AUCTORES
Globalize your Research

Case Report
*Corresponding Author: K Karavdić, Clinic for Pediatric Surgery, Clinic Center of University Sarajevo, Bosnia and Herzegovina.
Citation: A Firdus, K Karavdić, L K Zametica, D Anić, N K Spahović, et al. (2022). Hemorrhagic Shock Caused by Mesenteric Injury - Ski Pediatric Blunt Abdominal Trauma case report. Journal of Clinical Surgery and Research. 3(3); DOI:10.31579/2768-2757/040
Copyright: ©2022 K Karavdić, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 January 2022 | Accepted: 31 January 2022 | Published: 24 February 2022
Keywords: mesenteric injury; skiing; blunt abdominal trauma
Trauma is the leading cause of pediatric mortality and abdominal injury is a significant contributor to morbidity. Abdominal trauma in the population of injured children, is the third leading cause of death in this population, after head and thoracic injuries. It is the most common cause of death owing to unrecognized injury. They most often occur in traffic accidents, games and sports. The clinical presentation depends on the severity of the injury, the injured organ and the associated injuries. Mesenteric injury from blunt abdominal trauma is uncommon and can be difficult to diagnose. It is known that seatbelt trauma from motor vehicle accidents is the most common mechanism of mesenteric injury and that the mesentery of the small bowel is injured more frequently than that of the colon. We present an unusual case, a seven-year-old boy who was injured while skiing. The patient was in a state of hemorrhagic shock and underwent emergency surgery after an urgent diagnosis. During the operation, the leading trauma and the reason for the hemorrhagic shock were found to be a mesenteric injury, and bleeding from the branches of the superior mesenteric artery. Early transport, monitoring and diagnostics significantly contribute to reducing morbidity and mortality. The standard in surgery is non-operative treatment of injured parenchymal organs. A multidisciplinary approach that includes doctors of various specialties (pediatric surgeons, pediatricians, neurosurgeons, anesthesiologists and radiologists) who contribute to the diagnosis and treatment of injured children through diagnostic and therapeutic procedures has a key role. At the end, the decision regarding surgical treatment is responsibility of pediatric surgeon.
Intraabdominal injuries occur as a result of blunt abdominal trauma or penetrating trauma and it is the most common cause (85%), while penetrating trauma is present in a minority of cases (15%). Abdominal trauma is the third leading cause of death in children older than 1 year [1]. Approximately 50-75% of blunt abdominal trauma is caused by motor vehicle collisions. Other causes include sports injuries, falls and child abuse. Sports injuries most frequently cause isolated organ injuries [2].
There are two main mechanisms: a direct stroke in the abdominal area and high-energy mechanisms that produce multisystem trauma. The latter is associated with higher mortality. Solid organ injury refers to the liver, spleen, or kidneys [3]. The most commonly injured organs are the spleen, liver, and kidney; because the spleen is the most common cause of intra-abdominal bleeding. Although blunt kidney injuries are much less common than spleen or liver lesions, children are more susceptible to kidney injuries compared to adults due to anatomical aspects. Bowel and mesenteric injuries are the third most common type of injury from blunt trauma to abdominal organs [4]. Three basic mechanisms may cause bowe and mesenteric injuries of blunt trauma: Direct force may crush the gastrointestinal tract; rapid deceleration may produce shearing force between fixed and mobile portions of the tract; and a sudden increase in intraluminal pressure may result in bursting injuries [5].
Despite the frequency with which abdominal trauma occurs in children, there is still controversy over the optimal evaluation strategy to identify intra-abdominal injury.Assessment by the American Association for the Surgery of Trauma Surgery (AAST) is most commonly used to classify spleen, liver, and kidney injuries. Management of SOI has evolved since 1970 when a group of pediatric surgeons in Toronto advocated for non-operative management of spleen injuries. This new trend was accompanied by advances in diagnostic imaging techniques which allowed more accurate evaluation of the lesion and avoidance of treatment delays. However, the management of blunt trauma in children has been a reason for debate in recent years. Currently, hemodynamic status is considered the most relevant factor in the process decision making [6].
Injuries of the abdominal organs can be in the form of cracks, perforations and ruptures of the abdominal organs such as the spleen, liver, mesentery, kidneys, diaphragm, stomach, duodenum, pancreas, intestines. They can be in form of injuries to blood vessels or rupture of the mesentery which leads to intraabdominal bleeding. Also, perforation can occur which leads to the peritonitis [7].
Children have an increased risk for intraabdominal injuries compared to adults for several reasons. They weigh less and receive force that is subsequently dissipated over a smaller area . Their organs are less protected due to having less fat and weaker muscles. Their ribs offer less protection due to their increased pliability [8].
Aim of this case report is to show a case of 7-year-old who suffered heavy blunt trauma while skiing due to collision with another person. We discuss and consider the challenge of blunt trauma management in pediatric patients, as well as current guidelines.
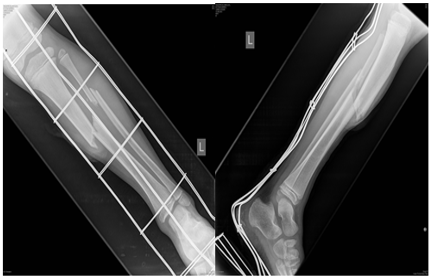
The case report is about a 7 years old boy, he was brought by ambulance accompanied by his father, who gave heteroanamnestic data regarding the child. Injury was caused during skiing by a direct collision from another person. On that occasion, he suffered head, abdomen and left lower leg injuries.Heteroanamnesis has indicated that after a collision with another skier, boy lost consciousness and had nausea. Blood pressure was 70/40 mmHg at the moment of arrival to hospital. At the time of examination he was conscious, communicative, oriented, did not reconstruct events, vomited twice, had nausea. The skin was pale. Abdomen was at chest level, tense, painful during palpation. Based on diagnostics (CT of the head, spine, pelvis with hips, thorax, abdomen, X-ray of lungs and left lower leg) as well as the laboratory findings (HTC 0.24, HGB 98) . CT showed a grade III spleen injury with a torn spleen greater than 3 cm and a hematoma with an irregular hypodense surface with obscure edges. The kidney had an irregular defect of the renal parenchyma deeper than 1 cm. The renal collecting system was not affected. This was considered grade III kidney damage. Free intraabdominal blood has been seen.(Figure 1.2.3).
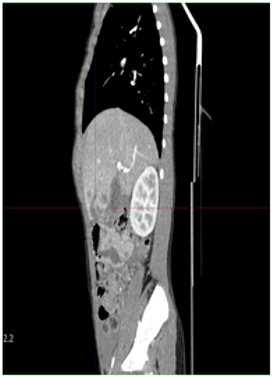
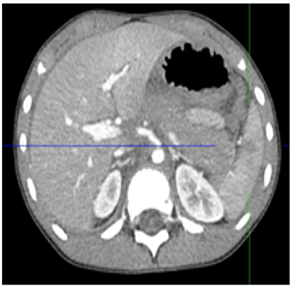


After admittance and after regular preoperative preparation (laboratory findings, radiological diagnostics – head, thorax, abdominal CT and consultation of various specialists), the same day after admission) the condition of hemorrhagic shock was verified and under general anesthesia, urgent surgical procedure was performed. The surgery was done as a vital indication due to clinical signs of hemorrhagic shock.
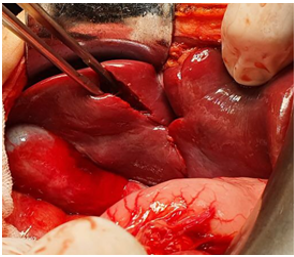
A medium laparotomy was chosen as the surgical approach and in abdominal cavity greater amount of fresh blood subhepatic right, paracolic on both sides, perihepatic, perisplenic and interintestinal was seen. The blood was evacuated and detailed exploration was done which pointed to subcapsular lesion of the spleen on the convexity in the middle part which did not bleed, hematoma of the lower part of spleen with incomplete demarcation to other tissue, traumatic liver lesion on the incision that is shallow, about 2 cm long, of slight depth, did not bleed or had a biliary leak; the second lesion is next to the fundus of the gallbladder just below the free edge of the liver, it is about 4 cm long and 1 cm deep, did not bleed actively or had biliary leak; the gallbladder was contused with a hematoma of the medial wall without elements of compression of the duct (Figure 7);
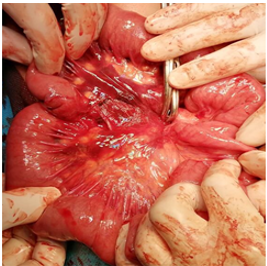
Traumatic lesion of the mesentery about 55 cm from Treitz with rupture of a bleeding blood vessel leading to a larger hematoma retroperitoneally on the left; the injury is taken care of by suture; lesion of the mesentery at about 70 cm with lesion of vascular branches with active bleeding (Figure 8);
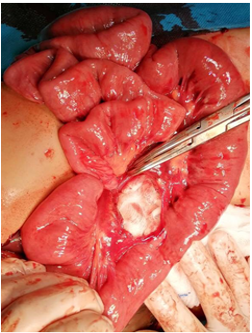
Traumatic rupture of the mesocolon in its half with a Riolan's arch lesion and consequent bleeding (Figure 9). The same is taken care of by blood vessel ligatures.
The exploration did not find other lesions or changes in the organs of the abdominal cavity.Lavage and hemostasis control are performed, and surgicell is placed on liver and spleen lesions. Ruptures of the mesentery and mesocolon are sutured and serous sutures are placed in two places. Throughout the operative work, the trophicity of the segment of the transverse colon and jejunum was monitored, which remained normal until the end and with preserved peristalsis. In conditions of induced hypertension, there was no active bleeding. Drains were placed: subhepatic right, subdiaphragmatic left and contact drain in Douglas space. The number of swabs were controled and operative wound was closed. The patient was transferred postoperatively to the Intensive Care Unit to continue monitoring and resuscitation treatment.
After surgical treatment abdomen was below level of thorax, postoperative wound was normal. Medial lap as well as the openings of three drains were covered with bandage material. Plaster was placed on the left thigh. On the right leg clinical finding was normal.The child wakes up regularly after general anesthesia. After that, the child is transferred to Pediatric Intensive Care Unit for the continuation of further treatment where he spends 10 days when the child was transferred back to Pediatric Surgery Clinic with recommendations.Antibiotic therapy was continued - Meropenem, Vankomycin for 11 days. Due to laboratory results (CRP 20, Le 10, SE 40) and due to small left basal pleural effusion and minor basal change corresponding to pulmonary infiltration on the left side of the lungs antibiotic therapy was modified - amoxicillin clavulanate 3x500 mg intravenously, with Fluconazole 1x200mg orally, according to the recommendation of the pulmonologist. In the therapy there were also analgetics, antipyretics and anticoagulants therapy enoxaparin sodium 1x4000mg subcutaneously due to high values of D-dimer and postoperative state.Since the child is still febrile on the 14th postoperative day, inflammatory markers were checked (CRP 9) and blood culture was done which was negative (sterile). On the 17th postoperative day a control X-ray of the lungs was performed and it was showing discrete basal changes, ultrasound of the abdomen corresponded to the postoperative condition, and the antimicrobial therapy was modified again due to recommendations of infectious disease specialist to oral Flucloxacillin 400mg 2x1 and Fluconazole tabletes 1x200mg.The child on the discharge properly tolerates oral intake, does not vomit, have a normal stool, was in good general condition, afebrile last 3 days, eupnoic, euhydric, with normal urinary function, and good local finding, wound was calm and dry.The child was discharged for further home treatment in good general condition and a satisfactory local finding with a recommendation of rest and further controls.
Blunt abdominal trauma is the most common cause of abdominal injuries in children. Blunt abdominal injuries are characterized by the transfer of high impact energy or acceleration and cause spraying of the capsule, laceration of the tissue of parenchymal organs, rupture of hollow organs filled with fluid or content.A special feature of abdominal injuries are lesions of the organs of the retroperitoneal space, and that is the space which, in addition to large blood vessels, also includes parts of the intraperitoneal organs. The pathophysiology, etiology, and clinical findings in children with internal abdominal injuries has some established characteristics. The first is that, generally, due to the anatomy, injuries in children tend to cause more organ damage and be more severe for the following reasons: 1) a small external force can cause severe injuries because the supportive tissues around the ribs, abdominal muscles, and organs are weak; 2) the relative capacities of solid organs such as the liver, pancreas, and spleen are large; and 3) the solid organs are not protected by the ribs because the diaphragm is almost horizontal [9-11] Other characteristics include the following: 1) since a small force is focused on a particular point, organ damage is often more severe than expected; and 2) compression between the abdominal wall and vertebral body by an external force often results in more severe organ damage. According to previous reports, in children who experienced non-accidental injuries, the frequencies of organ damage caused by blunt abdominal trauma were 64.1% in the liver, 19.2% in the kidney, 12.0% in the stomach and intestines, 9.0% in the spleen, and 7.3% in the pancreas [12, 13].
These injuries are often part of polytrauma, and special emphasis should be placed on the possibility of overlooking abdominal injuries with internal bleeding if a polytraumatized child is dominated by craniocerebral injury with loss of consciousness or apparently open fracture, which may distract physicians from discrete initial symptoms of internal injury.
In addition to the anamnesis, clinical findings and follow-up, as well as the laboratory findings, the most valuable diagnostic data on the location, type and extent of injury and possible free fluid in the peritoneal cavity can be obtained by echosonographic examination of the abdomen.If we do not have a clear diagnosis, we can expand the diagnosis with peritoneal lavage, and in ideal clinical conditions with laparoscopy and CT imaging. Although the patient was hypotensive, with signs of initial hemorrhagic shock, after Focused Assessment with Sonography in Trauma (FAST), together with anesthesiologists, who started resuscitation, we assessed that the patient is still hemodynamically stable and that CT was possible. FAST in unstable patients, is not useful for the diagnosis of lesions of intestinal and mesenteric injury because of its low sensitivity [14]. For hemodynamically stable trauma patients CT plays an importan role. Radiological signs associated with intestinal and mesenteric injuries are well defined [15]. Signs of intestinal wall injury include:discontinuity of the intestinal wall, thickening of the bowel walland increased or decreased enhancement of the intestinal walldefect after i.v. contrast injection. Images suggestive of mesentericinjury include: i.v. contrast extravasation (blush) or abrupt dis-continuation along a vascular branch, infiltration of mesenteric fatand hematoma.
Ruptures of the liver and spleen belong to the most common and most serious consequences of blunt abdominal injury. The exposure of these organs is higher than in adults due to their relatively larger volume and poorerweaker protection by a thin muscular wall. Symptoms relate to palpatory tension of the abdominal wall due to peritoneal stimulation and symptoms of bleeding. In splenic injuries, the pathognomonic clinical symptom of irradiation of pain in the left shoulder should be borne in mind. The patient should also be monitored if symptoms decrease and the red blood cell count stabilizes as subcapsular hematoma may rupture and subsequent bleeding may occur 24 to 48 hours after injury. Injuries to the urogenital system - the kidney is an organ that is functionally part of the urinary system but anatomically belongs to the retroperitoneal part of the abdomen and can be injured by blunt force injuries to the abdomen, and especially by a fall or blow to the back or groin.
The boy which we operated on had a lot of blood in the abdominal cavity, subcapsular lesion of the spleen on the convexity in the middle part which did not bleed, hematoma of the lower part of the spleen with incomplete demarcation to other tissue, two liver injuries (2 and 4cm) no bleed actively or had biliary leak; the gallbladder was contused with a hematoma of the medial wal without elements of compression traumatic lesion of the mesentery about 55 cm from Treitz with rupture of a bleeding blood vessel leading to a larger hematoma retroperitoneally on the left, lesion of the mesentery at about 70 cm with lesion of vascular branches with active bleeding; traumatic rupture of the mesocolon in its half with a Riolan's arch lesion and consequent bleeding. Ruptures of the mesentery and mesocolon are sutured and serous sutures are placed in two places.
Mesenteric and hollow organ injury represent 16% of all blunt abdominal traumas and occur as a result of high energy trauma involving motor vehicle accidents in 70–90% of cases [16]. Our case report was caused by a blow from another skier, which high energy obviously corresponded to the force and present in traffic accidents. Intestinal injuries and their mesenteries (mesocolon and mesentery) are con-sidered as a single clinico-anatomic entity. Small intestinal injuries constitute more than half of all blunt intestinal injuries, with equal involvement of the jejunum and ileum. The second most frequentlocation of injury is the colon: some studies show that left colonis more commonly injured than the transverse or right colon [17]. Our patient had an injured mesocolon transversum and branches of the arcus Riolani that give the arteries colica media and sinistra. Duodenal lesions are less common, representing 10% of the total and are often associated with pancreatic trauma. There are several types of intestinal and mesenteric injuries. The mesenteric injuries range from bruising, to hematoma, to frank bleeding through thetorn peritoneal envelope. Mesenteric disinsertion may occur with avulsion of the proximal or distal mesenteric root, which may cause intestinal perforation along the mesenteric surface of the bowel and localized devascularization of an intestinal segment resultingin ischemia and secondary perforation. Our patient did not have problematic intestinal vitality, although bleeding from the branches of the mesenteric vessels led to hemorrhagic shock [18].
The mechanism of mesenteric injury in blunt abdominal trauma involves compression and deceleration forces which result in a spectrum of injuries that range from contusions, to tearing of the bowel wall, to shearing of the mesentery, to loss of vascular supply or bleeding. Our patient was injured when another skier, an adult, crashed into a boy at high speed.Three basic mechanisms may cause bowel and mesenteric injuries of blunt trauma: Direct force may crush the gastrointestinal tract; rapid deceleration may produce shearing force between fixed and mobile portions of the tract; and a sudden increase in intraluminal pressure may result in bursting injuries [19].
The term solid organ injury refers to the liver, spleen, and kidney. Currently, non-operative management is the golden standard of care in favorable circumstances.A multidisciplinary approach that includes doctors of various specialties (pediatric surgeons, pediatricians, neurosurgeons, anesthesiologists and radiologists) who contribute to the diagnosis and treatment of injured children through diagnostic and therapeutic procedures has a key role. At the end, the decision regarding surgical treatment is responsibility of pediatric surgeon.
Due to the anatomy, injuries in children tend to cause more organ damage and be more severe.
In a polytrauma pediatric patient, with abdominal symptoms, clinical exa-ination and imaging studies (preferable a ct scan) are necessary.
Mesenteric injuries are difficult to diagnose and their undiagnosed complications are as a result of haemorrhage with high mortality rates
If the patient is hemodynamically unstable, polytraumatized, with signs of extensive mesenteric injuries, surgical treatment is indicated.
Intestinal or mesenteric pediatric injury should be suspected in all high energy blunt abdomia trauma.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
