AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Delaunays Road, Crumpsall, M8 5RB. Manchester. United Kingdom
Citation: Anthony Kodzo-Grey Venyo, (2023) Malignant Peripheral Nerve Sheath Tumour (MPNST) of the Prostate Gland: A Review and Update, J. Cancer Research and Cellular Therapeutics, 7(1) DOI: 10.31579/2640-1053/131
Copyright: © 2023 Anthony Kodzo-Grey Venyo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 November 2022 | Accepted: 26 December 2022 | Published: 13 January 2023
Keywords: malignant peripheral nerve sheath tumour; mpnst; prostate gland; radical prostatectomy; radical radiotherapy; chemotherapy; metastases
Even though adenocarcinoma of the prostate gland is the commonest malignant tumour of the prostate gland that is encountered in all countries globally, other rare tumours of the prostate gland do exist and because of their rarity most clinicians would not have ever encountered such rare tumours during their training and their practices. Serum prostate specific antigen tests tend to be undertaken globally in screening for early detection of adenocarcinoma of the prostate gland globally because most adenocarcinomas of the prostate gland tend to be associated with high serum prostate specific antigens in comparison with lower serum PSA levels that tend to be found in majority of individuals of the same age group who do not have adenocarcinoma of the prostate gland. Malignant peripheral nerve sheath tumour (MPNST) of the prostate gland is a rare malignant that tends to be sporadically diagnosed and quite often the tumour to be diagnosed at an advanced stage or locally advanced stage as well as the tumour has tended to portend an aggressive biological behaviour and poor prognosis. MPNST can be diagnosed in some patients who are younger than the ages of individual adenocarcinomas but the tumour can also be found in individuals whose ages are similar to ages of individuals who have adenocarcinoma of the prostate gland. MPNST may be diagnosed incidentally in some individuals who do not have any symptoms, and they can also be diagnosed in individuals who have lower urinary tract symptoms of recent onset that is progressive, and they could also manifest with urinary tract infections, retention of urine, or symptoms related to their metastases or obstruction of the ureter or difficulty in opening their bowels. The serum PSA of patients who have MPNST tends to be low even if digital rectal examination of the patients, have demonstrated features of an abnormal prostate mass that could be firm or nodular or large and in individuals who have radiology image evidence of metastases from MPNST also tend to have low serum PSA levels but the serum PSA level could be raised when there is a contemporaneous synchronous adenocarcinoma associated with the MPNST. Radiology images that have tended to be used in assessing the prostate gland of individuals who have MPNST in various parts of the word including developing countries include: trans-rectal ultrasound scan of the prostate gland, Computed tomography (CT) scan of the prostate, magnetic resonance imaging (MRI) scan of the prostate gland. Diagnosis of MPNST tends to be made sporadically, in association with neurofibromatosis or pursuant to radiotherapy. Diagnosis of MPNST is made based upon the pathology examination features of prostate biopsies. Gross examination of specimens of MPNSTs had tended to demonstrate the ensuing features: Fusiform to globoid, pseudo-encapsulated tumour which often tend to be associated with gross evidence of necrosis. If the MPNST tumour is found to be arising from a nerve, an attached medium or large nerve tends to be evident upon gross examination. The frozen section examination features of MPNST had tended to demonstrate the following features: With regard to high grade tumours, overt features of malignancy tend to be readily found, including nuclear pleomorphism, brisk mitotic activity as well as areas of geographic necrosis; The diagnosis of low-grade MPNST lesions have tended to be difficult in frozen section examinations of the tumours. With regard to NF1, mitotic activity, increased cellularity and nuclear atypia within a neurofibroma do raise concern for the diagnosis of MPNST. Histopathology examination of specimens of MPNST have been summated to include the following: Upon low power microscopy pathology examination of MPNST, marbled appearance tends to be seen due to alternating hypocellular and hypercellular areas with perivascular accentuation tend to be seen; Uniform spindle cells with hyperchromatic, thin, wavy, or focally buckled nuclei tend to be seen; MPNST, could have uniform cellularity with fibrosarcoma-like fascicular growth, which would raise the differential diagnosis of synovial sarcoma; Specimens of MPNST could have foci of myxoid stroma and hyalinization; Epithelioid morphology can be seen upon microscopy examination in cases of MPNST, In MPNST specimens, precursor lesion, such as neurofibroma, could be identifiable; In cases of MPNST, Nuclear palisading tends to be uncommon; In cases of MPSNT, heterologous differentiation could be visualized upon microscopy examination of the specimen which might include chondrosarcomatous, osteosarcomatous and rhabdomyosarcomatous components (malignant triton tumour). With regard to the immunohistochemistry staining features of MPNST, It has been stated that specimens of MPNST tend on immunohistochemistry staining studies to exhibit positive staining for the ensuing tumour markers with the following features; Upon immunohistochemistry staining of MPNST specimens for S100 and SOX10, the specimens usually tend to exhibit patchy or focal and only seen in up to 50% of cases; Immunohistochemistry staining studies of MPNST specimens tend to exhibit positive staining for Desmin, myogenin, as well as MyoD1 within the rhabdomyosarcomatous elements of the MPNST. There is no consensus opinion on the treatment of MPNST, however, it has been stated that with regard to the treatment of MPNST, an aggressive surgical resection which is ensued by radiotherapy to achieve local control is the treatment of choice. It had also been pointed out that treatment options for the management of metastatic MPNST are limited; as well as that conventional chemotherapy had usually been limited to patients who have metastatic disease. Considering the MPNT of the prostate gland is an aggressive tumour and the fact that serum PSA levels tend to be low in such tumours, a high index of suspicion is required to establish early diagnosis of MPNST at a lower stage by undertaking thorough assessment of all patients who manifest with severe lower urinary tract symptoms with benign, firm prostates and low serum PSAs by undertaking radiology image biopsies of the prostates early whilst treating them with medications including tamsulosin to reassure patients they have benign disease or MPNST of the prostate gland or a different type of prostate cancer. A global multi-centre trial of radical prostatectomy with complete excision of the tumour plus a combination of radiotherapy and chemotherapy for localized tumours would be recommended as well as a global multi-centre trial of various combination chemotherapy options would be required for the treatment of metastatic MPNSTs as well as development of new effective chemotherapy medications would be recommended for the treatment of MPNSTs of the prostate gland..
Hsieh et al. [1] iterated that prostate cancer is one of the commonest malignancies in males, which is important to identify male patients who have enlarged prostate. Serum prostate-specific antigen (PSA) level is stated to be one of the key examinations to screen the malignancy potential. [1] The majority of prostate cancer is adenocarcinoma, but there are still some uncommon malignancies developed from other origins [2] Hsieh et al. [1] also stated that in view of their non-acinar origin, the serum PSA level is typically not elevated in cases of malignant peripheral nerve sheath tumour (MPNST) of the prostate gland. Based upon this a high index of suspicion is said to be required as well a thorough examination of prostate biopsy specimens is required in order to establish a diagnosis of this rare tumour and because of the rarity of the tumour, it would be envisaged that majority of clinicians would not have encountered a case of the rare tumour before during their training and in their practices and they would also tend not to be familiar with the clinical and diagnostic features as well as the treatment and treatment outcome of the tumour. The ensuing review of the literature on MPNST of the prostate gland has been divided into two parts: (A) Overview and (B) Miscellaneous Narrations and Discussions Related to Some Case Reports, Case Series and Studies Related to MPNSTs of the Prostate Gland.
Aims
To Review and Update the Literature on MPNST of the prostate gland.
Internet data bases were searched including: Google; Google Scholar; PUBMED; and Yahoo. The search words that were used included: Malignant peripheral nerve sheath tumour of the prostate gland and prostatic malignant nerve sheath tumour. Sixty-five (65) references were identified which were used to write the article on MPNST of the prostate gland that has been divided into two parts: (A) Overview and (B) Miscellaneous Narrations and Discussions Related to Some Case Reports, Case Series and Studies Related to MPNSTs of the Prostate Gland.
[A] Overview
Definition / general [3]
Essential features [3]
Sarcoma with peripheral nerve sheath differentiation with typically aggressive behaviour [3]
Can occur in the following settings: [3]
Morphology: marbling at low magnification (alternating areas of hypocellularity and hypercellularity) with perivascular accentuation, uniform cytologic features [3]
Heterologous differentiation in 10 - 15% of cases [3]
Rhabdomyoblastic differentiation associated has been stated to be associated with adverse clinical behaviour. [8]
SOX10 and S100 IHC only seen in 50% of cases [3]
Terminology
It has been iterated that the terminologies that have been utilized for MPNST include the following [3]
Epidemiology
The epidemiology of MPNST had been summated as follows: [3]
It has been iterated that MPNST could occur within the ensuing settings: [3]
Plexiform neurofibroma is a common precursor lesion in patients who have NF1 [3]
It had been pointed out that other nerve sheath tumours (schwannoma, ganglioneuroma) could rarely give rise to secondary MPNST. [3] [12] [13] [14] [15]
Sites [3]
Pathophysiology [3]
It has been iterated that Germline mutations in NF1 does predispose to the development of peripheral nerve sheath neoplasms in patients who have type 1 neurofibromatosis [3] [16]
It has been iterated that with regard to the setting of NF1, lesions often tend to arise from plexiform neurofibroma [3] [16]
Clinical features [3]
It has been pointed out that there is no sex predilection for the development of MPNST. [3]
It has been iterated that patients who have NF1 tend to be typically younger in comparison than their sporadic and radiotherapy-associated counterparts [3] [18]
Diagnosis [3]
With regard to the diagnosis of MPNST, it has been iterated that histopathology Histologic evaluation is necessary but not always specific and requires correlation with clinical and radiologic findings [3]
It has been pointed out that helpful features for the diagnosis of MPNST do include close association with peripheral nerves and a history of NF1 or precursor lesions [3]
Radiology description features [3]
Association with a large peripheral nerve or neurofibroma on MRI [3]
FDG PET avid; not specific but can help distinguish MPNST from neurofibroma [19] [20]
Prognostic factors [3]
The prognostic features of MPNST had been summated as follows: [3]
Assessment and Investigations
Haematology Blood Tests
Full blood count and ISR
All individuals who have lower urinary tract symptoms including all individuals who have MPNST of the prostate gland do undergo routine haematology blood tests of full blood count and ISR, and the results could tend to be normal but those who have anaemia would be treated for anaemia and the cause of the anaemia would be thoroughly investigated.
Biochemistry Blood tests
Serum Prostate Specific Antigen.
Serum Prostate Specific Antigen (PSA) levels are undertaken in all cases of prostatism due to the fact that majority of prostate cancers are adenocarcinomas which tend to be associated with high PSA levels, and hence serum PSA levels are utilized in the screening for prostate cancer and individuals who have raised serum PSAs do undergo prostate biopsies to ascertain the pathology features of the prostate including confirming that the individual has adenocarcinoma of the prostate gland.
There are rare cancers of the prostate gland that tend to be associated with low serum PSA levels and hence clinicians need to bear this information in mind in order to investigate patients who have abnormal digital examination findings of the prostate with low PSA, those who have had radiotherapy as well as those individuals who have neurofibromatosis and lower urinary tract symptoms so that they can let such selected patients as well as younger patients who have severe lower urinary tract symptoms undergo prostate biopsy in order to diagnose MPNST at an early stage.
The level of PSA does not predict presence or absence of MPNST of the prostate gland. Nevertheless, an individual who has contemporaneous, synchronous adenocarcinoma of the prostate gland in addition to MPNST could have raised levels of serum PSA.
All individuals who have lower urinary tract symptoms including all individuals who have MPNST of the prostate gland do undergo routine biochemistry blood tests including CRP, Serum urea and electrolytes, eGFr, liver function tests, bone profile, and blood glucose, and the results could tend to be normal but those who have abnormal results would be investigated, and treated to provide improvement in their biochemistry functions. And those who have obstruction of their ureters would have insertion of nephrostomy or ureteric stents. Those who have urinary retention would be catheterised and some of them could undergo trans-urethral resection of prostate (TURP) to enable spontaneous voiding. .
Microbiology
Urine
Radiology
Chest radiography
Ultrasound scan
Trans-rectal ultrasound scan of prostate
Ultrasound scan of renal tract, abdomen and pelvis
Computed Tomography Scan
Computed tomography (CT) scan of renal tract, abdomen and pelvis is a common radiology image procedure which tends to be undertaken in the initial assessment of individuals who have MPNST to ascertain the size of the prostate and imaging features of the prostate as well as presence or absence of lymph node metastasis or metastasis elsewhere in the abdomen and pelvis.
CT scan of the thorax, abdomen and pelvis, and renal tract also tends to be undertaken in the follow-up assessment of individuals who have undergone treatment for MPNST of the prostate gland in order to ascertain progress of the disease and to establish if there is development or progress of metastasis.
CT-scan guided-biopsies tend to be undertaken in many places in the world but these days this has been superseded by the undertaking of MRI scan of the thorax, abdomen, and pelvis within a number of developed countries that have facilities for the undertaking of MRI scan.
Magnetic Resonance Imaging (MRI) scan
Magnetic Resonance Imaging (MRI) scan of renal tract, abdomen and pelvis is a common radiology image procedure which tends to be undertaken in the initial assessment of individuals who have MPNST to ascertain the size of the prostate and imaging features of the prostate as well as presence or absence of lymph node metastasis or metastasis elsewhere in the abdomen and pelvis.
MRI scan of the thorax, abdomen and pelvis, and renal tract also tends to be undertaken in the follow-up assessment of individuals who have undergone treatment for MPNST of the prostate gland in order to ascertain progress of the disease and to establish if there is development or progress of metastasis.
MRI-scan guided-biopsies tend to be undertaken in some developed areas with facilities for MRI scan
MRI scan of the prostate gland does tend to provide more detailed information about the prostate gland in comparison with ultrasound scan and computed tomography scan of the prostate and in many well established Urology Departments in developed countries MRI scan of the prostate gland is utilized to scrutinize the prostate gland so as to undertake template biopsies of the prostate which does include biopsies being taken from targeted lesions found in areas where prostate cancer does not usually develop.
Isotope Bone Scan
Isotope bone scan is a routine radiology imaging procedure that tends to be undertaken globally to ascertain whether there is bone metastasis or not in cases of prostate cancer including MPNST.
Positron Emission Tomography Computed Tomography (PET-CT) Scan
PET-CT scan is a radiology imaging procedure that is undertaken to ascertain if there is development of recurrence of tumour or metastases and this radiology imaging procedure tends to pick up recurrent and metastatic tumours that are too small to be identified by conventional CT scan of thorax, abdomen, and pelvis (CT-TAP).
Treatment [3]
The treatment localized and metastatic MPNST have been summated as follows: [3]
Macroscopy (Gross) description [3]
It has been iterated that macroscopy examination of specimens of MPNSTs had demonstrated the ensuing features: [3]
Fusiform to globoid, pseudo-encapsulated tumour which often tend to be associated with gross evidence of necrosis If the tumour is found to be arising from a nerve, an attached medium or large nerve tends to be evident upon gross examination
Frozen section description [3]
The frozen section examination features of MPNST had been summarized as follows: [3]]
Microscopic (histopathology) description [3]
During low power microscopy pathology examination of MPNST, marbled appearance due to alternating hypocellular and hypercellular areas with perivascular accentuation tend to be seen. [3]
Uniform spindle cells with hyperchromatic, thin, wavy, or focally buckled nuclei [3]
MPNST, could have uniform cellularity with fibrosarcoma-like fascicular growth, which would raise the differential diagnosis of synovial sarcoma [3]
Specimens of MPNST could have foci of myxoid stroma and hyalinization
Epithelioid morphology can be present in cases of MPNST [3]
In MPNST specimens, precursor lesion, such as neurofibroma, might be identifiable [3]
In cases of MPNST, Nuclear palisading tends to be uncommon [3]
In cases of MPSNT, heterologous differentiation could be visualized upon microscopy examination of the specimen which might include chondrosarcomatous, osteosarcomatous and rhabdomyosarcomatous components (malignant triton tumour) [3]
In cases of MPNFT, glandular elements tend to be exceedingly rare upon microscopy examination of the specimens [3] [29]
It has been iterated that proposed nomenclature for the spectrum of NF1 associated nerve sheath tumours had been summated to include the ensuing: [3] Atypical neuro-fibromatous neoplasm of uncertain biologic potential (ANNUBP): [3] In ANNUBP, at least 2 of the ensuing features tend to be found: cytologic atypia, loss of neurofibroma architecture, hypercellularity, > 1/50 HPF and < 3>
Cytology description [3]
Some of the cytology examination features of specimens of MPNST have been summated as follows: [3]
Positive immunohistochemistry stains [3]
It has been stated that specimens of MPNST tend on immunohistochemistry staining studies to exhibit positive staining for the ensuing tumour markers with the following features: [3]
Negative immunohistochemistry stains [3]
It has been iterated that immunohistochemistry staining for MPNST specimens does demonstrate negative staining for various tumour markers as follows; [3]
There tends to be loss of nuclear H3K27me3 within high grade sporadic and radiotherapy-associated tumours [3]
The sensitivity tends to be lower in low grade and NF1 associated- MPNST and complete loss has been reported in 88 out of 122 tumours that amounted 72% of the tumours and mosaic / partial loss within 23 out of 122 tumours that amounted to 19% of the tumours, loss of expression in 47 out of 68 tumours that amounted to 69% of the tumours [32] [33]
Loss of nuclear IN11immunoreactivity had been reported in a large subset of epithelioid MPNST which included 3 out of 6 tumours that amounted to 50% of the tumours, and in 35 out of 52 tumours that amounted to 67% of tumours. [3] [6] [7]
Molecular / cytogenetics description [3]
The molecular and cytogenetics examination features of MPNST have been summated as follows: [3]
MPNSTs are Cytogenetically complex sarcomas [3]
Inactivating mutations in CDKN2A / CDKN2B and PRC2 had been found in MPNSTs [3] [34] [35]
Germline NF1 mutations in the setting of NF1 had been documented.
As precursor lesions transform, they have been stated to tend to acquire additional mutations [3] Point mutations in BRAF V600 in a subset of cases of MPNSTs had been documented. [3] [36] [37] [38]
Differential diagnoses [3]
Some of the differential diagnoses of MPNST had been summated to include the following: [3]
Atypical neurofibroma [3]
Monophasic synovial sarcoma: [3]
Dedifferentiated liposarcoma: [3]
Spindle cell melanoma: [3]
Leiomyosarcoma: [3]
Neurofibroma: [3]
Low-grade fibromyxoid sarcoma.: [3]
Cellular Schwannoma: [3]
[B]Miscellaneous Narrations and Discussions from some case reports, case series and studies related to MPNST of the Prostate Gland
Hsieh et al. [1] made the ensuing iterations:
Hsieh et al. [1] reported a young man who had presented to their urology outpatient department because he was having lower urinary tract symptoms. The results of his prostate cancer survey demonstrated a markedly enlarged prostate gland that was associated with at very low serum PSA level. Pathology examination of specimens of his prostate biopsy was reported to have demonstrated features of very-rare cancer: malignant peripheral nerve sheath tumour (MPNST) of the prostate the prostate gland. Detailed report of the case was narrated as follows:
Hsieh et al. [1] reported a 44-year-old man, who did not have any systemic underlying disease who had manifested with painless visible haematuria, that was combined with urine retention some days. He had lower urinary tract symptoms (LUTS) for a number of years that had become worse recently preceding his presentation. During his digital rectal examination, a stony-hard prostate gland with markedly enlarged size was found, but his serum PSA level was found to be within the normal range (total PSA: 0.42 ng/mL). He had trans-rectal ultrasound scan of his prostate (TRUS) which demonstrated multiple nodules within his prostate gland. The largest prostate nodule measured 6.3 cm and the whole prostate gland measured about 300 grams. Architecture derangement of prostate, possible central necrosis with haemorrhage, and enlarged right internal iliac lymphadenopathy were demonstrated upon prostate magnetic resonance imaging (MRI) (see figure 1). No bony metastasis was identified upon isotope bone scan. Trans-rectal ultrasound scan-guided prostate biopsy (TRUS-guided prostate biopsy) was undertaken but massive gross haematuria ensued days pursuant to the procedure. Thus, cystoscopy for checking bleeding was undertaken and the specimen resected from the prostate gland was reported to have demonstrated features of a malignant peripheral nerve sheath tumour (see figure 2). For further staging, the patient underwent chest computed tomography (CT), which showed a solitary 0.9 cm nodule within the right upper lobe of the prostate gland.
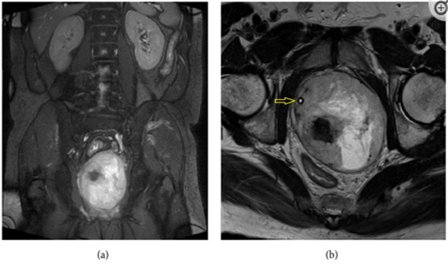
Figure 1: Prostate MRI with coronal (a) and axial (b) views showing marked enlargement of prostate gland with architecture derangement. Urethra with Foley (arrow) was shifted to the right side.

Figure 2: Microscopic findings of the transurethral resection biopsy specimen. (a) Low-power view shows spindle cells arranged in tightly packed fascicles, with alternating hypo- and hypercellular areas and geographic necrosis (H&E stain, ×40). (b) High-power view shows spindle-shaped tumor cells with hyperchromatic nuclei and frequent mitoses. Some entrapped prostatic glands are also seen (H&E stain, ×400). (c) By immunohistochemistry, the tumor cells demonstrate focal immunopositivity of S-100 protein (Immunoperoxidase, ×200) and (d) no immunoreactivity with CDK4 (Immunoperoxidase, ×200). Reproduced
Hsieh et al. [1] iterated that taking into consideration the difficulty of radical surgery due to huge size of the prostate gland, they had prescribed neoadjuvant chemotherapy, which had comprised of:5-Fluorouracil + Cisplatin + Ifosfamide for 5 cycles. Hsieh et al. [1] reported that regression of the patient’s previous lung nodule was found on his follow-up chest CT scan. The patient underwent pelvic MRI scan which demonstrated residual tumour lesion within the visible prostate gland, whose size had reduced to 83 grams. Radical cystoprostatectomy was undertaken, and invasion of tumour into the urinary bladder was found during the operation. Bilateral pelvic lymph node dissection was also undertaken and no metastasis was found. Pathology examination of the cystoprostatectomy specimen was reported as consistent with the diagnosis of MPNST. Pursuant to the cystoprostatectomy operation, Hsieh et al. [1] prescribed adjuvant concomitant chemoradiation therapy (Cisplatin + 5-Fluorouracil + Ifosfamide with external beam radiation therapy 6600 cGy, 33 fractions). The patient had a follow-up CT scan of abdomen 3 months pursuant to his operation which showed multiple ill-defined poorly enhanced nodules within his liver and a 3.5 cm gallbladder mass. Target therapy, of Pazopanib 400 mg per day, was given for palliative treatment due to suspicion of progression of his disease. Nevertheless, his clinical condition went downhill and he died three months later.
Hsieh et al. [1] made the ensuing summating discussions:
Hsieh et al. [1] made the ensuing conclusions:
Kim et al. [46] made the ensuing iterations:
Kim et al. [46] reported an extremely rare case of sarcoma of the prostate gland sarcoma in an early adulthood individual. Kim et al. [46] reported a 22-year-old man who had presented with a 2-week history of visible haematuria and voiding difficulty and who had visited the local urology clinic. He underwent digital rectal examination and transrectal ultrasound scan which demonstrated a hard mass within his prostate gland. He was referred to the urology department in the hospital of Kim et al. [46], He had magnetic resonance imaging (MRI) scan which showed a 6-cm mass within the left lobe of his prostate gland (see figure 3A [3A]). The level of his serum prostate-specific antigen (PSA) was 1.89 ng/mL (normal range 0–4.0 ng/mL). Pathology examination of his prostate core needle biopsy revealed features of a high-grade sarcoma, which was suggestive of poorly differentiated synovial sarcoma (SS).
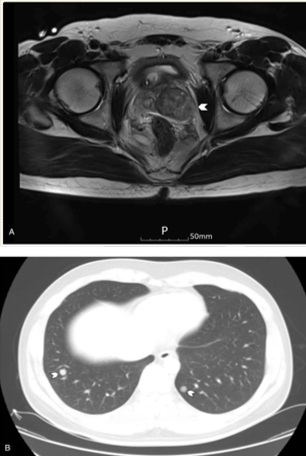
Figure:3
Magnetic resonance imaging (A) at diagnosis showed a 6-cm mass in the left lobe of the prostate, and (B) at recurrence showed multiple nodules in the lungs. Reproduced from:
[46] Kim H, Kim DY, Seol YM, Ku JY, Choi KU, Choi YJ. Primary malignant peripheral nerve sheath tumor of prostate in a young adult: A case report. Medicine (Baltimore). 2018 Sep;97(39):e12040. doi: 10.1097/MD.0000000000012040. PMID: 30278486; PMCID: PMC6181477. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6181477/ ] Copyright © 2018 the Author(s). Published by Wolters Kluwer Health, Inc. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal. http://creativecommons.org/licenses/by-nc-nd/4.0
He had Positron emission tomography-computed tomography (CT) on November 30, 2016 did not demonstrate any evidence of regional lymph node metastasis or distant metastasis. The patient underwent laparoscopic prostatectomy on December 6, 2016. Pathology examination of the prostatectomy specimen showed that the resection margin was positive, for the tumour which indicated R1 resection. The main differential diagnosis was documented by the pathologist to have included MPNST and synovial sarcoma (SS). SS was suspected more on the previous core needle biopsy because the tumour cells had exhibited negative immunohistochemistry staining for S100 protein, but it had exhibited positive staining for pan-cytokeratin (see Figure 4A [4A]). The resected tumour was reported not to have shown the presence of SYT-SSX fusion transcripts upon reverse transcription polymerase chain reaction, however it had exhibited focal immunoreactivity for S100 protein (see Figures 4B and 4C). Based upon the pathology examination features of the tumour, the tumour was reported to have shown features that were compatible with MPNST based on the microscopic findings, and also upon the results of ancillary studies.

Figure:4
Microscopic findings of the prostatectomy specimen. (A) The tumor was composed of fascicles of spindle cells showing alternating hypercellular and hypocellular areas, and heterologous cartilaginous differentiation (center) (H&E, ×40). (B) Malignant spindle cells showed hyperchromatic nuclei and numerous mitoses (H&E, ×200). (C) Immunohistochemistry showed focal staining for S100 protein (×200). Reproduced from: [46] Kim H, Kim DY, Seol YM, Ku JY, Choi KU, Choi YJ. Primary malignant peripheral nerve sheath tumor of prostate in a young adult: A case report. Medicine (Baltimore). 2018 Sep;97(39):e12040. doi: 10.1097/MD.0000000000012040. PMID: 30278486; PMCID: PMC6181477. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6181477/ ] Copyright © 2018 the Author(s). Published by Wolters Kluwer Health, Inc. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal. http://creativecommons.org/licenses/by-nc-nd/4.0
He was referred on to the oncology department, and adjuvant radiotherapy was planned. Nevertheless, he had computed tomography (CT) scan on January 1, 2017, preceding his radiotherapy, which demonstrated multiple pulmonary metastases with local recurrence and peritoneal seeding (see figure 3B [3B]). He received a chemotherapy regimen of doxorubicin and ifosfamide and his disease had shown partial response to 3 cycles of the regimen. Nevertheless, he did complain about having severe general weakness and poor oral intake, and therefore, was switched on to doxorubicin monotherapy. He received 3 cycles of doxorubicin monotherapy. His disease was reported to be stable during the administration of his chemotherapy; nevertheless, his disease had progressed 2 weeks after the last dose of his doxorubicin. He received second-line pazopanib chemotherapy treatment, but his tumour did not show any response, and third-line gemcitabine and docetaxel were also associated with no response. The patient further administered everolimus and olaratumab with doxorubicin, but his tumour continued to progress. He died 9 months pursuant to his surgery on September 4, 2017.
Kim et al. [46] made the following summating discussions:

Reproduced from: [46] Kim H, Kim DY, Seol YM, Ku JY, Choi KU, Choi YJ. Primary malignant peripheral nerve sheath tumor of prostate in a young adult: A case report. Medicine (Baltimore). 2018 Sep;97(39):e12040. doi: 10.1097/MD.0000000000012040. PMID: 30278486; PMCID: PMC6181477. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6181477/ ] Copyright © 2018 the Author(s). Published by Wolters Kluwer Health, Inc. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal. http://creativecommons.org/licenses/by-nc-nd/4.0
Ferakis et al. [54] stated that malignant Peripheral Nerve Sheath Tumour (MPNST) is a extremely rare soft tissue sarcoma as well as that sarcomas of the prostate gland are very rare. Ferakis et al. [54] iterated that they were reporting the first case of simultaneous prostatic adenocarcinoma and MPNST in the English literature. Ferakis et al. [54] reported that in December 2015, a 60-year-old man had visited the outpatient clinic of their department for routine urology examination. His past medical history had included hypertension, diabetes mellitus, acute myocardial infarction three years earlier, and ischemic cerebrovascular accident thirteen years earlier. He had digital rectal examination, which demonstrated that his prostate gland was painless, asymmetrically sizable, and tough, with no other clinical findings. The results of the patient’s full blood count and blood chemistry levels were reported to be within the normal range. His serum PSA level was 1 ng/mL He had transabdominal ultrasound scan which showed a solid, large mass, that was in contact with his urinary bladder. The volume of the prostate gland volume was 31 mL and his postvoid residual of urine volume on scanning was 62 mL. He had abdominal/pelvic computed tomography (CT) scan, which showed the presence of a solid, lobed, well-circumscribed mass, which had arisen from the left peripheral zone of his prostate gland and a possible infiltration of his left seminal vesicle. The wall of his urinary bladder was noted to be normal and the distal part of his left ureter had crossed between the mass and the urinary bladder wall. He had trans-rectal ultrasound-guided biopsy of his prostate gland and pathology examination of the biopsy specimen demonstrated a smooth muscle tumour with uncertain malignant potential (STUMP). He had magnetic resonance imaging (MRI) scan which demonstrated a fusiform, lobed, well-circumscribed, 6.5 cm × 6.5 cm × 6.0 cm in size mass, that had regular borders, which had arisen from the left peripheral zone of his prostate gland. The mass was found to have compressed the rectum, the posterior wall of the urinary bladder, and the left seminal vesicle/vas deferens. The lesion was reported to have a hyperintense signal upon T2-weighted sequences and hypointense signal upon T1-weighted sequences and it had contained thin septa. The adipose tissue encompassing the lesion was not infiltrated. There was heterogeneous enhancement of the lesion’s lobules following intravenous administration of paramagnetic contrast agent. He had Computed tomography (CT) scan of his thorax and isotope bone scan which were negative. The patient underwent 18-fluorodeoxyglucose-positron emission tomography (18-FDG-PET-CT) from the base of the skull to the mid-thigh, which demonstrated abnormal uptake within the prostatic mass. He had MRI scan of abdomen and CT scan of his thorax which were normal three months postoperatively and the patient had received adjuvant radiotherapy. His serum PSA level was 0 ng/mL. The patient was reported to have no signs of relapse and he was is in good general condition 6 months pursuant to his operation.
Ferakis et al. [54] made the ensuing summating discussions:
None
[1] Case Reports in Urology and Hindawi Publishing Group and the authors of articles in the journal for granting permission for reproduction of figures and contents of their journal article under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
[2] Medicine (Baltimore). For granting permission for reproduction of contents of their journal article as well as figures and tables under Copyright © 2018 the Author(s). Published by Wolters Kluwer Health, Inc. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal. http://creativecommons.org/licenses/by-nc-nd/4.0
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
