AUCTORES
Globalize your Research

Review Article
*Corresponding Author: YA TUO, The department of Anesthesia, The second affiliated hospital of Inner Mongolia Medical University, Hohhot, Inner Mongolia Autonomous Region, China.
Citation: Xueqiang Fu, Ya Tuo, Yanan Lv, Changxu Han, Yi Qiu, Caixia Wang (2022). Injection of local Anesthetic for Post-Operative Pain Management after Anterior Cruciate Ligament Surgery: a Systematic Review of RCTs. J. Scientific Research and Biomedical Informatics, 3(2); DOI:10.31579/jsrbi.2022/037
Copyright: © 2022 YA TUO, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 October 2021 | Accepted: 24 December 2021 | Published: 06 January 2022
Keywords: anterior cruciate ligament(acl); postoperative pain management; injection of local anesthetic; intra-articular injection; local infiltration analgesia
Background
Effective injection of local anesthetic for postoperative pain management after anterior cruciate ligament surgery in-created patients’ satisfaction.
Objectives
To collect evidence from randomized controlled trials (RCT) on injection of local anesthetic for pain management after anterior cruciate ligament surgery.
Study Design Systematic review.
Methods
A systematic literature review was performed using Cochrane Library, PubMed, Web of Science and Embase up to 2021. The end research time was Jun. 30, 2021.RCTs comparing injection of local anesthetic for pain management to other methods or placebo were included.The Cochrane Collaboration Network risk bias assessment tool was used to evaluate the literature bias.
Results
A total of 22 RCTs met inclusion criteria: 15 with only intra-articular injection, 3 with only local infiltration analgesia, 1 with only peri-articular injection, 2 with combined local infiltration analgesia and intra-articular injection, and 1 with combined peri-articular injection and intra-articular injection. Local anesthetic injection,intra-articular injection and peri-articular injection provided equivalent analgesia to regional nerve blocks. Intra-articular injection could obtain the same effect as a single femoral nerve block at postoperative pain management after anterior cruciate ligament surgery. Continuous-infusion catheters of a local anesthetic provided adequate pain relief but have been shown to cause chondrolysis. An increase in acute postoperative pain was found with local liposomal bupivacaine compared with femoral nerve block in postoperative pain management. But after the acute postoperative period, there were no significant differences.
However, the occurrence of nerve irritation postoperatively was found to be higher in the femoral nerve block.
Conclusion
Injection of local anesthetic is an effective form of analgesia. Local anesthetic injection would provide equivalent analgesia to single-never block. Despite the vast amount of evidence on this topic, further research is needed to improve the effectiveness of postoperative pain management and minimize pain and opioid consumption.
Clinical Relevance
These results provide the effective available evidence from RCTs on injection of local anesthetic for post-operative pain management after anterior cruciate ligament surgery.
As development and popularization of day surgery, anterior cruciate ligament reconstruction(ACLR)has been treated as day surgery in many countries. Therefore, as confirmed by previous studies, patients after ACLR suffered horribly postoperative pain, which prevents ACLR from becoming the day surgery. In arthroscopic ACLR postoperative pain management,the main sources of local anesthesia administration as follows: femoral nerve block, adductor canal block (ACB), or peri-articular infiltration of the knee joint. These analgesic methods were generally termed local infiltration analgesia (LIA) [4]. Nerve block is a effective method of pain management, but it not suit for day surgery. Femoral nerve block has been incriminated in cases of impaired postoperative mobility and falls. Meanwhile,the occurrence of nerve irritation postoperatively was found to be higher in the femoral nerve block. Continuous-infusion catheters of a local anesthetic provided adequate pain relief but has been shown to cause chondrolysis.
In fact,many of postoperative pain management options, the optimal approach is actually unknown.
To evaluate the analgesic availability of each postoperative pain management approach, we retrieved randomized controlled trials (RCT) of local injection for analgesia after arthroscopic ACL surgery and conducted a systematic review. We aimed to clarify the postoperative analgesic efficacy of various local injection approaches of narcotic analgesia and even to find an optimal postoperative analgesic regimen for this procedure.
We registered the system reviewer in https://www.crd.york.ac.uk. ID:CRD42021244080
Materials and Methods
Literature inclusion criteria
(1) object of study; Primary ACL reconstruction, performed in adult patients, ASA class
Ⅰ~III(include III), undergoing primary arthroscopic ACL reconstruction.
(2) study type:available published,randomized controlled trials (RCTs), defined in English.
(3) study subjects: in the experimental group or control group were treated with at least one of the previously described postoperative analgesic modalities (intra-articular injection, peri-articular injection, femoral nerve block, adductor canal block),
(4) described at least one of the primary or secondary outcome measures set by this
Systematic Review.
Literature exclusion criteria
(1) Duplicate published literature
(2) ASA class greater than III
(3) age less than or equal to 12 years
(3) non-primary surgery
(4) non-elective surgery
(5) systematic review and meta-analysis
(6) non-English literature
(7) non-human trials or animal experiments
(8) literature with unclear data description, incorrect statistical methods, or data presented that cannot carry on systematic review.
Outcome Measures
(1) Main outcome measures: postoperative VAS or NRS scores at any time point postoperatively.
(2) Secondary outcome measures:
1) the consumption and frequency of rescue analgesics /Supplementary analgesics during the postoperative period, the total consumption of postoperative opioid analgesics (eg. Tablet morphine, fentanyl, oxycodone hydrochloride, morphine, etc.) or nonsteroidal analgesics(ketorolac, tablet acetaminophen, etc.)
2) the postoperative knee movement (the measure was a range of motion at the physiotherapy control)
3) postoperative local and systemic adverse effects
4) Patients’pain management satisfaction or patients’ satisfaction.
literature search
We searched the Cochrane Library, PubMed, Web of Science, and EMBASE databases by computer. The retrieval time is limited to 2021. The keywords were “anterior cruciate ligament”, “postoperative pain management”, “injection of local anesthetic”, “intra-articular injection ” and “local infiltration analgesia ”. Study type was limited to a randomized controlled trials. Two researchers independently screened the literature and extracted the data. In case of disagreement, a third person would discuss and solve it.
Literature quality evaluation
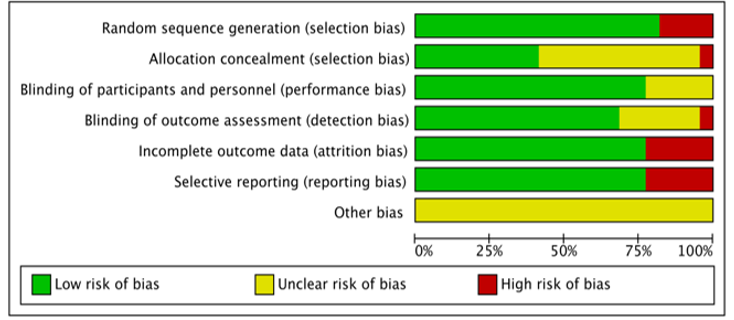
The risk of literature bias was assessed by two researchers using the criteria provided by Cochrane Handbook of systematic review (version 5.1.0) (included in Review Manager 5.4), including random allocation method, allocation concealment, blind method, lost follow-up report, and other biases. When the two researchers had different opinions, the third person participated in the discussion and made a decision together. If all the criteria are low risk, it is a low risk of bias. Which has the highest quality; If one or more types of risk are unknown, it is an unknown risk of bias. Which has a medium quality; If one or more types of high risk, it is a high risk of bias. Which has the lower quality. At the same time, the Jadad scoring method was used to evaluate the quality of the included literature.
Result
Search Results
A total of 685 literatures were obtained from the initial screening, and 446 literatures remained after the removal of duplicates according to the inclusion and exclusion criterias. Whereafter,396 literatures were removed because of irrelevant to the cases. There were 50 literatures were available for full text. In these 50 literatures, 4 meta-analyses and systematic review, 9 non-human experiments, 9 nerve blocks alone, 2 infant, and 4 academic artifacts literatures were eliminated. Finally, total of 22 RCTs met inclusion criteria: 15 with only intra-articular injections, 3 with only local infiltration analgesia , 1 with only periarticular injection , 2 with combined local infiltration analgesia and intra-articular injections and 1 with combined periarticular injection andintra-articular injections.A PRIMSA flow diagram is presented in Figure 1

Basic information of included literature
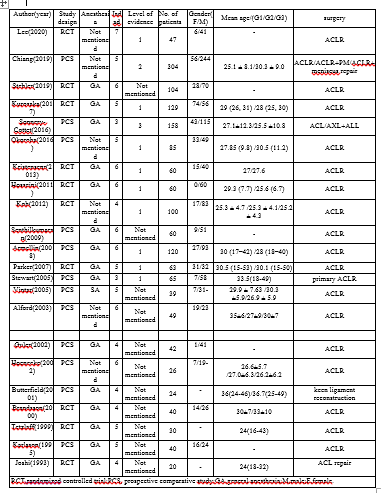
Basic information regarding patient demographics and characteristics of the included studies is presented in Table 1. A total of 1757 patients were included in this systematic review and there was a predominance of male patients in all studies. The mean age of patients ranged from 24 years to 36.7 years. And details of the intervention and outcomes of the included studies are presented in Table 2.
A, The patient's VAS or NRS score at any time point postoperatively;

or non-steroidal analgesics(including ketorolac、tablet acetaminophen);
C,Mobility of the knee joint after surgery(measure was range of motion at the physiotherapy control);
D,Post-operative local and systemic adverse effects(including vertigo, nausea, vomiting)
E,Other post-operative complications;
Literature bias evaluation
In this paper, the Cochrane Collaboration Network risk bias assessment

Nerve block
As a common postoperative analgesic modality, the nerve block is widely used after various types of surgery. The most commonly used nerve block way after arthroscopic anterior cruciate ligament surgeries are femoral nerve block (FNB) and adductor canal block(ACB).
Pia Kjaer Kristensen et al think that after anterior cruciate ligament reconstruction with
hamstring tendon graft,there was no significant difference in postoperative NRS pain scores between intra-articular local injection of anesthetics and femoral nerve block alone. There was also no significant difference in analgesic consumption during the 48 hours postoperatively.
Although there was a trend to decrease opioid consumption in the femoral block group during the first 3 postoperative hours, the trend was not significant[1].
Kelechi R. okoroha et al. refined groups of different graft sites in a trial when injecting local anesthetics. And they chose different injection sites depending on the site of graft taken. It was found that patients in the local infection anesthesia (LIA) group had significantly higher acute pain at 5-8 hours postoperatively than those in the FNB group. However, when statistical analysis was performed, it was found that the mean postoperative pain level and the postoperative morphine consumption equivalents in both groups did not differ significantly[2].
Kenji Kurosaka et al. found that patients who received a peri-articular injection of local anesthetics have lower pain scores at rest in the first 24 hours, 4 hours, 8 hours, and 2 days after surgery. In addition, patients consumed fewer opioids in the first 24 hours postoperatively at the latest. Nevertheless, Opioids related complications did not differ significantly between patients assigned to the two modes of analgesia[3].
Although the postoperative analgesic efficacy of FNB is precise. And it can provide comparable analgesic effect to intra-articularly injection of local anesthetic drugs into and local infiltration anesthesia at the graft site. But there is the non-negligible side effects of FNB, such as prolonged quadriceps inhibition,[2] prolonged sensory disruption in the anterior proximal high[2].
Although the postoperative analgesic efficacy of FNB is precise. And it can provide comparable analgesic effect to intra-articularly injection of local anesthetic drugs into and local infiltration anesthesia at the graft site. But there is the non-negligible side effects of FNB, such as prolonged quadriceps inhibition,[2] prolonged sensory disruption in the anterior proximal high[2].
So, it is of particular importance to select a postoperative analgesic modality that can both provide equivalent postoperative analgesia and circumvent the various side effects associated with FNB.
After researching, Kevin stebler et al. indicated that ultrasound-guided adductor canal block (ACB) and local infiltration analgesia did provide equivalent analgesic effect after ACLR surgery. Meanwhile, they found that the consumption of intravenous morphine analgesics within 24 hours after the operation is similar. And there is no significant difference in both secondary pain and functional related results. Although the resting pain score in 48 hours after surgery is lower in the ACB group, the authors believe that it is likely to be related to one type of statistical errors.[4]
That is to say, the difference in resting pain scores found in this study, which credibility is needed to be weighed.
In other words, ACB can provide the same postoperative analgesic effect as FNB and make up for the defect of femoral nerve block caused by FNB, which makes ACB a better choice than FNB, especially after arthroscopic anterior cruciate ligament reconstruction surgery.
Although nerve block is widely used in clinic, through our systematic review of a large number of literatures, local infiltration anesthesia can provide equivalent postoperative analgesia and avoid the side effects related to nerve block. This may suggest that local anesthesia is a better choice in the future clinical practice.
The donor site injection
As we all know, there are differences in the details of the arthroscopic anterior cruciate ligament reconthe tendon donor site. So, is local anesthetic injection at the corresponding tendon donor site a possible choice for postoperative analgesia?
According to the study of Heinz R. hoenecke et al., continuous injection of local anesthetic (0.25% bupivacaine) at the donor site can significantly reduce
within 48 hours after the operation. And it can also reduce the dosage of opioid analgesics postoperatively.[5]
Pia kjaer Kristensen et al. found that the donor site postoperative analgesia effect with FNB. In their study, within 48 hours after the operation, the donor site injection group was superior to the FNB group in both postoperative pain score and postoperative pain relief. At the same time, the local anesthesia of the donor site injection can good to avoid the side effects of femoral nerve block.[1] Furthermore, the author even confirmed that local injection of local anesthetics at the graft site can achieve comparable postoperative analgesic effect with a femoral nerve block, which may reflect that the main source of pain after arthroscopic ACL surgery is the pain derived from the donor site. It may also lead us to think in another aspect that whether FNB can block the pain from the donor site or not.
Bertrand sonnery-cott et al. also found that the hamstring donor site injection and intra-articular local injection of narcotic drugs can provide similar postoperative analgesic effect. At the same time, there was no significant difference both in consumptions of opioid analgesics and in anesthesia related side effects.[6]
Kelechi R. okoroha et al. also used the local infiltration anesthesia of the donor site injection in their trial. But they came to the opposite conclusion.They found that the acute pain score of the donor site injection group was significantly higher than that of the FNB group in 5-8 hours after operation. However, this difference only exists in the postoperative acute pain period. After the acute pain period, the donor site injection can provide the comparative analgesic effect as FNB but avoiding the inherent risk of femoral nerve block. This may be related to the type of local anesthetic they choosed. Among the many local anesthetics, they chose liposomal bupivacaine as their local infiltration anesthetics. The author specifically points out in the article that they choose liposomal bupivacaine because of the delayed release from lipid storage delivery. Studies have shown that there is 10 hours lag time before optimal local concentration of liposomal bupivacaine.[2]
Kevin stebler et al. mainly compared postoperative morphine consumption. Morphine consumptions, resting and dynamic pain scores and postoperative nausea and vomiting at 2 hours and 24 hours postoperatively were comparable between experimental group and control group in their study. And there was no analgesic technique impacted either early or late functional outcomes.[4]
Intra-articular injection
Through our systematic search of literatures, we found that intra-articular injection of drugs for pain management after arthroscopic ACLR surgery was mentioned in the literature as early as 1993[7]. From 1993 to 2020, scholars from different countries and regions continued to explore the postoperative analgesia of intra-articular injection.
The injected drugs are different, including morphine alone, local anesthetics alone ( bupivacaine, ropivacaine), combined local anesthetics with morphine or other opioid analgesics, combined local anesthetics with non-steroidal analgesics, and a new drug combination method,multimodal drug cocktail (MDC), etc. In addition, some recent studies have explored the postoperative analgesic effect of intra-articular injection of tranexamic acid.
At the same time, the way of injection is not same. Such as indwelling catheter for continuous infusion of drugs, single injection of drugs and so on.
After systematic analysis of literatures, we found that intra-articular injection of morphine can produce exact postoperative analgesic effect, which was confirmed by GP Joshi et al. In 1993. They found that patients in the intra-articular morphine group had lower postoperative VAS pain scores than those in the intra-articular saline group[7]. Later, in the study of s brandsson et al., the optimal dose of intra-articular injection of morphine was explored in more details. They found that the postoperative VAS pain scores was significantly lower in patients with intra-articular injection of 5 mg morphine than in patients with intra-articular injection of 1 mg morphine. What's more, they found that the postoperative pain scores of patients who received intra-articular injection of 5 mg morphine from 24 hours to 1 week after operation was continuously lower than that of patients who received intravenous injection of 5 mg morphine.[8] It seems to suggest that the analgesic effect of applicating morphine locally is better than applicating morphine systemically . It does support the view that the analgesic effect caused by intra-articular morphine is a local effect in the peripheral tissue in the site of injection.[8]
In comparison with non-steroidal analgesics , tenoxicam, Guler g et al. found that intra-articular injection of tenoxicam and intra-articular injection of morphine can also significantly reduce the postoperative VAS scores[9]. Although the VAS scores of patients in the tenoxicam group was continuously lower than that in the morphine group within 48 hours after operation, the difference has statistical difference only within 30 minutes after surgery. However, based on the fact that the patients in the tenoxicam group require less supplementary analgesic drugs in and 6 hours after operation than who in the morphine group, the article finally points out that tenoxicam can provide better analgesic effect than morphine.[9] This also leads to our thinking that non-steroidal analgesics may be a more selective option for morphine in postoperative pain management after arthroscopic ACLR surgery.
Since the advent of morphine, medical workers have been enthusiastic about its research. While intra-articular injection of morphine alone has been widely studied, the injection of morphine combined with local anesthetics is also the focus of medical workers. In the literatures we included, researchers chose bupivacaine with morphine, ropivacaine with morphine, added a non-steroidal analgesics or even an antibiotic. For the arrangement and combination of different drugs, of course , people's starting point is to integrate the advantages of various drugs and minimize their respective side effects. Previous studies have shown that the onset time of morphine is generally 3-6 hours after surgery[9]. So, if morphine can be combined with fast acting drugs, it can theoretically reduce the pain of patients 3-6 hours after surgery. After a systematic review of the literatures, we found that bupivacaine with morphine, tramadol hydrochloride, methadone and ropivacaine with morphine, ketorolac, clonidine, sufentanil, and even KOH's multimodal drug injection can significantly reduce the postoperative VAS scores. First of all, the combination of local anesthetics and morphine dose improve the pain scores in the early postoperative period, but there was no significantly difference in VAS or NRS scores between local anesthetics combined with various drugs. In addition, the increase in the variety of mixed drugs did not increase the analgesic effect of postoperative analgesia. And it also did not increase the incidence of postoperative adverse reactions. This may suggest that the combination of rapid onset local anesthetics with slow onset opioid analgesics or non-steroidal analgesics can achieve satisfactory analgesic effect.
However, in the study of the mixture of local anesthetics and morphine, the conclusion in a literature seems to be in contradiction with the conclusion of Brandssons[8] .Brandssons found that the VAS pain scores of patients with intra-articular injection of 5 mg morphine was significantly lower than that of patients with intra-articular injection of 1 mg morphine[8]. It seems that with the increase of morphine dosage, the postoperative analgesic effect will be enhanced. However, the study of Tetzlaff, J. E. found that patients given 3 mg morphine had higher pain scores at 0 minutes and 30 minutes after operation than those given 1 mg morphine.[11]They combined bupivacaine with morphine, and they finally found that bupivacaine with 3mg morphine group had higher pain scores than bupivacaine with 1mg morphine group at 0 minutes and at 30 minutes postoperatively[11].
However, the specific reasons for this result have not been clarified, which provides a new idea for our future research work. Perhaps we can explore the optimal intra-articular dose of morphine from the perspective of the hypothesis of peripheral opioid activation.
The specific analgesic mechanism of intra-articular local injection of morphine has not been clarified yet. The exact mechanism by which local opioids reduce pain after peripheral administration is not yet fully known . It is an urgent problem to be solved in our future research.
In addition to studies on the postoperative analgesic effects of intra-articular injection of analgesic drugs, there are also studies on the postoperative analgesic effects of intra-articular injection of local anesthetic drugs alone. Intra-articular injection of local anesthesia has focused on bupivacaine and ropivacaine.
According to the research of Alford, J. W.et al[12],the bupivacaine infusion catheter group has lower maximum pain than other groups. But it has higher maximum pain after removal catheter than other groups. The bupivacaine infusion catheter patients had lower maximum pain than the placebo or control groups while the catheters are still in place. But it is unexpected that this positive analgesic effect was reversed after the catheter was removed. After the catheter was removed, patients in the bupivacaine group had higher maximum pain than other two groups.[12]
On the contrary, Parker, R. D. et al .[13] and Vintar, N. et al. [16] found that there was no significant difference in postoperative pain scores between patients with intra-articular bupivacaine group and control group.
In the study of Chiang, E. R. etal [14] and Lee, J. W. etal [15], they selected intra-articular injection of Tranexamic acid (TXA) to test whether it could relieve postoperative pain in patients undergoing arthroscopic ACLR surgery.
In the literatures we included, only two literatures mentioned the method of intra-articular injection of Tranexamic acid (TXA), but their conclusions were exactly the opposite. Chiang, E. R. et al,. found that intra-articular injection of TXA group had significantly lower VAS pain scores on postoperative day 3, and no difference on week 4[14]. However, Lee, J. W. et al. found that intra-articular injection of TXA had no effect in reducing VAS pain scores after ACLR surgery [15] . But, a consistent conclusion was reached in these two studies that intra-articular local TXA injection did reduce bleeding in patients undergoing arthroscopic ACLR surgery.(Table2)
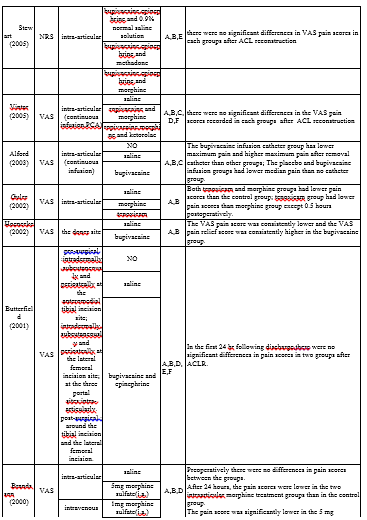
Table 2. Summary of interventions and outcomes of the included studies
Among the included literatures, 3 were provided for continuous analgesia [12] [13] [16]. In their study of continuous postoperative analgesia, they found that the psychological effects of patients also play a significant role in the experience of postoperative pain. This can be reflected in the changes in the pain experience of patients before and after remove the catheter. It suggests that the psychological comfort of patients is also very important. At the same time, bad psychological hints should not be given to patients not only before but also after surgery.
Alford, J. W. etal. especially pointed out in the end of their article that the data for median pain ratings suggest some element of placebo benefit of postoperative catheter placement in the joint . In other words, patients believed in the benefit of the catheter itself, rather than its contents. It may promote low narcotic consumption and high motivation to perform therapy tasks[12].
Meanwhile,It should also be noted that continuous infusion of anesthetic drugs with joint catheters, while providing adequate pain relief, has been shown to cause chondrolysis.
In the literature we included, all patients were given supplementary analgesics after surgery as needed (when the VAS pain scores was greater than or equal to 5 ) , in accordance with the requirements of medical ethics. Although the total dose of analgesic supplementation has been evaluated in the literature, whether the VAS pain scores or NRS pain scores measured at the later stage of analgesic supplementation can reflect the true analgesic effect of various postoperative analgesic methods remains to be discussed. The VAS or NRS pain scores obtained for all trials were based on a dose of supplemental analgesics. Although the consumption of supplementary analgesics was systematically evaluated in almost all experiments, the assessment methods of the consumption of supplementary analgesics were not identical in all the included literatures, so we could not draw a conclusion on the consumption of supplementary analgesics for reference.
Vintar, N. et al.pointed out that regarding of postoperative pain, their study was designed to be as comfortable for patients as possible. They emphasized this point at the end of their article. They think all patients accessed to morphine PCIA did provide satisfactory analgesia in the placebo group at rest and during physical rehabilitation. But this maybe explain why there are no statistically significant differences in pain scores among groups[16].
This is a general deficiency in these experiments, which is also a problem we need to solve in the future research work. But due to ethical considerations and patient-centered principles, it seems that we cannot simply for scientific purposes not give any additional analgesics when patients are suffering from severe postoperative pain. As we can imagine, this is a very bad medical experience for patients. This is the paradox of all clinical research.
What is clear, however, is that the consumption of opioid analgesics after intra-articular morphine injection is significantly reduced. However, the mechanism of the analgesic effect induced by the peripheral application of morphine is still not clear. Although some scholars have proposed the hypothesis of peripheral opioid receptors, the specific mechanism of the analgesic effect induced by the peripheral opioid receptors is still unclear. There have been studies to evaluate the analgesic effect of morphine with the active metabolite M6G in plasma.[8] After S Brandsson applied 5mg morphine in the articular space, the concentration of metabolite M6G in plasma was much lower than that of M6G after the same dose of morphine intravenous infusion. And it's nowhere near the level that would produce a systemic analgesic effect. This is not a good explanation for why the same dose of morphine injected into the joint cavity is so much more effective than intravenous injection of morphine. But one aspect of this is that the analgesic effect of the topical application of morphine to the peripheral tissues is not through systemic action but through the action of the peripheral opioid receptors. But that still doesn't shed light on the mechanism. This is a very good inspiration for our future research work, we can carry out more in depth research in this aspect, and to explore the mechanism of peripheral opioid receptors activation.
It is still the aspect of intra-articular injection of morphine. All articles using intra-articular injection of morphine or opioids have come to the conclusion that intra-articular injection of morphine can not only reduce the consumption of postoperative morphine or opioids, but also reduce the systemic adverse reactions related to morphine or opioids, such as nausea, vomiting, dizziness, etc. This undoubtedly tells us that intra-articular local opioid analgesics is a better choice than systemic use of morphine after arthroscopic ACLR surgery. So, whether this way of administration can be extended to other knee joints operations or other joint operations, and whether the advantages of this way of administration still exist when applied to other situations, these are the problems that we need to solve in the future research work.
In addition, only non-English literatures were excluded in the literature screening process. In the included literature, none of the experiments made detailed classification and comparison on demographic characteristics such as gender, age, race and ethnicity. There was no significant difference in these demographic characteristics between all of the experimental group and the control group. But ,pain tolerance is known to vary across genders, ages, and ethnicities. Patients undergoing ACLR surgery are relatively young. This provides a clear research idea for our future research work. We can carry out more detailed grouping and research on the above factors, aiming to find individualized postoperative analgesia programs for different groups of people, so as to minimize the pain suffered by patients after surgery.
Injection of local anesthetic is an effective form of analgesia. Local anesthetic injections would provide equivalent analgesia to single-never block. Despite the vast amount of evidence on this topic, further research is needed to improve the effective of postoperative pain management and minimize pain and opioid consumption.
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Availability of data and materials
Not applicable
Competing interests
Not applicable
Funding
Not applicable
Authors' contributions
Acknowledgements
Not applicable
Authors' information (optional)
Not applicable
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
