AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Yadsan Devabalan, Federa Department of Otolaryngology, University College Hospital, London
Citation: Yadsan Devabalan, Zaid Awad, Neil Tolley (2022) How Can We Best Manage Patients With Oligometastatic Disease In Head And Neck Cancer? Journal of Clinical Otorhinolaryngology 4(2); DOI: 10.31579/2692-9562/043
Copyright: © 2022, Yadsan Devabalan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 December 2021 | Accepted: 18 December 2021 | Published: 26 February 2022
Keywords: head and neck neoplasms, neoplasm metastasis
Background: Oligometastatic disease in head and neck cancer is a new entity that is beginning to gather significant attention. It is a concept that is defined as <5 lesions with control of the primary lesion.
Methods: In this paper, we explore the literature for the presentation and management of patients presenting with oligometastatic disease in the head and neck from non-head and neck primaries.
Results: The most common infraclavicular primary tumours to metastasise to the head and neck are breast, lung and renal carcinomas. Management of these oligometastatic lesions is currently very variable and surgery and/or ablative therapies can in fact be associated with good survival outcomes or locoregional control compared to patients with widespread metastatic disease.
Conclusion: The recommendations in this paper will help towards establishing clear guidelines in the future for surgical and ablative therapies for these patients.
Oligometastasis was a term first proposed by Hellman and Weichselbaum in 1995 to identify a group of patients with limited ‘few’ metastatic deposits (1). They attempted to broadly fit this group of patients in between those with localised lesions, with potentially good prognosis, and those with widespread metastatic disease, with typically very poor prognosis. Over time, this definition has been debated and refined, and the current generally accepted definition of oligometastatic disease refers to <5>
The importance of this concept, and why its treatment has generated significant research recently, is because of the potentially curative intent of malignancy for this group of patients. Traditionally, patients with metastatic disease are associated with poor prognosis and have treatment options limited to systemic chemotherapy and molecular targeted therapy to improve or prolong quality of life. It has been shown that metastatic disease burden is negatively correlated to prognosis in many cancers (3, 4), so it stands to reason that patients with oligometastases have better survival outcomes compared to patients with widely-disseminated metastatic disease. Research has focused on both detection and treatment modalities for these patients. Detection modalities including CT, MRI, PET-CT and bone scintigraphy scans have been explored in relation to timing, detection rates and histological subtypes (5). Treatment modalities have centred on locally ablative therapies such as stereotactic body radiotherapy and radiofrequency ablation (6) to curative surgical resections. This shift in thinking has allowed patients to greatly benefit, but has also given clinicians a potential new problem with new treatment options without robust guidelines present.
Before we explore the potential benefits of treatment an individual with oligometastatic disease, it is important to explore the biology behind its development. Cancer development and pathogenicity had always been thought of in a traditional ‘seed and soil’ hypothesis (7) whereby 2 distinct states existed at time of diagnosis. The patient either had localised disease, or systemic disease with positive lymph nodes and a high probability of metastasis. These two groups of patients were seen as entirely distinct entities, with different treatment options offered and subsequent survival outcomes. It wasn’t until the aforementioned Hellman and Weichselbaum proposed their oligometastatic theory that the progression of cancer was thought to be multi-stepped. It was proposed that a cancer’s full metastatic potential hadn’t been reached yet, but was limited to certain receptive sites of the body. Four factors have been found to favour an oligometastatic state over a widespread polymetastatic state: (5)
Additionally, microRNA sampling and detection has identified certain clustered microRNA patterns in patients with polymetastatic disease compared to oligometastatic disease. For example, in breast cancer, clusters of miR-200c were found in the metastatic population, and subsequently in mouse models this was able to convert oligometastatic models to polymetastatic models. (8) There is sufficient evidence to class oligometastatic disease as a separate entity from metastatic disease both on a genomic and a phenotypic level. As such, further research and a better understanding of the molecular and biological frameworks involved in oligometastatic disease development and progression is needed to allow more evolved and robust treatment options to be developed.
Colorectal, prostate, lung, renal, sarcoma and renal cancers have all been found to predispose to an oligometastatic state. Radiotherapy and surgical managements remain the primary focus of research for treatment options for these patients. Metastasectomy is a procedure that involves surgical resection of isolated metastases, and is one that been increasing in incidence and in efficacy over the last 2 decades. (9) Colorectal, lung, breast cancer and melanoma are the most common indications for metastasectomy. Resection of colorectal liver metastases is well known and has led to increased long-term survival benefit in these patients, with 5-year survival rates up to 50% and 3-year local recurrence free survival rates up to 95% (10). Additionally, pulmonary metastasectomy has been increasing in practice over the last decade, and colorectal metastases in the lung remain its primary indication. However, despite its widespread use there remains a lack of sufficient evidence advocating its benefits. Its use is based on retrospective case series and follow-up studies (11). Of note, there has only been one randomised controlled trial, PulMiCC (12), but this was stopped due to low recruitment. However, it did report an increased estimated survival of 9% over the control group. Evidence-based surgical practice appears not to have been as thorough with this particular group of patients, perhaps due to the fact that these oligometastatic patients would traditionally have been given palliation treatments rather than those aiming for locoregional control. Thomford et al (13) first proposed the Thomford criteria for selecting metastatic patients to undergo surgical treatment, and over the years it has been refined. The generally accepted consensus, for patients with pulmonary metastases at least is: i) controlled primary tumour ii) no extrapulmonary lesions. By extension, these fit the criteria for oligometastatic patients, and significant research on surgical resections need to be explored both in multiple other primary cancers and in resections in other locations.
Radiotherapy has largely focused on localised ablation therapies for oligometastatic patients. One of these methods is stereotactic body radiotherapy (SBRT), also known as stereotactic ablative radiotherapy (SABR), which involves using external beam radiotherapy to target sites with high-dose radiation while sparing the surrounding healthy tissue. Again, use of this has largely focused on colorectal cancers, with retrospective studies showing a 2-year local control rate of greater than 80% for liver metastases in colorectal cancer (10), without the morbidity associated with surgery. In breast cancer, 2-year progression free survival and 2-year local control rates of 97% have been achieved in SBRT trials with oligometastatic patients. (8) In lung cancer, many phase II and III RCTs are currently in progress exploring a combination of metastasectomy vs SBRT vs systemic therapy (14). Some of these trials have already been stopped or modified for showing a significant improvement in progression-free survival in SBRT over systemic therapy in oligometastatic patients. Clearly, this field of therapy hold significant interest and could lead to many solid evidence-based recommendations for the treatment of oligometastatic patients based on site and primary tumour.
Within head and neck cancer, research into oligometastatic disease has remained fairly less extensive than some of the cancers discussed above. Cancers of this group are comprised of many different tumours within the head and neck region, with the most common being of these five subtypes:
Of these, the most predominant histology is squamous cell carcinomas (SCCHN). It is the sixth most common malignancy in the world, and up to 40% of patients may have metastases during their surveillance (15, 16). Analysis of the national cancer database revealed that metastatic patients who received both systemic therapy and high-intensity local therapy had a 13% improvement in 2-year survival over those with systemic therapy alone (17). Similarly, a retrospective study in Germany revealed a significant survival benefit in oligometastatic patients who received local therapy over those matched controls who didn’t, irrespective of site of the metastases (18). Regarding metastasectomy, in HNSCC patient, pulmonary resection for limited lung metastatic has yielded 5-year survival rates of 59%, which is similar to those with non-metastatic disease (19). A recent RCT called SABR-COMET (SABR Therapy for the comprehensive treatment of oligometastatic tumours) (20) evaluated the use of SABR/SBRT on oligometastatic patients, including HNSCC patients. The HNSCC cohort reported a 5-year survival overall survival of 42%, which is significantly higher than those undergoing no treatment and similar to those undergoing metastasectomy.
Despite these promising signs, the retrospective nature of these studies needs to be taken into context, and more data from RCTs and clinical trials will provide stronger evidence to guide future management. In particular the heterogenic nature of head and neck cancers will make this difficult, and a deeper analysis into each subtype is required.
Metastatic disease to the head and neck from non-head and neck primaries is infrequent. Less than 1% of all head and neck cancers has been estimated to be attributable to infraclavicular primary malignancies (21). Oligometastatic disease to the head and neck, in fact, remains far more infrequent than this. 10 years ago, Barnes et al (22) identified lung, breast, kidney and skin (melanoma) to be the most common primary tumours. Even at this time, solitary metastases were found to have unexpectedly good prognosis. To date, there remains no large review in literature exploring oligometastatic disease to the head and neck, and its impact on survival and treatment options.
Due to the increased recognition of oligometastatic disease and the potential curative benefit, or significantly improved survival benefit, therapeutic options for these patients are being explored. As such, there is an increasing number of patients presenting with metastases in the head and neck area with primaries elsewhere. This poses a clinical challenge for many ENT surgeons, clinical oncologists and radiologists.
There remains a dearth of high-level evidence for these groups of patients, so it is essential to explore what is currently present in literature both in terms of the primary tumour and of the metastatic location in the head and neck to best guide future management.
A literature search was performed on English Medline between 1995 until 2020 on the following key words or combinations:
Oligometstat*, head and neck, single/isolated/solitary metast*
Articles only from 1995 onwards were selected because this is the date this term was first proposed by Hellman and Weichselbaum. Retrospective and prospective studies were included, along with case series and case reports. Squamous cell carcinomas were excluded.
The results were then subdivided into the nature of the primary tumour. Only the most common cancers to the head and neck were selected:
Breast, renal/kidney, lung.
Skin (BCC/SCC/melanoma), colorectal and ovarian were also explored, but not included in this review due to very few numbers.
Due to the heterogenous nature of head and neck cancers, these results were further split up into location with the head and neck region.
Breast cancer is the most common cancer in women worldwide. 4-6% of women with breast cancer initially present with distant metastases at the time of diagnosis (8, 23), and the majority of mortality in these patients is attributed to distant metastases or recurrence with a 5-year survival of 26%. The rate of recurrence at distant sites is very high, with 20-30% in literature (24). The most common subtype is invasive ductal carcinoma, compromising up to 80% of all breast cancers. Breast cancer commonly metastasise to the lungs, bones, brain and liver.
Spread to the head and neck is rare, but has been identified in literature with multiple case series and reports. In fact, breast carcinoma is one of the most common tumours to metastasise to the head and neck, and has been shown to comprise up to 15-20% of all metastases in this region (25). Table 1 has been collated to show all the identified reports in literature, since 1995, with oligometastases to the head and neck region from a primary breast tumour. Studies with significant missing information for the chosen columns were excluded.
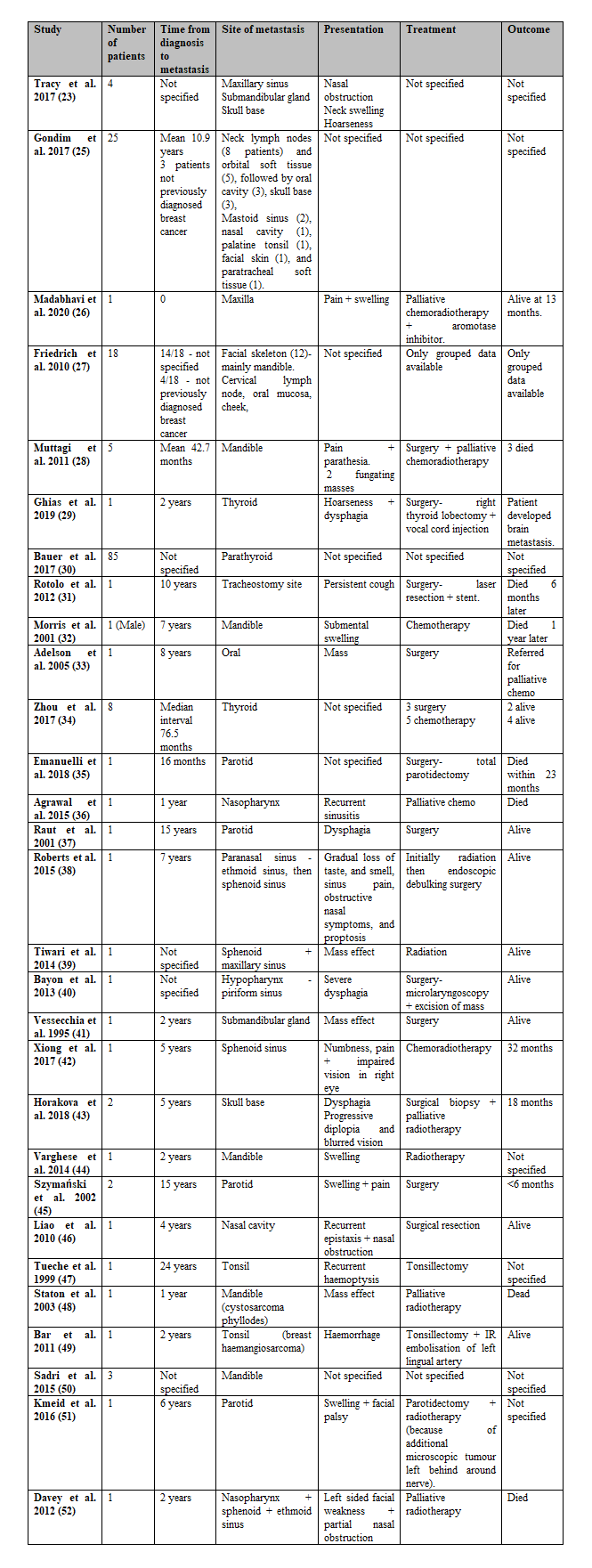
It is already well established that breast carcinoma has a predilection for bony metastases, the second most common site after the lungs. Within the head and neck region, this translates to the mandible and maxilla being the most common site, a finding that is supported by table 1. In fact, Hirshberg et al (60) found in a large retrospective study that up to 40% of female metastatic lesions to the jaw were breast metastases to the mandible, and up to 20% overall. However, interestingly, breast cancer metastases have been reported in virtually all of the subsites of the head and neck. Salivary glands, in particular parotid, was relatively common in table 1, as well as paranasal sinuses.
There are different proposed mechanisms for this spread:
This is a low-pressure valveless network of veins connecting the deep pelvic veins and the thoracic veins (intercostal veins, vena cava and azygous system) to the internal vertebral venous plexus. Therefore, blood can be diverted away from the caval venous system and can go into this valveless system. This provides a direct route for breast cancer cells (and other thoracic, abdominal and pelvic) tumours to spread directly into the head and neck region, bypassing the other sites of metastases (61). Oligometastatic disease, in the form of solitary lesions within the head and neck, can therefore develop from breast carcinomas.
Another possibility for oligometastatic disease to the head and neck is via a direct haematogenous route. Breast tumour cells can directly extend into the caval system and into the subsequent head and neck arterial system. To reach the paranasal sinuses, the cells can travel up to the pterygoid plexus and cavernous sinus. This in particular explains why the maxillary sinus was the most common site out of the paranasal sinuses because they are very highly vascularised through branches of the external carotid which communicate with the pterygoid plexus. It has also been hypothesised that the Valsalva manoeuvre or increased intrathoracic pressure may help push the tumour emboli through the pterygoid plexus into the paranasal sinuses (62).
Another route involves tumour emboli from regional lymph nodes flowing into the thoracic duct. They are then able to reach the head and neck through retrograde flow via intercostal, mediastinal or supraclavicular lymph vessels.
These different mechanisms for oligometastatic disease can create avenues for different treatment options by targeting isolated head and neck metastases.
Strikingly, in the cases identified in literature, there appears to be quite a large time interval between the primary breast cancer diagnosis and detection of the head and neck lesion. The largest such lag identified was 24 years (47), but the mean reported time in literature appears to be 10-11 years. It is already established that in breast cancer oestrogen and progesterone receptor positivity and human epidermal growth factor 2 (HER2) positivity are very strong risk factors for local or distant recurrence after 5 years (63). Clearly, this presents a problem because it implies that despite control of the primary tumour, there is still a chance for oligometastatic recurrence in other sites. This raises new questions of regular active surveillance within the head and neck region for patients with previously thought to be controlled/remitted breast carcinomas, particularly for those with strong risk factors for distant recurrence.
Interestingly, there were at least 7 identified cases in table 1, where the head and neck lesions were the first diagnostic specimen of breast carcinoma. Clearly this presents a challenge to head and neck pathologists because they have to be aware of breast carcinomas in this region as the initial presenting lesion. Special immunohistochemical stains, not routinely tested in head and neck specimens, such as pankeratin, mammaglobin, GATA binding protein 3, erbB-2 (61) as well as receptors for oestrogen and progesterone can help histopathologists identify oligometastases of breast origin.
a.Management options:
There is no clear guidance for the treatment of oligometastatic breast carcinoma in the head and neck. As evidenced in table 1, the treatment options varied immensely with very different survival outcomes. Treatment options varied particularly due to the site of the lesion. Treatment options fell into one of 3 arms for these groups of patients: chemotherapy, radiotherapy and surgery.
Chemotherapy, for this subset of patients, tended to be palliative, and in fact survival outcomes were not great. Due to the sparsity of this group, it is difficult to extrapolate any meaningful conclusions about the effective of chemotherapy for this subset over metastatic breast cancer patients. It is worth conducting large scale retrospective studies comparing the survival outcomes of both groups to guide future chemotherapy use in oligometastatic breast cancer patients.
Biological agents are another avenue that can be explored, particularly with anti-VEGF treatments such as Bevacizumab having shown significant progression free survival and objective response rates when used in combination with chemotherapy. This is a treatment option worth exploring in oligometastatic breast carcinoma to the head and neck.
Radiotherapy has also tended to be preferred as a palliative option in these patients thus far. Stereotactic body radiotherapy (SBRT) has been explored in breast cancer patients, and studies have shown a 74% overall 2 year survival (8). In fact, bone metastases were found to be particularly sensitive to SBRT, with one study reporting no rates of recurrence and no grade 3 toxicity in bone compared to 10/68 lesions recurring at other sites. Mandible and maxilla breast metastases may be particularly amenable to SBRT, and RCTs involving this or comparing SBRT to surgery seems the next logical step.
The benefits of surgery in liver metastasectomy and pulmonary metastasectomy have already been discussed. Within the head and neck, curative resections were performed for many patients identified in table 1. Particularly with oligometastatic disease to the thyroid, parathyroid and major salivary glands, curative resections are a treatment option. The patients that had good survival outcomes lacked any other significant disease burden, and hence fit the oligometastatic mould. Oligometastatic disease to the paranasal space is more contentious. Palliative surgery is not an overly familiar concept. Endoscopic sinus surgery in this regard is a low morbidity-associated operation that has been shown to significantly improve patient comfort by reducing proptosis and sinonasal complaints from oligometastatic disease to the sinuses (38). However, there are very few indications for it being curative, even in the oligometastatic setting, possibly due to the tumour disease burden present to breach into the pterygoid plexus and into the paranasal sinuses.
Tabaee et al (64) were able to take one further step and establish criteria for palliative surgery in their group of patients.
This is a criteria that ENT surgeons can adapt for patients with oligometastatic disease, as a significant proportion of them will be fit patients that can survive anaesthesia, and so surgical options should be explored despite there being a lack of understanding of cure. Of course, this is a decision that requires significant input from the rest of the multi-disciplinary team.
Lung cancer is currently the second most common cancer worldwide, and the leading cause of cancer-related deaths in both men and women (65). It is responsible for 1.3 million deaths worldwide every year. It currently has a 10-year survival rate of 10% in the UK (66). The most common histological subtype is non-small cell carcinoma, which compromise of squamous cell, adenocarcinoma and large cell lung cancer. Small cell carcinomas make up the remaining 15-20% of lung cancers, and are generally associated with the most metastatic potential and worst survival outcomes. In fact, the majority of small cell carcinomas have metastatic disease at the time of initial presentation (67) . Lung cancers are also prone to paraneoplastic syndromes, which increase patient morbidity and mortality.
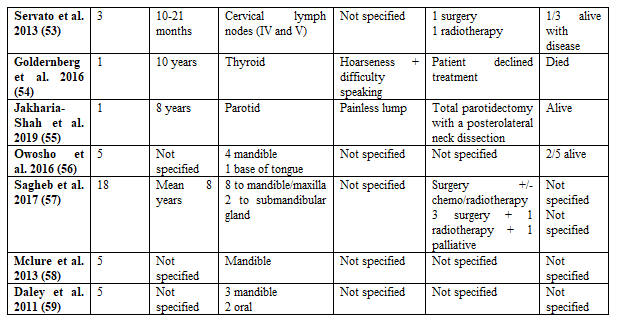
Lung cancer has a tendency to metastasise to the liver, brain, bones and adrenal glands. Small cell and adenocarcinomas tend to metastasise to the brain preferentially, while liver metastases almost never arise from adenocarcinomas exclusively (68). Lung cancer oligometastatic disease to the head and neck is rare but has been reported in literature. However, it remains the second most common after breast oligometastatic disease (69). Table 2 has been collated to show all the identified reports in literature, since 1995, with oligometastases to the head and neck region from a primary lung tumour. Studies with significant missing information for the chosen columns were excluded. It is also worth noting that a lot of the lung cancer patients, in particular small cell carcinoma, had widespread disseminated metastatic disease at presentation and so were excluded.
As evidenced in table 2, a significant proportion of these patients had undiagnosed primary lung carcinomas at their time of presentation. Synchronous metastasis are generally those defined as presenting within 6 months of the initial lesion, while metachronous lesions are defined as greater than 6 months. Lung oligometastases to the head and neck tend to favour a synchronous nature whilst breast tended to be metachronous with a relatively long time interval. In fact, even in histologies other than small cell carcinoma, the head and neck lesion was the first presenting lesion of the primary lung carcinoma. This presents a challenge for clinicians because it is essential to investigate for lung primaries with appropriate immunostaining and imaging as a part of staging, and there have been reports of lung metastases being misdiagnosed as primary head and neck tumours, especially in small cell and squamous cell carcinomas (85, 86).
Unlike for breast cancer, Batson’s plexus, which traditionally bypasses the lung is therefore not thought to be involved in the spread of lung cancer to the head and neck region. The highly vascularised microenvironment of the lungs makes it very easy for distant spread, especially with central lesions. The exact nature of this spread is not clearly defined and is believed to involve the major head and neck vessels en route to brain metastases.
The lymphatic route is thought to be of relevance in lung cancer due to pattern of distribution of oligometastatic sites, with the parotid gland and tonsils being very common. The concept of retrograde lymphatic flow to the head and neck is one that is explored in literature (68, 76, 78). It suggests that as a result of involvement of cervical lymph nodes, there is a higher down-stream pressure in the lymph vessels which then causes an inversion of flow. There is usually a mechanism to inhibit retrograde flow involving bi-leaflet vales but their function becomes defective as a result of tumour cell adhesion. This is particularly the mechanism that has been described for the palatine tonsils as they lack afferent lymphatic vessels. In combination with this, is pagetoid spread, which is the concept of invasion of the upper epidermis from below. This was noted by Tajima et al (76) in microscopic findings, and suggests that there does not need for there to be direct continuity with the epithelium of the primary tumour. This could allow even small pulmonary adenocarcinoma to metastasise to the cervical lymph nodes, and then subsequently onto the palatine tonsils.
Another theory proposed for the spread of oligometastatic disease to the head and neck, unique to lung cancer is direct implantation. It is known that metastases prefer sites of trauma, and lung cancer patients undergo bronchoscopic procedures either for diagnostic purposes with biopsies or interventional therapeutic purposes with debulking. There is a risk of damage particularly to the oropharynx and the tonsils, and this has been reported in literature (68, 74) with patients developing tonsillar metastases after rigid bronchoscopies. In fact, this has been shown in other conditions too, particularly with port-site metastases secondary to instruments in laparoscopic surgery and percutaneous endoscopic gastrostomy sites. These isolated lesions tend to have good survival outcomes after surgical resections.
Survival outcomes in table 2 for lung oligometastatic disease to the head and neck tended to be poorer than for primary breast carcinomas. This is in a large part due to the fact that significantly more patients presented with the head and neck metastasis as their presenting lesion with an as of yet undiagnosed primary lung carcinoma. Despite not having widespread disseminated metastatic disease at time of presentation, their primary had most likely remained untreated for a prolonged length of time. Treatment options varied in the literature depending on site of the lesion and on the primary histology.
Small cell carcinomas had the worst survival outcomes. Small cell oligometastatic disease to the parotids had a survival life expectancy of less than 10 months (70), while mandible oligometastases had a mean survival of 7-16.6 months (72). Patients with metastases of small cell origin had chemotherapy regimes due to the sensitivity of the primary small cell carcinoma in the lung to chemotherapy. However, despite this, the majority of patients received palliative regimes and had very poor survival outcomes. Combination with radiotherapy yielded marginally better results, and in fact Wong et al (75) proposed solitary nasopharyngeal metastases from primary lung tumour to be a separate entity entirely. This form of tumour responded preferentially well to radiotherapy despite an advanced stage of primary lung cancer, and the patient remained disease free for over 10 years. Clearly, further research is needed on palliative chemoradiotherapy regimes in patients with advanced lung primaries and oligometastatic disease to best optimise patient comfort and provide an improvement to quality of life as well as possible overall survival.
Newer biological therapies have also been tried in primary lung cancer and metastatic disease. Molecular profiling studies have allowed the identification of many genomic alterations and oncogenes that are histology specific and potential therapeutic targets. In adenocarcinoma particularly, many exist and one such target is the EGFR (epidermal growth factor receptor) which exhibits tyrosine kinase activity. Hence this can be inhibited with EGFR-tyrosine kinase inhibitors, and large scale RCTs have shown higher response rates and longer progression free survival compared to platinum-based chemotherapy (87). This finding has in fact been translated into oligometastatic disease too, and both Chen et al (71) and Kim et al (88) were able to demonstrate partial tumour response with EGFR-tyrosine kinase inhibitor in patients with lung adenocarcinoma metastases to the tonsils and bilateral internal auditory canal respectively. However, despite this, studies have so far failed to demonstrate an improvement in overall survival, although this has been argued that this is due to the high level of treatment crossover as disease progresses. Other therapeutic targets such as FGR-1 (fibroblast growth factor receptor 1) gene in squamous cell carcinomas are still being investigated (89), and they can perhaps play a major role in as treatment options in lung oligometastatic disease to the head and neck if identified early.
SBAR (Stereotactic ablative radiotherapy)/SBRT (Stereotactic body radiation therapy) has gathered significant attention in role of treating lung oligometastases. This is particularly in relation to non-small cell carcinomas, which are much less likely to present with widespread metastatic dissemination. A recent systematic review has revealed 4 prospective phase II randomized trials, 4 prospective non-randomized studies and eleven retrospective studies that have been fully completed and published results (90). Despite including head and neck sites, it is difficult to draw out any meaningful conclusions about the effect of SBAR on oligometastases to the head and neck because of the way the data has been grouped. However, overall, these studies have thus far demonstrated prolonged progression-free survival and overall survival compared to systemic therapy (chemotherapy +/-biological therapy). There are currently many ongoing phase III trials (90, 91), and once these are published, they will give a better idea of whether SBAR/SBRT is a feasible management option. However, there is no identifiable phase II/III trial looking at the use of SBAR in head and neck oligometastases only. This is something that can be established relatively easily in line with the current trials, and can provide good evidence-based guidance for future use of ablative radiotherapy for lung oligometastases in the head and neck.
Surgical resections in lung oligometastases were performed in the literature, and these had the potential to be either curative or of symptomatic benefit. This particularly applied to tonsillar metastases. Some advocate for a tonsillectomy in view of a biopsy regardless (68), and the mechanism of tonsillar spread as a form of direct implantation post-bronchoscopy favours it being an isolated lesion without any further tissue involvement. However, whether this translates into direct overall survival benefit is difficult to see with the low number of cases in literature. Certainly tonsillar oligometastases of other origin, in particular renal carcinoma, has demonstrated curative benefit after tonsillectomies, and this advocates this practice as a management option for oligometastases of lung origin.
Surgical management for parotid lesions from lung oligometastases is a bit more contentious. Some have advocated for parotidectomies with negative margins and preservation of the facial nerve in the presence of single parotid metastasis (35). However, in the literature, no cases of surgery to the parotid alone has resulted in curative treatment. Addition with chemo/radiotherapy may yield a greater overall survival benefit. In fact, Cui et al (70) revealed that with small cell metastases to the parotid gland, the life expectancy is less than 10 months, due to its aggressive nature. In addition to having an estimated 5 year survival rate of 10%, this means that curative or radical parotidectomies cannot be realistically performed in this population cohort. Combining parotidectomies with radiotherapy however, will allow greater symptom control such as preventing morbidity associated with fungating masses and nerve invasion, and allow greater locoregional control. Ipsilateral neck dissections have been performed in some cases in literature, but this is thought to be unnecessary because the metastasis is much more likely to have originated via the haematogenous route rather than the lymphatic route (70). It is not recommended because it avoids the morbidity associated with neck dissections and does not impact on locoregional control.
Metachronous oligometastatic disease tended to have better surgical outcomes than synchronous disease. This is especially well demonstrated in metastases to the thyroid (81). Squamous cell carcinomas also tended to present with metachronous disease. However, it can be argued whether synchronous disease can be included in the criteria of oligometastatic disease in the first place because there is no control of the primary lesion, and this has the potential to negatively impact upon the state of the lesion within the head and neck. Certainly for small cell carcinomas, many of the patients had very poor survival outcomes because despite locoregional control with surgery, there was limited control of the primary lung tumour and this would have led to metastases uncovered later that contributed to the patients’ deaths. The question of whether better surgical outcomes are associated with longer time intervals between initial diagnosis of the primary lesion and diagnosis of the metastatic lesion is one that needs to be answered, and retrospective analyses of national cancer databases can help establish this.
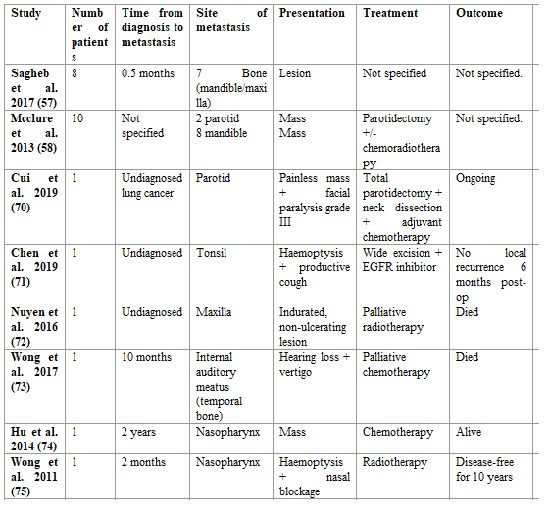
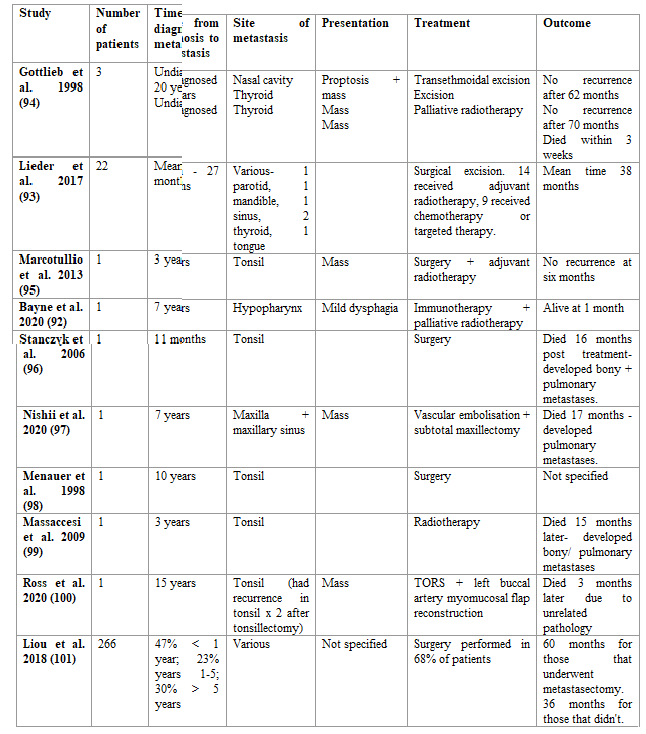
Renal carcinomas (RCC) are the 9th most common worldwide (92) and commonly metastasise to the lungs, bone and liver. However, they are in fact the third most common infraclavicular tumour to metastasise to the head and neck (93). 85% of all malignant renal tumours are comprised of the clear cell subtype (94). It has a very high risk of metastatic disease, primarily because of haematogenous spread due to its frequent invasion of the local vascular renal network. The most common sites to the head and neck involve the bone, skin, subcutaneous tissue and lymph nodes (92). Table 3 has been collated to show all the identified reports in literature, since 1995, with oligometastases to the head and neck region from a primary renal tumour that are of significant clinical relevance in terms of management. Studies with significant missing information for the chosen columns were excluded.
There are three proposed mechanisms in literature for renal cancers to metastasise to the head and neck. Haematogenous spread seems to the be most important mechanism, and this is relatively easy to explain because of the nature of invasion of the local vessels surrounding the kidney. Anatomically, this would however mean that lung metastases develop before head and neck oligometastases do. The concept of micro-seeding of the lungs proposed by Gottlieb et al (94) can help explain this phenomenon. In most likely case, oligometastatic disease of the head and neck is accompanied by microscopic seeding of the lungs which is not picked up on routine imaging, and explains why many of the patients with poor survival outcomes die as a result of pulmonary metastases. The other mechanisms are by Batson’s venous plexus and retrograde lymphatic flow, both of which have been explained.
Survival outcomes in table 3 demonstrate better outcomes than for breast oligometastases. Additionally, there are far fewer patients presenting with synchronous disease, and the time interval between diagnosis of primary tumour and oligometastatic lesion can even range up to 20 years. Lieder et al (93) demonstrated a rate of metastatic disease to the head and neck from RCC of 3.3% (22/671 patients) of all patients they treated with RCC, which they felt was sufficient enough to recommend for neck to be included in staging investigations for RCC. Liou et al (101) in a systematic review found a much higher rate of 14-16%, and so this advocates this recommendation even further. Crucially, metastases to the head and neck can result in severe morbidity and mortality involving airway obstruction, haemorrhage and airway obstruction, and for this reason both screening and treatment can be advocated.
RCC is a radioresistant tumour, and therefore radiotherapy is not often used as a treatment option. However, with metastatic lesions, SBAR has demonstrated significant progression-free and overall survival benefit with bone and brain metastases (102). Studies exploring its use within head and neck metastases have yet to sufficiently conclude or yield any significant results so far. A number of phase III trials with new immunotherapies such as bevacizumab + IFNα have demonstrated better response rates and progression-free survival over current regimes and this is something that can be explored in the oligometastatic cohort of patients.
To achieve locoregional control, surgery is still considered by many to be the definitive management option. There is a lot more evidence supporting surgical resections for oligometastases of renal origin than for breast and lung. A systematic review of 266 patients found that median overall survival of renal oligometastatic disease to the head and neck was 36 months. 68% of these patients underwent a metastasectomy. Interestingly, the median survival for those treated with complete metastasectomy was significantly higher at 60 months compared to 12 months for those with incomplete or no metastasectomy. It is however important to consider that the cohort of patients selected for surgery may have been fitter in the first place. However, after multivariate analysis to consider for cofounders, surgical metastasectomy remained associated with a reduced risk of death. Even in terms of locoregional control, recurrence only occurred in 16% of those treated with complete metastasectomy in this review and a local control rate of over 90% for oral cavity oligometastases of RCC origin in another review (97). Surgery is therefore advocated both for improved survival and for locoregional control.
The major complication with surgery for RCC in the head and neck is haemorrhage and this is why there may be a lot of hesitancy amongst ENT surgeons for performing them. Renal metastases have a rich blood supply, and this is of particular concern with oral cavity lesions. Involvement of interventional radiology with vascular embolisation of feeding vessels is a technique that has yielded successful results (97).
Recommendations/ Future studies:
Based on this review, the following can be recommended with regards to management of patients with oligometastatic disease to the head and neck.
Oligometastatic disease in head and neck cancer is a new entity that is beginning to gather significant attention. The most common infraclavicular primary tumours to metastasise to the head and neck are breast, lung and renal carcinomas. Management of these oligometastatic lesions is currently very variable and surgery and/or ablative therapies can in fact be associated with good survival outcomes or locoregional control. The recommendations in this paper will help towards establishing clear guidelines in the future for surgical and ablative therapies for these patients.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
