AUCTORES
Globalize your Research

Review
*Corresponding Author: Anthony Kodzo-Grey Venyo. North Manchester General Hospital, Department of Urology, Delaunays Road, Crumpsall, Manchester, United Kingdom.
Citation: Anthony K-G Venyo. (2022). Inclusion of Immunotherapy in the Management of Primary and Metastatic Malignant Tumours of the Kidney Including Adult Renal Cell Carcinoma: A Review and Update. Clinical Research and Clinical Trials. 5(3); DOI:10.31579/2693-4779/071
Copyright: © 2022 Anthony Kodzo-Grey Venyo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 November 2021 | Accepted: 05 January 2022 | Published: 17 February 2022
Keywords: kidney tumours; carcinoma of kidney; renal cell carcinoma; clear cell carcinoma of kidney; active surveillance; partial nephrectomy; radical nephrectomy; targeted therapy; radiotherapy; chemotherapy, immunotherapy; cryotherapy, radiofrequency
Various tumours of primary malignant tumours of the kidney exist bot the most common type of primary malignant tumour of the kidney is renal cell carcinoma (clear cell carcinoma of the kidney tend to be encountered most often globally. The biological behaviour of a kidney tumour tends to depend upon the size of the tumour, the histological grade and stage of the tumour. Most kidney tumours that are very small (less than 7 cm) and localized to the kidney of low-grade histopathology pattern tend not to be aggressive or develop further so these days a number of patients who have small low-grade / low stage renal tumours tend to be offered expectant management of regular periodical radiology imaging and if there is any subsequent evidence of increase in the size of small localized kidney tumours, then patients who have these tumours tend to be offered treatment of curative intent. Larger localised kidney tumours that are clear cell / renal cell carcinoma tend to be treated by surgical complete excision of the tumour with the undertaking of partial nephrectomy or radical complete nephrectomy, Individuals who have locally advanced tumours tend to be treated by means of radical nephrectomy plus excision of the lymph nodes within the para-renal and para-aortic region plus adjuvant radiotherapy plus / chemotherapy. Some of the treatment options that have been used form the management of metastatic renal cell carcinoma do include surgery, immunotherapy, targeted treatment, radiotherapy, and chemotherapy. Some of the systemic font-line treatment options which are available include: immune check point inhibitor based combination (IBC) treatment with the inclusion of pembrozulimab / axitinib, nivolumab / pilimumab, as well as avelimab / axitinib. It has been iterated that with unusual exceptions, the utilization of monotherapy with vascular growth factor tyrosine kinase inhibitors or mTOR inhibitors have been considered not to be appropriate options of treatment with regard to the front-line setting. Some of the immunotherapy strategies that are utilized do include: cancer vaccines, oncolytic viruses, adoptive transfer of ex vivo activated T as well as natural killer cells and administration of antibodies or recombinant proteins which either co-stimulate cells or bloc the so-called immune checkpoint pathways. The success of many immunotherapy treatment options recently, including monoclonal antibody blocking of cytotoxic T lymphocyte-associated protein 4 (CTLA-4) as well as programmed cell death protein 1 (PD1), had boosted the development of immunotherapy and this has been ensued by description of new therapeutic targets and schemes that combine various immunology agents at a fast pace. Despite the confirmed efficacy of frontline IBC in the treatment of renal cell carcinomas, majority of the patients would eventually require the need to undergo additional options of treatment and based upon this oncologists have been advised to take into consideration this knowledge carefully when they are switching to other forms of treatment, especially with regard to situations of intolerable drugs or apparent progression of disease. Considering that the biological behaviour of kidney malignant tumours depend upon the size, the histological cell type, the histological grade and stage of tumour, oncologists and urologists have tended to use different treatment options in the management of advanced / metastatic kidney tumours. There are many common side effects of the various immunotherapy treatment options that are common and there are also rare and serious side effects and complications associated with immunotherapy which clinicians and patients need to know about. Various immunotherapy options have been used over recent years in the management of various malignant kidney tumours but it does appear that immunotherapy tends to be beneficial to the management of high risk kidney tumour groups when as well as in the setting of advanced / metastatic kidney tumours.Nevertheless, Immunotherapy does tend to be associated with a number of side effects including nephropathy and it is important for clinicians to be aware of all the complications and complications associated immunotherapy of advanced / metastatic tumours of the kidney. Considering that radical surgical excision of localised tumours tends to be very effective and associated with good long-term prognosis, it would not be very necessary under most circumstances in utilizing immunotherapy to treat such cases. However, immunotherapy has been demonstrated to be associated with improved prognosis when compared with treatment of advanced / metastatic kidney tumours that had been undertaken earlier when immunotherapy was not available.
Even though there is evidence to suggest the usefulness of immunotherapy in the treatment of cancers side effects and common as well as rare complications do occur and because these complications and side effects tend to be non-specific, a high index of suspicion would be required to quickly establish the diagnosis. Side effects of PD-1 inhibitors could include fatigue, cough, nausea, itching, skin rash, loss of appetite, constipation, joint pain, high blood pressure abdominal pain and diarrhoea. More serious side effects occur less often, but are possible. These drugs work by removing the brakes on the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious problems in the lungs, intestines, liver, hormone-making glands (like the thyroid), kidneys, the nervous system or other organs. In some people these side effects can be life threatening. Other possible side effects include: flu-like symptoms (fever, chills, muscle aches), nausea, low blood pressure, fluid build-up within the lungs, breathing difficulties, kidney damage, heart attacks, intestinal bleeding, rapid heartbeat, mental changes, neurological side-effects within the central and peripheral nervous system. These side-effects tend not to be uncommon; nevertheless, they tend to be clinically relevant to the management of patients which clinicians need to be aware of. Some of the neurological side effects of immunotherapy that tend to be found do include:
multiple sclerosis-type syndromes, Guillain-Barré syndromes, neurasthenic syndromes, as well as various infections of the peripheral nervous system and muscular system, such as myopathies and necrotising myopathies. There is generally no clear cut prevention of complication and side effect strategy for immunotherapy, other than the better selection of patients for immunotherapy. Suppression of the immune system with utilization of immunosuppressive medicaments such as corticosteroids has tended to be the main therapeutic strategy for neurological side effects of immunotherapy. Nevertheless, there is the possibility that a patient’s cancer would progress while receiving immunosuppressants. Intravenous immunoglobulins or plasmapheresis could also be utilized; nevertheless, there has tended not to be clear recommendations or consensus opinion on treatment of these side effects. There is need for the undertaking of a global multi-centre studies to ascertain the effect of
immunotherapy in the management of the various types of kidney tumour to enable a consensus opinion to be established on the role of immunotherapy for the various types of kidney tumour and not only clear cell carcinoma of the kidney. The ensuing article on immunotherapy in malignant tumours of the kidney is divided into two parts: (A) Overview which has discussed miscellaneous aspects of kidney tumours and (B) Miscellaneous narrations and discussions related to case reports, case series, and studies related to immunotherapy of various kidney tumours.
Deleuze et al. [1] made the following summations related to immunotherapy in renal cell carcinoma:
Renal cell carcinoma is the third type of urological malignant tumour and has a poor prognosis with 30% of metastatic patients at diagnosis.
The antiangiogenics and targeted immunotherapies led to treatment remodelling emphasizing the role of the tumour microenvironment.
However, long-term responses are rare with a high rate of resistance.
New strategies are emerging to improve the efficacy and the emerging drugs are under evaluation in ongoing trials.
With the different treatment options, there is an urgent need to identify biomarkers in order to predict the efficacy of drugs and to better stratify patients.
Owing to the limitations of programmed death-ligand 1 (PD-L1), the most studied immunohistochemistry biomarkers, and of the tumour mutational burden, the identification of more reliable markers is an unmet need. New technologies could help in this purpose.
Renal cell carcinoma is the third urological cancer, representing 3% of all cancers in women and 5% in men with an incidence of around 400,000 cases worldwide [ 2]The prognosis is poor: 30% of patients are metastatic at diagnosis and almost 30% of the remaining patients will develop metastases detected during the follow-up [3].
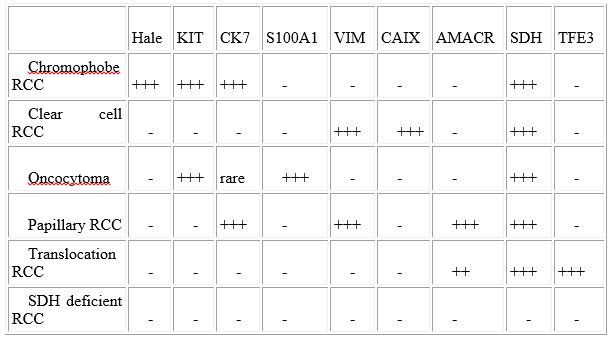
Clear cell renal cell carcinomas (ccRCC) represent the vast majority of RCC (around 75%). The other histology subtypes mainly include papillary (20%) and chromophobe RCC (5%). The other entities are very rare including translocation-associated RCC, medullar RCC and collecting duct carcinoma. The histological entities based upon distinct pathological features present different molecular alterations. Indeed, ccRCC are hallmarked by a frequent alteration of the VHL gene, a tumour suppressor gene, leading to angiogenesis through the transcription of genes regulated by HIF such as VEGF [4-8].
Non ccRCC (nccRCC) represent a heterogeneous group with papillary, chromophobe RCC and translocation RCC, the most frequent entities. Papillary RCC (pRCC) include tumours with indolent outcome (type 1) and more aggressive tumours (type 2) [9] Type 1 and type 2 pRCC commonly harbour frequent MET alterations. However, alterations of SETD2, CDKN2A, EGFR, NF2 and TERT have been described in type 2 and suggest the activation of MAP kinases pathway, cell cycle and deregulation of chromatin remodelling [10]. Chromophobe RCC (cRCC) are rarely metastatic and characterize mitochondrial alterations, frequently mutated p53 and activation of mTOR pathway [10]. Translocation RCC (tRCC) harbour gene fusions involve TFE3 and TFEB, members of the MiTF family [11]. These transcription factors have multiple partners, mainly involving messenger RNA splicing [12].
The other entities do constitute less than 2% of renal tumours. The collecting duct carcinoma have been described as immunogenic tumours with high lymphocyte infiltration resulting from the upregulation of genes involved in T-cell activation and proliferation [13] Renal medullary carcinoma present a frequent loss INI1 (SMARCB1) implicated in the chromatin remodelling complex [14]. Among familial RCC syndromes, patients with hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome harbour Fumarate Hydratase (FH) germline mutation and develop clinical aggressive tumours [15]. The FH mutation by inactivating the enzyme alters the function of the Krebs cycle.
The sarcomatoid component could be found within all the histological subtypes and demonstrates an increased tumour mutation burden (TMB) with high frequency of p53, CDKN2A and NF2 mutations and also genes involved the chromatin remodelling such as ARID1A and BAP1 [16].
The treatment and management of metastatic renal cell carcinoma (mRCC) had radically changed over the preceding 20 years [17]. Initially, first-generation immunotherapy with cytokines: interleukins or interferon represented standard approaches but with poor results [19]
The development of tyrosine kinase inhibitors, mainly vascular endothelial growth factor (VEGF) receptor inhibitors, largely improved the prognosis of both progression free survival (PFS) and overall survival (OS) [20].
The emergence of immune checkpoint inhibitors (ICI) alone or in combination (anti-cytotoxic T-lymphocyte antigen-4 (CTLA4) and anti-programmed death 1 (PD-1)) had shown interesting results [21] [22]. Targeted immunotherapy does represent an alternative to antiangiogenics because ccRCC is also considered an immunogenic tumour with high numbers of immune cells such as tumour-infiltrating lymphocytes (TIL) [23-25] Recent trials proposed antiangiogenics in association with targeted immunotherapy to overcome resistance emphasizing the role of the tumour microenvironment (TME) and this strategy is currently an option in first line treatment. [26, 27].
Mechanisms of resistance with ICI can be primary or innate and secondary or acquired [28]. They encompass neo-antigen loss, defect of antigen presentation, alternative immune checkpoints and defective interferon signalling. Interferon-γ is a major mechanism of resistance by enhancing programmed death-ligand 1 PD-L1 expression and inducing the expression of immune inhibitory molecules [29]. Other immune checkpoints such as TIM-3, LAG-3 and TIGIT play a role in the resistance by inhibiting antitumour immune response [30]. Novel /new therapeutic approaches are trying to overcome these mechanisms of resistance and are under evaluation in ongoing trials.
Identifying biomarkers is the key to better select treatments, reduce costs and improve survival in patients with metastatic kidney cancer. However, the limitations of the most studied biomarkers: PD-L1 immunohistochemistry and TMB make necessary the identification of robust markers. New technologies could help in this purpose.
The ensuing article on Immunotherapy in the Management of Adult Renal Cell Carcinoma and other types of malignant tumours of the kidney is divided into two parts: (A) Overview of renal cell carcinoma and other types of malignant tumours of the kidney and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to renal cell carcinomas and other types of malignant tumours of the kidney.
To review and update the literature on immunotherapy in primary and metastatic malignant tumours of the kidney.
Internet data search bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Immunotherapy in Renal Cell Carcinoma; Immunotherapy in primary kidney tumour; Immunotherapy in metastatic kidney tumour. One hundred and six (106) references were identified which were used to write the article which has been divided into two parts: (A) Overview which has discussed miscellaneous aspects of immunology in general and related to malignancies of the kidney both primary and metastatic from or to the kidney and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to primary and metastatic tumours originating from the kidney as primary tumours and from elsewhere into the kidney.
Overview
Definition / general comments [31].
Adult renal cell carcinoma (RCC) or hypernephroma is a tumour that originates primarily from the kidney and does contain clear cells.
Apart from renal cell carcinomas of the kidney that originate primarily from the kidney or elsewhere with metastases developing in the kidney have been alluded to in the article.
Essential features
It has been iterated that adult renal cell carcinoma is the sixteenth most common cause of death from cancer worldwide; estimated 143,000 deaths from kidney cancer in 2012 [31-32].
Terminology [31].
Adult renal cell carcinoma has historic synonyms which include: nephrocellular carcinoma, Grawitz tumour, hypernephroma (due to perceived origin from adrenal gland)
Various types of kidney malignant tumours [31].
It has been iterated that renal cell carcinoma does account for 85% of kidney tumours and other authors have documented greater than 90% of kidney cancer [33] but subtypes of renal cell carcinoma include:
Clear cell carcinoma of kidney (in about 70% of RCCs).
Papillary cell carcinoma of kidney (in about 10% to 15% of RCCs).
Chromophobe carcinoma of kidney (in about 5% of RCCs).
Translocation renal cell carcinoma (in 3% to 4% of RCCs).
Unclassified renal cell carcinoma of kidney (in 3% to 4% of RCCs).
Renal medullary carcinoma (in younger adults).
Colleting duct carcinoma of kidney also called Bellini duct carcinoma (in less than 3% of RCCs).
Clear cell papillary Renal Cell Carcinoma (in less than 3% of RCCs) in less than 3% of RCCs).
Cystic Renal Cell Carcinoma (in 2.5% of cases).
Collecting duct carcinoma of kidney [34].
Medullary carcinoma of kidney associated with sickle cell trait
Mucinous tubular carcinoma of kidney
Spindle cell carcinoma of kidney
Tubulocystic carcinoma of kidney
Oncocytoid renal carcinoma in neuroblastoma survivors.
Renal carcinoma associated with end-stage renal disease.
Clear cell papillary carcinoma
Oncocytic papillary renal cell carcinoma
Follicular renal carcinoma
Leiomyomatous renal carcinoma
Other types of kidney tumours do include:
Lymphoepithelioma-like carcinoma of kidney [35].
Squamous cell carcinoma of the kidney.
Malignant schwannoma of kidney [36].
Fibrosarcoma of kidney [37].
Liposarcoma of kidney [38].
Primary Mesenchymal Chondrosarcoma of Kidney [39].
Primary osteosarcoma of the kidney [40].
Primary angiosarcoma of the kidney [41].
Neurilemoma of the Kidney [42].
Primary leiomyosarcoma of the kidney [43].
Primary rhabdomyosarcoma of the kidney [44].
Sarcomatoid carcinoma of kidney [45].
Carcinosarcoma of the kidney [46].
Other types of Sarcomas of the kidney.
Lymphomas of the kidney [47].
Transitional cell carcinoma of the kidney [48].
Wilms tumour of the kidney [49].
Primary malignant melanoma of the kidney [50-51].
Metastatic tumours within the kidney that have originated from primary malignant tumours from elsewhere I the body [52].
Hsieh et al. [33] made the ensuing summations related to renal cell carcinomas as follows:
Renal cell carcinoma (RCC) denotes cancer which does originate from the renal epithelium and does account for greater 90% of cancers in the kidney.
The disease does encompass more than 10 histological and molecular subtypes, of which clear cell RCC (ccRCC) is the commonest and does account for most cancer-related deaths.
Even though VHL mutations had been described for some time, more-recent cancer genomic studies have identified mutations within epigenetic regulatory genes and have demonstrated marked intra-tumour heterogeneity, which could be associated with prognostic, predictive and therapeutic relevance.
Localized RCC can be successfully managed by means of surgery, but metastatic RCC tends to be refractory to conventional chemotherapy.
Nevertheless; over the preceding decade, marked advances with regard to the treatment of metastatic RCC had been made, with targeted agents including sorafenib, sunitinib, bevacizumab, pazopanib and axitinib, which do inhibit vascular endothelial growth factor (VEGF) and its receptor (VEGFR), and everolimus and temsirolimus, which do inhibit mechanistic target of rapamycin complex 1 (mTORC1), being approved.
Since 2015, agents with additional targets aside from VEGFR have been approved, including cabozantinib and lenvatinib; immunotherapies, such as nivolumab, have also been added to the armamentarium for the treatment of metastatic RCC.
Epidemiology
Incidence: [31]
With regard to incidence it has been iterated that worldwide as of 2012, adult renal cell carcinoma of the kidney had represented the ninth most common cancer in men (214,000 cases) and fourteenth most common in women (124,000 cases) [31].
Male to female ratio (M:F) is approximately 2:1 [31].
Adult renal cell carcinoma is stated to be about 70% of new cases that occur in countries with high socioeconomic development [31].
The incidence of RCC is stated to vary widely from region to region with the highest rates in the Czech Republic and North America [31].
It has been stated that within the United States, there are nearly 64,000 new cases and almost 14,000 deaths from RCC each year [2, 31].
Sites of tumour
Primary renal cell carcinomas tend to be found within the kidney
Pathophysiology
It has been iterated that various molecular pathways do exist for kidney cancer [32].
Aetiology
Some of the aetiological factors associated with primary renal cell carcinoma have been summated as follows: [31]
Risk factors attributable to the development of kidney cancers do include: obesity, smoking, hypertension, acquired cystic kidney disease due to end stage renal disease, occupational exposure to trichloroethylene, treated neuroblastoma [31].
Genetic susceptibilities to renal cell carcinoma has been estimated to account for 2 - 4% [31, 32].
Usually renal cell carcinomas tend to affect individuals who are older than 50 years of age [31].
Hereditary renal cell tumours
Hereditary renal cell tumours have been summated to include or to be associated with: [31]
[1] Von Hippel-Lindau Syndrome.
Autosomal dominant, due to germline mutation of VHL gene at chromosome 3p25
Renal lesions: renal cysts and clear cell renal cell carcinoma.
It has been iterated that Von Hippel-Lindau Syndrome tend to be associated with bilateral or multiple renal cell carcinomas in 50% of cases [53].
Other organs as well as lesions that have been iterated to be involved in Von Hippel-Lindau Syndrome do include: hemangioblastomas of cerebellum and retina, cysts of pancreas, liver and kidney, clear cell tumours of other sites, papillary cystadenoma of epididymis, pheochromocytoma [2].
Hereditary papillary renal cell carcinoma.
It has been iterated that hereditary papillary renal cell carcinoma tends to be:
Due to activating mutation of MET oncogene at chromosome 7q31 [31].
Autosomal dominant, late-onset bilateral papillary renal cell tumours. [31].
[3] Hereditary leiomyomatosis and renal cell carcinoma.
It has been iterated that hereditary leiomyomatosis and renal cell carcinoma tend to be:
Autosomal dominant, familial [31].
Due to germline fumarate hydratase mutations [31].
Cutaneous or uterine leiomyomas [31].
Renal tumours are often papillary with characteristic large nucleus with a very prominent inclusion-like eosinophilic nucleolus (HLRC) [31].
[4] Familial papillary thyroid carcinoma. [31].
[5] Hyperparathyroidism-jaw tumour syndrome [31].
[6] Birt-Hogg-Dubé syndrome [31].
It has been iterated that Birt-Hogg-Dubé syndrome tends to be associated with: [31]
Autosomal dominant lesion with incomplete penetrance
Due to germline mutations in BHD gene at chromosome 17p112, which codes for folliculin. [31].
Skin lesions: fibrofolliculomas, trichodiscomas, acrochordons
Lung: cysts, spontaneous pneumothorax
Renal tumours that tend to be variable including: oncocytoma, as well as clear cell carcinoma and hybrid oncocytic / chromophobe tumour associated with areas of clear cells [54].
[7] Tuberous sclerosis [31]
It has been iterated that in tuberous sclerosis, there tends to be: [31]
Mutations in TSC1 and TSC2 genes via an alternate pathway not involving VHL mutations [31]. [55]
Multiple, bilateral angiomyolipomas or epithelioid angiomyolipoma [31].
[8] Constitutional chromosome 3 translocations [31].
Diagnosis [31].
It has been iterated that radiology image guided biopsy of solitary small renal masses could be used for planning of treatment, since pathology findings of the tumour / lesion cannot be predicted by clinical features [56, 57].
Radiology imaging description [31].
"Classic" clinical features of costovertebral pain, palpable mass and haematuria are now present in only 10%
Most tumours are detected incidentally due to increased use of imaging; historically were large (10 cm) at diagnosis
"Great mimic" due to associated paraneoplastic syndromes of Cushing syndrome, gynecomastia, hypercalcemia, hypertension, leukemoid reaction, polycythaemia, Stauffer syndrome (hepatomegaly with hepatic dysfunction), systemic amyloidosis, polyneuromyopathy
Prognostic factors [31].
It has been iterated that the prognosis of malignant tumours of the kidney / clear cell carcinoma of the kidney does tend to be associated with the following factors: [31]
The WHO / International Society of Urologic Pathology (ISUP) Grading for Clear Cell and Papillary RCC:
Grade 1: nucleoli inconspicuous or absent at 400x (objective magnification 40x)
Grade 2: nucleoli prominent at 400x
Grade 3: nucleoli prominent at 100x magnification
Grade 4: extreme nuclear pleomorphism, multinucleated giant cells, sarcomatoid or rhabdoid change
The stage of the tumour [31].
Histological subtype type of the tumour. [31]:
Treatment [31].
Resection (partial or radical nephrectomy)
Depends on subtype
Chemotherapy and radiation traditionally considered ineffective; however, increasing use of interferon, cytokine IL2,antiangiogenic agents and immunotherapy (sorafenib, sunitinib, temsirolimus, everolimus, bevacizumab, pazopanib, nivolumab)
5 year survival: 68% (all histologic types and stages), varies from 60% - 80% in stage I versus 5% in stage IV, lower for renal pelvis carcinoma (51%) compared with RCC (70%)
Other treatments options that have been used to treat some renal cell carcinomas depending upon the size and stage of the tumour to include.
Conservative / watch and wait expectant observation with regular periodic radiology imaging to ascertain if the lesion is growing bigger or not and treating tumours that show evidence of growing bigger.
Cryotherapy of the kidney tumour.
Radiofrequency ablation of the kidney tumour.
Irreversible electroporation of the kidney tumour.
Selective renal artery angiography and super-selective embolization of the arterial branch feeding the tumour.
Immunotherapy [31].
The ensuing summations have been made related to immunotherapy generally. [58] The immunotherapy of malignant tumours has made significant strides in the past few years in view of the improved understanding of the underlying principles of tumour biology and immunology.
These principles have been critical with regard to the development of immunotherapy in the laboratory and in the implementation of immunotherapy in the clinic.
The improved understanding of immunotherapy, which has been enhanced by increased insights into the mechanism of tumour immune response and its evasion by tumours, has currently enabled the manipulation of this interaction and has elucidated the therapeutic role of immunity with regard to cancer.
It is also relevant that, this improved understanding of immunotherapy and the mechanisms that underly immunity in cancer has fuelled an expanding array of new therapeutic agents for various types of cancers.
Pegylated interferon-α2b as an adjuvant treatment and ipilimumab as treatment for advanced disease, both of which were approved by the United States Food and Drug Administration for melanoma in March 2011, are 2 prime examples of how an increased understanding of the principles of tumour biology and immunology have been translated successfully from the laboratory to the clinical setting.
Principles which guide the development and application of immunotherapy do include antibodies, cytokines, vaccines, and cellular therapies.
The identification and further elucidation of the role of immunotherapy in different types of tumour, as well as the development of strategies for combining immunotherapy with cytotoxic and molecularly targeted agents for future multimodal therapy for cancer would enable even greater progress and eventually emanate in improved outcomes for patients that receive cancer immunotherapy.
Handling and staging guide [31].
The ensuing handling and staging guides for kidney tumours had been documented: [31]
Perinephric fat invasion: either the tumour touching the fat or extending as irregular tongues into the perinephric tissue, with or without desmoplasia
Renal sinus invasion: when the tumour is in direct contact with the sinus fat or the loose connective tissue of the sinus, clearly beyond the renal parenchyma or if it involves any endothelium lined spaces within the renal sinus If uncertain, at least 3 blocks of the tumour renal sinus interface should be submitted
Renal vein margin: margin is positive only when adherent tumour is visible microscopically at the actual margin If there is a submitted separately as “caval thrombus” take 2 or more sections to look for adherent caval wall tissue
Uninvolved renal parenchyma: should be sampled, distant from tumour, for underlying renal disease
Lymph nodes: should be sought but are found in less than 10% of radical nephrectomy specimens [59].
Macroscopic pathology description [31].
The gross pathology examination features of adult renal cell carcinoma have been summated as follows: [31]
The tumour tends to be well circumscribed, centred on cortex, and might bulge / distort the contour of the kidney.
The tumour often tends to extend into the renal vein or vena cava
Renal sinus invasion tends to be common in large tumours
The tumour could have satellite nodules, often haemorrhage, necrosis, calcification and cystic change
Cytology examination features [31].
The cytology examination features of adult renal cell carcinoma have been summated as follows: [31]
The tumour cells tend to have abundant cytoplasm which is vacuolated, fluffy or granular, usually with indistinct cell borders (chromophobe renal cell carcinoma has distinct borders)
The nuclei of the tumour tend to have variable atypia, irregular contours, haphazard orientation with abnormal chromatin, variably prominent nucleoli
The renal tubular cells tend to have well defined cell borders, homogenous cytoplasm, round, regular and orderly nuclei
It has been iterated that important features to differentiate the tumour from other neoplasms include heterogeneous cell population, small cytoplasmic vacuoles and hemosiderin deposits. [60]
It has been stated that a high false positive rate for FNAs was found in one study [31, 61].
Immunohistochemistry staining studies [31].
Positive immunohistochemistry staining [31].
It has been iterated that the tumour cells of primary renal cell carcinoma tend to exhibit positive immunohistochemistry staining for the following tumour markers:
PAX8 and PAX2 [31].
CAIX in which the positive staining tends to be: diffuse, membranous in 75 - 100% of clear cell renal cell carcinoma (RCC) [31].
Generally, CD10 (proximal tubular marker), RCC, vimentin and epithelial markers including AE1/AE3, CAM 5.2, EMA [31].
Negative immunohistochemistry staining [31].
It has been iterated that the tumour cells of primary renal cell carcinoma tend to exhibit negative immunohistochemistry staining for the following tumour markers:
Generally CK20, inhibin, [31] [62], Melan A/ MART1, calretinin, TTFI, and CEA. [31]
Obtained by [31] from References: [63-68]
Differential diagnosis [31].
Gross differential diagnosis
It has been iterated that up to 15% of renal epithelial neoplasms tend to be cystic upon radiographic and macroscopic examination and that selected differential diagnoses have been detailed out below [31, 69, 70].
[1] Multi-locular cystic renal neoplasm of low malignant potential [31].
It has been iterated that: [31]
Multi-locular cystic renal neoplasm of low malignant potential tends to be composed entirely of numerous cysts, the septa of which contain individual or groups of clear cells without expansile growth [32] and the clear cells tend to have low grade nuclei (ISUP 1 or 2) [31].
Multi-cystic with no expansile growth / solid nodules [31].
[2] Cystic clear cell papillary renal cell carcinoma [31].
It has been iterated that in cystic clear cell papillary renal cell carcinoma, there tends to be: [31]
Linear arrangement of nuclei away from basal membrane [31].
Co-expression of CK7 and CAIX with features of cup shaped positivity [31].
[3] Clear cell renal cell carcinoma with cystic degeneration [31].
It has been iterated that in clear cell renal cell carcinoma, the following would tend to be observed: [31]
An extensively cystic / necrotic tumour might still exhibit aggressive behaviour even if only rare identifiable tumour cells [31,71].
Haemorrhage, necrosis, thick irregular cyst wall, could be papillary / pseudopapillary, could have large areas of solid architecture or few residual tumour cells.
[4] Clear cell renal cell carcinoma originating in a benign cyst [31].
Controversial - It has been iterated that clear cell renal carcinoma originating in a benign cyst cases do include multilocular renal cysts with renal cell carcinoma [31,72,73].
[5] Acquired cystic disease associated renal cell carcinoma [31].
It has been iterated that acquired cystic disease associated with renal cell carcinoma tends to be: [31]
Most common kidney tumour in patients who have end stage renal disease and acquired cystic disease [31].
Characterized by abundant calcium oxalate crystals and variable morphology: papillary, solid, eosinophilic and clear cell-like areas [31].
[6] Tubulocystic renal cell carcinoma [31].
It has been stated that the diagnostic features of tubulocystic renal cell carcinoma do include the following: [31]
The tumour tends to be sponge-like, and composed of small to intermediate size cysts [31].
The tumour usually tends to contain enlarged nuclei and ISUP grade 3 nucleoli [31].
The tumour tends to shares cytogenetic abnormalities with papillary RCC (trisomy 7 / 17) [31].
[7] Cystic nephroma in adult [31].
It has been iterated that cystic nephroma in adult tends to: [31]
Be multiloculated benign tumour with cysts that are lined by flat to hobnailed epithelial cells which tend to be separated by fibrous septa containing pauci-cellular or ovarian-like stroma; no septal nodules of clear cells [31].
Be part of a spectrum of renal epithelial and stromal tumours which includes mixed epithelial and stromal tumour [31, 74, 75].
Raman et al. [76] stated that localized renal cell carcinoma (RCC) is often curable by surgery alone. However, metastatic RCC is generally incurable. In the 1990s, immunotherapy in the form of cytokines was the mainstay of treatment for metastatic RCC. However, responses were seen in only a minority of highly selected patients with substantial treatment-related toxicities. The advent of targeted agents such as vascular endothelial growth factor tyrosine kinase inhibitors VEGF-TKIs and mammalian target of rapamycin (mTOR) inhibitors led to a change in this paradigm due to improved response rates and progression-free survival, a better safety profile, and the convenience of oral administration. However, most patients ultimately progress with about 12 being alive at 5 years. In contrast, durable responses lasting 10 years or more are noted in a minority of those treated with cytokines. More recently, an improved overall survival with newer forms of immunotherapy in other malignancies (such as melanoma and prostate cancer) has led to a resurgence of interest in immune therapies in metastatic RCC. In this review we discuss the rationale for immunotherapy and recent developments in immunotherapeutic strategies for treating metastatic RCC.
Bedke et al. [77] stated that they had reviewed The treatment landscape in advanced and metastatic renal cell carcinoma (RCC) is moving from the inhibition of tyrosine kinases (TKI) and the mammalian target of rapamycin (mTOR) inhibitors to specific immunooncology agents like immune checkpoint inhibitors (ICI). The review focussed on the recent immunooncology developments and available trial results within the last 12 months. Bedke et al. [77] stated that recent findings had been made which had shown that ICI as monotherapy (nivolumab) or immunooncology and immunooncology combinations (nivolumab and ipilimumab) demonstrated positive results on prolonged overall survival in phase III trials. The combination of ICI (atezolizumab) and bevacizumab provided positive signals in prolonged PFS in the PD-L1 positive subgroup. Combinations of ICI and TKI are promising in early phase I and phase II trials. Results are currently expanded in larger phase III studies. The combination of vaccine and TKI in mRCC has not provided beneficial results so far. Bedke et al. [77] made the ensuing summations:
The current treatment landscape in metastatic renal cell carcinoma (mRCC) has been shifting towards immunooncology agents, which already had gained ground in the clinic as ICI monotherapy (nivolumab) or is likely to do in the near future as ICI combination (nivolumab and ipilimumab).
The future would hold promise of new combinations with TKIs and ICI or other immunooncology agents like vaccines and metabolic immune checkpoint inhibitors.
Singla et al. [78] evaluated the pathological response, safety, and feasibility of nephrectomy following the receipt of immune checkpoint inhibition (ICI) for renal cell carcinoma (RCC). With regard to the methods of their evaluation, they stated that patients who had undergone nephrectomy for renal cell carcinoma (RCC) after exposure to nivolumab monotherapy or combination ipilimumab/nivolumab were reviewed. Primary surgical outcomes which included operative time (OT), estimated blood loss (EBL), length of stay (LOS), readmission rates, and complication rates were documented. The pathological response in the primary and metastatic sites constituted secondary outcomes of their study. Singla et al. [78] summarised the results as follows:
Eleven nephrectomies that included 10 radical nephrectomies and 1 partial nephrectomy were undertaken in 10 patients after ICI with median postoperative follow-up 180 days.
Six patients had received 1 to 4 cycles of ipilimumab/nivolumab, while 5 patients did receive 2 to 12 infusions of nivolumab preoperatively.
Five surgeries were undertaken laparoscopically, and 4 patients did undergo concomitant thrombectomy. One patient did exhibit complete response (pT0) to ICI, and 3out of 4 patients who underwent metastasectomy for hepatic, pulmonary, or adrenal lesions did not exhibit any detectable malignancy in any of the metastases that were resected. None of the patients experienced any major intraoperative complications, and all surgical margins were negative.
The Median OT, EBL, and LOS were 180 minutes, 100 ml, and 4 days, respectively.
Four patients had experienced a complication, which included 3 that were addressed with interventional radiology procedures. One patient died of progressive disease more than 3 months after surgery, and 1 patient succumbed to pulmonary embolism complicated by sepsis. No complications or readmissions were noted in 6 patients.
Singla et al. [78] made ensuing conclusions:
Nephrectomy following ICI for renal cell carcinoma (RCC) is safe and technically feasible with favourable surgical outcomes and pathological response.
The timing of the nephrectomy relative to checkpoint dosing did not appear to impact outcome.
Biopsies of lesions responding radiographically to ICI might warrant attention prior to surgical excision.
Rassy et al. [79] made the ensuing iterations:
The treatment landscape of metastatic renal cell carcinoma (mRCC) had been transformed with the advent of antiangiogenics, taking into consideration tyrosine kinase inhibitors (TKIs) targeting vascular endothelial growth factor receptor (VEGFR), and immune checkpoint inhibitors (ICIs).
Both treatment options had improved upon the outcomes of patients and has modified the natural history of mRCC.
Clinical investigations had focused upon the evaluation of combination regimens that contain ICIs and VEGFR-directed TKIs. Namely, the combinations of axitinib plus pembrolizumab (KEYNOTE-426) and axitinib plus avelumab (JAVELIN RENAL 101) had demonstrated improved outcomes compared with sunitinib in treatment-naïve patients with mRCC.
Feng et al. [80] stated that hereditary leiomyomatosis and renal cell cancer (HLRCC)-associated kidney cancer is an uncommon and exceptionally aggressive tumour, with early metastasis and a patient who has this type of cancer tends to die at a young age. They also stated that majority of reported patients manifest usually with back pain and haematuria, and they died within 5 years pursuant to the diagnosis of the tumour. They additionally stated that at the time of publication of their article, there was no guideline or census about the management of HLRCC. On April 19, 2019, the Food and Drug Administration (FDA) of the USA did approve utilization of the combination of pembrolizumab and axitinib for first-line treatment of patients who have advanced renal cell carcinoma based upon the results of KEYNOTE-426 trial. They recommended that the combination of immunotherapy and targeted therapy should be considered for HLRCC. Feng et al. [80] reported a case of a 46-year-old man without family history, possessing specific mutation and sensitive to the combination of immunotherapy and targeted therapy. After he had completed seven cycles of combined treatments, his discomfort did improve and the lesions of his pleura almost disappeared and the mass within his left kidney area was basically stable. Feng et al. [80] stated that their reported patient might be the first one to receive the combination therapy and the efficacy seemed acceptable.
Motzer et al. [26] iterated that in a single-group, phase 1b trial, avelumab plus axitinib had resulted in objective responses in patients who had advanced renal-cell carcinoma. They conducted a phase 3 trial which involved previously untreated patients who had advanced renal-cell carcinoma compared avelumab plus axitinib with the standard-of-care sunitinib. With regard to the methods of the study, Motzer et al. [26] stated that they randomly assigned patients in a 1:1 ratio to receive avelumab (10 mg per kilogram of body weight) intravenously every 2 weeks plus axitinib (5 mg) orally twice daily or sunitinib (50 mg) orally once daily for 4 weeks (6-week cycle). The two independent primary end points of the study were progression-free survival and overall survival among patients with programmed death ligand 1 (PD-L1)-positive tumours. Their key secondary end point was progression-free survival in the overall population; and their other end points did include objective response and safety. Motzer et al. [26] summarised the results as follows:
A total of 886 patients had been assigned to receive avelumab plus axitinib (442 patients) or sunitinib (444 patients).
Among the 560 patients who had PD-L1-positive tumours which accounted for 63.2% of the patients, the median progression-free survival was 13.8 months with avelumab plus axitinib, in comparison with 7.2 months with sunitinib (hazard ratio for disease progression or death, 0.61; 95% confidence interval [CI], 0.47 to 0.79; P<0>
Among the patients who had PD-L1-positive tumours, the objective response rate was 55.2% with avelumab plus axitinib and 25.5% with sunitinib; at a median follow-up for overall survival of 11.6 months and 10.7 months in the two groups, 37 patients and 44 patients had died, respectively.
Adverse events during treatment had occurred in 99.5% of patients who were in the avelumab-plus-axitinib group and in 99.3% of patients who were in the sunitinib group; these events were grade 3 or higher in 71.2% and 71.5% of the patients in the respective groups.
Motzer et al. [26] concluded that the progression-free survival was significantly longer with avelumab plus axitinib in comparison with sunitinib among patients who received these agents as first-line treatment for advanced renal-cell carcinoma.
Rini et al.[27] stated that the combination of pembrolizumab and axitinib had shown antitumor activity in a phase 1b trial that involved patients who had previously untreated advanced renal-cell carcinoma. They also remarked that whether pembrolizumab plus axitinib would result in better outcomes in comparison with sunitinib in such patients was not clear. With regard to the methods of their study, Rini et al. [27] stated that in an open-label, phase 3 trial, they had randomly assigned 861 patients who had previously untreated advanced clear-cell renal-cell carcinoma to receive pembrolizumab (200 mg) intravenously once every 3 weeks plus axitinib (5 mg) orally twice daily (432 patients) or sunitinib (50 mg) orally once daily for the first 4 weeks of each 6-week cycle (429 patients). Their primary end points were overall survival and progression-free survival in the intention-to-treat population. Their key secondary end point was the objective response rate. All reported results were from the protocol-specified first interim analysis. Rini et al. [27] summarized the results as follows:
Pursuant to a median follow-up of 12.8 months, the estimated percentage of patients who were alive at 12 months was 89.9% in the pembrolizumab-axitinib group and 78.3% in the sunitinib group (hazard ratio for death, 0.53; 95% confidence interval [CI], 0.38 to 0.74; P<0>
The median progression-free survival was 15.1 months with regard to the pembrolizumab-axitinib group and 11.1 months with regard to the sunitinib group (hazard ratio for disease progression or death, 0.69; 95% CI, 0.57 to 0.84; P<0>
The objective response rate was 59.3% (95% CI, 54.5 to 63.9) with regard to the pembrolizumab-axitinib group and 35.7% (95% CI, 31.1 to 40.4) with regard to the sunitinib group (P<0>
The benefit of pembrolizumab plus axitinib was found across the International Metastatic Renal Cell Carcinoma Database Consortium risk groups (i.e., favourable, intermediate, and poor risk) and regardless of programmed death ligand 1 expression. Grade 3 or higher adverse events of any cause occurred in 75.8% of patients in the pembrolizumab-axitinib group and in 70.6% in the sunitinib group.
Rini et al. [27] made the ensuing conclusions:
Out of patients who had previously untreated advanced renal-cell carcinoma, treatment with utilization of pembrolizumab plus axitinib had resulted in significantly longer overall survival and progression-free survival, as well as a higher objective response rate, in comparison with treatment with sunitinib.
Gao et al. [81] made the ensuing iterations:
Oncological immunotherapy is a form of therapy which is intended to reactivate the immune response to tumour cells utilising agents that modulate immune checkpoints, such as programmed cell death protein 1 and its ligand (PD-1/PD-L), and cytotoxic T-lymphocyte-associated antigen 4.
Together with activation of the immune system to tumours, immune-mediated kidney side effects had been reported, majority of which had tended to be cases of interstitial nephritis. Glomerular disease, nevertheless. Does appear to be rare.
Gao et al. [81] reported a patient who had nephrotic syndrome related to treatment with an anti-PD1 antibody for Hodgkin lymphoma. After the third dose of anti-PD1 antibody, the patient did develop massive proteinuria and nephrotic syndrome. Kidney biopsy was undertake and pathology examination of the biopsy specimen demonstrated diffuse podocyte foot process effacement upon electron microscopy, which was consistent with minimal change disease. Corticosteroid treatment was administered and this yielded full and rapid remission of nephrotic syndrome in 1 month. Gao et al. [81] made the ensuing conclusions:
Their reported case had suggested an association between anti-PD1 therapeutic immune activation and the development of nephrotic syndrome.
Given the increasing prevalence of oncological immunotherapy, patients should be routinely monitored for kidney side effects that are associated with these agents.
Iribe et al. [82] stated that hereditary leiomyomatosis and renal cell cancer (HLRCC) is a rare autosomal dominant disorder that results from a germline mutation in the fumarate hydratase gene (FH). Individuals with FH mutations are at risk of developing renal cell carcinoma (RCC). Patients with HLRCC-associated RCC (HLRCC-RCC) have aggressive clinical courses, but there is as yet no standardized therapy for advanced HLRCC-RCC. We report an aggressive RCC case in a 49-year-old man. Nine weeks after undergoing a total nephroureterectomy of the right kidney, he had a metastasectomy at port site. Within 14 weeks of the initial surgery, multiple recurrent tumours developed in the right retroperitoneal space. The pathological diagnosis was FH-deficient RCC. Genetic testing identified a heterozygous germline mutation of FH (c.641_642delTA), which confirmed the diagnosis of HLRCC-RCC. He received combination therapy with the immune checkpoint inhibitors (ICIs) nivolumab and ipilimumab as the first-line therapy. After 31 weeks of ICI treatment, a complete response was achieved. The disease-free condition has been prolonged for 24 months since the initial surgical treatment. This is the first case report of successful treatment of HLRCC-RCC with nivolumab plus ipilimumab. This combination immunotherapy is expected to be an effective approach to treat patients with advanced-stage HLRCC-RCC.
Ball [83] stated the following:
Immunotherapy has been a mainstay of treatment for metastatic renal cell carcinoma (mRCC) since the introduction of high-dose interleukin-2.
Recently, improved knowledge of immune regulation and tumour-host immune interactions had led to the development of many new immunotherapies.
Immune checkpoint blockade showed promise in early clinical trials and this eventually resulted in the FDA approval of nivolumab (anti-PD-1) as a second-line treatment for mRCC.
Despite encouraging results, PD-1 blockade alone does not achieve durable responses in the majority of patients treated. Improved biomarkers for patient selection, tumour vaccines and combination therapy could augment the efficacy of existing immunotherapies.
Ball [83] also stated that recent progress with immune checkpoint blockade monotherapy has ushered in a new era of immunotherapeutic for metastatic renal cell carcinoma (RCC) and that combination immune checkpoint blockade, cancer vaccines, modulation of Tregs as well as T cell activation are all exciting areas of active investigation; nevertheless, the plethora of possible combinations means that careful clinical trials are essential in order to glean early signals of efficacy and to rule in or rule out promising combination approaches.
Kwatra et al. [84] stated the following:
Transplant patients were excluded from the pivotal phase III trials of checkpoint inhibitors in metastatic melanoma.
The efficacy and toxicity profiles of checkpoint inhibitors in this cohort of patients had not been well described.
To the best of their knowledge, their reported case was the first case report of a renal transplant patient with stage IV melanoma treated with a programmed cell death protein 1 checkpoint inhibitor that led to both treatment failure and renal graft rejection.
Kwatra et al. [84] reported a case of a 58-year-old white male who had a long-standing cadaveric renal transplant and who was diagnosed as having a B-Raf Proto-Oncogene, Serine/Threonine Kinase wild-type metastatic melanoma. He was treated with first-line pembrolizumab but he did experience subsequent graft failure and rapid disease progression. Kwatra et al. [84] made the ensuing conclusions:
Their reported case did highlight the risks associated with the administration of checkpoint inhibitors in patients who have a renal transplant and on immunosuppressive treatment.
More specifically, it does add to the literature which indicates that, compared with the cytotoxic T-lymphocyte-associated protein 4 inhibitor ipilimumab, anti-programmed cell death protein 1 agents are more likely to lead to renal graft failure.
Furthermore, these novel immunotherapy medicaments could be ineffective in transplant patients; therefore, clinicians should be very aware of those risks and they should carefully consider the selection of agents and full disclosure of the risks to their patients.
Brayer et al. [85] made the ensuing iterations:
Aldesleukin [interleukin-2 (IL-2) does induce durable complete responses in some kidney cancer and melanoma patients.
Nivolumab is an investigational antibody drug targeting programmed death-1 (PD-1) as a therapy, which does demonstrate activity within multiple types of cancer.
An expanding complement of immunotherapeutic agents does raise pertinent issues that relate the best way to utilize them.
Issues exist beyond the identification of an agent that does provide the superior-front-line response with the inclusion of: (a) when does one treatment potentiate another immune treatment? (b) When is the capacity of immune response exhausted and an approach without immune mechanism the better treatment?
Brayer et al. [85] reported a patient who had metastatic renal cell carcinoma (mRCC) which was not associated with regression of tumour as evident upon a PD-1 blockade that was given on an investigational trial, who then did achieve near complete response to bolus high-dose IL-2 treatment, maintaining a persistent response off treatment. Brayer et al. [85] iterated that their reported case did emphasize upon the need to develop improved predictors of response to immune treatments, especially as they could be applied in order to optimize sequential. They also iterated that immunotherapy modalities do predict when to turn to targeted agents in renal cell carcinoma, and represents as example of efficacious IL-2 application as a second-line therapy.
Birkhäuser et al. [86] analysed the outcomes of patients who had metastatic renal cell carcinoma who were treated with salvage-targeted therapy after progressing on high-dose interleukin (IL)-2 immunotherapy in a tertiary referral centre. They studied a retrospective nonrandomized cohort of patients that consisted of 286 patients who had metastatic renal cell carcinoma and who were treated from 2003 to 2010 who were analysed from the University of California, Los Angeles (UCLA) Kidney Cancer database. All of the patients had undergone cytoreductive nephrectomy, and 21 patients had undergone salvage-targeted therapy after progression on high-dose IL-2, whereas 111 patients received targeted therapy alone. The remaining 154 patients had undergone other treatment combinations or experimental targeted therapy agents only. Since 2003, selection of patients for high-dose IL-2 was increasingly based upon clinical, pathological, and molecular criteria (UCLA CPM criteria). The disease-specific survival was calculated from the time of the diagnosis of metastatic renal cell carcinoma. Birkhäuser et al.[86] summarised the results as follows:
The patients were selected according to UCLA CPM criteria and they were treated with salvage-targeted therapy after progressing on high-dose IL-2 experienced a significantly greater disease-specific survival (median not reached) than those treated with targeted therapy alone (30 months; P = 0.004).
Since 2006, all high-dose IL-2 patients had met the UCLA CPM criteria and they were able to receive salvage-targeted therapy upon progression.
The disease-specific survival calculated from initiation of targeted therapy was comparable for patients who were treated with salvage-targeted therapy after progression on high-dose IL-2 (34 months) versus first-line targeted therapy (26 months; P = 0.175).
Birkhäuser et al. [86] stated that:
Patients who were selected for high-dose IL-2 based on UCLA CPM criteria and who were treated with salvage-targeted therapy upon progression had achieved outstanding disease-specific survival.
Their data did suggest a new algorithm for carefully selected patients who have metastatic renal cell carcinoma based on UCLA CPM criteria to receive first-line high-dose IL-2 while reserving their option for salvage-targeted therapy with uncompromised efficacy upon progression.
Pizza et al. [87] reported that from April 1986 to September 2000, 122 MRCC patients had undergone treatment by monthly intra-lymphatic injections (containing a mean of 573 IL-2 U and 26 × 106 LAK cells) and intra-muscular administration of IFN and TF; 71 patients also had received a 3-day cycle of monthly IL-2 inhalations with a mean of 998 daily U. MRCC cases that were not treated by immunotherapy (n = 89) represented their historical controls. Pizza et al. [87] reported the results as follows:
Adverse clinical side effects related to treatment were negligible. CR (n = 11) and PR (n = 13) were noticed in 24/122 patients. Of 24 responding patients, 17 resumed progression, whereas 7 remain in remission 11-69 months later.
The overall median survival of treated patients (28 months) was 3.5-fold higher in comparison with the median survival of historical controls (7.5 months), and a Kaplan-Meier curve showed 25% survival 11 years after the beginning of immunotherapy.
Apparently, the addition of IL-2 by inhalation had improved survival.
Pizza et al.[87] made the following conclusions:
The present immunotherapy protocol does appear to be efficacious, safe, devoid of adverse side effects, far less costly in comparison with others and able to offer a good quality of life to MRCC patients.
If their results are confirmed in a multi-centre trial, it could set the basis for developing low-dose immunomodulatory treatments.
Belldegrun et al. [88] stated that the management of renal cell carcinoma (RCC) is evolving toward less extirpative surgery and the utilization of targeted therapy. Belldegrun et al. [88] undertook a prospective database study including clinical and pathological variables for 1632 patients who had RCC who were treated between 1989 and 2005. The patients were stratified using the University of California-Los Angeles Integrated Staging System (UISS) into low-, intermediate-, and high-risk groups. They measured the disease-specific survival (DSS). They also assessed the response to systemic treatment for patients who had advanced disease. Belldegrun et al. [88] summarised the results as follows:
Nephrectomy was undertaken in 1492 patients.
The Overall 5-, 10-, and 15-year DSS was 55%, 40%, and 29%.
For localized disease, 5- and 10-year DSS for UISS low-, intermediate-, and high-risk groups was 97% and 92%, 81% and 61%, and 62% and 41%, respectively.
For metastatic disease, 5- and 10-year DSS for UISS low-, intermediate-, and high-risk groups was 41% and 31%, 18% and 7%, and 8% and 0%, respectively.
Patients who had metastatic disease who were receiving immunotherapy (n = 453) had complete response in 7% (median survival [MS], 120+ months), partial response in 15% (MS, 42.8 months), stable disease in 33% (MS, 38.6 months), and progressive disease in 45% (MS, 11.6 months
Belldegrun et al. [88] made the ensuing conclusions:
Majority of patients who had localized RCC did well with surgery alone, but effective adjuvant therapy was needed for patients who were identified as at high risk for the development of recurrence.
For advanced disease, newer targeted and potentially less toxic treatments should be at least as effective as those achieved with aggressive surgical resection and immunotherapy.
Vaishampayan, et al. [89] stated that with the advent and availability of targeted treatment, the treatment of advanced/metastatic renal cell carcinoma (RCC) had undergone a drastic change in 2005 and that the effect of this change on clinical outcome within the population had not been studied. Vaishampayan, et al. [89] evaluated the overall survival (OS), before, and after availability of targeted therapy, for advanced RCC cases in the population-based Surveillance, Epidemiology, and End Results (SEER) cancer registry. With regard to the materials and methods, Vaishampayan, et al. [89] stated that all advanced (regional and distant stage) RCC cases that were diagnosed within the 2000 to 2008 time periods were included in their study. Because SEER does not report the exact therapy, and because targeted therapy was initially approved in 2005, they evaluated and compared the overall survival (OS) outcomes of advanced RCC cases that were diagnosed between the years 2000 and 2003 (before targeted therapy era) with that of those diagnosed between 2005 and 2008 (targeted therapy era). Vaishampayan, et al. [89] summarised the results as follows:
There was a significant improvement in overall survival (OS) for advanced RCC patients who were treated in the targeted therapy era (n = 12,330) in comparison with those who were treated in the era before targeted therapy (n =11,565) (median OS 20 months vs. 15 months, P = .0006).
Multivariate analysis had revealed that in the time period before targeted therapy, age older than 65 years, black race, and lack of nephrectomy were predictors of a shorter OS.
Vaishampayan, et al. [89] made the following conclusions:
In univariate and multivariate analysis, targeted therapy demonstrated improvement in OS.
Increasing access to targeted therapies is likely to improve outcomes in advanced RCC.
Klapper et al. [90] stated that the treatment of metastatic renal cell carcinoma (RCC) with high-dose interleukin-2 (HD IL-2) had had been ensued with durable regression of tumour in a minority of patients. Klapper et al. [90]] reported their 20-year experience of administering this immunotherapeutic agent. With regard to the methods, Klapper et al. [90] stated that patients who had metastatic RCC in 259 patients who were treated with HD IL-2 alone from January 13, 1986 through December 31, 2006 at the Surgery Branch of the National Cancer Institute. Potential predictive factors for response and survival, both pre-treatment and treatment-related, were first subjected to univariate analysis and then to multivariate logistic regression or a Cox proportional hazards model. The authors finally investigated Memorial Sloan-Kettering Cancer Center (MSKCC) prognostic factors for survival in order to assess their predictive value in the patient population in the current study. Klapper et al. [90] summarised the results as follows:
A total of 23 patients did experience a complete response and 30 of the patients had achieved a partial response, for an overall objective response rate of 20%.
All partial responders did develop disease recurrence at the time of the last follow‒up, but only 4 complete responders had did develop disease recurrence by that time.
Despite toxicities, only 2 patients of the patients had developed treatment-related mortalities over this same time period.
A higher baseline weight (P = .05) and MSKCC prognostic factors (P = .02) were noted to be the variables that were mostly associated with response.
For survival longer than 4 years and overall survival, several pre-treatment and treatment‒related factors had maintained significance, but none of them was more so than response (P < .0001).
Klapper et al. [90] made the following conclusions:
HD IL-2 could induce complete regression of tumour in a small number of patients, and many patients had experienced extended disease-free intervals.
Given its relative safety, HD IL-2 should still be considered a first-line treatment option in patients who have metastatic RCC who do have an overall good performance status.
Peláez Bejarano et al. [91] stated that Pembrolizumab is a monoclonal antibody which was approved for adult patients who have advanced non–small-cell lung cancer (NSCLC). They also stated that even though immune related adverse events are considered to be well tolerated, complications could occur and discontinuation of the treatment could be needed.
Peláez Bejarano et al. [91] reported a 62-year old patient who was diagnosed with advanced non-small cell lung cancer who experienced a decline in the renal function after receiving seven cycles with pembrolizumab. After excluding other common causes of interstitial nephritis, pembrolizumab was attributed as a cause of the patients’ interstitial nephritis. At first, the toxicity was managed with corticosteroids and closely monitoring the patient was undertaken, but eventually pembrolizumab had to be discontinued due to the fact that the kidney function did not recover. Peláez Bejarano et al. [91] stated that renal and urinary disorders were reported in less than 3% of patients who had been treated with pembrolizumab, being interstitial nephritis the most reported toxicity. They additionally stated that the kidney damage could be a complication to consider in patients who are receiving pembrolizumab as well as early identification of an increase in serum creatinine levels could be helpful with regard to prevention by establishing an effective treatment, although it might not mean a total recovery of kidney function.
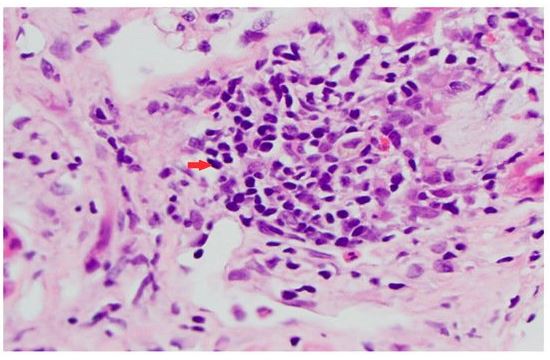
Basnet et al. [92] stated that Pembrolizumab is a novel immune checkpoint inhibitor which was approved for utilisation in non-small cell lung carcinoma and that there had been a few cases that had associated adverse renal outcomes with pembrolizumab. Basnet et al. [92] reported a case of acute kidney injury in a patient who was on pembrolizumab and who was noted to have acute tubulointerstitial nephritis on renal biopsy. Pembrolizumab was discontinued and the patient was commenced on long-term corticosteroids with a taper. Her renal function did improve partially with treatment. The illustrated figure 1 shows histology examination features of the kidney biopsy specimen that confirmed the diagnosis of tubulointerstitial nephritis.
Vakil et al. [93] stated that kidney injury that is associated with the use of immune checkpoint inhibitors that target the programmed death-1 molecule commonly does present as acute tubulointerstitial nephritis on kidney biopsy. Vakil et al. [93] reported a case of a 66-year-old male who had developed acute kidney injury at 6 months pursuant to initiation of treatment with anti-programmed death-1 antibody, nivolumab, for treatment of metastatic urothelial carcinoma. He had a renal biopsy and pathology examination of the biopsy specimen demonstrated focal moderate-to-severe lymphocytic tubulitis with minimal interstitial inflammation. Programmed death ligand-1 immunopositivity was identified only in tubules exhibiting lymphocytic tubulitis. The patient’s renal function improved to baseline with conservative management which consisted of discontinuation of nivolumab followed by prednisone treatment.
Haineala et al. [94] stated that kidney cancers do account for about 2% of human malignancies and that in recent decades, the incidence of this cancer type had gradually increased, mainly in view of advances in imaging. Haineala et al. [94] additionally stated the following:
The metastatic potential of these cancers is significant and a quarter of patients would immediately manifest with metastases and more than one third of patients who are treated with nephrectomy for a localized disease would develop metastases during their course.
In total, more than half of the patients would suffer from the consequences of metastasis.
The median survival at this stage is only thirteen months, so the therapeutic challenge is immense.
Haineala et al. [94] reported a case left renal clear cell carcinoma with brain, lung, right adrenal, bone and lymph node metastases in a 55-year-old man The patient had received only one line of anticancer treatment with sunitinib, which could not be continued due to his haemorrhagic manifestations in brain metastases. His treatment was changed with immunotherapy which showed its effect even if it was stopped due to the patient wishes in the context of the COVID-19 epidemic. Haineala et al. [94] concluded that immunotherapy does open the doors to a new era in treatment of metastatic renal cancer and does show efficiency even after it has been stopped.
Daanen, et al. [95] stated that immune checkpoint inhibitors had taken an important place with regard to the treatment of different types of malignancies and that these drugs are known to have specific immune-mediated adverse events. They described a case of severe nephrotic syndrome following treatment with nivolumab in a patient who had renal cell carcinoma. Daneen et al. [95] reported a 62-year-old male who was treated with nivolumab for papillary renal cell carcinoma type 2 for a period of 8 weeks when he was admitted to the hospital with a severe nephrotic syndrome and acute kidney injury. He underwent renal biopsy and pathology examination of the biopsy specimens showed focal segmental glomerulosclerosis. Treatment with high-dose corticosteroids was associated with insufficient effect; however, the addition of mycophenolate mofetil resulted in remission of the nephrotic syndrome and recovery of renal function. Proteinuria did subsequently relapse during tapering of his corticosteroid treatment. Daanen et al. [95] .made the following conclusions:
The time course in the patient had strongly suggested that the nephrotic syndrome occurred as an adverse drug reaction to nivolumab treatment.
If during nivolumab treatment renal insufficiency, hypoalbuminemia, or proteinuria does develop, further analysis for a possible nephrotic syndrome would be warranted for early detection and treatment of this life-threatening complication.
Wu and Mou. [95] stated the following:
For early-stage upper urothelial carcinoma, total nephroureterectomy which is combined with urinary bladder sleeve resection is the standard treatment.
Nevertheless, for patients who have advanced disease, there is a lack of effective therapeutic strategies.
Over recent years, with an increased understanding of cancer immunobiology, systemic immunotherapies targeting immune checkpoint inhibition had been explored and clinically utilised in the area of urothelial carcinoma.
The programmed cell death 1 receptor (PD-1) and its ligand (PDL1) are important negative regulators of immune activity, which prevent the destruction of normal tissues and autoimmunity.
These days, five immune checkpoint inhibitors blocking PD-1 (pembrolizumab, nivolumab) or PD-L1 (atezolizumab, durvalumab, and avelumab) have been approved by the United States Food and Drug Administration (US FDA) for the first- or second-line utilisation in urothelial carcinoma, based upon durable response and manageable safety profiles which had been observed in relevant clinical trials.
Wu and Mou. [95] reported the case of a 64-year-old patient who had renal pelvis carcinoma and who went on to develop lung metastasis pursuant to post-operative chemotherapy. CT scan was undertaken which showed multiple scattered solid small nodule foci within both lungs that were considered as metastases. The patient received immunotherapy with PD-L1 monoclonal antibody (Durvalumab) alone, and did achieve complete remission (CR) after 3 cycles of treatment. During the treatment, slight weakness was reported by the patient, and no nausea, fever and other adverse events were observed. Wu et al. [95] stated that their case had shown that durvalumab could effectively and safely treat a case of renal pelvis carcinoma with lung metastases.
Kobayashi et al. [96] stated that γδ T-cells had recently attracted considerable attention in the development of novel cancer immunotherapy, and many different approaches had been designed and employed in clinical trials. Kobayashi et al. [95] reported a patient who developed lung metastasis following radical nephrectomy for renal cell carcinoma who had six cycles of adoptive immunotherapy using autologous in vitro-activated γδ T-cells followed by low-dose interleukin-2 and zoledronic acid intravenous infusion. They reported that complete remission was achieved which had been maintained for 2 years without any additional treatment. They also reported that immunological analysis did demonstrate a high level of interferon-gamma four hours through one day following the transfer and peripheral blood γδ T-cells increased 10-fold from the baseline value, 7 days after the transfer. They additionally reported that no serious adverse events were observed. Kobayashi et al. [96] concluded that:
Adoptive immunotherapy utilising γδ T-cells was shown in their reported case to be clinically beneficial and safe, and could become a treatment option for patients who have advanced renal cell carcinoma (RCC).
Pizza et al. [97] stated that in a limited study, which comprised of only ten patients, they had previously reported that allogeneic irradiated RCC-cell-line cells, engineered to produce IL-2 (ACHN-IL-2), admixed with autologous metastatic formalin-treated tumour cells were used to vaccinate MRCC patients in progression of disease and also receiving IL-2 immunotherapy. The cells, admixed to autologous TC, were administered subcutaneously. Pizza et al. [96] in 2004 reported an extended study on thirty patients and one hundred thirty-one controls. The patients received 4ñ20 injections (mean 10 ± 4), containing an average of 92 × 106 ± 45 × 106 ACHN-IL-2 transfected cells (a minimum of 25 × 106, and a maximum of 200 × 106). Autologous TC, admixed to allogeneic, were also administered by 4ñ16 s.c. injections (mean 7 ± 3), i.e. a total of 12 × 106ñ160 × 106 cells. Vaccination was administered during 73ñ1451 (307 ± 316) days, and the follow-up continued for 1122 ± 1240 days (106ñ5137). Throughout the entire period, the patients had continued receiving the previously set immunotherapy treatment. No adverse side effects related to the treatment were observed. One complete and four partial tumour responses were found, as well as nine cases of stable disease. Pizza et al. [96] additionally reported that thirteen patients died in the treated group (43%) and 63 (44%) died within the control group. Responding patients resumed progression in 4ñ11 months and died 18 and 36 months after commencing the vaccine therapy. The Gehan Wilcoxonís test revealed a significantly (P < 0>
Tani et al. [98] produced lethally irradiated retrovirally GM-CSF-transduced autologous renal tumour cell vaccines (GVAX) from six Japanese patients with stage IV renal cell cancer (RCC). They reported that four patients received GVAX ranging from 1.4 × 108 to 3.7 × 108 cells on 6–17 occasions. They also reported that throughout a total of 48 vaccinations, there were no severe adverse events and following the vaccinations, DTH skin tests became positive to autologous RCC (auto-RCC) in all patients. The vaccination sites did show significant infiltration by CD4+ T cells, eosinophils, and HLA-DR-positive cells. The kinetic analyses of cellular immune responses utilising peripheral blood lymphocytes had revealed an enhanced proliferative response against auto-RCC in four patients, and cytotoxicity against auto-RCC was augmented in three patients. T cell receptor β-chain analysis did reveal oligoclonal expansion of T cells in the peripheral blood, skin biopsy specimens from DTH sites, and tumours. Western blot analysis was undertaken which demonstrated the induction of a humoral immune response against auto-RCC. Two of the four patients were alive at the time of publication of their article 58 and 40 months after the initial vaccination with low-dose interleukin-2. They concluded that the results had suggested that GVAX substantially enhanced the antitumor cellular and humoral immune responses, which might have contributed to the relatively long survival times of our patients in the present study
Werthmann et al. [99] stated the following:
Metastatic renal cell carcinoma does have a poor prognosis.
Treatment approaches with utilization of immunotherapy do show promising results in subpopulations.
Viscum album extracts that are used as an adjunct to cancer treatment do have cytotoxic, apoptogenic, and immune-stimulating properties and they do show synergistic effects with chemotherapy agents.
Werthmann et al. [99] reported a 51-year-old male who was diagnosed as having metastatic renal cell carcinoma of clear cell histology which was classified as pT3a, N1, M1, G3. The patient underwent nephrectomy, and he received chemoimmunotherapy (interferon-α2a, interleukin-2, fluorouracil, isotretinoin). Additionally, the patient received V. album extracts as intravenous infusions and subcutaneous injections. One year pursuant to his surgery, the patient was in complete remission, which was ongoing 18 years following the initial diagnosis. Werthmann et al. [98] stated that their reported case had shown an extraordinarily long survival of a metastasized renal cell carcinoma patient under chemoimmunotherapy and fever-inducing V. album extracts and that his combined treatment might have synergistically contributed to the remission of his tumour and control of tumour. They also stated that with regard to clinical relevance, further investigations are required
Bedke et al. [100] stated that the treatment landscape in advanced and metastatic renal cell carcinoma (RCC) has been moving from the inhibition of tyrosine kinases (TKI) and the mammalian target of rapamycin (mTOR) inhibitors to specific immune-oncology agents like immune checkpoint inhibitors (ICI). They focussed their review on the recent immunooncology developments and available trial results within the preceding12 months. They also stated that ICI as monotherapy (nivolumab) or immunooncology and immunooncology combinations (nivolumab and ipilimumab) had demonstrated positive results on prolonged overall survival in phase III trials. They also stated that the combination of ICI (atezolizumab) and bevacizumab had provided positive signals in prolonged PFS in the PD-L1 positive subgroup. They further stated that the results of combinations of ICI and TKI are promising in early phase I and phase II trials as well as the results are currently expanded in larger phase III studies. Furthermore they found out that combination of vaccine and TKI in mRCC had not provided beneficial results so far. Bedke et al. [100] made the ensuing summations:
The current treatment landscape in mRCC has been shifting towards immunooncology agents, which already have gained ground in the clinic as ICI monotherapy (nivolumab) or is likely to do so within the near future as ICI combination (nivolumab and ipilimumab).
The future would hold promise of new combinations with TKIs and ICI or other immunooncology agents like vaccines and metabolic immune checkpoint inhibitors.
Labbate et al. [101] made the following statements related to localized renal cell carcinoma:
Clinically localized renal cell carcinoma has tended to be treated primarily with surgery followed by observation or adjuvant sunitinib in selected high-risk patients.
The checkpoint inhibitor immunotherapeutic agents nivolumab and ipilimumab have recently demonstrated a survival benefit in the first-line metastatic setting.
Up to the time of the publication of their article, there had been no reports on the response of localized renal cancer to modern immunotherapy.
They had reported a remarkable response of an advanced tumour thrombus to combined immunotherapy which facilitated curative-intent resection of the non-responding primary renal tumour. They also characterized the tumour microenvironment within the responding and non-responding tumours.
Labbarte et al. [101] reported a 54-year-old female who was diagnosed as having a locally advanced clear cell renal cell carcinoma with a level IV tumour thrombus of the vena cava. She was at first deemed to be unfit for surgical resection due to her poor performance status. She underwent neoadjuvant immunotherapy with nivolumab and ipilimumab which was associated with a complete response of the vena cava and renal vein tumour thrombus, but she had stable disease within her renal mass. She underwent complete surgical resection of the tumour with negative surgical resection margins and had remained disease-free longer than 1 year pursuant to her diagnosis with no further systemic therapy. Notably, pathological analysis showed a complete response within the vena cava and renal vein, but substantial viable cancer had remained within the kidney. Multichannel immunofluorescence was undertaken and which showed marked infiltration of immune cells including CD8+ T cells and Batf3+ dendritic cells in the thrombus, while the residual renal tumour demonstrated a non-T cell-inflamed phenotype. Labbarte et al. [01] made the following conclusions:
Preoperative immunotherapy with nivolumab and ipilimumab for locally advanced clear cell renal cancer had resulted in a complete response of an extensive vena cava tumour thrombus, which enabled curative-intent resection of a non-responding primary tumour.
If validated in larger cohorts, preoperative immunotherapy for locally advanced renal cell carcinoma might ultimately impact upon the surgical planning and long-term prognosis.
Gouttefangeas et al. [102] stated the following:
Carcinomas of the kidney generally tends to be associated with a poor prognosis and do respond minimally to classical radiotherapy or chemotherapy.
Immunotherapy does constitute an interesting alternative to these established forms of treatment, and indeed, cytokine-based therapies have been utilised for many years, which had led to favourable clinical responses in a small subset of patients.
During the past few years, immunotherapeutic trials that target renal cell tumour-associated antigens had also been reported, with diverse passive or active approaches utilising antibodies or aimed at activating tumour-directed T lymphocytes.
Ansari et al. [103] stated the following:
Treatment of patients who have metastatic renal cell carcinoma (mRCC) and end-stage renal disease (ESRD) on dialysis does pose a treatment challenge, particularly because this patient group was excluded from the pivotal clinical trials.
Additionally, there is no certainty regarding drug dosing/pharmacokinetics, lack of safety and efficacy data, and potential for increased toxicity when utilising targeted therapy or immunotherapy for the management of patients with mRCC who are on dialysis.
Nivolumab, an anti-programmed death-1 immune checkpoint inhibitor antibody, is indicated for the therapy of patients with mRCC who have received prior antiangiogenic therapy.
Given the aforementioned uncertainties, clinicians might be reluctant to utilise nivolumab for this patient population, leading to potential denial of life-prolonging medications.
Ansari et al. [103] reported a 72-year-old gentleman who manifested with a 6-week history of haematuria and he had a computed tomography (CT) scan which revealed a left kidney tumour that was suggestive of renal cell carcinoma (RCC). His comorbidities did include type 2 diabetes mellitus and hypertension. He had no family history of any malignancy. He was a life-long non-smoker and his Eastern Cooperative Oncology Group (ECOG) performance status was 1. He did undergo left partial nephrectomy and histopathology examination of the specimen revealed the tumour to be a locally advanced clear cell RCC, Fuhrman grade 2, with involvement of 3 out of 20 lymph nodes (pT3A N1 M0). He post-operatively, developed ESRD and he was commenced on dialysis 3 times/week. Two years subsequently, he developed a local recurrence within his left kidney and he underwent left radical nephrectomy. Histopathology examination of the surgical specimen demonstrated a 5 cm, clear cell carcinoma, Fuhrman grade 2 with invasion of the perinephric fat and renal vessels. He did remain on regular follow-up and unfortunately 2 years subsequently developed further disease progression with a renal bed recurrence together with multiple bone and lung metastases. He did receive high-dose palliative radiotherapy to the renal bed 40 Gray in 20 fractions which was ensued by the commencement of systemic treatment with dose-reduced pazopanib. The dose of pazopanib was reduced to 200 mg daily due to his poor ECOG performance status of 3 and ongoing renal dialysis. Unfortunately, he had follow-up CT scan 3 months later which demonstrated significant disease progression within his renal bed, bone, and lung metastases. He also developed significant pain that was scored as 8 out of 10 over his left loin secondary to the finding of his renal bed metastatic deposit. He was commenced on nivolumab 3 mg/kg in the first instance and this was later switched to 240 mg flat dose intravenously every 2 weeks. He had tolerated the treatment extremely well with no grade 2 to 4 toxicities. Clinically, there was a significant improvement in his pain control with a noticeable reduction in his pain score from 8 out of 10 to 3 out of 10 and his ECOG performance status improved to 2. Follow-up CT scans showed a partial response as per response evaluation criteria in solid tumours (RECIST) version 1.1. There was a significant reduction in the size of his lung and renal bed metastases (Figures 2 and 3). He has remained on nivolumab 22 months from the commencement of his treatment with serial imaging showing ongoing response.
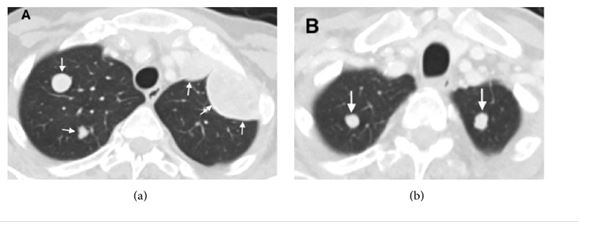
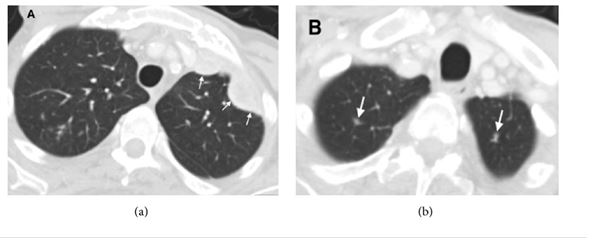
Ansari et al. [103] stated that their case report had added further to literature by highlighting the usage of nivolumab in an elderly patient who had mRCC with ESRD and dialysis. Despite many comorbidities, he had tolerated the treatment well with minimal treatment-related toxicities. Treatment with nivolumab was associated with a partial radiological response as per RECIST v1.1 together with an improvement in his pain control as well as in his nd performance status. Even though he median duration of nivolumab treatment in the CheckMate-025 trial was 5.5 months, it was interesting to note that, despite the afore-mentioned comorbidities, their reported patient had been on nivolumab treatment for 22 months with ongoing treatment response. Ansari et al. [103] made the following conclusions:
In a resource-limited healthcare setting, clinicians might opt to strictly follow the inclusion criteria of the pivotal trials and show reluctance to offer nivolumab to mRCC patients who have ESRD on dialysis.
Nevertheless, the evidence outlined in their article had demonstrated the pharmacokinetic data and case studies to make a compelling case for the consideration of nivolumab in patients with mRCC and ESRD requiring dialysis after failure of prior antiangiogenic therapy.
They would recommend that patients who have mRCC with ESRD and dialysis should be treated with standard protocols applicable to those with normal renal function.
Olsen et al. [104] stated that Combination regimens that include immune checkpoint (ICI) and vascular endothelial growth factor (VEGF) inhibition had opened the door to new treatment opportunities for patients who had metastatic renal cell carcinoma (mRCC). They also stated that whilst these treatment options had provided improved tolerability and better outcomes compared to older regimens, many patients still experience a myriad of treatment-related adverse events. They additionally stated that considering that these regimens had been recently approved for mRCC, the complete side effect profile might not be fully elucidated yet. Olsen et al. [104] reported a We report a case of a 73-year old white man, who had metastatic renal cell carcinoma (mRCC), who was managed with an ICI-VEGF inhibitor combination regimen. He did experience a partial response (see Fig. 4) but he did have side effects which included symptomatic cyanosis which was diagnosed as methemoglobinemia that led to treatment discontinuation. Upon holding his treatment, his methemoglobinemia and cyanosis resolved. Olsen et al. [104] made the ensuing conclusions:
VEGF-ICI therapy does provide novel treatment regimens for advanced solid tumour malignancies including mRCC.
While demonstrated to have improved efficacy in clinical trials, it is crucial that oncologists do ascertain the full side effect profile of these novel agents especially as their utilisation does become more standard in the management of advanced malignancies.
To their knowledge, their reported case is the first reported case of a patient experiencing symptomatic methemoglobinemia as an adverse event associated with a VEGF-ICI combination regimen.
While the cause of this side effect is not clear, in their reported article, they had attempted to elucidate a process that is in line with the mechanism of action of these therapies to explain how these agents, specifically the axitinib, could had caused the methemoglobin to rise to a symptomatic level.
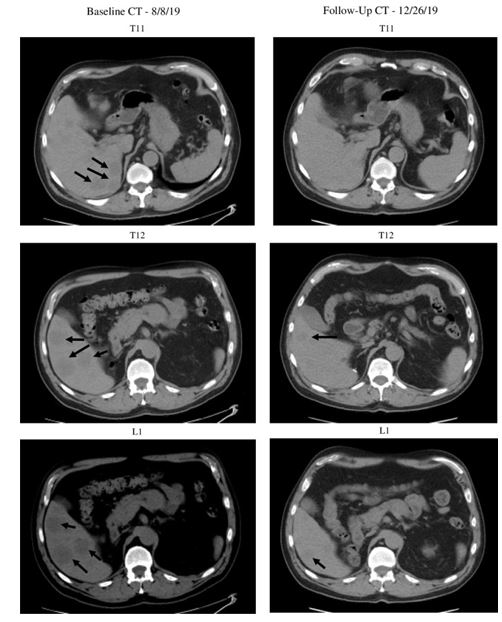
Olsen et al. [104] made the ensuing conclusions:
Combination immune therapy does provide an exciting new treatment option for metastatic renal cell carcinoma (mRCC) patients which does combine the benefits of multiple potent therapies for an even greater treatment effect.
These agents could provide clinical oncologists with additional treatment options for the management of aggressive malignancies like mRCC.
Nevertheless, it is very important that medical oncologists do appreciate the benefits and costs these treatment regimens would impose upon patients.
Adverse events, such as the one they had reported their case report, could be life-threatening and could have significant impacts upon the patient’s prognosis and quality of life.
Current trials that use PD-1 and VEGF-TKI combination treatment have demonstrated promising results and FDA approval for patients with advanced RCC [27]
Their reported case had illustrated one such example of a renal cell carcinoma (RCC) patient who had experienced an uncommon but important adverse hematologic event.
The novelty of their reported case is both a strength and a weakness in the case study.
The resulting methemoglobinemia for the patient could have equally been involved with another underlying disease process as it could represent a true side effect of VEGF-TKI and ICI combination therapy.
Current clinical trials should make ongoing efforts to note these uncommon side effects in order to better appreciate the side-effect profile of these novel treatment agents.
Cases, such as their reported case, could hopefully assist practicing oncologists to recognize the rare and potentially severe side effect of methemoglobinemia in metastatic renal cell carcinoma (mRCC) patients treated who are treated with ICI and VEGF-TKI combination therap
Olsen et al. [104] summarized the patient’s voluntary perspective as follows:
I was given pembrolizumab by intravenous means every 21 days for three months.
I also was placed on 5 MG tablets of Axitinib.
The combination treatment did have great success with decreasing and/or eliminating a tumour from my pancreas and two on my liver. Nevertheless, the side effects had caused me to have to stop the treatment.
The first symptom was a loss of appetite which in turn was ensued by fatigue, tiredness, loss of weight, and loss of voice volume. There was no sickness,
I just did not feel well. My lips and eye whites turned blue and I was ultimately diagnosed with methemoglobinemia. I was weak, and I needed weekly infusions of fluid, and ultimately I had to quit the treatment after three months.
There was never any pain from anything.
Dehydration became my biggest issue as I spent most of my time sleeping and not wanting to eat.
I did find success managing this situation with my general practitioner who is an internist specializing in kidney and diabetes.
It is best to start this journey with a good oncologist who will take the time to determine what is happening with your systems. I was fortunate enough to find great doctor(s).
Ohta et al. [105] stated that immunotherapy using a Wilms tumour (WT1) peptide had been undergoing clinical trials for adulthood leukaemia and solid cancer with promising results. Ohta et al. [104] used WT1 peptide vaccination to treat a 6-year-old girl who had metastatic alveolar rhabdomyosarcoma. She received weekly intradermal injection with HLA-A*2404-restricted, 9-mer WT1 peptide against residual bone disease. After 3 months of treatment, her bone disease disappeared, concurrent with an increase in the frequency of WT1-specific cytotoxic T lymphocytes (CTLs). A high proportion of WT1-specific CTLs with effector or effector memory phenotype were detected in the patient’s peripheral blood. At the time of the report of the case, she (the patient) was still on continued WT1 peptide immunotherapy in a disease-free condition for 22 months. Ohta et al. [105] suggested that WT1 peptide-based immunotherapy should be a promising option for high-risk rhabdomyosarcoma in childhood.
Kopecky et al. [106] stated that great progress had recently been made with regard to the treatment of metastatic renal cell carcinoma, including the introduction of nivolumab, an immune checkpoint inhibitor. Despite the results of the treatment having been promising, the treatment has brought a completely new spectrum of adverse events, which is distinct from those experienced with small-molecule kinase inhibitors. Neurologic immune-related adverse events could be serious and potentially life-threatening complications that require immediate immunosuppressive treatment. Only a few cases of immune-related encephalitis induced by checkpoint inhibitors had been described and the data regarding the management of this serious adverse event had been limited. Kopecky et al [106] reported the case of a 63-year-old white man who had metastatic renal cancer and who developed severe chorea-like dyskinesia during nivolumab treatment. The findings on magnetic resonance imaging scan of his brain and flow cytometry of cerebrospinal fluid, and the positivity of anti-paraneoplastic antigen Ma2 immunoglobuline G class autoantibodies were consistent with a diagnosis of immune-related encephalitis. High-dose intravenous corticosteroid therapy was commenced immediately, with no signs of improvement, even when infliximab was added. The patient refused to have further hospitalization and he was accordingly discharged. Three weeks later, he manifested with signs of severe urosepsis. Despite intensive therapy, he died 4 days following his admission. Kopecky et al. [106] made the following conclusions:
The treatment of less frequent immune-related adverse events has not been fully established and more information is needed to provide uniform recommendations
Immune-related encephalitis is a severe and potentially fatal complication that requires immediate hospital admission and extensive immunosuppressive treatment.
The examination of cerebrospinal fluid for paraneoplastic antibodies, such as anti-N-methyl-D-aspartate receptor and anti-Ma2 antibodies, in order to distinguish autoimmune aetiology from other possible causes is essentially important and highly recommended.
Immunotherapy in the treatment of locally advanced / metastatic carcinomas has been demonstrated to provide improvement in the overall survival of a number patients; nevertheless, some patients potentially could develop side effects and complications associated with immunotherapy which all clinicians need to be aware of these side effects and complications in order to identify them quickly and treat them.
There is the possibility that immunotherapy may not be easily available to be utilized in the treatment of advanced / metastatic kidney cancers due to the high cost of this treatment especially in developing countries where perhaps the patients as well as the health care facilities might not have enough funds to enable provision of immunotherapy.
Some of the possible side effects include: flu-like symptoms (fever, chills, muscle aches), nausea, low blood pressure, fluid build-up within the lungs, breathing difficulties, kidney damage, heart attacks, intestinal bleeding, rapid heartbeat, mental changes, neurological side-effects within the central and peripheral nervous system.
Other possible side effects and complications related to immunotherapy in the treatment of metastatic / advanced carcinoma of the kidney include methemoglobinemia, nephritis, tubulointestinal nephritis, nephrotic syndrome as well as chorea-like dyskinesia,
It would be important for clinicians that treat patients who have malignant kidney tumours to report their experiences in the management of their malignant tumours so that more lessons would be learnt about further developments related to immunotherapy in kidney cancers as well as a global multi-centre related to immunotherapy in malignant kidney tumours should be established for the management of various cell types of primary and metastatic kidney cancers which would hopefully lead to the establishment of consensus opinions related to immunotherapy in the management of various cell types of malignant kidney tumours.
Acknowledgements to:
Medicina. For granting permission for reproduction of figures and contents of their Journal article under copyright: This is an open access article distributed under the Creative Commons Attribution Licence which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Case Reports Immunol and Hindawi for granting permission for reproduction of contents and figures of their journal article under copy right: Copyright: Copyright © 2018 Jawaher Ansari et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
J Med Case Reports for granting permission for reproduction of figures and contents of their journal article under copy right: Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
The author has no conflict of interest to declare (None).
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
