AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Sheehama Jacob, Department of Public Health, University of Namibia, Oshakati, Namibia, School of Health Sciences, Cardiff University, Wales, UK.
Citation: Tuyapeni Sharon Grace, Sheehama Jacob and Hermine Iita, (2022), Malaria Infection Socio-Economic Factors in the Outpatients in District Hospitals, Sub-Saharan Africa. J. Biomedical Research and Clinical Reviews. 8(2); DOI:10.31579/2692-9406/149
Copyright: © 2023, Sheehama Jacob. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 March 2023 | Accepted: 21 March 2023 | Published: 28 March 2023
Keywords: malaria; transmission; infection; prevention
Background: Malaria has become a threat in Namibia,more especially in Engela Districtsince 2010, with cases being reported to increase and the number of deaths rising as well. With the rising of these cases, the economy was slowly decreasing due to purchasing of mosquito nets, repellents and others. Based on a malaria case investigation done in Namibia for 5 years, it is stated that the incidence fell from 53.6 to3.6 cases per 1000 population, and then increased again to 47.3/1000.
Method: A preliminary search will be conducted in the databasessuch as: GoogleScholar, the PubMed,and the Library. This scoping review was also conducted by using key words such as malaria, social factors, economic factors, effects and outpatients. Scoping review framework used in the study is by Joanna Briggs Institute that will be followed throughout the review process and the reporting of the main reviewwill follow the PRISMA-ScR.
Results: The evaluation of the studies that have occurred some have indicated gaps in their research due to reasons unknown. The use of long lasting insecticide nets was indicated although not all were in accordance with the WHO requirements of malariaprevention. Lack of income, strongsocial support was also observedand indicated to be the major cause of Malariain many areas of the world.
Conclusion: This scoping review will assist in the mapping out of evidence on the socioeconomic factors of malaria effects on outpatients which can help out the Health Professional with the right approaches to be used in terms of elimination of malaria, educating the patients about malaria itself before prescribing them medications.
Malaria is a major public health problem in the world where cases are also increasing and recorded. Based on the latest World malaria report, released in December 2019, there were 228 million casesof malaria in 2018 comparedto the 231 million cases in 2017. The estimated number of malaria deaths stood at 405 000 in 2018, comparedwith 416 000 deaths in 2017.
There were 228 million estimatedcases malaria worldwide and the estimated number of malaria deaths stood at 405 000 in 2018 as well. Children with ages below 5 years are the most vulnerable group affected by malaria; in 2018, they accounted for 67% (272 000) of all malaria deaths worldwide. The African Region carriesa disproportionately high share of the global malaria burden. In 2018, the region was home to 93% of malaria cases and 94% of malaria deaths. Total funding of malaria control and elimination reached an estimatedUS$ 2.7 billion in 2018. Contributions from governments of endemic countriesamounted to US$ 900 million,representing 30% of total funding. In 2018, 6 countries accounted for more than half of all malaria cases worldwide: Nigeria (25%), the Demographic Republicof the Congo (12%),Uganda (5%), and Cote d’Ivoire,Mozambique and Niger (4% each).Most importantly, malariais typically found in tropicaland sub tropicalclimates where the parasites can live. The WHO statesthat, in 2016, there were an estimated 216 million casesof malaria in 91 countries.
In the United States, the Centers for Disease control and Prevention (CDC) reported 1700 cases of malaria annually. Most cases of malaria develop in peoplewho travel to countries where malaria is more common. [1]
Malaria remains a major global public health concern, as in 2014, an estimated 214 million cases and 438 000 deaths were reported worldwide, hence the significance of the research is to improve and engage in more efficient solutions on how to eliminate malaria, to decrease the death cases of malaria and educate the population on the dangers of malaria and its prevention and control measures altogether. The research will also serve as an educational platform and implication of changes on how to control transmission of malaria from other African countries at the borders.
It appears that factors influencing malaria includes lack of long –lasting insecticide treated nets, poor hygienic surrounding with the presence of swamps, grass, and wastes, poor education on malaria. It is mostly believed to be influenced by the fact that some people are ignorant to signs of malaria, uneducated and also ignorant when it comes to taking prevention measures of malaria. Future consequences of Malaria may include severe malaria, which is deadly, increase in number of death cases and increasedgovernment expenditure towards malaria in terms of medication and nets. The other social and economic factors that can increase malaria and its cases include whetherthe outpatients are most likelyto live in rural areas,they lack enoughresources to acquire required protective gear of malaria like mosquito nets as mentioned earlier, it is also believed to be influenced by alcohol abuse by the people who in the end run out of money, use of traditional treatment of malaria is also believedto have an impact and lastly they might be uneducated. [2]
Study design
It evaluates and assesses the socioeconomic factorsof Malaria on outpatients. This qualitative scopingreview protocol was done followingthe Joanna Briggs Institute, (JoannaBriggs Institute, 2015) methodology scoping reviews. Collection of information from the library books, journals and websitessuch as chrome,Google scholar will be used. This will be done following five stages such as: identifying the research question, identifying the relevant studies,study selection, chartingof data and collating, summarizing and reporting the results and an optional step of a consultation which is to validate the findings from the scoping review.
Study Population and Period of Evaluation
The study population used included all those articles that ranged from 2006 to 2020 were included in the study. All articles that were written in English and were in correlation with the study’s objectives, aims and title were included in the study. It considered also both the published and unpublished studies,and it was done using words like socioeconomics, malaria,effects and outpatients. The databases used and chosen contained due studies relevantto the research question. [3]
Study Sites
Amongst all those continents where Malaria existed,the articles done in Sub- SaharanAfrica were used as a site due to the fact that it containedmuch cases and deaths due to Malaria. These articles all ranged or came from different departments including Epidemiology, Public Health, Economics, Science and many others.These sites were all part of the same continent that contained similarclimates, weather and economic status,as they were easier to compare and locate. [4]
Descriptions Of Interventions and Contributing Factors Education level
This indicated that those who had formal education about malaria or just different types of diseases in particular are less likely to get malaria as they know all about its prevention measures, and those who lacked formal education tend to get more sick due to the fact that they might not get jobs to support their families and buy measures to prevent against malaria such as building houses with proper windows and doors.
Age
The young people with ages between 15 and 27 are more at least of malaria as they tend to be more ignorant in its prevention, treatment and health education campaigns. Although all ages can be infected or can get malaria especially babies and the elderlyor those with low immune system.
Attitudes
Those with the wrong attitude towards malaria are more likely to suffer the consequences of malaria. This involves not taking part in any of malaria programs such as having your house sprayedagainst mosquitoes, not attending health education or so on.
More research needs to be done on the socioeconomic factors of malaria as malaria cases keep increasing every now and then as it has become an everyday thing or occurrence. Some studies focused on general factors of malaria only, others on socioeconomics whilst others focused on both the factors which results in less information being given to each of the factors individually. [5]
Data Collection Procedures
During the study period, all the articles with similarities with the title of the study were being recorded in a table form and described according to their findingsand characteristics. In all the sites or articles, eligibility and screening was being used to identified the most needed and important articles.The table below shows the results and hw the data was collected:
| Author | Main characteristics and findings |
| Shr-Jie Wang | A cross sectional study, with a sample size of 200 and controls of 200 in total as well. The Plasmodium falciparum infection ranged in a total of 1 054 subjects and only 705 were mainly children under 5. 425 subjects declared havinghad a malaria attack withinone month of the survey. Among them, 60.7%were treated by traditional herbs and healers, 27.8% in health facilities, while 5.2% of the sample population only purchased drugs in a pharmacy or a drugoutlet. The prevalence of malaria parasites was low: 0.8%, 1.4%, 2.7% and 3.7% in the centre, intermediate, periphery and surrounding rural areas, respectively. Health facilities surveysshowed that only37/717 (5.2%) of presenting fevercases and 22/781(2.8%) of non-fever cases. A remarkably high coverage of insecticide-treated nets and a corresponding reduction in malarial infection risk were found.(13) |
| Anne Caroline Krefis, Norbert Georg Schwarz | A diagnostic assessment with a sample size of 1496 children and adults. It was found that those factors indicating the family's socioeconomic status the proportion of literate fatherswas very high(> 75%) and evenly distributed under children withand without malaria. Likewise, the variables "house type", "income manage", "membership in a health insurance", "existence of an indoor kitchen" and "mother's |
and father's occupation" did not showany distinct association with malaria (Seeadditional file 1 describing characteristics of the study group). In the univariate analysis, the variables "existence of electricity", "indoor toilet", "use of freezing as food conservation", "mother's ability to readand write" anda "closed water supply" were negatively associated with malaria odds (OR = 0.72, OR = 0.67, OR = 0.63, OR = 0.68, OR = 0.70, respectively, all p-values < 0 xss=removed> in children from families, which reported the use of mosquito protection measures | |
| Ivan Mboambogoh Yakum, GodfreyForgha Njimanted | A cross sectional studyand indicator surveywith a samplesize of 400 households. Thisstudy found thatamongst the respondents’ knowledge of malaria prevention methods, 0.75% of the respondents indicated that they did not know how best malaria can be prevented, 25% of the respondents indicated good personal hygiene as the best way of preventing malaria, 18.3% of them indicated that malaria can be prevented by avoiding excessive heat, 0.3% of them said malaria can be prevented while 5% of them indicated that it can be preventing through eating balanced diet. Amongst all the respondents on ways tobest prevent malaria, the study found that 56.6% indicated that the best way is to clear bushes around while 28.7% of them indicated creating a good drainage system as the best way to prevent malaria and 17% of them indicated the use of insect sprays to be the best practice to prevent malaria. Among the measures to prevent mosquito bites, 30.5% of the respondents indicated always closing doors and windows, 34.8% of them indicated the use of repellents, 15.8% of them indicated the fitting of nets on doors and windows (housemodification) and 92% of themindicated sleeping under ITNswhile 26% of them indicated the frequent useof anti-malaria drugs.However, among themeasures indicated, measures best known by the respondents are firstly theuse of ITNs,secondly clearing of bushes aroundand thirdly the use of repellents. The finding also involves the fact that many households chose malaria prevention options that is free(34.3%), seconded by those thatare cheaper (26.5%), then those thatchoose because it is the one they know (20.8%), those that choose because it is readily available (19.3%), no particular reason (6.3%) and lastly those that prefer an optionbecause it is effective (1.3%). |
Pascalia Chanda, Marianela Castillo- Riquelme | An observational study, which had indicated that about 60 ResultsThe findings of the study were presented in tables, narrative summaries as well as figures. The 10 used studies and their findings are summarized into different categories for easier identification and are denoted by descriptive labels. The following tables and figures represent the possible contributing general factors and socioeconomic factors based on the number of studies that acertain factor has appeared in. 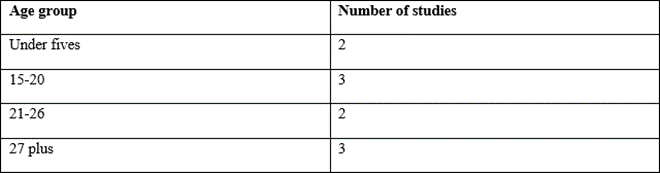 Table 1: Number of studies per age group of outpatients (n=10) Sixty percent of the viewed studies studied and concentrated more on the working youth and education level, making it a much contributing factor to malariaother others. Others also found that being unemployed contributes to malariaillness too. 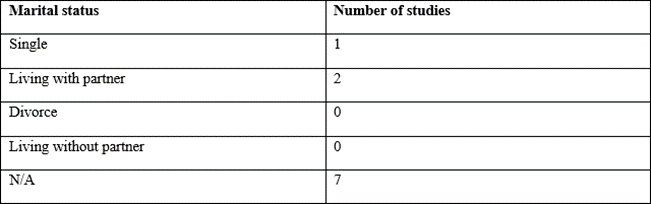 Table 2: Number of studiesfocusing on marital status(n=10) Majority of studies included and concluded that whetherbeing single, marriedor not, malariadoes not discriminate, hence it can affect anyone,although the socioeconomic factors mostly affectedsingle people.  Table 3: Education levelon the symptoms and treatment of malaria (n=10) The lack of formal education on malaria has lead to the increasein malaria cases, the spread and deaths. Majority of those that lack knowledgeon malaria have suffered the consequences. 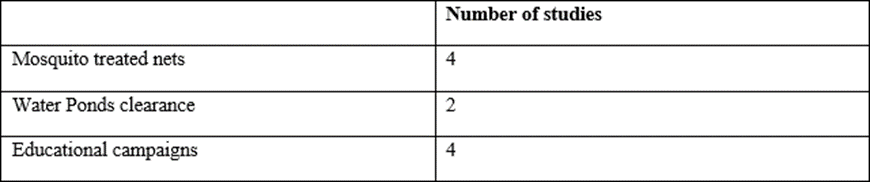 Table 4: Actions taken against malaria (n=10) These actionshave been indicated by many studiesto be the contributing factorsof malaria as they were never done or taken into consideration by community members.  Table 5: Sources of bed nets (n=10) Studies have found that majority of own nets that are used have contributed greatly to the spread and increase of cases of malaria in Sub-Sahara. DiscussionAccording to a research on “Cost effectiveness analysis of the available strategies for diagnosing malaria in outpatients”, and another research by Obumneke A. Obieche,it is stated that the treatments and diagnosis procedures of Malaria were too much expensive for the outpatients to undergo, hence the slow progression involved in eliminating the health condition for good. Furthermore, those patients with health care insurance found the treatments very affordable and others without the insurances thought otherwise. Based on certain read article, it is stated that the highest costs of malaria treatmentdone affected the patients in such a way that many failed to undergo for tests, days were lost for that and lastly, earnings were foregone.It also accountsfor 15% of health relatedabsenteeism from school.Malaria’s cost is not entirely due to the fact that the outpatients could not afford it, but it is also due to the fact that they do not necessary considerit to be that much of a problem or of higher concern for them, hence without malaria confirmation, it is difficult to exclude fevers, which are not due to malaria, thus the true burdenof the disease proves difficultto quantify, whileObumneke A. Obieche stated that despite the provision of free malaria services, households incur significant direct and indirect costs associated with the disease. Lastly, once the bread winner of the family gets malaria, they might lose their jobs due to too much absenteeism and the family members fail to pay for health care spending for treating the person, lack of moneyto buy bread occurs. The malaria drainsthe resources of families and overall, households in Africa lose up to 25% of incometo the disease. [8] The mentioned and searched studiesidentified different socioeconomic factors of malaria, although there are some studies that found out same or similar factors such as low income level, low and lack of formal education, house qualities and geographical access to health care facilities. There are a number of increasing cases of malaria indicated in the studies which are caused mostly by lack of awareness to malaria, absence of treated mosquito nets, malariacampaign programmers in most affectedand at-risk communities and also negligence among the people. These studies were all done in similar regions or countries in the Sub-Sahara, which are all the risk of getting malaria and having low or moderate economic rates and other unmentioned characteristics. Malaria cases are tracked in different ways in order to treat, prevent or minimize the spread of its transmission through ways such as house visits of both the suspected and confirmed case by healthprofessionals, outreach points such as health centers or community halls for health education and distribution of mosquito nets and spray days and finally also at the hospital were the victimgoes him/ herself for tests. When it comes to comparing these findings to Namibia, given that they were done in all the Sub-Saharan region of which Namibia is a part of, we can conclude that these factors are also likely to occur in Namibia since they all share similar weather conditions, economic rates and developing nations. Although this was the case, some socioeconomic factorsand study review of cases occurrence and knowledge done in Namibia are not so similar or common in other countries, but this is not much of a bigger problem as they can be concluded to not being exactly the same, given that each of these countrieshave their own differentclimate conditions, healthcare systems and settingsand also their profiles differs. 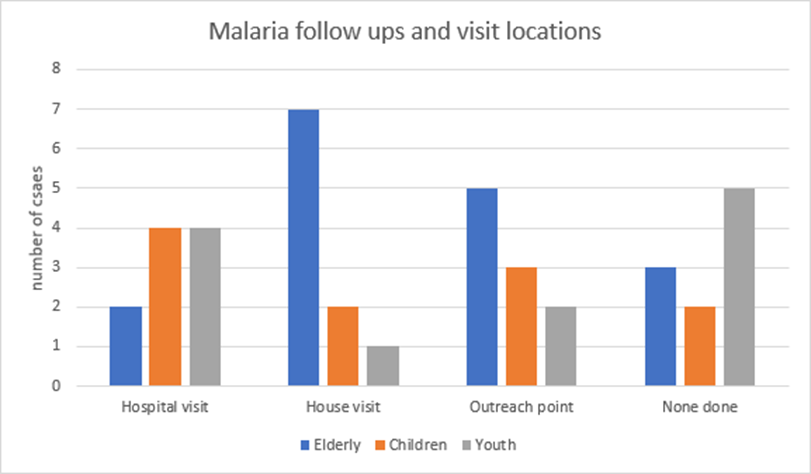 Figure 1: Malaria followsup visits Studies have shown that malaria casesor visits among the youth that have not been done are mostlythe ones affectedby malaria, but it does not mean that other age groupsare safe. They too are atrisk of getting malariaif no visits have been done at either health points. 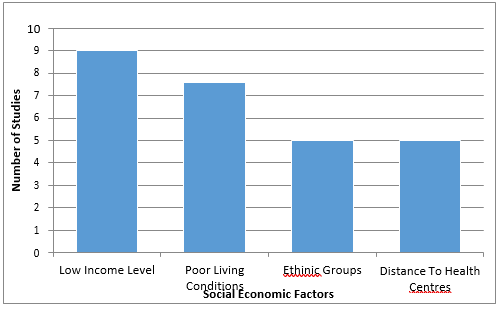 Figure 2: Socioeconomic factorsof Malaria Studies have indicated and found that the above socioeconomic factors, although not all were mentioned, are the major causes of malaria in especially people living average lives and those that are considered to be poor. LimitationsThese are influences or certain factors that a researcher is unable or cannot control at all duringthe research. These involve the conditions or influences, shortcomings that cannot be controlled by the researcher and tends to place restrictions on the researcher’s conclusions and methodology during the conduction f the research. Impressions and conclusions of or about the generality and effectiveness of the findings cannot be made due to the fact that a scoping review does not by any way formally evaluate the quality of evidence and they also often gather evidence from wide range of study designs and methods. Some studies have been over looked or excluded because of language used, location, titles or aims and in other cases some human errors, although efforts were made and done in order to access and review the relevant studiesto be used. Finally, the researcher could not fullycarry out the planned field research study due to the state of the emergency or lock down brought about by COVID-19. [9] ConclusionIn conclusion, research on socioeconomic factors of malaria has increased although not only in sub Saharan regions but also in other partsof the world those have the mosquito Plasmodium that causes malaria, even though not all countries have really placed much effort in preventing or overcoming malaria. The focus of malaria should be more on the less advantaged groups such as those with low income levels or those that do not earn a thing, pregnantmothers and their unborn babiesas they tend to be more at risk, also on communities with the highest occurrence of malaria cases due to the presence of mosquitoes, the youth as well since they are more at risk due to their negligence and lack of participation in malaria control programs and also on other factors that were less considered in the reviewed studies. The governments of these countries need to be more effort and much money on carryingout prevention measuresof malaria such as the provision of insecticides treated mosquito nets, giving out health education on how the communities can protect themselves from malaria, asking for loans for their malaria programs in case they do not have enough money to carry them out on their own. The researcher has concluded that there are many factors causing malaria, not only the socioeconomic ones but also the general ones. These factors include low income distributions, lack of formal education, low quality houses,negligence, cultural factors as well as the age. [10] References

Virginia E. Koenig

Delcio G Silva Junior

Ziemlé Clément Méda

Mina Sherif Soliman Georgy

Layla Shojaie

Sing-yung Wu

Orlando Villarreal

Katarzyna Byczkowska

Anthony Kodzo-Grey Venyo

Pedro Marques Gomes

Bernard Terkimbi Utoo

Prof Sherif W Mansour

Hao Jiang
Dr Shiming Tang

Raed Mualem

Andreas Filippaios

Dr Suramya Dhamija

Bruno Chauffert

Baheci Selen

Jesus Simal-Gandara

Douglas Miyazaki

Dr Griffith

Dr Tong Ming Liu

Husain Taha Radhi

S Munshi

Tania Munoz

George Varvatsoulias

Rui Tao

Khurram Arshad

Gomez Barriga Maria Dolores

Lin Shaw Chin

Maria Dolores Gomez Barriga

Dr Maria Dolores Gomez Barriga

Dr Maria Regina Penchyna Nieto

Dr Marcelo Flavio Gomes Jardim Filho

Zsuzsanna Bene

Dr Susan Weiner

Lin-Show Chin

Sonila Qirko

Luiz Sellmann |