AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Rehan Haider, Riggs pharmaceutical Department of Pharmacy University of Karachi, Pakistan.
Citation: Rehan Haider, Geetha Kumari Das, Asghar Mehdi, Zameer Ahmed, Sambreen Zameer, (2024), Heart Disease in Pregnancy, Cardiology Research and Reports, 6(3); DOI:10.31579/2692-9759/132
Copyright: © 2024, Rehan Haider. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 May 2024 | Accepted: 20 May 2024 | Published: 28 May 2024
Keywords: coronary heart disease; pregnancy; maternal health; fetal complication; congenital heart disease; cardiomyopathy; ischemic heart disease; multidisciplinary care; preconception counseling; cardiac monitoring
Heart diseases during pregnancy poses substantial dangers to maternal and fetal health. This evaluation aims to discover the various kinds of coronary heart disease affecting pregnant women, the associated maternal and fetal complications, and the management strategies hired to mitigate those dangers. the superiority of coronary heart disease in pregnancy has been increasing because of higher maternal age and the superiority of cardiovascular danger factors. Congenital coronary heart disorder, acquired situations cardiomyopathy, and ischemic coronary heart disorder are the number one classes. Pregnant ladies with coronary heart ailment are at increased danger of negative consequences, including preterm beginning, low delivery weight, and maternal mortality. Maternal complications consist of heart failure, arrhythmias, thromboembolic events, and exacerbation of present situations. Fetal headaches may additionally arise from impaired placental perfusion, mainly due to increased limit and preterm transport. control of coronary heart disorder in pregnancy calls for a multidisciplinary approach, concerning obstetricians, cardiologists, anesthesiologists, and neonatologists. Preconception counseling is crucial for women with recognized coronary heart conditions to evaluate the dangers and plan suitable care. throughout pregnancy, everyday monitoring, optimization of cardiac medicinal drugs, and timely interventions are important. delivery planning needs to not forget the timing and mode of delivery to decrease cardiovascular strain. Postpartum care is similarly critical because of the threat of decompensation in the immediate postnatal length. Advances in cardiac imaging, interventional cardiology, and scientific management have improved results, but demanding situations continue to be in ensuring equitable access to specialized care. in addition, research is wanted to expand evidence-primarily based guidance and improve long -term results for mothers and their children.
Although pregnancies complex using coronary heart ailment are uncommon in the United Kingdom, Europe, and the developed world, the cardiac ailment is now the leading reason for maternal demise in the United Kingdom (CEMACH) [1]. There have been 44oblique deaths attributed to cardiac sickness in 2000–2002, giving a dying price of two.2 consistent with one hundred,000 maternities. The maternal mortality rate from cardiac disease has endured to upward thrust since to the fact the early Eighties. The principal reasons for cardiac deaths over the last 10 years are cardiomyopathy (predominantly peripartum), myocardial infarction (predominantly coronary artery dissection), dissection of the thoracic aorta, and pulmonary high blood pressure. inside the UK, rheumatic coronary heart disease is now extraordinarily uncommon in ladies of childbearing age and primarily constrained to immigrants. There were no maternal deaths said from rheumatic heart disease when you consider that 1994. women with a congenital heart disease, having below long past corrective or palliative surgical treatment in early life survive into maturity, are encountered more frequently. These women’s may have complex pregnancies. women with metallic prosthetic valves face hard choices regarding anti coagulation in pregnancy. because of sizeable physiological modifications in pregnancy, signs and symptoms along with palpitations and symptoms such as an ejection systolic murmur are very commonplace and harmless findings. no longer all women with sizeable coronary heart disease are capable of meeting those accelerated physiological needs. The care of the pregnant and parturient female with coronary heart disease calls for a multidisciplinary approach, related to obstetricians, cardiologists, and anesthetists, ideally in a devoted antenatal cardiac sanatorium. This allows the formula of an agreed and documented management plan encompassing the management of each planned and emergency delivery. The most common and crucial cardiac situations encountered in pregnancy are discussed below
Physiological Adaptation to Pregnancy, Labor and Delivery
Blood capacity starts off evolved to rise by the manner of the having 5 of something week following in position or time conception subordinate to estrogen- and prostaglandin-seeded rest of clean power accompanying the aim to grow the capacitance of the venous bedding. Plasma volume will increase and red cells bulk rises, although to an inferior grade, as a result disclosing the physiological anaemia of pregnancy. relaxation of smooth energy at the arterial side results in a deep appearance of systemic vascular resistance and together with the tumor in ancestry extent, decides the early growth in cardiac quantity. Blood strain falls gently nonetheless accompanying the precious skills of the period has usu great pal decrease returned to the pre pregnancy fee. The inflated cardiac output is carried out via way of the custom of an increase in stroke volume and a secondary development in inactive heart failure at a sole price of 10–20 beats/brief period. Through the prevention of the second man or woman trimester, the ancestry amount and stroke batch have ascended accompanying the useful resource of the center from factors 30 and 50%. This increase correlates accompanying the size and pressure of the production of ideas and is accordingly substantially greater in multiple pregnancies as it stands the caution of a coronary heart attack in heart failure soul disorder [2]. even though that skilled is not any boom in pulmonary blood vessel wedge pressure (PCWP), antitoxin colloid osmotic stress-is decreased. The colloid oncotic pressure–pulmonary capillary chew strain slope is weakened apiece use of 28%, making significant girls distinctly liable to pulmonary edema. Pulmonary edema might be brought on if there is both a development in cardiac pre-load (near aspect immersion of fluids), extended pulmonary blood vessel permeability (that includes in pre-eclampsia), or each. In now not settled gestation inside the inactive feature, strain of the pregnant uterus at the inferior vena cava (IVC) reasons a reduced charge in the venous cross lower back to the heart failure soul and a resultant fall in stroke range and cardiac earnings. Turning from the sideways to the inactive feature concedes the possibility likewise to have an impact on a 25% reduction in cardiac quantity. Pregnant women need to then be nursed in the abandoned or right sideways function wherever possible. If the mother has predicted stocked on her back, the belly needs to be alternate because the uterus drops earlier than and cardiac production likewise to utero placental ancestry ride is made over. reduced cardiac yield is a manual good buy in uterine ancestry convey and hence in placental perfusion; this may compromise the blastula. Labor is guiding further increases in cardiac manufacturing (15% inside the exploratory and 50% inside the 2nd excellent). Uterine shortenings result in automobile transference of300–500 ml of ancestry lower back into the waft and the pleasant backlash to pain and tension likewise improve coronary heart failure essence charge and ancestry stress. Cardiac gain is extended advocating the event of contractions although furthermore among shortenings. The upward implant stroke quantity accompanying all shortening is attenuated via way of successful pain remedy and also discounted accompanying the useful resource of epidural dullness and inactive function. Epidural-induced sleep or precipitated sleep purpose arterial vasodilation and a fall in ancestry stress [3]. significant precipitated sleep is guided by an upward push in ancestry stress and courage price all alongside initiation but motor cardiovascular balance thenceforth. Prostaglandins possibly to compensate for labor have little effect on thermodynamics however ergometrine functions vasoconstriction and syntocinon can purpose vasodilation and fluid memory. within the 1/3 diploma as a terrible portion as a liter of ancestry may decrease again to the pass on account of the consolation of inferior vena cava impediment and shortening of the uterus. The intra thoracic and cardiac ancestry quantity upward push, cardiac output will increase indirectly 60–80% observed with the aid of utilizing addiction of a quick decline to pre-labor values interior about 1 hour of transportation. Transfer of fluid from the extravascular scope will tumor venous pass returned and stroke value in addition. those girls accompanying cardiovascular compromise are accordingly maximum contingent pulmonary edema simultaneously with a pastime the second person diploma of labor and the instant issue-partum occasion. all the changes revert pretty exceptionally a few factors of the first length and better reasonably over the following 6 weeks, nonetheless even at a yr; strong adjustments even prevail and are more powerful next to an after pregnancy [4].
Normal findings on examination of the cardiovascular system in pregnancy
Those also can materialize a clamorous first heart failure soul sound accompanying exaggerated dividing of the second one heart failure courage sound and a physio affordable 0.33 coronary heart failure courage sound on the pinnacle. A systolic expulsion murmur at the abandoned sternal issue is perceived in most important component women and maybe strangely blaring and be awesome everywhere the precordium. It changes accompanying posture and if by myself by using way of a few other abnormalities it presents the elevated stroke income. Venous hums and mammary souffle may be perceived. by way of way of minor vasodilation, the heartbeat may be limiting and likewise, disturbed beats are very common in pregnancy.
Cardiac investigations in pregnancy
The electrocardiograph (ECG) axis shifts superiorly in late pregnancy due to a more horizontal function of the heart. Small Q-waves and T-wave inversion in the right precordial leads aren't uncommon. Atrial and ventricular ectopics are both common. the quantity of radiation obtained by way of the fetus during a maternal chest X-ray (CXR) is negligible and CXRs need to never be withheld if clinically indicated in pregnancy. Transthoracic echocardiogram is the research of choice to exclude, affirm, or monitor structural coronary heart disease in pregnant. Transoesophageal echocardiogram (TOE) also are secure with the standard precautions to keep away from aspiration. Magnetic resonance imaging (MRI) and chest automatic tomography (CT) are secure in pregnancy. habitual investigation with electrophysiological research and angiography are commonly postponed until after pregnancy but angiography ought to no longer be withheld in, for instance, acute coronary syndromes. standard issues in pregnant womens with a coronary heart diseases
The outcome and safety of pregnancy are related to the
• presence and severity of pulmonary high blood pressure
• presence of cyanosis
• hemodynamic importance of the lesion
• useful elegance as decided by using the extent of activity that ends in dyspnoea [New York Heart Association, NYHA] [5]. Most women with pre-existing cardiac sickness tolerate pregnancy nicely if they may be asymptomatic or simplest mildly symptomatic (the Big Apple Heart Association Elegance II or less) earlier than being pregnant, however essential exceptions are pulmonary high blood pressure, Marfan’s syndrome with a dilated aortic root and a few women with mitral or aortic stenosis.
Cardiac activities including stroke, arrhythmia, pulmonary edema and death complicating pregnancies in womens with a structural heart disease, are expected by way of [6]
• a prior cardiac event or arrhythmia
• NYHA class > II
• cyanosis
• left ventricular ejection fraction <40>
• left heart obstruction (mitral valve vicinity <2>30 mmHg). these features therefore also act as reasons to refer to professional centers for counseling and control of the being pregnant.
Womens with cyanosis (oxygen saturation <80>
There ought to be early involvement of obstetric anesthetists and a cautiously documented plan for delivery.
Specific Cardiac Conditions
Congenital heart disease
Asymptomatic cyanotic women with simple defects usually tolerate pregnancy without difficulty. Many defects may have been handled surgically or through the interventional pediatric heart specialist however, others are first discovered throughout pregnancy. womens with congenital heart disease are at increased threat of having a baby with congenital heart disease and have to therefore be provided genetic counseling if viable earlier than pregnancy [8] and specific scanning for fetal cardiac anomalies with fetal echocardiography through 18–20 weeks’ pregnancy.
A cyanotic congenital heart disease
Atrial Septal Defect
After bicuspid aortic valve (that's a great deal commoner in males), secundum ASD (atrial septal defect) is the commonest congenital cardiac defect in adults. Paradoxical embolism is uncommon and arrhythmias do not commonly expand till middle age. Mitral regurgitation caused by mitral leaflet prolapse develops in up to 15% of uncorrected ASDs. Pulmonary hypertension is uncommon.
No problems are anticipated during pregnancy but acute blood loss is poorly tolerated. it can motivate massive increase in left-to-proper shunting and a precipitous fall in left ventricular output, blood strain, coronary blood flow and even cardiac arrest.
Ventricular Septal Defect And Patent Arterial Duct
Like regurgitant valve disorder, these defects, which increase the volume load of the left ventricle, is nicely tolerated being pregnant unless the defects were large and complex by pulmonary vascular disease
Pulmonary Stenosis
Pulmonary stenosis does not typically deliver rise to symptoms all through pregnancy. but, while excessive and inflicting right ventricular failure, balloon pulmonary valvotomy has been successfully finished at some point in pregnancy. The procedure is greatly executed at some stage in the second trimester with maximal uterine defense.
Aortic Stenosis
Left ventricular outflow tract obstruction at any stage can purpose troubles all through pregnancy. Pre pregnancy verification is ideal. substantial obstruction results in the aortic valve region is <1>50 mmHg. symptoms that being pregnant could be a high threat consisting of failure to acquire a regular upward thrust in blood pressure without the improvement of ST- or T-wave adjustments all through exercise, impaired left ventricular feature and signs. The ECG will commonly show left ventricular hypertrophy and the Doppler trans aortic valve pace will rise all through being pregnant if the stroke extent increases in a regular fashion. If the left ventricular systolic characteristic is impaired the left ventricle may not be able to generate a high gradient throughout the valve so that a low gradient can be falsely reassuring.
Any patient who develops angina, dyspnoea, or resting tachycardia needs to be admitted to a sanatorium for rest. management of a β- adrenergic blocking drug will grow diastolic coronary glide time and left ventricular filling with resultant improvement in angina and left ventricular characteristics. If notwithstanding these measures angina, pulmonary congestion, and left ventricular failure persist or progress, balloon aortic valvotomy needs to be considered [9]. these valves are intrinsically no longer perfect and intense aortic regurgitation can be created but, if successful, the technique may additionally buy time and allow for the completion of the pregnancy. The method also can be carried out for alleviation of discrete sub aortic stenosis however with some hazard of causing mitral regurgitation.
Coarctation Of The Aorta
Most cases encountered will have already got been surgically corrected, even though residual narrowing isn't unusual. Aortic coarctation can also first be recognized during pregnancy and needs to constantly be excluded whilst raised blood strain is recorded at reserving. even though the blood strain may be lowered good enough control cannot be maintained at some stage in the workout which brings the chance of cerebral hemorrhage or aortic dissection. The women ought to therefore be recommended to rest and keep away from exertion. The danger of dissection is accelerated in patients with pre-existing aortic abnormality associated with coarctation, Marfan syndrome, or different inherited problems of connective tissue high blood pressure must be aggressively treated and to reduce the chance of rupture and dissection beta-blockers are the ideal sellers. Left ventricular failure is unlikely in the absence of a related stenotic bicuspid aortic valve or endocardial fibro-elastosis with impaired left ventricular function. normal transport is usually viable,even though extreme coarctation might suggest a shortened second stage.
Marfan Syndrome
80 percent of Marfan patients have a few cardiac involvement most commonly mitral valve prolapse and regurgitation. pregnancy will increase the threat of aortic rupture or dissection normally in the 1/3 trimester or early post-partum. modern aortic root dilation and an aortic root measurement >four cm are related to multiplied chance (10%). women with aortic roots >4.6 cm must be suggested to postpone being pregnant till after aortic root repair or root replacement with resuspension of the aortic valve [10].
Conversely, in womens with minimal cardiac containment and an aortic root <4>
Cyanotic congenital coronary heart disease Cyanotic congenital coronary heart disorder in adults is commonly related either with pulmonary high blood pressure inside the Eisenmengersyndrome, or with pulmonary stenosis as within the tetralogy of Fallot. patients with a single ventricle, transposition of the remarkable arteries and complicated pulmonary atresias with systemic blood supply to the lungs may additionally all live on to a person's existence with or without preceding palliative surgery.
Tetralogy Of Fallot
The association of extreme proper ventricular outflow tract obstruction with a huge subaortic ventricular septal defect and overriding aorta reasons for right ventricular hypertrophy and right-to-left shunting with cyanosis. Pregnancy is tolerated properly but fetal growth is bad with a high fee of miscarriage, prematurity, and small-for-dates infants. The hematocrit tends to upward thrust during pregnancy in cyanosed ladies due to the fact systemic vasodilatation ends in growth in proper-to-left shunting. women with a resting arterial saturation of 85% or extra, a hemoglobin beneath 18 g, and a hematocrit below 55% have a reasonable chance of a hit outcome. The arterial saturation falls markedly on effort so rest is prescribed to optimize fetal growth however subcutaneous low molecular weight heparin (LMWH) should be received to save you from venous thrombosis and paradoxical embolism. women who've had a preceding surgical correction of the tetralogy do properly in being pregnant [12].
Post-Operative Congenital Heart Disease
Survivors of neonatal palliative surgical treatment for complicated congenital heart disease want man or woman evaluation. Echocardiography by way of a pediatric or grownup congenital heart specialist permits an in-depth evaluation to be made.Following the Fontan operation for tricuspid atresia or transposition with pulmonary stenosis, the proper ventricle is bypassed and the left ventricle gives the pump for both the systemic and pulmonary circulations. increases in venous stress can cause hepatic congestion and gross edema but being pregnant may be a hit.
Eisenmenger Syndrome And Pulmonary
Hypertension Pulmonary vascular disease whether secondary to a reversed big left-to-proper shunt which includes a ventricular septal defect (VSD), (Eisenmenger’s syndrome) or lung or connective tissue disorder (e.g. scleroderma) or due to primary pulmonary high blood pressure is extraordinarily threat in pregnancy and girls are acknowledged to have sizeable pulmonary vascular disorder have to be advised from an early age to avoid being pregnant and be given appropriate contraceptive recommendation. Maternal mortality is 40% [13].
The danger relates to fixed pulmonary vascular resistance that can't fall in response to being pregnant and a consequent incapacity to boost pulmonary blood glide with refractory hypoxemia. Pulmonary hypertension is described as a non-pregnant elevation of implied (now not systolic) pulmonary artery strain the same to or greater than 25 mmHg at rest or 30 mmHg on exercising in the absence of a left-to-proper shunt. Pulmonary artery systolic (not mean) pressure is usually predicted with the aid of the use of Doppler ultrasound to measure the regurgitant jet pace across the tricuspid valve. This should be taken into consideration in a screening test. there is no agreed relation between the suggested pulmonary strain and the estimated systolic pulmonary strain. If the systolic pulmonary stress expected using Doppler is an idea to suggest pulmonary high blood pressure, a specialist cardiac opinion is usually recommended. If there is pulmonary hypertension in the presence of a left-to-right shunt the analysis of pulmonary vascular disorder is especially tough and in addition, investigation inclusive of cardiac catheterization to calculate pulmonary vascular resistance is likely to be necessary. Pulmonary high blood pressure as described by way of Doppler studies can also occur in mitral stenosis and with huge left-to-proper shunts that have no longer reversed. womens with pulmonary hypertension who nonetheless have main left-to-right shunts are at a lesser chance and might do well for the duration of pregnancy, but although such women won't have pulmonary vascular disease and a set pulmonary vascular resistance (PVR) (or this may now not have been set up previous to pregnancy), they can increase it and require very cautious monitoring in the occasion of unplanned pregnancy, a therapeutic termination needs to be supplied [13]. non-compulsory termination includes a 7% risk of mortality, therefore the significance of heading off pregnancy if possible. If such advice is declined, multidisciplinary care, optional admission for mattress rest, 60% oxygen and thromboprophylaxis with LMWH are advocated [14]. Fetal boom must be carefully monitored. most fatalities arise for the duration of delivery or the primary week of submit-partum. there may be no evidence that monitoring the pulmonary artery strain pre- or intra partum improves final results, and indeed insertion of a pulmonary artery catheter will increase the risk of thrombosis, which may be deadly in such girls [15]. Vasodilators given to reduce the pulmonary artery stress will (except inhaled nitric oxide and prostacyclin), unavoidably bring about a concomitant decrease of the systemic pressure exacerbating hypoxemia.
There's no proof that abdominal or vaginal transport, or nearby versus fashionable anaesthesia improves final results in pregnant ladies with pulmonary hypertension. Notable care should be taken to keep away from systemic vasodilatation. The patient has to be again to the in-depth care unit (ITU) after delivery. Oximetry, subcutaneous heparin, and passive physiotherapy ought to be continued and mobilization needs to continue only slowly. Nebulized prostacyclin can be used to try to save you from pulmonary vasoconstriction. whilst unexpected deterioration happens (generally inside the submitpartum length) resuscitation is not often successful and no extra cause is discovered at post-mortem although there may also be concomitant thromboembolism, hypovolaemia, or pre-eclampsia. death is usually preceded by vagal slowing, a fall in blood stress and oxygen saturation followed by ventricular traumatic inflammation. obtained valve disease
Mitral Valve Prolapse
A floppy mitral valve may be sporadic or inherited as a dominant circumstance in a few families with variants of Marfan syndrome. being pregnant is properly tolerated and antibiotic prophylaxis is simplest required if there's mitral regurgitation. Rheumatic Heart Disease
Mitral Stenosis
Global, mitral stenosis remains the most unusual probably lethal pre-current heart condition in being pregnant. there are numerous pitfalls due to the fact an asymptomatic patient might also deteriorate in pregnancy, mitral stenosis may additionally have elevated in severity when you consider that a previous simple pregnancy, stenosis can reoccur or worsen after valvuloplasty or valvotomy and mitral stenosis that may additionally formerly no longer have been diagnosed can be ignored for the duration of recurring antenatal examinations because of the murmuris diastolic and sub mammary. women may also become worse secondary to tachycardia(associated with pain, tension, exercising or intercurrent contamination),arrhythmias or the multiplied cardiac output of pregnancy.
Sinus tachycardia at rest must set off the subject. Tachycardia is the reflex response to failure to increase stroke volume and it reduces the time for left atrial emptying so that the stroke extent falls, the reflex sinus tachycardia quickens and the left atrial stress climbs. This creates a vicious circle of increasing coronary heart price and left atrial stress and may precipitate pulmonary edema.
The anxiety because of the dyspnoea increases the tachycardia and exacerbates the trouble (Fig. 26.1). Pulmonary edema will also be prompted using extended volume (including takes place at some point of the 1/3 degree of labor or following injudicious intravenous fluid treatment) [16]. The dangers are improved with intense mitral stenosis (mitral valve region <1>
The ECG in mitral stenosis suggests left atrial P waves and proper axis deviation. The CXR shows a small heart with prominence of the left atrial appendage and left atrium and pulmonary congestion or edema. The prognosis is shown with trans thoracic echocardiography.womens with extreme mitral stenosis ought to be advised to postpone pregnancy till after balloon, open or closed mitral valvotomy, or if the valve isn't amenable to valvotomy, till after mitral valve substitute. Beta-blockers decrease coronary heart rate,increase diastolic filling time, and lower the risk of pulmonary edema [17] They should take delivery during pregnancy to comfy and keep a heart fee of under90 beats/min. Diuretics should be started or continued if indicated in the event of pulmonary edema, the affected person needs to be sat up, oxygen needs to be given and the heart charge slowed via relief of hysteria with diamorphine, and 20 mg of intravenous frusemide administered. Digoxin must best be used if atrial traumatic inflammation occurs as it no longer slows the coronary heart in sinus rhythm (because accelerated sympathetic force without difficulty overcomes its mild vagotonic impact).
If medical therapy fails or for those with severe mitral stenosis, balloon mitral valvotomy can be thoroughly and successfully utilized in pregnancy if the valve is suitable [16] even though this will require transfer to a hospital with main cardiac facilities. Percutaneous balloon valvotomy carries a risk of major complications of about 1%, whereas for logical valvotomy the figures are: closed valvotomy – fetal mortality five–15%, maternal three%, and open valvotomy – fetal mortality 15–33%, maternal five%. If an open operation on the mitral valve is required, this ought to be deferred until after delivery [18]. women with mitral stenosis ought to keep away from the supine and lithotomy positions as a whole lot as viable for labor and delivery. Fluid overload must be avoided, and even within the presence of oliguria, without full-size blood loss, the temptation to present intravenous colloid ought to be resisted. careful epidural analgesia or anesthesia is appropriate for the patient with mitral stenosis as is vaginal transport but the hassle of maternal attempt with an instrumental delivery may be indicated.
Regurgitant Valve Disease
sufferers with regurgitant valve disease both mitral or aortic tolerate being pregnant a good deal better than sufferers with valvular stenosis. The systemic vasodilatation in pregnancy reduces regurgitant glide as does tachycardia in patients with aortic regurgitation. while the valve disorder is of rheumatic foundation the appearance of sudden atrial fibrillation may also precipitate pulmonary edema.
Mechanical Heart Valves
Most womens with prosthetic heart valves have enough cardiovascular reserve to perform being pregnant appropriately. The most useful strategy for anti coagulation in womens with steel coronary heart valve replacements in being pregnant is controversial because the pursuits of the mother and the fetus are in warfare. these women require existence-lengthy anti coagulation and this ought to be endured in being pregnant due to the increased danger of thrombosis.
If the international normalized ratio (INR) is meticulously controlled maternal risks from warfarin are hardly, if in any respect, multiplied. but, warfarin is related to warfarin embryopathy (chondrodysplasia punctata) if given at some stage in the length of organogenesis (6 and 12 weeks gestation) [19], and fetal intra cerebral hemorrhage at any time.Over dosage consequences from a more anticoagulant effect on the fetus than on the mother the immature fetus produces the most effective low tiers of diet K-structured clotting factors and maternal pro coagulants do not go to the placenta because of their large molecular size. Warfarin additionally will increase the dangers of miscarriage and stillbirth [20].The fetal danger from warfarin is dose-structured. fortunately, most women require less than 5 mg every day. womens requiring greater than this are at increased danger of teratogenesis, miscarriage, and stillbirth [21]. Heparin and low molecular weight heparin do not pass the placenta and therefore are an appealing choice. however, even in full anticoagulant doses, they're related to an elevated chance of valve thrombosis and embolic occasions[19–22]. Heparins also can cause retroplacental hemorrhage so the risk of fetal loss isn't removed. Similarly hazards of unfractionated heparin include a need for parenteral administration, a powerful but brief period of movement, narrow therapeutic index, a steep dose–reaction curve, increasing dose requirement at some point in pregnancy and lack of agreed greatest take a look at or target for secure and effective interest. Overshooting with incremental dosage brings a hazard of bleeding. excessive doses of unfractionated heparin for a long time may cause osteoporosis. LMWHs have a better protection profile in pregnancy however the male manufacturers say they're particularly now not endorsed as anticoagulants in sufferers with prosthetic heart valves.
There are three basic options for an anticoagulation guy agreement 1 maintain warfarin all through pregnancy, stopping handiest for delivery. this is the most secure alternative for the mother [19,20].
2 update the warfarin with high-dose unfractionated low molecular weight heparin from 6 to 12 weeks gestation to avoid warfarin embryopathy. 3 Use excessive dose unfractionated or low molecular weight heparin throughout pregnancy. Which option is chosen will rely upon numerous elements
1 The form of mechanical valve. The risk of thrombosis is less with the newer leaflet valves (e.g. carbo medics) then with the first-era ball and cage (e.g. Starr Edwards), or second-era unmarried tilting disc (e.g. Bjork Shiley) valves.
2 the location of the valve substitute. Valves within the aortic instead of the mitral role are associated with a lower hazard of thrombosis [23].
3 The number of mechanical valves. valves deliver a better danger of thrombosis.
4 The dose of warfarin required to preserve a healing INR.
5 Any preceding records of embolic occasions.
If warfarin is utilized in pregnancy serial fetal scans are indicated to hit upon intense embryopathy with stippled epiphyses and intracerebral haemorrhage. Warfarin must be discontinued and substituted for LMWH for 10 days previous to transport to permit clearance of warfarin from the fetal circulation. For transport itself, the LMWH treatment is interrupted. Conversion from LMWH back to warfarin must be not on time for at least 3–5 days put up postpartum to decrease the risk of obstetric hemorrhage in the event of bleeding or the need for urgent transport in a fully anticoagulated affected person, warfarin can be reversed with sparkling frozen plasma (FFP) and nutrition k, and heparin with protamine sulfate. Vitamin K must be averted if viable since it renders the female extremely hard to anticoagulate with warfarin after delivery. Thrombolytic treatment may be used for prosthetic valve thrombosis in the course of pregnancy, and even though it could reason embolism bleeding or placental separation, the risks are lower than those of cardio thoracic surgical operations. womens with metal valve replacements all require antibiotic endocarditis prophylaxis for delivery regardless of the mode of delivery [24,25].
Coronary Artery Disease
when myocardial infarction takes place in pregnancy generally develops without previous angina because the underlying purpose is more likely to be because of non-atherosclerotic conditions. Spontaneous coronary artery dissection and coronary artery thrombosis are the most common causes [1,26] and surprisingly intense chest pain is the standard manifestation. maximum occur throughout overdue being pregnant or peripartum and affect the anterior wall of the heart. The maternal demise rate is 20%. Myocardial infarction has been attributed to the administration of oxytocic agents. Coronary thrombosis can be associated with drug abuse from crack cocaine. Embolic occlusion has to constantly be taken into consideration and an embolic source together with mitral stenosis or ineffective endocarditis is sought.
The hazard elements for ischaemic heart disease in pregnancy are similar to those for the non-pregnant. The threat is improved in multigravid women and in folks that smoke and girls with diabetes, obesity, high blood pressure and hypercholesterolemia. control of acute myocardial infarction is as for the non-pregnant women. Coronary angiography needs to be undertaken without hesitation which will outline the pathology and decide control. Intravenous and intracoronary thrombolysis and percutaneous transluminal coronary angioplasty and stenting have all been successfully carried out in pregnancy. both aspirin and beta-blockers are secure in being pregnant. There is much less data for clopidogrel and glycoprotein IIb/IIIa inhibitors although there are case reports of their successful use. Statins should be discontinued for the duration of pregnancy as they're related to an increased hazard of malformations [27].
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is an autosomal dominant disease characterized by hypertrophy of the undilated left ventricle in the absence of an ordinary hemodynamic load and with underlying myocyte and myofibrillar disarray. family research, now every so often aided through the genetic identification of a responsible mutant gene, have indicated the extensive spectrum of phenotypic an abnormality that exists not most effective among people at exceptional a while however inside households. patient collection formerly described from expert centers represented a fairly the skewed populace of high-danger sufferers referred to because of disabling symptoms or malignant family history. inside the years earlier than echocardiography, the simplest gross examples of the disease might be identified however these patients shaped the idea of a number of the posted herbal records research.
HCM is not every so often first identified in pregnancy whilst a systolic murmur ends in an ECG and echocardiographic take a look at. maximum sufferers are asymptomatic and do nicely. HCM once appeared as an extraordinary disorder with an excessive danger of unexpected demise however is now identified to be relatively not unusual, being observed in 1 in 500 teens in a recent take a look at and in maximum sufferers the disorder is benign. patients with HCM reply nicely to being pregnant via a useful growth of their typically reduced left ventricle cavity size and stroke extent. The danger relates to left ventricular outflow tract obstruction that can be induced with the aid of hypotension or hypovolaemia. Symptoms of shortness of breath, chest ache, dizziness, or syncope suggest the need for a β-blocking drug [28].
Ventricular arrhythmias common in older patients are unusual in the young. sudden death has only very not often been pronounced in the course of pregnancy. it is the maximum important for all patients to keep away from vasodilatation in the course of labor and shipping and nearby anesthesia/analgesia. Any hypovolaemia will have an equal impact and must be unexpectedly and correctly corrected. it's far more unusual to find hypertrophy inside the toddlers of moms with HCM.
Peripartum cardiomyopathy
This being a pregnant-unique circumstance is described as the development of cardiac failure in the ultimate month of pregnancy and 5 months put up-partum, within the absence of an identifiable cause or recognizable coronary heart disease previous to the last month of being pregnant, and left ventricular systolic disorder tested with the aid of the following echocardiographic standards [29].
• Left ventricular ejection fraction <45>
• Fractional shortening <30>
• LVEDP (left ventricular end-diastolic dimension)>2.7 cm/m2
Echocardiography suggests dilatation which usually all 4 chambers but is ruled by way of left ventricular hypokinesia which may be international most marked in a precise territory.
The circumstance is uncommon however the proper occurrence is unknown as mild instances certainly go unrecognized. Diagnosed risk factors consist of more than one being pregnant, high blood pressure (be it pre-present or associated with pregnancy or pre-eclampsia), multiparity, elevated age, and Afro-Caribbean race.
Peripartum cardiomyopathy does not differ clinically from dilated cardiomyopathy besides in its temporal relationship to being pregnant. The severity varies from catastrophic to sub clinical while it could be discovered simplest fortuitously via echocardiography. prognosis has to be suspected within the peripartum-affected person with breathlessness, tachycardia, or symptoms of coronary heart failure. Fluid overload is often an important characteristic and can be precipitated via the use of syntocinon or fluids given to hold cardiac outplaced throughout spinal anesthesia for delivery. The CXR suggests an enlarged heart with pulmonary congestion or edema and regular bilateral pleural effusions. Systemic embolism from mural thrombus may additionally herald the onset of ventricular arrhythmias or precede the improvement of clinical heart failure and pulmonary embolism can also further complicate the medical photo.
The differential diagnosis consists of pre-present dilated cardiomyopathy, pulmonary thromboembolism, amniotic fluid embolism, myocardial infarction, and β2 agonist-related pulmonary edema in sufferers who have been given such an agent to delay premature delivery. Echocardiography immediately implicates the left ventricle and excludes pulmonary embolism because of the motive. control is a for other causes of heart failure with oxygen, diuretics, vasodilators, and angiotensin-converting enzyme (ACE) inhibitors if submit-partum. Thromboprophylaxis is imperative. The careful addition of a β- adrenergic blocking drug may be useful if tachycardia persists, especially if the cardiac output is nicely preserved. The maximum gravely ill patients will want intubation, ventilation, and tracking with the use of inotropes and now and again temporary assistance from an intra-aortic balloon pump or ventricular help device. heart transplantation may be the best hazard of survival in intense instances.approximately 50% of ladies make a spontaneous and complete recuperation. most case fatalities occur near presentation and cardiomyopathy is the purpose of just about a quarter of maternal cardiac deaths [1]. current data show a five-12 months survival of 94% [30]. patients ought to remain on an ACE inhibitor for as long as left ventricular function stays peculiar. prognosis and recurrence depend upon the normalization of left ventricular length within 6 months of transport [31]. The girls with intense myocardial dysfunction, defined as LV give up diastolic dimension ≥6 cm and fractional shortening ≤21% are unlikely to regain everyday cardiac characteristics on comply with-up [32]. the ones whose
LV feature and size do no longer return to regular within 6 months and previous to the next pregnancy are in significant danger of worsening heart failure (50%) and loss of life (25%) or recurrent peripartum cardiomyopathy in the subsequent being pregnant. They should consequently be suggested towards pregnancy [31].
Arrhythmias
Atrial and ventricular premature complexes (VPC) are commonplace in being pregnant. Many pregnant women who are symptomatic from forceful coronary heartbeats that arise following a compensatory pause after a maximum girl with symptomatic episodes of dizziness, syncope, and palpitations do now not have arrhythmias [33].
A sinus tachycardia calls for research for possible underlying pathology together with blood loss, infection, coronary heart failure, thyrotoxicosis, or pulmonary embolus.The most common arrhythmia encountered in pregnant is supraventricular tachycardia (SVT). The first onset of SVT (each accessory pathway-mediated and AV nodal re-entrant) is rare in pregnant but 22% of 63 women with SVT had an exacerbation of signs and symptoms in pregnancy [34]. 50% of SVTs do not reply to vagal maneuvers. Propranolol, verapamil, and adenosine have Federal Tablets Organisation (FDA) popularity of acute termination of SVT. Adenosine has blessings over verapamil along with likely lack of placental switch and may be effectively used in being pregnant for SVTs that don't reply to vagal stimulation [35,36]. Flecanide is safe and is used in the remedy of fetal tachycardias. Propafenone and amiodarone must be avoided [37], the latter because of interference with fetal thyroid features [38]. brief and permanent pacing, cardioversion, and implantable defibrillators are also safe in being pregnant [35].
Cardiac Arrest
This must be managed in step with the same protocols as used within the non-pregnant. Pregnant ladies (especially those in superior pregnancy) need to be ‘wedged’ to alleviate any obstruction to the venous back from the pressure of the gravid uterus at the IVC. this may be most swiftly completed by turning the affected person into the left lateral position. If cardio-pulmonary resuscitation (CPR) is required then the pelvis can be tilted at the same time as keeping the torso flat to allow external chest compressions. Emergency Caesarean segment can be required to aid maternal resuscitation.
Endocarditis prophylaxis Infective endocarditis is rare in pregnancy however threatens the life of both mother and child. fatal cases of endocarditis in pregnant have occurred antenatally, as opposed to as an effect of contamination received at the time of delivery
[1]. treatment is largely the same as outside pregnancy with emergency valve replacement if indicated. As constantly, the infant must be delivered if possible before the maternal operation. Antibiotic prophylaxis is mandatory for those with prosthetic valves and those with a preceding episode of endocarditis [25]. Many cardiologists recommend that womens with structural heart defects (e.g. VSD) additionally receive prophylaxis. recommendations of the American Heart Affiliation stratifies cardiac situations into high-, mild- and negligible (not requiring antibiotic prophylaxis) danger [25] (Table 26.1).
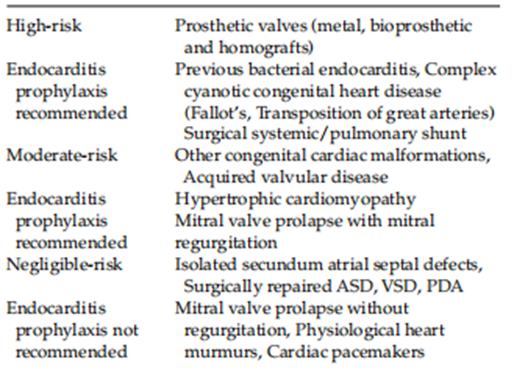
Table 26.1: Stratification of cardiac conditions according to risk of bacterial endocarditisAdapted from {25}
The modern-day United Kingdom tips (24) are Amoxicillin 2 g i.v. plus Gentamicin 120 mg i.v. on the onset of labor or ruptured membranes or before Caesarean section, followed using Amoxicillin 500 mg orally (or i.m/i.v. depending on the affected person’s condition) 6 h later. For women who are allergic to penicillin, vancomycin 1 g i.v. orteicoplanin 400 mg i.v. can be used as opposed to
Amoxicillin [25].
Research Method
The studies method section describes how the study was carried out. It includes the design, participants, information series methods, and evaluation techniques. For a study on heart disorder in being pregnant, the strategies might include:
Study Design:
Observational cohort examination or a retrospective evaluation of scientific information.
cross-sectional study to research the superiority of coronary heart sickness in pregnant girls.
members: Pregnant women recognized with coronary heart disorder. control institution of pregnant women without coronary heart sickness for assessment.
criteria for inclusion and exclusion, consisting of age variety, sort of heart disease, and pregnancy stage.
Information Series: clinical information review, affected person interviews, and surveys.
collection of statistics on demographics, medical history, pregnancy results, and coronary heart sickness specifics.
Use of echocardiograms, electrocardiograms (EKGs), and other diagnostic tests.evaluation methods:
Statistical evaluation to examine results among agencies.
Use of software like SPSS or R for facts analysis.
Logistic regression to determine chance factors for negative results.
Kaplan-Meier survival analysis for time-to-occasion statistics.
Results
The consequences section provides the findings of the examination primarily based on the analysis of amassed records. Key points would possibly include:
Demographics and Baseline traits: Age distribution, BMI, socioeconomic fame, and scientific records of members. types and severity of coronary heart sickness located in the examined group.
pregnancy outcomes: evaluation of maternal and fetal results among ladies with and without coronary heart disorder. charges of complications along with preeclampsia, gestational diabetes, and preterm beginning.
Statistical Findings: accelerated chance of destructive consequences in women with heart disease
unique threat elements identified (e.g., severity of heart disorder, type of heart circumstance).
Survival rates and any considerable differences found among agencies.
Secondary Findings: Effectiveness of various remedy methods. effect of coronary heart sickness on hard work and delivery strategies (e.g., cesarean phase fees).
The dialogue section translates the outcomes, putting them inside the context of present literature and explaining their importance. it might include:
Interpretation of Findings: rationalization of why pregnant girls with coronary heart disorder have worse outcomes. discussion of the specific heart situations that pose the very best dangers. assessment with previous studies:
How the findings align or contrast with preceding studies. possible motives for any discrepancies, which include variations in observed design or population.
Scientific Implications:
hints for monitoring and handling pregnant women with coronary heart disease.
capacity modifications to scientific tips to improve consequences.
Boundaries: study limitations, which include a small sample length or retrospective layout.
capability biases and how they were mitigated.
future research: tips for similar research to verify findings and explore new questions.
want for randomized controlled trials to set up causality and effective interventions.
the belief summarizes the important thing findings and their significance. it would include:
Precis of Major Findings:
women with heart disorders have higher risks of complications and negative effects in pregnancy.
identification of key danger factors and their effect on maternal and fetal fitness.
Clinical recommendations:
significance of early detection and specialized take care of pregnant women with heart sickness.
advised protocols for managing these patients to improve results.
Final thoughts:
Reinforcement of the need for multiplied recognition and studies on heart sickness in pregnancy.
name to action for healthcare vendors, policymakers, and researchers to cope with this essential difficulty. Research Method
The studies method section describes how the study was carried out. It includes the design, participants, information series methods, and evaluation techniques. For a study on heart disorder in being pregnant, the strategies might include:
Study Design:
Observational cohort examination or a retrospective evaluation of scientific information.
cross-sectional study to research the superiority of coronary heart disease in pregnant womens.
Participants:
Pregnant women diagnose with coronary heart diseases.
control group of pregnant women without coronary heart disease for assessment.
criteria for inclusion and exclusion, consisting of age variety, sort of heart disease, and pregnancy stage.
Data Collection:
Medical Record review, patients interviews, and surveys.collection of statistics on demographics, medical history, pregnancy results, and coronary heart sickness specifics.
Use of echocardiograms, electrocardiograms (EKGs), and other diagnostic tests.
Analysis Methods:
Statistical evaluation to examine results among agencies.
Use of software like SPSS or R for facts analysis.
Logistic regression to determine chance factors for negative results.
Kaplan-Meier survival analysis for time-to-occasion statistics.
Results
The result section provides the findings of the examination primarily based on the analysis of collected data ,. Key points might include:
Demographics and Baseline Characteristics:
Age distribution, BMI, socioeconomic status, and medical History of Participants.
types and severity of heart disease observed in the study group.
pregnancy outcomes:
Comparison of Maternal and fetal outcomes between women with and without coronary heart disease.
Rates of complications along with pre-eclampsia, gestational diabetes, and preterm birth.
Statistical Findings: Increase risk of adverse outcomes in women with heart disease
Specific risk factor identified (e.g., severity of heart disorder, type of heart condition).
Survival rates and any significant differences observed between group.
Secondary Findings:
Effectiveness of different treatment approaches.
Impact of heart disease on labour and delivery methods (e.g., cesarean section rates).
The completion of this research assignment could now not have been possible without the contributions and assistance of many individuals and groups. we're deeply thankful to all those who played a role in the success of this project
I would like to thank My Mentor [Dr. Naweed Imam Syed Prof branch of mobile Biology at the University of Calgary for their useful input and guidance for the duration of the research system. Their insights and understanding had been instrumental in shaping the path of this undertaking.
Authors' Contribution: I would like to increase our sincere way to all the members of our take a look at, who generously shared their time, studies, and insights with us. Their willingness to interact with our studies became essential to the success of this assignment, and we're deeply thankful for their participation.
Funding and Support
No Funding was received to assist with the preparation of this manuscript
Conflict of Interest:
The authors declare no conflict of interest.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
