesiologists, being involved in a variety of aerosol generating procedures during daily practice, are rendered especially vulnerable to the COVID-19 virus.
Our unit, situated in India’s epicenter, is managing both Covid and non Covid patients. The aim of this retrospective study was to analyse the impact of modifications in anaesthesia techniques and safety protocols at the outset of the COVID-19 pandemic.
Methods: We reviewed anaesthesia charts of 454 consecutive patients requiring anaesthesia services between 25 March 2020 and 31 May 2020. An anonymous survey was carried out by circulating a questionnaire among the 26 Anaesthesiologists of the Department using an android application.
Results: Anaesthesia technique modifications were performed in 55.7% of the studied cohort. Modifications included, no mask ventilation, use of rapid sequence intubation, shutting the carrier gas flows at breathing circuit disconnection (45.6%), use of intubation box (32.2%), conversion of GA to SA (11.0%), use of plastic sheet (7.7%), use of L screen for SA (0.9%).
Skill limitation due to PPE and discomfort using intubation box occurred in 84.61% and 53.85% anaesthesiologists respectively. 18.5% anaesthesiologists developed symptoms, however none of them tested RT-PCR positive. No anaesthesiologist required isolation or hospitalization due to COVID-19 infection.
Conclusions: The Lockdown period at the outset of the COVID-19 pandemic enabled strict triage and transmission prevention practices to be introduced and practiced. None of the anaesthesiologists in our department required hospitalisation or quarantine due to COVID-19.
Once the pandemic of COVID-19 was declared by the World Health Organisation (WHO) a nationwide lockdown was implemented to prevent the community spread between March 25th to May 31st2020. It followed the initial reports of the rampage caused by the Severe Acute Respiratory Syndrome-Corona Virus-2 (SARS-CoV-2) in health care facilities of the most developed nations of the world. As of December 2020, 6,52,57,767 cases and 15,13,179 deaths have occurred worldwide. In India, 96,08,211 cases and 1,39,700 deaths have been reported [1].
Anaesthesiologists are involved in a variety of aerosol generating procedures during a typical working day [2]. The vulnerability to the virus resulted in anaesthesia and intensive care to be classified as high-risk specialities [3]. Various guidelines have been suggested by national and international anaesthesia societies for the safety of healthcare workers [4, 5].
Our hospital, a corporate tertiary referral centre started admitting COVID-19 patients as per local Government (Brihanmumbai Municipal Corporation) policy since the outset of the pandemic. It is situated in Mumbai city which has been declared the epicentre of India’s corona virus outbreak, accounting for more than a fifth of the total case count. Being Joint Commission International (JCI) and National Accreditation Board of Hospitals (NABH) accredited standard practices of hygiene and infection control were already maintained at the workplace. However, we quickly realised that constant mindfulness of each action would be our only armamentarium and the way forward.
There being no definitive treatment available, we studied the impact of modifications in anaesthesia techniques and operation theatre safety protocols implemented by our unit at the onset of the COVID-19 pandemic.
This single centre, retrospective study was approved by the Institutional Ethical Committee. (Ref: IEC 2020/OAS/20). The requirement for informed consent was waived under the regulations of the committee.
Anaesthesia charts of consecutive outpatients and admitted patients requiring anaesthesia services during the period of lockdown between March 25th to May 31st 2020 were reviewed. Data pertaining to the type of procedure performed, type of anaesthesia given, pre-operative real time reverse transcription polymerase chain reaction (rRT-PCR) test status of the patient were collected. Suspected Covid positive patients included untested patients as well as those patients whose throat swab had been collected for rRT-PCR analysis but did not have the test results preoperatively. Modification of anaesthesia technique constituted the use of intubation box or plastic sheet, conversion of procedures normally performed under general anaesthesia (GA) or total intravenous anaesthesia (TIVA) to spinal anaesthesia (SA) and others (no mask ventilation, use of rapid sequence intubation, shutting the carrier gas flows whenever breathing circuit disconnected from the patient.)
26 Anaesthesiologists comprising 15 consultants and 11 registrars who were working full time in the department (in Covid and non Covid areas of the hospital) during the study period were asked to complete a questionnaire. This was done anonymously via SurveyMonkey (Google) application and forwarded to the participants via android mobile.
The primary outcome was to estimate the need of anaesthesiologists to visit COVID-19 fever clinic, undergo isolation, or hospitalization.
Statistical analysis -
Categorical data was analyzed using chi-square test. A two-sided P value <0.05 was considered statistically significant. Analyses were performed using SPSS version 20 (SPSS, Inc., Chicago, IL, USA).
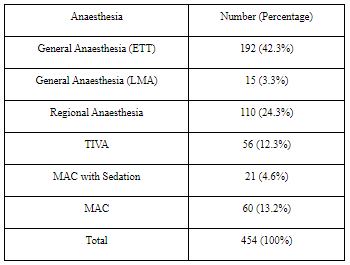
The analysis was done for 454 patients. Anaesthesia technique modification was performed in 55.7% of the studied cohort. 42.3% cases were done under GA with ETT, least number of cases were done using LMA (3.3%).
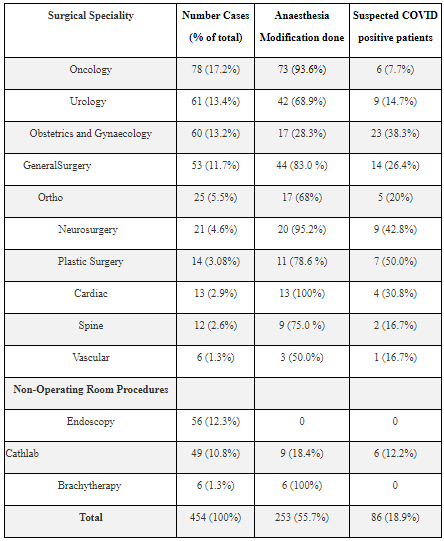
In the operation theatre, maximum modification was done for cardiac surgery (100%) and least for obstetric and gynaecology procedures (26.7%). The most common type of anaesthesia modification was avoidance of mask ventilation, use of rapid sequence intubation, shutting the carrier gas flows whenever breathing circuit was disconnected from the patient (45.6%). This was followed by use of intubation box (32.2%), conversion of GA to SA (11.0%), use of plastic sheet (7.7%), use of L screen for SA (0.9%). Plastic surgery, neurosurgery and obstetrics and gynaecology were the specialities with the most COVID suspect patients.
In non-operating room areas, all brachytherapy cases had conversion of technique from GA to SA. Although majority of cases were done in endoscopy, no modifications in technique was possible. All cases in endoscopy and brachytherapy had RT PCR results available before they were taken up.
18.5% anaesthesiologists from the department had symptoms related to COVID, however, none tested positive or required hospitalisation. 1 consultant was in self-isolation as a close contact had returned from overseas. All anaesthesiologists from the department, were motivated to come to work in spite of the fear of getting infected.
Following the declaration of lockdown, the work pattern in the hospital was continuously evolving. Triage at entry points allowed restricted entry to the hospital or diversion to the Covid fever clinic. Green stickers to wear indicated symptom free state, thus permission to enter. A revised standard operating procedure document incorporated the modifications in requirements of anaesthesia. Part telephonic pre anaesthesia consultations were encouraged in an attempt to reduce physical contact with the patient. Maintaining communication with patients while still avoiding close contact, presented a clinical and ethical dilemma.
In our analysis of the modifications of Anaesthesia, we noted that all patients receiving General Anaesthesia (GA) had implemented the suggested protocols of adequate pre oxygenation with face mask, rapid sequence intubation and mandatory shutting off of fresh gas flows whenever intubation was undertaken and when the circuit was disconnected [6].This was a result of simulations for conduct of GA with mannequins which was mandatory for all anaesthesia technicians and anaesthetists alongside the Personal Protective Equipment (PPE) training in the early part of the pandemic [7].
All airway interventions, were treated as a potential risk for transmission. Acrylic intubation boxes or plastic sheets were available as barriers for transmission of aerosols generated [8].More than half of the anaesthesiologists had difficulty using the intubation box. There was a learning curve owing to the altered ergonomics, hampered vision due to fogging and reflection of light on multiple layers of plastic. Begley et al have shown that aerosol boxes may paradoxically increase the risk to clinicians involved in COVID-19 airway management [9]. Rosenblatt et al have also questioned the use of the same [10].
The use of Laryngeal Mask Airways (LMAs) during the pandemic was very low with only 15 out of 263 cases conducted under GA being done with the LMA. (Table1.) Concerns have been expressed over the possible air leaks as well as requirement of adjustments of the device which in turn necessitates proximity to a possible source of infection [11]. The evidence for use of LMA in COVID is limited. Yang et al have recommended its use in an airway rescue scenario over face mask ventilation before and in between attempts at laryngoscopy [12]. Other authors have not shared these concerns and have advised regular use of LMAs due to their advantages over general anaesthesia with endotracheal tube [13].
Our analysis also revealed that whenever appropriate for the surgery, regional anaesthesia was chosen over general anaesthesia (which would have been a choice in the pre-pandemic era) given its advantages of lesser aerosolization during intubation and extubation as well as accidental circuit disconnections [14,15]. Also, given the propensity for pulmonary involvement in the Covid patients, avoiding general anaesthesia could have pulmo-protective effects due to prevention of atelectasis and maintained ciliary function and pulmonary clearance.
Regional anaesthesia was used in 80% of obstetrics and gynaecology and 54% of urology patients. (Graph 1.) In short cases such as radiotherapy for cancer cervix (brachytherapy), short urosurgeries, spinal anaesthesia (SA) replaced GA. (Table 3.) The short duration of action of Chloroprocaine made it the drug of choice for spinal anaesthesia. After a 15 to 20minute period of observation in the operation theatre (OT), these patients were shifted to their respective wards. An L-shaped metal bar called the L-screen had been locally suggested to enable positioning of patients during neuraxial blockade and reduce the close contact of attendants with the patient. However, its use was not favoured in the department. Attempts were made to reduce the use of total intravenous anaesthesia (TIVA) thus preventing airway manipulation in case of deeper planes of sedation. However, Choksi et al favoured TIVA [16]. Use of TIVA could not be avoided in endoscopy patients.
Plastic surgery, Obstetrics and Gynaecology and Neurosurgery were the specialities with the highest number of suspected Covid patients as a result of their emergent nature. One obstetric patient in our cohort, tested RT-PCR positive postoperatively after undergoing an emergency caesarean section under SA uneventfully. All patients from endoscopy and brachy therapy had RT PCR results available pre procedure.
The anaesthesiologists were divided into two groups that worked alternately on weekly basis in the operating rooms. A third group contributed to rotas in emergency room, intensive care units (ICU) and Covid ICU. Restricting the operating list to urgent or semi-emergency surgeries made this division possible.
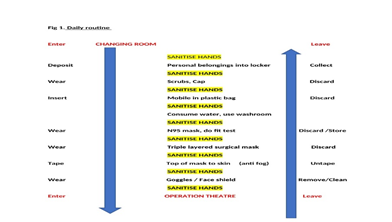
The drill of wearing basic personal protection formed a daily routine (Fig 1) In the first week standard 3 ply masks were used, thereafter, a set of five N95 National Institute for Occupational Safety and Health (NIOSH) certified masks were used in rotation, stored in paper bags and discarded after five uses per mask [17]. The previous SARS outbreak in 2003, suggested the use of positive airway pressure respirators (PAPR) along with N95 masks [18]. However, PAPR was not used in our setup. Maintaining interpersonal distance, long-sleeved cotton gown, frequent hand washing / sanitisation, double layered gloves for airway procedures were encouraged [19].
PPE was donned for all suspected cases. In our study, most anaesthesiologists experienced skill limitation due to PPE. Fogging, discomfort, restriction of movements, difficulty in communication, were limitations of PPE use. Repeated mask or goggle adjustment without prior hand sanitisation was discouraged. Donning and Doffing of PPE was assisted by dedicated nurse, signages on the OT walls and segregated sites [20].
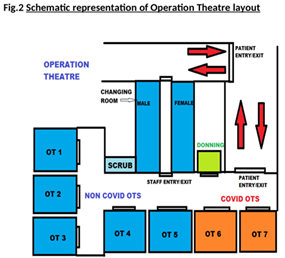
Two adjacent OTs containing only the essential equipment were designated for COVID-19 positive or suspected patients. (Fig 2). Proximity to the entry area of the OT complex minimised contamination of the premises [21]. One of them had an automatic door opening system and served as a doffing area. Recommendations of conversion to negative pressure operating theatres have been made. [22, 23]. The endoscopy unit had a negative pressure room. However, operation theatres had positive pressure systems. Here, the heating ventilation and air conditioning (HVAC) units of the COVID-19 OTs were kept separate from the other theatres. The temperature was maintained between 20 – 22 degrees Celsius and humidity at 55 – 60%. High Efficiency Particulate Air (HEPA) filters with 25 room air exchanges per hour was the standard. Plastic sheets covered most surfaces including electrocautery, anaesthesia workstation and monitor. Necessary high alert medications and anaesthesia drugs were dedicated to the OT [24]. Once the patient entered, doors were shut. A runner (nurse) ready in PPE stationed outside the OT provided equipment, drugs, essential documentation or called for help if required.
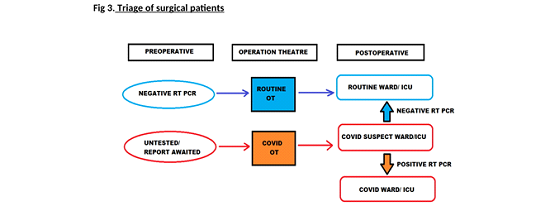
All awake patients came into the OT wearing a triple layered surgical mask. Protection during transfer included plastic sheet covers and heat and moisture exchange filters (HMEF) to minimise aerosolization in ventilated patients. Triage of surgical patients was maintained. (Fig.3)
OTs were kept closed for 20 minutes after each suspected and positive case to allow for air exchanges before housekeeping staff entered for cleaning [25]. Instruments were sent to the central sterile services department (CSSD) in a separate pack. Floor, walls were cleaned with 1% hypochlorite, surfaces with 75% alcohol and fogging with vaporised hydrogen peroxide [24, 26]. Manufacturer instructions were followed for video laryngoscope cleaning. Filters, breathing circuit, soda lime were changed for each case receiving general anaesthesia. Wherever possible, disposable material was used. Hospital protocol defined the collection of waste in bin liners. They were labelled - suspected or Covid positive and discarded at the end of the case as per biomedical waste management policy.
The dining area within the OT complex, remained one of the most difficult areas to enforce discipline. Reduction in the number of chairs limited the number of people present at a time. Diagonal seating or one-way facing seating was permitted.
OT and housekeeping staff were retrained regarding proper use of mask, importance of handwashing and maintaining interpersonal distance. Mock drills for donning, doffing, instructional videos and webinars on the subject were used as tools for the same
ICMR had recommended the use of Hydroxychloroquine (HCQ) prophylaxis for health care workers [27]. In our unit however, it was an individual choice, taken by 50 % of the personnel.
Anaesthesiologists from the department who visited the Covid fever clinic (OPD) had fatigue as the commonest symptom. None of them tested RT- PCR positive. One anaesthesiologist had self-isolated due to close contact with a family member who had travelled overseas. No anaesthesiologist required isolation or hospitalisation due to COVID -19 infection.
In spite of the lurking fear of getting infected and carrying the virus home, all the department members were committed to their work. Positive re-enforcement and working in high-risk zones by example went a long way in encouraging the team members to continue the smooth functioning of the department and ICU areas of the hospital. Anaesthesiologists thus played a dual role in managing COVID ICU and COVID suspected patients in operation theatre.
The Lockdown period enabled new practices to be tested and personnel became accustomed to them. Staff were trained, drills could be carried out. Stringent hygiene techniques and triage at each level became the pillars of support. None of the anaesthesiologists in our department required hospitalisation or quarantine due to COVID-19.
With the lockdown easing off, the number of COVID-19 cases in the community is rising and we will be definitely encountering a higher number of infected cases. Further modification of protocols may be required to accommodate increasing OT lists and anaesthesia personnel requirements in other areas of the hospital.
Modifications in anaesthesia techniques and safety protocols have become the new normal. They have kept us in good stead so far and we must not let our guard down. These practices may be considered as a model for other Covid-care setups and similar contingencies in the future.
Funding source – Nil
Acknowledgement – Would like to thankDr Vaishali Shende for data collection and Dr
Hemalata Iyer for critical review of the manuscript.
Presented as part of meeting / publication – No
Registration number in case of clinical trial – Not applicable
Conflicts of interest – Nil
Criteria for inclusion in authors list
Dr Sangeeta Shetty – Concept, design, definition of intellectual content, literature search, manuscript preparation.
Dr Vijay Shetty – Definition of intellectual content, manuscript editing, manuscript review.
Dr Gita Baria – Design, data acquisition, data analysis, manuscript editing.
Dr Nishigandha Sawant – Literature search, manuscript editing, manuscript review.
Dr Hitesh R Singhavi – Statistical analysis, manuscript editing, manuscript review.
Manuscript has been read by all authors – Yes as mentioned in Contributors form
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
