AUCTORES
Globalize your Research

Review Article
*Corresponding Author: N. Tsonev, Clinic of Gastroenterology, Second MHAT Sofia – Sofia, Bulgaria.
Citation: N. Tsonev , D. Vandeva, K. Toncheva, D. Zvezdov. (2022). Management Of Therapy of Anticoagulants and Antiplatelets in Acute Gastrointestinal Bleeding and In the Periendoscopic Period. Cardiology Research and Reports. 4(4); DOI:10.31579/2692-9759/076
Copyright: © 2022 N. Tsonev, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 September 2022 | Accepted: 10 October 2022 | Published: 16 November 2022
Keywords: anticoagulants; antiplatelet agents; gastrointestinal bleeding; management
Management of anticoagulant and antiplatelet therapy is a common clinical problem in case of urgent or elective gastrointestinal endoscopic procedures. Anticoagulants and antiplatelet agents are widely used drugs for cardiovascular prevention and reducing the risk of thromboembolic events. Gastrointestinal bleeding represents a serious complication of their use. It’s recommended temporary interruption of anticoagulants in clinically significant gastrointestinal bleeding. For the antiplatelet therapy the decision is when to stop and restart the therapy, depending on whether it’s for primary or secondary cardiovascular prevention. Treatment with antithrombotic drugs in the periprocedural endoscopic period is based on balancing the bleeding risk against the thromboembolic risk. It’s recommended temporary discontinuation of antithrombotic treatment in high-risk endoscopic procedures with high risk for bleeding and to consider the use of “bridging” therapy with LWMH for patients on vitamin K antagonists who are at high thrombotic risk. Antithrombotic agents in endoscopic procedures with lower bleeding risk are not needed to be withheld. Evaluating cardiovascular risk and management of antithrombotic therapy could be a challenge for gastrointestinal endoscopists, therefore collaboration with a cardiologist is of great importance, at least for some patients.
Anticoagulants and antiplatelets are widely used drugs for several cardiovascular and thrombotic conditions. These drugs increase the risk of bleeding during endoscopic procedures and discontinuation of their administration carries a risk for thromboembolic events. The assessment of whether and when to interrupt and reverse the antithrombotic drugs intake in case of urgent or elective gastrointestinal endoscopy creates difficulties, as the thrombotic risk and the risk of bleeding are different for each patient [1].
In case of GIT bleeding, the coagulation status (platelets, INR and aPTT) must be examined, and the correction of coagulation is carried out depending on the situation. In case of acute bleeding, endoscopic intervention can be performed regardless of laboratory parameters. Significant disorders in hemostasis are corrected regardless of the time of endoscopy. A study on the routine examination of coagulation status before endoscopic or surgical treatment showed no correlation with the actual incidence of bleeding without a history of predisposing disease or previous hemorrhage [2]. The anamnestic history reveals evidence of acquired or congenital coagulopathy, for example bleeding from a previous procedure, diseases associated with an increased risk of bleeding Ehler Danlos, Marfan syndrome congenital thrombocytopathies, congenital plasma coagulopathies, Willebrand syndrome, congenital deficiency of Factor VIII and IX, acquired platelet dysfunction and coagulopathies in liver, nephrological diseases, long-term biliary obstruction, long-term antibiotic treatment, malnutrition or myeloproliferative diseases [2].
When should antiplatelet and anticoagulant therapy be stopped and in which diseases should it be continued? There are no established data on the optimal INR for emergency endoscopy.A retrospective analysis of patients with supratherapeutic INR (INR > 4) and patients with therapeutic values reported similar outcomes for recurrent bleeding, need for blood transfusion, and hospital mortality [3]. In an English study, results differed, reporting poorer endoscopic bleeding control at INR > 1.5 [4]. Some authors recommend an INR < 2>2.5 OR 7.9) and of mortality in non-variceal GIT bleeding (INR>1.5 OR 5.6 [10]. This is indicative of the role of INR as an indicator of comorbidities. Neutralization of the effect of anticoagulant therapy in acute gastrointestinal bleeding is based on the use of IV vitamin K, fresh frozen plasma, and concentrated prothrombin complex for warfarin users [11,12] and activated charcoal - oral, hemodialysis, idarucizumab or prothrombin complex for DOAC users [13,14]. The effect of prothrombin complex in DOAC hasn’t been studied. A heparin bridge does not significantly alter the risk of rebleeding and thromboembolism in gastrointestinal bleeding [9]. In a retrospective study in patients treated with warfarin, a higher rate of bleeding was reported in the non-bridging group, with no difference in periprocedural thromboembolism [15].Similar results were also reported in periprocedural DOAC users [16].
When to resume taking of anticoagulants? A meta-analysis showed that restarting anticoagulants reduced the incidence of thrombotic events in patients with discontinued therapy due to bleeding (HR 0.68 95 Percentage CI 0.52-0.88) and mortality (HR 0.76 95 Percentage CI 0.66- 0.88) without significantly increasing the incidence of recurrent bleeding (HR 1.20 95 Percentage CI 0.97-1.48) [17].
A study comparing the administration of DOAC and warfarin showed that the incidence of recurrent bleeding at day 90 after endoscopy was similar in the DOAC-resumed and non-resuming groups. In this study, a history of venous thrombosis was associated with thromboembolic events (HR 3.30 95 Percentage CI 1.29-7.38) [18]. Another study determined the risk of acute gastrointestinal bleeding with anticoagulant use based on five factors (absence of PPI, chronic kidney disease, COPD, ulcer history, and liver cirrhosis). The new statistical rating system (0.65) outperforms that of HAS-BLED (0.57) [18,19].
Anticoagulants and risk of bleeding in elective endoscopic procedures
Annually, about 10 Percentage of patients taking anticoagulants require temporary discontinuation of therapy due to surgical or other invasive elective procedures, such as gastrointestinal endoscopy [20]. A serious complication of anticoagulant therapy is severe GIT bleeding, with an incidence of approximately 1-4 Percentage per year and a fatal incidence of up to 10 Percentage [21,22 ]. About 15 Percentage of patients with acute upper GIT bleeding and up to 32 Percentage of patients with lower GIT bleeding take anticoagulants [23,24].
The recommendations of the British Gastroenterology Association (BSG) and the European Gastrointestinal Endoscopy Association (ESGE) for anticoagulant therapy in patients undergoing routine endoscopy are based on stratification of patients at risk categories according to the risk of bleeding in the endoscopic procedure and thromboembolic risk (table. 1 and table. 2) [25,26].
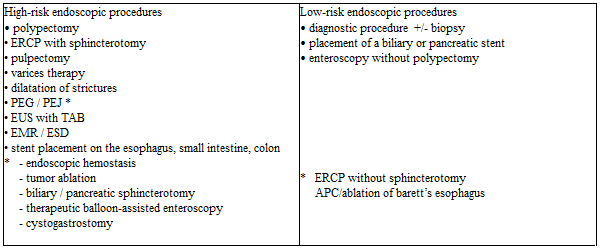
Тable 1: Endoscopic procedures with high and low risk of [25,26,27]
ERCP - endoscopic retrograde cholangiopancreatography; PEG - percutaneous endoscopic gastrostomy; PEJ - percutaneous endoscopic jejunostomy; EUS – endoscopic ultrasound; TAB - fine-needle aspiration biopsy; EMR - endoscopic mucosal resection; ESD - endoscopic submucosal dissection; APC - argon plasma coagulation
* Endoscopic procedures included in the guideline of the American Society of Gastrointestinal Endoscopy

*AF – atrial fibrillation
Таble 2: Conditions with high and low thromboembolic risk [25,26].
Studies have found that gastrointestinal bleeding is a typical complication of vitamin K using antagonists as a difference in risk between vitamin K antagonists (VKA) and direct-acting oral anticoagulants (DOAC) were not observed [21]. A meta-analysis involving 23 prospective studies, comparing the use of DOAC (apixaban, dabigatran, edoxaban, and rivaroxaban) and vit K antagonists on the risk of massive gastrointestinal bleeding, did not show any difference (RR 1.08) [28]. A meta-analysis of 43 prospective randomized trials reported a slightly increased risk of gastrointestinal bleeding with DOAC compared to vit. K antagonists (OR 1.45) [29]. A Finnish study in 100,000 patients reported a risk of 2.3 Percentage per year for hospitalized ones for gastrointestinal bleeding at the start of therapy and 0.9 Percentage during long-term treatment. The risk was the highest in the first 30 days of initiating anticoagulant therapy [30]. The risk of severe bleeding also depended on comorbidity, concomitant therapy, duration of anticoagulant therapy, and indications for anticoagulation (the incidence is 2.5 Percentage in patients with atrial fibrillation and 0.5 Percentage in patients with pulmonary embolism) [28].
The risk of bleeding increases when using an anticoagulant with an antiplatelet agent and especially with two antiplatelet agents. The “Stent Anticoagulation Restenosis Study” reported a higher number of bleeding events with an anticoagulant and Aspirin compared to the Aspirin-only group - 6.2 Percentage to 1.8 Percentage [31], as bleeding events from the GIT were not reported. In a retrospective analysis of 666 patients on triple therapy with aspirin, clopidogrel, and enoxaparin, with short-term use in patients with acute coronary heart disease, gastrointestinal bleeding was observed in 2.7 Percentage of the patients on day 30 [32]. In a Danish retrospective study of 118,606 patients, bleeding cases were reported with triple therapy with aspirin, clopidogrel, and vit. K antagonist - 15.7 Percentage per year, and in a double therapy group with vitamin K antagonist and clopidogrel - 13.9 Percentage per year [33]. Comparing monotherapy with vitamin K antagonist with dual therapy with clopidogrel, a 3.1-fold increase in risk and respectively 3.7-fold increase with triple therapy was reported. The gastrointestinal bleeding was 5.1 Percentage per year, a 5.38 times increase compared to oral anticoagulant monotherapy. The risk of bleeding after myocardial infarction with triple therapy was 1.4 times higher than with vitamin K antagonist therapy and antiplatelet agent. The proportion of patients with fatal GIT bleeding compared with non-fatal cases was 45.3 Percentage to 33.8 Percentage [34]. In a prospective study where the bleeding was targeted, a significantly higher frequency was reported. Episodes of bleeding were reported annually in 19.4 Percentage of patients on dual therapy and in 44.4 Percentage of patients on triple therapy, with 2 Percentage to 8.8 Percentage of patients experiencing GIT bleeding [35].
In the study by Sorensen et al., the risk of hospitalization due to hemorrhage associated with various antithrombotic regimens was investigated. It covered 40,812 patients over the age of 30 who were admitted to a hospital with myocardial infarction for the first time. They were divided into the following groups: monotherapy with aspirin, clopidogrel, or vitamin K antagonist; double therapy with aspirin plus clopidogrel, aspirin plus vitamin K antagonist, or clopidogrel plus vitamin K antagonist, or triple therapy involving all three drugs. The risk of bleeding, recurrent myocardial infarction, and death has been assessed. During the mean follow-up of 476.5 days (SD ± 142.0), 1891 (4.6 Percentage) patients were admitted to the hospital with bleeding. The annual bleeding rate was 2.6 Percentage for the aspirin group, 4.6 Percentage for clopidogrel, 4.3 Percentage for the vitamin K antagonist, 3.7 Percentage for the aspirin plus clopidogrel, 5.1 Percentage for the aspirin plus vitamin antagonist. K, 12.3 Percentage for clopidogrel plus vitamin K antagonist and 12.0 Percentage for triple therapy. With aspirin as the reference drug, the corrected risk factor for bleeding was 1.33 (95 Percentage CI 1.11-1.59) for clopidogrel, 1.23 (0.94-1.61) for vitamin K antagonist, 1.47 (1.28-1.69) for aspirin plus clopidogrel, 1.84 (1.51-2.23) for aspirin plus vitamin K antagonist, 3.52 (2.42-5.11) for clopidogrel plus vitamin K antagonist, and 4.05 (3.08-5.33) for triple therapy. 702 (37.9 Percentage) of 1852 patients with non-fatal bleeding had a recurrent myocardial infarction or died during the study period compared with 7178 (18.4 Percentage) of 38 960 patients without non-fatal bleeding (HR 3.00, 95 Percentage CI 2.75-3.27, p less than 0.0001). In patients with myocardial infarction, the risk of bleeding increases with the number of antithrombotic drugs used [36].
According to the recommendations of BSG and ESGE, anticoagulants could be continued in low-risk endoscopic procedures but should be discontinued in all high-risk procedures. In procedures with a low risk of bleeding, the INR values should be checked one week before the procedure and should be at therapeutical limits. For INR values above therapeutical limits but below 5, it is recommended to reduce the daily dose until therapeutic levels are reached. Discontinuation of VKA may also be considered in diagnostic procedures that are likely to become high-risk, such as colonoscopy polypectomy [25,26]. In this regard, studies have shown that it is safe to perform a polypectomy of a colon polyp below 10 mm without interrupting the VKA, provided that endoscopic clips are prophylactically inserted [37] or that an end loop polypectomy technique is used to reduce the risk of late bleeding [38].
In patients on vitamin K antagonist therapy who is undergoing an endoscopic procedure with a high risk of bleeding but a low thrombotic risk is recommended to discontinue vitamin K antagonist intake 5 days before the procedure for Warfarin, 3 days for acenocoumarol. For this period, the INR values reach ≤ 1.5 in 93 Percentage of patients. After the endoscopic procedure, the intake of vitamin K antagonist can be restored on the same day at the usual daily dose [25,26].
In endoscopic procedures with a high risk of bleeding and conditions with a high thrombotic risk, it is recommended to discontinue the oral anticoagulant and switch to bridging therapy with a direct-acting parenteral anticoagulant, usually low molecular weight heparin (LMWH) /100 UI / kg 2x / to reduce the periprocedural risk of thromboembolism.
LMWH should be discontinued 24 hours before the procedure and resumed the next day in low-risk post-procedural bleeding or after 48 hours in high-risk post-procedural bleeding (according to the 2012 ACCP guideline) [39]. On the other hand, ESGE's recommendations for bridging heparin therapy do not include patients who are traditionally considered to be at high risk for thromboembolic events, such as those with non-valvular atrial fibrillation and previous thromboembolic events and/or CHADS2 score 5 or 6, and those with recent (up to 3 months) venous thromboembolism [20].
After decades in which vit. K antagonists were the only oral anticoagulants, the spectrum of these drugs was expanded to include a new class of drugs, such as direct oral anticoagulants - directly inhibiting thrombin/dabigatran - Pradaxa® / or activated factor Xa (Rivaroxaban – Xarelto®; Apixaban- Eliquis®). DOAC has several advantages over vit. K antagonists - due to more predictable pharmacokinetics, are prescribed in a fixed-dose, no routine monitoring of coagulation status is required. The rapid onset of action / 1-4 hours / and short half-life / 9-17 hours / makes the initiation and interruption of therapy relatively easier and safer than vitamin K antagonists [1].
There is also a risk of bleeding when taking DOAC. In a retrospective study in patients stratified into three age groups with non-valvular atrial fibrillation and dabigatran, rivaroxaban, or apixaban, Mayo researchers evaluated the incidence of total GIT bleeding and compared rivaroxaban with dabigatran in 31,574 patients, apixaban with dabigatran in 13,084 patients and for apixaban with rivaroxaban in 13,130 patients. Apixaban was found to have the most favorable safety profile for GIT compared to dabigatran and rivaroxaban in the three age groups. Rivaroxaban has the most unfavorable safety profile for the GIT. Patients using apixaban were 61% less likely to experience GIT bleeding than those on dabigatran (HR 0.39; 95% CI, 0.27-0.58). Dabigatran patients were 20% less likely to bleed than rivaroxaban (HR, 1.20; 95% CI, 1.00-1.45). It is observed that the cases of bleeding from the GIT in patients taking DOAC increase with age, with the greatest risk observed in persons aged 75 years and older. The researchers concluded that Apixaban had the safest profile of the three drugs studied in this age group [40].
Due to the short half-life of DOAC, they can be discontinued hours before the endoscopic procedure, and due to the rapid onset of action, anticoagulation is achieved within a few hours after inclusion [1]. These pharmacokinetic properties of DOAC eliminate the need for bridging heparin therapy. On the other hand, this class of drugs is not indicated for use in patients at high thrombotic risk [25,26].
For endoscopic procedures with a low risk of bleeding, ESGE recommends skipping the morning dose of DOAC. The optimal window for the endoscopic procedure is considered to be when the anticoagulant effect is relatively low - about 10 hours after the last dose for drugs taken twice daily and about 20 hours - for the once-daily medication (Rivaroxaban). In high-risk procedures - the last dose is recommended to be taken 48 hours before the endoscopic procedure, for Dabigatran (with CrCl - 30-50 ml/min) - 72 hours before the manipulation [25,26].
Antiplatelet agents are widely used drugs in clinical practice, mainly for primary and secondary prevention of cardiovascular diseases [41]. The use of antiplatelet agents has been associated with outweighing clinical benefits [42], but may nevertheless cause upper and lower GIT bleeding [43,44,45]. Antiplatelet agents lead to the formation of erosions and ulcers in the duodenum and stomach and can provoke bleeding from existing ones [43]. The role of antiplatelet agents for bleeding from the large intestine, mainly from diverticula [45], as well as for bleeding from the small intestine, mainly in erosive enteropathy, is also discussed [44]. Antiplatelet agents also increase the risk of bleeding on endoscopy. A retrospective study suggests that the risk of bleeding in mucosal biopsy varies between 0.02 Percentage -0.1 Percentage, increasing in those patients taking antiplatelet agents as well as with the number of biopsies [39]. In a prospective study, a bleeding episode requiring endoscopic hemostasis was observed in 2.2 Percentage of 1015 patients who underwent polypectomy of colonic polyps less than 10 mm with an endoloop technique. In this study, antiplatelet monotherapy (aspirin or ticlopidine) was associated with a 4-fold increase in the risk of bleeding (95 Percentage CI 1.5-10.6) [46]. A study by Lanas and Gargallo found that the risk of severe upper GIT bleeding was high when two antiplatelet agents were included in the therapy and were increasing 1.8-fold with low-dose aspirin and 7.4-fold with aspirin and clopidogrel [47].
A meta-analysis of prospective studies involving more than 100,000 patients found that the risk of total bleeding (OR 1.70) as well as of severe or significant bleeding (OR 1.31) was increased with medications [48]. Another meta-analysis showed an increase in the risk of bleeding annually by 0.13 Percentage for severe bleeding and by 0.12 Percentage for light bleeding with prolonged use of aspirin. The relative risk remains 2.22 for severe gastrointestinal bleeding and 1.23 for fatal bleeding [49]. The CAPRIE STUDY showed a lower risk of gastrointestinal bleeding with Clopidogrel compared to Aspirin (RR 1.45) [50]. The use of an antibody against GP2II3a in patients with myocardial infarction increases the risk of bleeding [51]. The risk of bleeding from GIT with double antiplatelet therapy was found to be higher than with monotherapy and reaches HR 2.7 [52]. In triple antiplatelet therapy, when cilostazol was added to aspirin and clopidogrel, the same risk of bleeding was observed compared to dual antiplatelet therapy - 2.39 Percentage vs. 2.04 Percentage, but the risk of gastrointestinal bleeding was significantly higher with triple anti-aggregation (OR 2.46) [ 53]. In the study of Luis et al., the risk of upper gastrointestinal bleeding associated with the use of low doses of acetylsalicylic acid (75 to 300 mg / d) alone and in combination with other gastronomic drugs was assessed in 2049 patients. Researchers found that the risk of upper GIT bleeding was increased in low-dose aspirin (RR, 1.80; 95 Percentage CI, 1.59 to 2.03) or clopidogrel users(RR, 1.67; 95 Percentage CI, 1.24 to 2.24) compared with non-users. The risk of upper GIT bleeding was significantly increased when aspirin is used in combination with clopidogrel (RR 2.08; 95 Percentage CI, 1.34 to 3.21), with oral anticoagulants (RR 2.00; 95 Percentage CI, 1.15 to 3.45), low/medium dose nonsteroidal anti-inflammatory drugs (RR 2.63; 95 Percentage CI, 1.93 to 3.60), high dose nonsteroidal anti-inflammatory drugs (RR, 2.66; 95 Percentage CI, 1.88 to 3.76) or with high-dose oral corticosteroids (RR, 4.43; 95 Percentage CI, 2.10 to 9.34) compared to low-dose aspirin monotherapy. The risk was not significantly increased when co-administered with statins (RR, 0.99; 95 Percentage CI, 0.81 to 1.21) or low-dose oral corticosteroids (RR, 1.01; 95 Percentage CI, 0.58 to 1.77) [54].
In the study of Weil et al., the risks of hospitalization due to peptic ulcer bleeding (gastric or duodenal) were determined against the background of prophylactic regimens with aspirin of 300 mg daily or less in 1121 patients. In 144 (12.8 Percentage) cases, regular use of aspirin (at least five days a week in the previous month) was found compared to 101 (9.0 Percentage) patients in the control hospitalized group and 77 (7.8 Percentage) community controls. The odds ratio was increased for all doses of aspirin taken, whether compared to hospital or municipal controls (compared to combined controls: 75 mg, 2.3 (95 Percentage CI 1.2 to 4.4), 150 mg, 3.2 (1.7 to 6.5), 300 mg 3.9 (2.5 to 6.3) Results are not affected by obscuring factors such as age, gender, previous ulcerative disease or dyspepsia or concomitant use of non-aspirin NSAIDs Researchers have not established a conventional prophylactic regimen of aspirin which is without risk of complications of the peptic ulcer [55].
On the other hand, the potential cardiovascular risk associated with the discontinuation of antiplatelet agents is ignored [56]. If the patient is on long-term antiplatelet therapy for primary or secondary cardiovascular prevention, a cardiovascular event may occur when antiplatelet agents are discontinued for several days. Most (60-70 Percentage) serious cardiovascular events occur within 10 days of antiplatelet discontinuation [57,58].
The use of antiplatelet agents in routine endoscopic procedures is based on an assessment of the risk of bleeding during endoscopy and the patient's thrombotic risk [57]. BSG and ESGE recommend that antiplatelet agents are continued in patients undergoing endoscopic procedures with a low risk of bleeding [25,26]. Aspirin can be continued with all endoscopic procedures, except for ESD, colon EMR over 2 cm, upper EMR, and pulpectomy. The risk of thrombosis versus the risk of bleeding should be assessed in these procedures for each patient [25]. In patients receiving dual antiplatelet therapy, only clopidogrel should be discontinued 5 days before high-risk endoscopic procedures when the risk of thrombosis is low. In case of high thrombotic risk, a consultation with a cardiologist is required [25,59]. When the thrombotic risk of stopping clopidogrel is high (30 days after coronary stent placement), the endoscopic procedure should be postponed. Clopidogrel can be resumed after the procedure when endoscopic hemostasis has been achieved [59].
The use of antithrombotic drugs is associated with an increased risk of bleeding from the GIT. In endoscopic interventions, it is necessary to balance the risk of bleeding and the thromboembolic risk in each patient. In addition to assessing the risk of bleeding, the endoscopist must be familiar with the criteria for assessing cardiovascular risk. In this area collaboration with a cardiologist is essential, especially in the manipulation of certain patients.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
