AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Elsa Hoti, Lausanne University, Faculty of biology and medicine, Lausanne, Switzerland.
Citation: Elsa Hoti, Roger Hullin, Matthias Kirsch, Frédéric Schütz, Piergiorgio Tozzi, (2023), How Donor Profile Affects the Outcome of Heart Transplant: A New Score to Predict Primary Graft Failure, J Thoracic Disease and Cardiothoracic Surgery, 4(5); DOI:10.31579/2693-2156/064
Copyright: © 2023, Elsa Hoti, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 September 2023 | Accepted: 12 September 2023 | Published: 21 November 2023
Keywords: heart transplantation; organ donor; primary graft failure; data base analysis
Aim: This study aimed to identify demographic and clinical parameters in donors that could predict the ischaemic time tolerated by the heart transplant in order to increase the number of heart transplantation performed in our centre by expanding the area of graft recruitment.
Methods: A single site retrospective study was conducted on 116 heart transplantations performed in our centre between 2013 and 2021. Multivariate logistic regression analyses were used to identify interactions between the different donor parameters.
Results: Sex, weight, height, total graft ischemic time were the donor parameters independently correlated with primary graft failure (p < 0.1). The logistic regression model included 11 variables, with an AUC of 0.81, this model appears to perform well in the prediction of primary graft failure in the recipient.
Conclusions: A predictive score of primary graft failure was created based on identified donors parameters that may help identify grafts with a higher tolerance to ischemia.
In Switzerland in 2021, 126 patients were placed on the waiting list for a heart transplant but only 33 were able to benefit from a transplantation based on the annual report of Swisstransplant. Recently, the number of patients on the waiting list has been constant and it is known that the longer the wait, the greater the risk that heart failure will negatively impact the functioning of other organs such as the kidneys [1]. Knowing that heart transplant is still the gold standart treatement for end stage heart failure, this mismatch between donors and receivers needs to be improved [2]. Moreover, we live in a time where cardiovascular diseases are the leading cause of death and the ageing of the population suggests that the needs for heart transplants are likely to increase [3]. Since the first heart transplantation performed by Barnard in 1967 [4], many advances have been made in organ preservation [5]. Thanks to all this discoveries the ischemic time that the myocardium can tolerate is now approximately four hours. During this time, the heart of the donor is flushed in-vivo with a cardioplegic solution and then stored at 4°C during the transport to the centre where it will be re-implanted into the receiver. Although this high potassium solution allows diastolic cardiac arrest by inducing membrane depolarisation, the induced calcium overload, myocardial ischemia and hypothermia result in time dependent injury to the heart. Therefore, the commonly accepted total ischemic time is 4 hours, thus limiting the distance at which heart grafts can be procured [4]. Although some studies have already looked at the impact of certain donor parameters (e.g. ABO group [6]) on receiver survival, there are still no guidelines for estimating the ischemic time that a graft can withstand. However, identifying biological and clinical parameters of the donor that would allow to predict the ischemic time that the graft can tolerate, could possibly reduce this mismatch between donors and receivers by increasing the area of graft recruitment. Grafts refused due to ischemia time exceeding 4 hours could be accepted if the donor meets the identified criteria. This could lead to an increase in the number of heart transplants per year and therefore reduce the number of patients who die while on the waiting list for a transplant by practising a more personalised medicine [5].
Study design
A single center retrospective study was conducted on heart transplants performed in our center between January 2013 and December 2021. After identifying the main relative knowledge of the subject by reviewin grelevant scientific publications. Clinical and biological parameters in the donors were selected and compared with the total ischemic time (cold + warm ischemic time corresponding to the implant time) that their graft underwent and with the outcomes in the recipients. This was to determine whether an association between the criteria identified in the donor and the ischemic time that the graft could tolerate existed. Given that the negative effects of longer graft ischemic time are mainly manifested in the early post-transplant period, the outcome was defined by whether or not Extra Corporeal Membrane Oxygenation (ECMO) was required following transplantation, allowing to determine indirectly the presence of a primary graft failure (PGF). Indeed, the marker used for the tolerance of the graft to ischaemia was primary graft failure. As primary graft failure occurs within 24 hours post-transplant and requires the use of ECMO for the cases of a severe presentation of the disease, the use of ECMO in the recipient was recorded only within 24 hours post-transplant. [7]
Data
After the acceptance of the project by the Ethics Commission of the Canton of Vaud (CER-VD 2022-00562), the data of the heart transplants performed in our center from January 2013 to December 2021 were collected. Including all adult donnors and receivers ( 18 years old) and excluding both donnors and receivers for whom a document attesting to a refusal existed (N = 116). The mean donnor age was 46 +/- 14.4 years, 64 (55%) were men. The data collected are presented in Table 1.
18 years old) and excluding both donnors and receivers for whom a document attesting to a refusal existed (N = 116). The mean donnor age was 46 +/- 14.4 years, 64 (55%) were men. The data collected are presented in Table 1.
| Donor variable | Definition |
| Age | |
| Gender | |
| BMI | |
| Weight | |
| Height | |
| Clinical parameters | |
| Ejection Fraction (EF) | As reported by organ procurement center |
| Blood type | A, B , AB, O |
| Medical history | |
| Diabetes | Positive diabetes history includes type 1 and type 2 with or without treatement. |
| Hypertension | As reported by organ procurement center |
| Malignancy | Defined positive if a history of tumor exists with a 5 year remission phase before the transplantation |
| Active smoker | Includes donnors who were active smokers |
| Biological parameters | |
| Troponins | |
| Creatin Kinase (CK) | |
| Creatinin | |
| Graft ischemic time | Cold + warm meaning the time interval between the application of aortic clamping during cardiac harvesting in the donor and reperfusion of the graft in the recipient |
| Recipient variable | Definition |
| ECMO | Yes/No |
Table 1: Collected data
Analysis were conducted using RStudio version 2021.09.2. First, an independant correlation between each donnor parameter and the use of ECMO in the recipient was investigated in order to evaluate if the association found in our data set are alligned with literature. Therefore boxplots were drawn for continuous values (age, weight, height, BMI, EF, creatinin, troponins, CK and total graft ischemic time). The association was tabulated for categorical values (gender, diabetes, hypertension, malignancy, active smoker and ABO group). For ease of analysis, the values in the tables have been converted to percentages. The continuous variables were transformed using a logarithmic scale to get a better representation for parameters with highly skewed data (troponins, CK, creatinin). T-tests determined wether a statistically significant difference existed between the ECMO and non-ECMO group. The data all followed a normal distribution except for the “age” variable.
At a second phase, multivariate logistic regression tests were performed to create a score that could predict the use of ECMO in the recipient. The parameters included in the second phase were all the relevant parameters found in previous research as good predictors of the tolerance to ischemia of the graft and parameters that had a significant independant correlation with use of ECMO in our data set. Finally, a model was created with the logistic regression test, trained on a fraction equal to 70% of our sample and then tested on the ramaining 30 %. Taking into account our sample size, spliting randomly in half our data set could not provide enough data to the model to train. The model performance was evaluated using ROC analysis and a score was created based on the coefficients of each parameter of the model.
Between 2013 and 2021, 116 patients underwent heart transplatation in our center and met our inclusion criteria. The mean donnor age was 46 +/- 14.4 years, 64 (55%) were men. 25% of recipients were on ECMO within 24 hours post-transplant, i.e. 29 recipients.
After performing the t-tests, the results with p ≤ 0.1 were considered significant. The median of age in both groups was around 50 years old although 75% of the donors of recipients who needed ECMO are above 40 years old (figure 1a). However, there was not a significant interaction between the age of the donor and the use of ECMO in the recipient (p = 0.20). The weight of the ECMO group is slightly higher with an outlier exceeding 140 kg. 50% of the values in the ECMO group are above 80 kg (figure 1b). Likewise, in general, donors in the ECMO group were taller with values ranging from 155 cm to almost 200 cm compared to the non-ECMO group where values ranged from 140 cm to 190 cm. In addition, the median height of the ECMO group was 175 cm compared to 170 cm for the non-ECMO group (figure 1c).These two last parameters were significatly correlated with ECMO use in the recipient (p = 0.06 and p = 0.09, respectively). No significant interaction was observed between the BMI of the donors and a PGF in the recipient (p = 0,50) and not for the ejection fraction either (p = 0.73).The BMIs in both groups were similar with a median at 25 kg/m2 and a single outlier in the ECMO group at more than 50 kg/m2 (figure 1d). The median of the ejection fractions of both groups was around 60% with a single outlier at 80% for the non-ECMO group (figure 1e). The analysis show the total graft ischemic time to have a significant interaction with the use of ECMO in the recipient (p = 0.06). In fact, for half of the patients who were under ECMO, the graft had undergone more than 160 minutes of ischemia with a maximum of 275 minutes. The median stood at 152 minutes for the non-ECMO group and the maximum was 252 minutes (figure 1f).
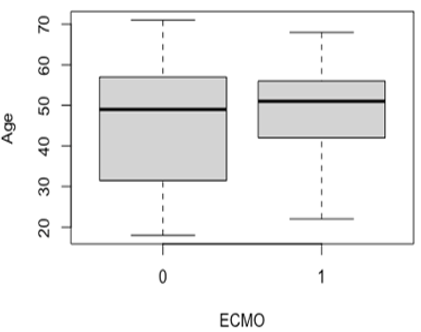
Figure 1a: Boxplot representing the independent association between the age of the donor and the use of ECMO in the recipient
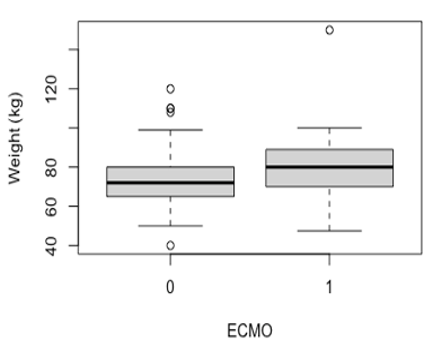
Figure 1b: Boxplot representing the independent association between the weight of the donor and the use of ECMO in the recipient
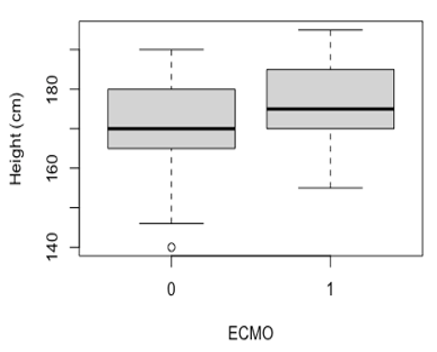
Figure 1c: Boxplot representing the independent association between the height of the donor and the use of ECMO in the recipient
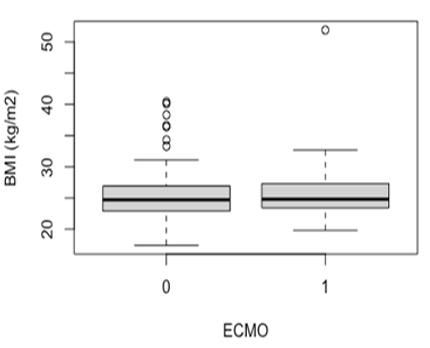
Figure 1d: Boxplot representing the independent association between the BMI of the donor and the use of ECMO in the recipient
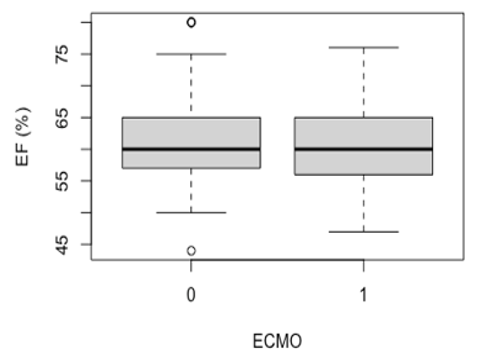
Figure 1e: Boxplot representing the independent association between the ejection fraction of the donor and the use of ECMO in the recipient
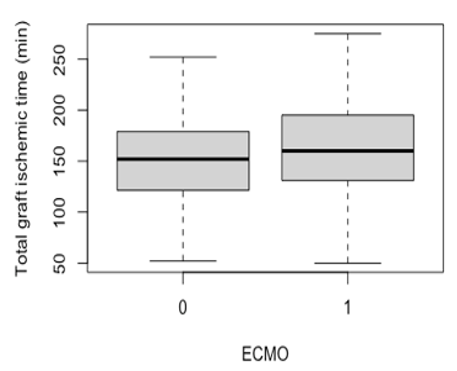
Figure 1f: Boxplot representing the independent association between the total graft ischemic time and the use of ECMO in the recipient
Box plots representing the independent association between creatinine, troponins, CK levels in the donor and ECMO use in the recipient are presented with numerical values (left box plots) and with logarithmic values (right box plots), the transformation of these values into logarithmic scale allows to better observe the distribution of the data. The creatinin levels in the non-ECMO group appears to be more spread with higher outliers. However, the median of both groups is close to 90 umol/l (figure 2a, 2b). Creatinin levels of the donors appears to not be correlated with an ECMO use in the recipient (p = 0,78) as well as troponins and CK levels (p > 0.5 for both parameters). Although the median troponins levels are similar in the 2 groups, maximum values are higher in the non-ECMO group (figure 2c, 2d). As for the CK level, the differences between the 2 groups are minimal except for an outlier which clearly stands out in the ECMO group at over 1000 microg/l (figure 2e, 2f).
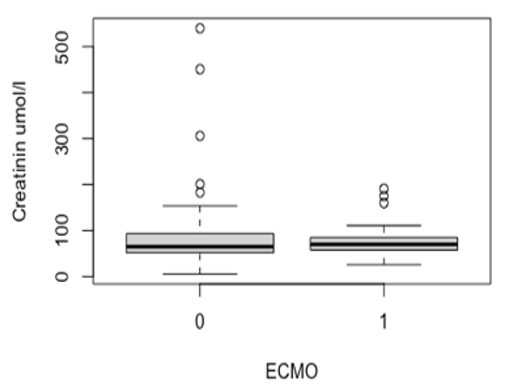
Figure 2a: Boxplot representing the independant correlation between the creatinin level of the donor and the use of ECMO in the recipient (numeric values)
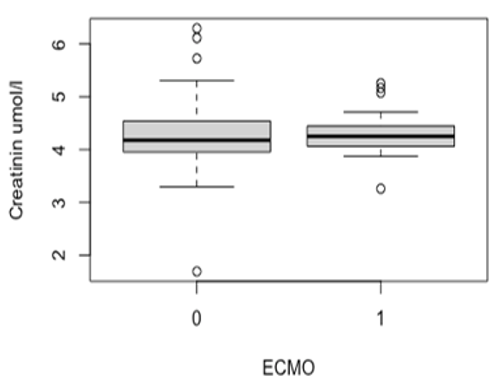
Figure 2b: Boxplot representing the independant correlation between the creatinin level of the donor and the use of ECMO in the recipient (logarithmic values)
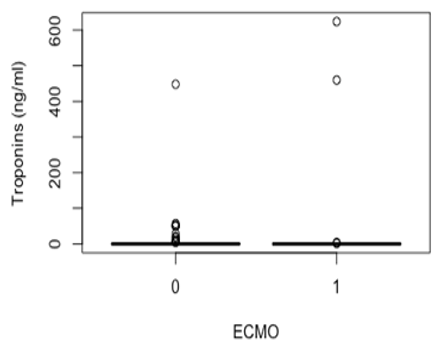
Figure 2c: Boxplot representing the independant correlation between the troponins level of the donor and the use of ECMO in the recipient (numeric values)
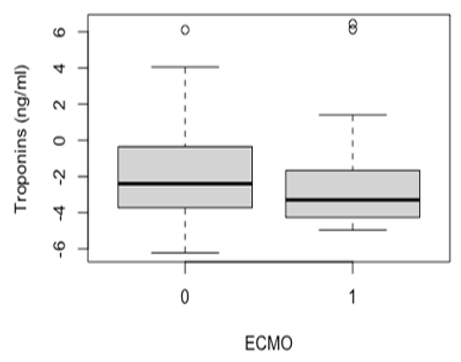
Figure 2d: Boxplot representing the independant correlation between the troponins level of the donor and the use of ECMO in the recipient (logarithmic values)
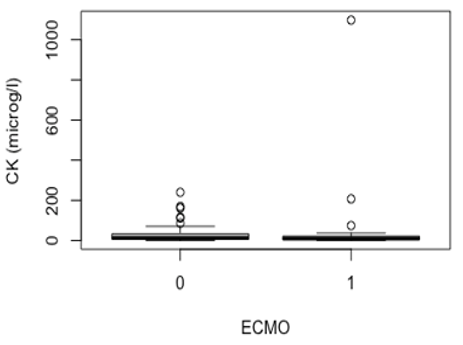
Figure 2e: Boxplot representing the independant correlation between the CK level of the donor and the use of ECMO in the recipient (numeric values)
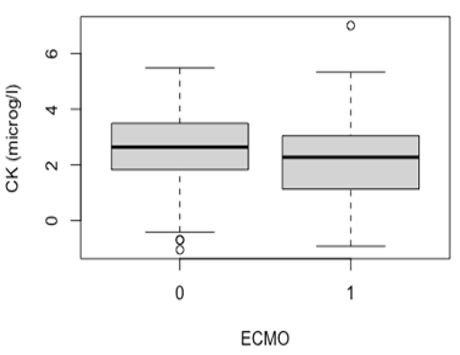
Figure 2f: Boxplot representing the independant correlation between the CK level of the donor and the use of ECMO in the recipient (logarithmic values)Categorical values
After tabulating the independent correlations between the categorical donor parameters and the occurrence of primary graft failure in the recipient, as well as for the continuous parameters, we assessed whether the difference between the 2 groups was significant (table 2). Male donors seem to be significantly more associated with an ECMO use in the recipient (p = 0.07). Although we observed higher proportions of PGF in recipients with a diabetic, hypertensive, active smoker and/or AB blood group donor, the differences between the 2 groups are not significant with p-values ranging from 0.22 to 0.52. The proportions being almost the same in both groups, shows that the history of malignancy in the donor does not seem to be correlated with the use of ECMO in the recipient.
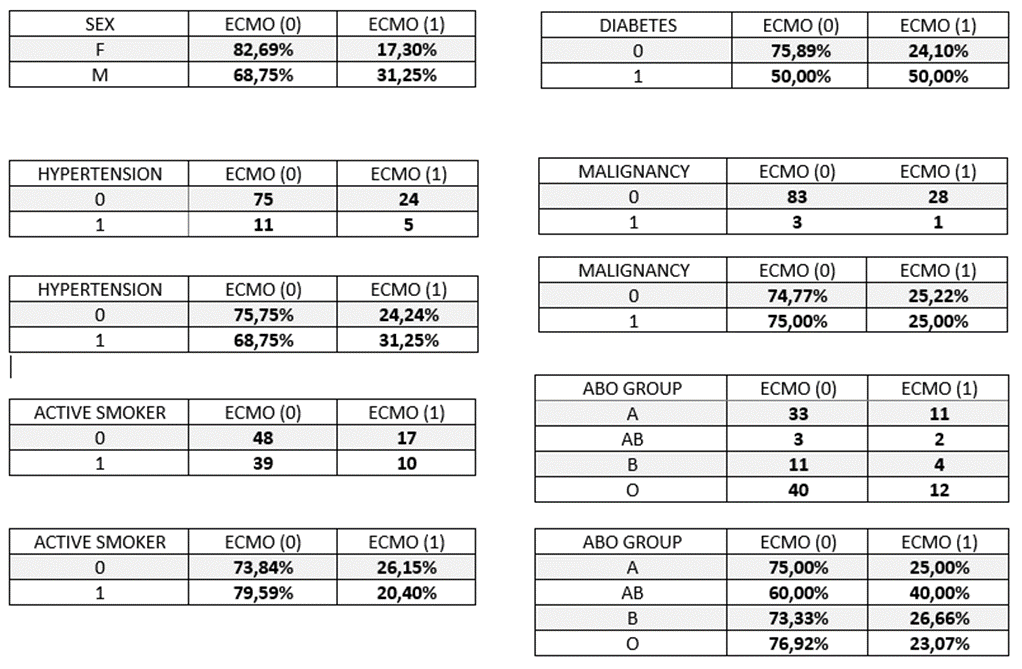
Table 2: The independant correlation between the categorical parameters of the donnor and the use of ECMO in the recipient
Multivariate analysis
In order to create a model based on which a score will be derived, multivariate logistic regression tests were performed. The first model included all donor parameters for which we a significant interaction was found with ECMO use in the recipient (weight, height, total graft ischemic time, gender) as well as donor age. The interaction between these parameters does not appear to play a role in the prediction of a primary graft failure in the recipient. The predictions of the model only slightly match the actual use of ECMO with an accuracy of 0.641 and this is confirmed by the ROC curve of the model, AUC = 0,68 (figure 3a and 3b).
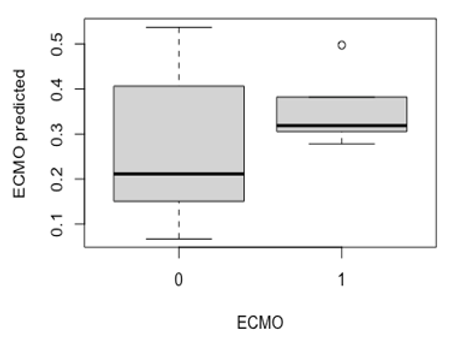
Figure 3a: Boxplot reprensenting the distribution of the predicted values of ECMO for each group with the first model
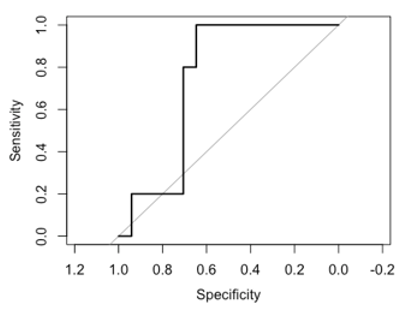
Figure 3b: ROC curve based on the predicted values of ECMO with the first model and the actual values of ECMO in our dataset
The second model included age, gender, total graft ischemic time, height, weight, BMI, EF, hypertension, malignancy, diabetes, troponins, creatinin and CK. With an accuracy of 0.719, this model seems to perform better in the prediction of ECMO use in the recipient. Indeed, as shown in the boxplot (figure 4a), not only the second model predicts more often ECMO in the recipient when it actually was used but is also better to predict when the recipient will not suffer from a primary graft failure as shown by the ROC curve, AUC = 0,81 (figure 4b). The specificity and the sensitivity of the model are respectly of 0,64 and 1.
Scoring system
Based on the ROC curve of the second model, an optimal threshold was calculated at 0.19. The coefficients of each parameter were extracted from the logistic regression model (table 3) which provides the weight of each parameter and allows to calculate a score that could predict the occurrence of PGF in the recipient.
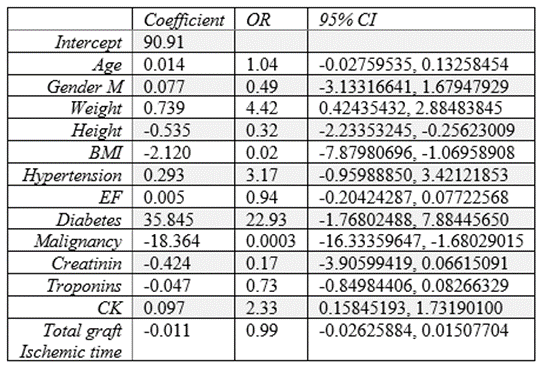
Table 3 : coefficients, OR and 95% CI of each variable of the logistic regression model
By multiplying each parameter of the donor by the corresponding coefficient and additionning all the products and the intercept, a value is obtained. This value is passed through a sigmoid function to obtain a probability between 0 and 1. If the result is under 0.19, the graft can be accepted even with a longer ischemic time with high reliability since the negative predictive value of the score is 100%. With a positive predictive value of 43.75%, if the score is greater than 0.19, the recipient has a 43.75% risk of suffering from PGF. For continuous paramters (age, weight, height, BMI, EF, creatinin, troponins, CK and total graft ischemic time), the value of the donor would be entered in the formula. For the binomial parameters, the coefficient would be multiplied by 1 or 0 wether the medical condition is present in the donor or not. With regard to the sex of the donor, the coefficient is multiplied by 1 if the donor is male and by 0 if the donor is female.
The formula for the score calculation :
x = 90.91 + (age * 0.014) + (sex * 0.077) + (weight * 0.739) + (height * -0.535) + (BMI * -2.120) + (hypertension * 0.293) + (EF * 0.005) + (diabetes * 35.845) + (malignancy * -18.364) + (creatinine * -0.424) + (troponins * -0.047) + (CK * 0.097) + (total graft ischemic time*-0.011) prob = 1 / (1 + exp(-x))
Graft allocation is a complex process faced by a heart transplant clinician. Many parameters have to be taken into account both in the donor (organ function, circumstances of death, medical history) and the recipient. It is therefore quite often difficult to predict the interaction of these different factors and the impact on post-transplant outcome. The current landscape of heart transplantation makes decision making even more complicated. Indeed, with the current demographic shift towards an older population and advances in heart failure management, the number of patients reaching an end stage disease is increasing [8]. However, this increase in patients on the waiting list is not accompanied by an increase in the number of donors. Faced with this discrepancy, different solutions have been proposed. One of them is to adopt extended criteria in organ allocation by accepting transplants from older donors, diabetics or with transmissible diseases [9]. Other teams suggested a scoring system that could predict the perceived risk of graft failure [10,11]. Although there are no standardised guidelines to help the clinician decide whether to accept or reject a graft and this is reflected in organ acceptance rates that vary from one institution to another [12], certain clinical and demographic parameters of the donor are known to affect the outcome in the recipient. One of the major parameters commonly accepted to affect post-transplant mortality in the recipient is the age of the donor. Older age (>40 or >50 years old depending on the study) is associated with a decrease in recipient survival [7, 10, 13, 14, 15]. In our study, the age of the donor does not seem to have a significant interaction with the use of ECMO in the recipient, taking into account our relatively small sample size, the results with a p-value ≤ 0.1 were considered significant. However, some of the studies previously mentioned look at the impact on medium to long term survival (3 months to 5 years) and not directly on primary graft failure which may explain the difference in results obtained, due to a different timing of occurrence [16]. In view of the scientific consensus on this parameter, the age was nevertheless included in our model. The impact of the sex of the donor on the outcome in the recipient is a source of disagreement in the literature. With fairly equal proportions of both sexes in our sample, the association of male sex with ECMO use in the recipient can be considered reliable. On the contrary, in the studies of Kuzemchak MD and al. and Sorabella RA and al., female sex seems to be associated with complications in the recipient in the short term [2,13]. An other study suggested that the mismatch of the sex between the donnor and the recipient depending on the age of the donnor had an impact on the survival of the recipient. Female sex donor was associated with worse long term survival in male recipients when they received a heart from an older donor (>45 years old) [17]. The study of Stehlik J and al. shows that history of hypertension and diabetes mellitus in the donor compromises the survival of the recipient when the heart came from a male donor [12]. The interactions between the different donor parameters mentioned above could explain our results. History of diabetes mellitus and hypertension in the donor is commonly associated with worse survival in the recipient as mentioned also in the report-2020 of the the International Society for Heart and Lung Transplantation [14]. No significant interaction was observed between the presence of these medical conditions in the donor and the developpement of a PGF in the recipient, however, as shown in table 2, the proportions of donors in our sample presenting a history of diabetes mellitus or hypertension are low.
As these diseases are cardio-vascular risk factors, this could lead to a more frequent refusal of hearts from donors with diabetes and/or hypertension, thus explaining the low prevalence in our sample. An other cardio-vascular risk factor is smoking and the smoking history of the donor is also considered in the decision making for the use of a graft [14, 18]. In our study, only the prevalence of active smoker in our sample was accessible, which doesn’t provide information about the history of tobacco use of the donor or the quantity smoked, however these factors are known to play an important role [19]. Therefore, this parameter was considered unreliable. As well as for hypertension and diabetes mellitus, the proportion of donors with malignancy history in our sample is very low (table 2). The severity of the disease could explain the low number of people who are able to fulfil the conditions for being a donor, including being in remission for at least a period of 5 years [20]. The results found for ABO group weren’t significant because of the low number of patients in the AB group. This is compatible with the distribution of blood groups in the general population in Switzerland. Our sample contained 38% of patients with A group, 13% of B, 4% of AB and 45% of O. The distribution in the general population is of 45% of group A, 9% of group B, 5% of AB and 41% of O [21]. This small difference in proportions in our sample compared to the general Swiss population can be explained by the fact that not all hearts come from Swiss centres. Moreover, hearts from O-donors need only ABO-compatible matching and not ABO-identical matching [22] which might explain the higher proportion of O-donors in our sample. Nevertheless, in the literature, O donors appear to be associated with poorer recipient outcomes [6,23]. Size mismatch, BMI, weight, height are well studied and as mentioned in the 2019 report of the International Society of Heart and Lung Transplanation, BMI is not an optimal metric to assess the size match between the donor and the recipient [24]. Although overweight and obesity are associated with cardiovascular risk, it is also known that a high BMI is not necessarily a manifestation of one of these medical conditions. This could explain why no significant difference in BMI was found between the 2 groups in our study. On the contrary, a higher weight and height in the donor seems to be associated with PGF in the recipient. The weight of male recipients shouldn’t be greater than 30 percentage above the weight of the donor and for female recipients the threshold is at 20 percentage according to the recommandations of the International Society of Heart and Lung Transplanation [25]. However, body weight is not well correlated with heart weight neither for women nor for men [26] which may explain our results. In the search for good predictors of outcome in the recipient, biological parameters were also investigated, the transformation of these values into logarithmic scale allows to better observe the distribution of the data. The higher level of troponins found in the non-ECMO group may be the result of the myocardiac suffering as well as any skeletal muscle suffering [27], therefore troponins levels in the donor were not considered to be good predictors of the occurrence of PGF in the recipient. The literature is also sceptical about this parameter with contradictory studies [28,29]. Knowing the relationship between kidney injury and heart failure [30], it could be assumed that the donor's creatinine level is an indirect reflection of their heart health. However, the creatinin levels are similar in both groups, this parameter appears to not be correlated with an ECMO use in the recipient. Indeed, some studies show that creatinin alone is not a good predictor of the outcome, they identified the ratio BUN (Blood Urea Nitrogen) / creatinin to be more representative of the cardiac performance [31]. The final biological parameter analysed was CK level and similarly to troponins level, a slightly higher level of CK was found in the non-ECMO group. This could be explained by the fact that, as with troponins, CKs are not specific to myocardial tissue and can therefore also be a manifestation of skeletal muscle injury or brain damage [32]. And finally, a significant interaction was found between longer total graft ischemic time and the occurrence of PGF in the recipient. As mentioned previously, a total graft ischemic time of more than 4 hours is associated with a worse survival in the recipient [7,13,14].
It is important to mention that genetic studies have also been carried out in the area of tolerance to graft ischaemia. The role of the anti-aging gene Sirtuin 1 for example is critical to heart function and Sirtuin downregulation is associated with endothelial dysfunction and cardiovascular disease. Sirtuin 1 activators versus inhibitors may determine the success of heart transplantation [33-38].
As other teams have done before us, we created a score based on our second model and applicable to the data in our center. The score developped by Eric S Weiss and al was predictive for 30-day mortality with an OR = 0.11 and includes 4 parameters : ischemic time, donor age, race mismatching, and blood urea nitrogen (BUN)/creatinine ratio [11]. Although this score is easier to use and can help in the allocation of donor hearts, we believe that our score brings accuracy in predicting the outcome in the recipient. Firstly, by entering the values of the donor variables directly into the formula instead of assigning points by value range. Secondly, by taking into account more parameters that reflect the donor's cardiac performance. Finally, to ensure the safety of accepting grafts with longer ischemic times, a threshold of 0.19 was fixed in the predictive score. This threshold allowed to reach a negative predictive value of 100% for the prediction of the occurrence of a PGF in the recipient. This is based on our data only, therefore, studies with larger sample sizes and data from other centres would be needed. However, it was ensured that most recipients who were predicted to not require ECMO, will not experience complications such as a PGF by setting the threshold that would minimise the occurrence of false negatives.
This study was conducted in order to consider a possible increase in the number of heart transplants performed in our centre by increasing the area of graft recruitment. Therefore, the score was developed with data from heart transplants performed in our center and may not be applicable in other centres or countries, especially as the sample size was limited to the experience of our centre. Missing data is another limitation inherent to databases such as SOAS, it cannot be excluded that these data would have influenced the results. Due to our sample size, 70% of our data set was used to allow robust training of the model. This implies that our model was tested on the remaining 30%. Therefore, it would be necessary to collect new data in order to not only test the model on a larger sample but also to provide statistically stronger results. And finally, the aim of the study was to identify donor parameters that could affect the time of ischaemia tolerated by the graft by overlooking recipient parameters that could influence post-transplant outcome. It would also be relevant to study factors in the recipient that might predict tolerance to a graft with prolonged ischaemic time.
In this study, demographic and clinical parameters were identified in donors that could predict the ischaemic time tolerated by the heart transplant. The aim was to create a score that would allow the acceptance of transplants from centres further away from ours. The clinicians in charge of heart transplants could easily input donor values in the score calculation formulated in a user-friendly tool such as Excel and obtain a result ranging from 0 to 1. The score threshold being predetermined at 0.19. Although our score is an aid to decision making, it is based on data from heart transplants performed at our centre, further studies are needed before its potential application on a larger scale.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
