AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Ahmed N. Ghanem, Retired Consultant Urologist Surgeon & Independent Investigator Mansoura University, Faculty of Medicine, No1 President Mubarak Street, Mansoura 35511, Egypt.
Citation: Shoichiro Ozaki. (2020) in clear water no fish can live. Water purification promote global warming, decline of countries. Biomedical Research and Clinical Reviews. 3(2); DOI: 10.31579/2692-9406/037
Copyright: © 2021 Ahmed N. Ghanem, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 December 2020 | Accepted: 21 January 2021 | Published: 25 January 2021
Keywords: fluid therapy; ards; fluid overload; volume kinetic; capillary physiology; starling’s law; hydrodynamics, hemodynamics
Fluid therapy (FT) was introduced during WW2. Ever since its complications have been frequently reported but notably some serious complications have been overlooked. The role of volumetric overload (VO) in inducing VU shocks (VOS) and causing the acute respiratory distress syndrome (ARDS) has remained overlooked, unrecognized, and underestimated till recently.
The role of FT complications in inducing VOS and causing ARDS is hard to detect because VOS is a shock that complicates another existing shock seamlessly and un-noticed. The author attributes this to the faulty rules on FT dictated by the wrong Starling’s law that causes many errors and misconceptions of FT which mislead physicians into giving too much fluid during shock resuscitation. The research findings on the wrong Starling’s law and how it has been corrected based on the hydrodynamic of the porous orifice (G) tube and the newly recognized VOS and the new patho-aetiology and therapy of ARDS are summarized here. Other authors in support of this contention are quoted. The errors on current FT and its corrections are given.
Finally, a new prospective cohort study on FT and ARDS is recommended and a call for new guidelines on FT is urgently needed.
Abbreviations
FT fluid therapy
VOS Volumetric Overload Shocks
ARDS Acute Respiratory Distress Syndrome
WW2 World War 2
Introduction
The great benefit that fluid therapy (FT) brought to humanity is undoubted since its introduction during World War 2 (WW2) and has continued in civilian hospital medical practice ever since. However, it has complications and the most serious remain overlooked and underestimated. Fluid therapy is used for fluid maintenance and in the management of shock resuscitation, acutely ill patients and during prolonged major surgeries. The last two are the situation during which FT complications occur.
Despite consistent reporting of FT complications since WW2, the most important and serious complications remain unrecognized and underestimated: This is precisely the current state of FT recommendations that induce Volumetric Overload Shocks (VOS) [1] and cause the Acute Respiratory Distress Syndrome (ARDS) [2,3]. This article addresses this issue by identifying the errors and misconceptions and providing the corrections and the new scientific basis for the future recommendations on FT guidelines. It starts by documenting the evidence that FT induces VOS and causes ARDS.
Evidence provided by the Author
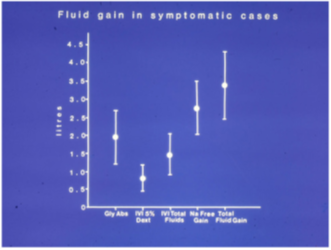
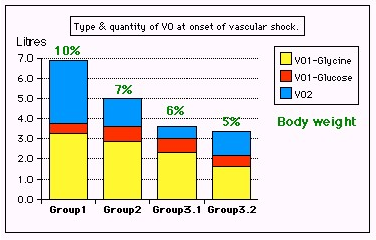
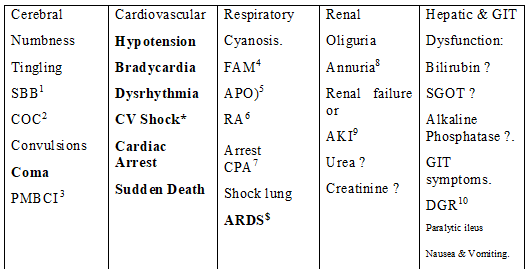
The author reported on VOS or Volume Kinetic (VK) shocks in clinical practice affecting mostly surgical patients [1, 4]. The clinical evidence is summarized in (Figures 1 and 2 and Table 1). It is reported that VOS cause ARDS [2, 3]. The identified underlying culprit is Starling’s law that dictates the faulty rules on FT, causing many errors and misconceptions [4] that mislead physicians into giving too much fluid during the resuscitation of shock [5] that induce VOS [1] and cause ARDS later [2,3]. The correction as based on the hydrodynamic of the porous orifice (G) tube is shown in (Figure 3) that is a diagrammatic representation based on many photographs. It demonstrates the magnetic field-like fluid circulation between fluid in the lumen of the G tube and that around it in surrounding chamber C.
Abbreviations for Table 1
SBB1 Sudden bilateral blindness
COC2 Clouding of consciousness
PMBCI3 Paralysis mimicking bizarre cerebral infarctions, but is recoverable on instant use of HST of 5%NaCl and/or NaCo3, and so is coma and AKI
FAM4 Frothing around the mouth
APO5 Acute pulmonary oedema
RA6 Respiratory arrest
CPA7 Cardiopulmonary arrest
ARDS $ Manifests later on ICU
AKI9 Acute kidney injury
DGR10 Delayed gut recovery
CV Shock* Cardiovascular shock of VOS reported here as VOS 1 and VOS2.
Annuria8 That is unresponsive to diuretics but responds to HST of 5%Ncl and/or 8.4%NaCo3
AKI8 Acute kidney injury
Also occurs the excessive bleeding at the surgical site and
Leukocytosis occurred in the absence of sepsis and septic shock
Evidence provided by other eminent researchers
Other researchers have recently reported that too much fluid infusions causes clinical problems identified and gathered in (Table 1) which are manifestations of the multiple organs dysfunction syndromes (MODS) that include ARDS, Coma, AKI, hepatic and hematological dysfunctions.. However, they have stopped short of recognizing that VOS and ARDS are caused by excessive infusion of FT.
Professor Hahn has reported massively on VK in healthy volunteers and patients [7,8]. He reported in conclusion that: "Guidelines for fluid therapy rarely take into account that adverse effects occur in a dose-dependent fashion. Adverse effects of crystalloid fluids are related to their preferential distribution to the interstitial of the subcutis, the gut, and the lungs. The gastrointestinal recovery time is prolonged by 2 days when more than 2 liters is administered. Infusion of 6-7 liters during open abdominal surgery results in poor wound healing, pulmonary oedema, and pneumonia. There is also a risk of fatal postoperative pulmonary oedema that might develop several days after the surgery. Even larger amounts cause organ dysfunction by breaking up the interstitial matrix and allowing the formation of lacunae of fluid in the skin and central organs, such as the heart. For both crystalloid and colloid fluids, coagulation becomes impaired when the induced hemodilution has reached 40%. Coagulopathy is aggravated by co-existing hypothermia. Although oedema can occur from both crystalloid and colloid fluids, these differ in pathophysiology."
Other authors also found a significant effect of crystalloids overload on morbidity and mortality of ARDS as they did the research during the first 24-48 hours from hospital admission. I have found only one study on adults' trauma patients by Jones et al (2016) [9], and one paediatrics study by Coons et al (2018) [10] and a remarkable review article by Schrier reported in 2010 [11] that incriminate saline overload and recommend judicious use of fluid infusion during resuscitation. In patients of these adult and paediatric trauma trials there is no sepsis involved and both studies were done over a period of 24 and 48 hours, respectively. Both articles detected a significant relationship of VO with morbidity and mortality of ARDS.
Jones et al [9] reported: "Large-volume crystalloid resuscitation is associated with increased mortality and longer time ventilated. Based on this data, we recommend judicious use of crystalloids in the resuscitation of trauma patients.”
The conclusion by Coons et al [10] was: "Early administration of high volumes of crystalloid fluid greater than 60 ml/kg/day significantly correlates with pulmonary complications, days NPO, and hospital length of stay. These results span the first 48 h of a patient's hospital stay and should encourage surgical care providers to exercise judicious use of crystalloid fluid administration in the trauma bay, ICU, and floor"
The huge prospective multicenter trials [12, 13] also documented massive volumetric overload (VO) retained in surviving ARDS patients of 3-10 liters but have neither recognized VOS nor incriminated VO in the patho-aetiology of ARDS. They also did not recognize the high association of VO with the mortality which was estimated at 60 or 90 days not at the immediate period of 24-48 hours after admission as demonstrated by the above reports [9, 10]. Excellent example of these huge multicenter trials is that study reported by Rowan et al in 2017 [12].
In the results section, Rowan et al reported: “Each study day the liberal-strategy group received more fluid than the conservative-strategy group and on days 1 through 4 had a lower urinary output, resulting in a higher cumulative fluid balance (Table 2). During the study, the seven-day cumulative fluid balance was -136±491 ml in the conservative-strategy group, as compared with 6992±502 ml in the liberal-strategy group (P<0.001) (Figure 1 of the Supplementary Material). For patients who were in shock at baseline, the cumulative seven-day fluid balance was 2904±1008 ml in the conservative-strategy group and 10,138±922 ml in the liberal-strategy group (P<0.001). For patients who were not in shock at baseline, the cumulative fluid balance was −1576±519 ml in the conservative-strategy group and 5287±576 ml in the liberal-strategy group (P<0.001)”
Errors and misconceptions on current FT practice
The errors and misconceptions in current clinical practice and its corrections are documented here. For references on this section please see [5].
Error I
Every arterial hypotension is considered synonymous with hypovolemia or at least treated as such with volume expansion in every clinical case of shock, anesthetic induction, or operative period!
Correction I
Hypotension is not synonymous with hypovolemia. The cause of the primary recognized shock and hypotension must be differentiated. The difference between the therapeutic/physiological VO regarding (quantity versus response) in contrast with the paradoxes of pathological VO on arterial pressure and renal response must be precisely identified. Two paradoxical responses of pathological VO require recognition: one is inducing hypotension shock and the second is causing AKI. The transition from the hypovolemic hypotension shock into the VO hypotension shock during overzealous volume expansion occurs seamlessly unnoticed and undetected by any monitoring until it manifests, later on ICU, with torso edema and increased body weight (BW) of ARDS or MODS.
Error II
The volume-pressure relationship of the vascular system is perceived as infinite strait line!?
Correction II
The volume-pressure relationship particularly that of vascular volume and arterial pressure is a limited line segment, beyond which the relation collapses. Within limits, increasing vascular volume (physiological or therapeutic VO) increases arterial pressure but when such limit is exceeded (pathological VO) a paradoxical hypotension occurs. A similar VO paradox exists on the renal function while physiological VO induces diuresis a pathological VO causes AKI as part of the features of MODS. These two paradoxes are not new but hardly recognized.
Error III
The central venous pressure (CVP) and pulmonary capillary wedge pressure (PCWP) as monitoring parameters guiding fluid therapy are given a value of 18 to 22cm water as currently practiced on many ICUs. Although current recommendations indicate that CVP and PCWP are unreliable and no longer being used, evidence from prevalence of ARDS and MODS on ICU testify differently, and it remain part of its definition. The confounded error underlying the misconception of high positive CVP is related to a deeply rooted physiological error.
Correction III
The given figures of CVP and PCWP are erroneously too high yet remain widely practiced. Persistence to achieve such high CVP using massive volume expansion is among the misleading reasons for inducing pathological VO causing ARDS. The infused fluid rapidly shifts out of the vascular system and CVP may drop back to below 10cm water, then another bolus VO is given before the gross torso edema and increase of BW becomes obvious. The correct CVP figures are given in all physiology textbooks that swing around 0 (at mid-axillary line) with a range of +7 to -7cm water. If we do not understand how Nature works, we must faithfully imitate until reliable methods of monitoring fluid therapy are found.
Error IV
The capillary forces responsible for irrigating and oxygenating the ISF space and cells are mixed up with that causing edema, flooding, and drowning.
Correction IV
It is strongly recommended that every physician involved in fluid therapy, ARDS and MODS management should reconsider what is the physiological function of the arterial and venous pressures and which pressure is responsible for what? In particular relating the pathological ISF accumulation or subcutaneous edema with the forces on which the hypothesis that dictates capillary-ISF transfer on the causation of dropsy, proposed by Starling at the Lancet in 1886, reveals the error. The reason is that the forces on which this hypothesis is based govern the volume and pressure regulation of the vascular and ISF compartments, and subsequently cell viability are incorrect. Being false, this hypothesis underlies most mentioned erroneous concepts on fluid therapy. Starling’s hypothesis was wrongly made later into physiological law. It may be realized that this is the major error responsible for the current dilemma on ARDS and MODS concealing its real patho-aetiology of VO.
Error V
The major misconception, and unfortunately the most prevailing, is wrongly assuming that the vascular system is an all positive pressure system, in which not only the mentioned arterial volume-pressure relationship is misconceived as infinite strait line but also keeping high venous pressure and ISF tissue over-hydrated are erroneously believed to enhance cell nourishment and oxygen delivery. This underlies the liberal volume expansion pumping in too much fluid that creates edema, flooding and drowning of the ISF tissue as well as vital organs and cells! This is precisely the error underlying the pathological VO inducing ARDS and MODS.
In the circulatory system is the arterial pressure seems to be so for very good reason: it is the driving force for ejecting fluid through the capillary orifice creating the side negative energy pressure that drives the dynamic autonomous magnetic field-like fluid circulation between capillary lumen and surrounding tissues - keeping the ISF tissue pressure negative, appearing almost dry, while efficiently irrigated and oxygenated!
Correction V
To assume that CVS to be an all positive pressure system is quite simply wrong. In fact, there is a lot of negative physiological pressure under the skin. It is well known that the pleural spaces have negative pressure and the pressure in alveoli alternates. The CVP of normal subjects may swing around Zero, between positive +7 and negative -7 mmhg [14-16]. The intracranial pressure is also negative. Thus, the ISF space of subcutaneous tissues, most organs and parts of the body have negative pressure of -7 cm water that has been demonstrated [20] and re-affirmed [21] but neither considered nor satisfactorily explained.
Identifying Starling’s law as the culprit dictating the faulty rules causing the errors and misconceptions on FT
The wrong Starling’s law is the culprit dictating the above-mentioned errors and misconceptions that mislead physicians into giving too much fluid during the resuscitation of shock, acutely ill patients, and prolonged major surgery [5]. It was investigated at both physics and physiological fronts. As Starling based his hypothesis on the hydrodynamic of Poiseuille’s tube which is large brass tube of uniform diameter, I constructed the porous orifice G tube us based on the capillary ultra-structure of having a narrow orifice that is the precapillary sphincter and intercellular slit wide pores that allow the passage of plasma proteins thus nullifying the oncotic pressure in vivo. The hydrodynamic of G tube proved totally different from Poiseuille’s tube. The G tube has a side pressure that exert negative pressure on the wall near the inlet and positive pressure near the exit. This creates the unique, rapid magnetic fluid-like circulation between fluid in lumen and fluid around it (Figure 3). Thus, Starling’s law is proved wrong on both of its forces. The G tube phenomenon replaces Starling’s law for the capillary-interstitial (ISF) transfer.
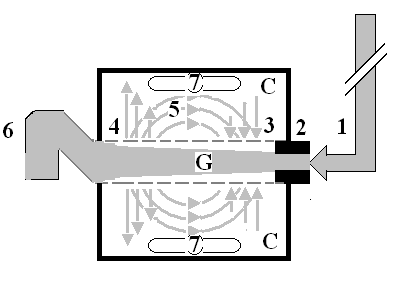
The numbers should read as follows:
1. The inflow pressure pushes fluid through the orifice
2. Creating fluid jet in the lumen of the G tube**.
3. The fluid jet creates negative side pressure gradient causing suction maximal over the
proximal part of the G tube near the inlet that sucks fluid into lumen.
4. The side pressure gradient turns positive pushing fluid out of lumen over the distal
part maximally near the outlet.
5. Thus, the fluid around G tube inside C moves in magnetic field-like circulation (5)
taking an opposite direction to lumen flow of G tube.
6. The inflow pressure 1 and orifice 2 induce the negative side pressure creating the dynamic G-C circulation phenomenon that is rapid, autonomous, and efficient in moving fluid and particles out from the G tube lumen at 4, irrigating C at 5, then sucking it back again at 3,
7. Maintaining net negative energy pressure inside chamber C.
**Note the shape of the fluid jet inside the G tube (Cone shaped), having a diameter of the inlet on right hand side and the diameter of the exit at left hand side (G tube diameter). I lost the photo on which the fluid jet was drawn, using tea leaves of fine and coarse sizes that runs in the centre of G tube leaving the outer zone near the wall of G tube clear. This may explain the finding in real capillary of the protein-free (and erythrocyte-free) sub-endothelial zone in the Glycocalyx paradigm. It was also noted that fine tea leaves exit the distal pores in small amount maintaining a higher concentration in the circulatory system than that in the C chamber- akin to plasma proteins.
The new scientific basis for future guideline recommendations on FT
The G tube hydrodynamic as the correct replacement for the wrong Starling’s law form the scientific bases for future guidelines on the practice of FT. Two other misconceptions on capillary physiology were corrected by the newly discovered tree branching law (under consideration) [13,14]. The two other misconceptions on capillary physiology add to understand the correct model for the capillary-ISF transfer that adequately provide for the cells’ viability at rest and during strenuous exercise.
Therapy of FT complications of VOS and ARDS
Prevention
Being iatrogenic complications of fluid therapy, both VOS and ARDS are preventable.
To prevent VOS and ARDS a limit to the maximum amount of fluid used during shock resuscitation or major surgery must be agreed upon (New guidelines are required).
Surgical care providers must exercise judicious use of crystalloid fluid administration in the trauma bay, ICU, and floor.
Replace the loss in haemorrhagic hypovolemic shocks but do not overdo it.
If hypotension develops despite volume replacement later during ICU stay, inotropic drugs, hydrocortisone 200 mg and hypertonic sodium therapy (HST) should be used-please, see later. The latter restores the pre-capillary sphincter tone (peripheral resistance) so that the capillary works as normal G tube again, but NO isotonic crystalloids or colloids over-infusions is required.
To learn the new correct science, one must unlearn the old incorrect habits.
The following practices should be abandoned:
A. Bolus fluid therapy in surgical patients
B. Abandon the aggressive current liberal regimen of Early Goal-Directed Therapy (EGDT) in treating shocked and septic patients [26]. Multiple huge multicenter trials have proved it to be the wrong practice.
C. Please refrain from persisting to elevate CVP to levels above 12 and up to 18-22 cm saline in shock management. This is a major cause for inducing VOS and ARDS during shock resuscitation, particularly septic shock.
Therapeutic
Hypertonic sodium therapy (HST) of 5%NaCl and/or 8.4%NaCo3 has truly proved lifesaving therapy for the TURP syndrome and acute dilution HN as well as secondary VOS 2 that complicates fluid therapy of VOS 1 causing ARDS. It works by inducing massive diuresis being a potent suppressor of antidiuretic hormone. It may also work on the pre-sphincter capillary restoring its tone.
My experience in using it for treating established ARDS with sepsis and primary VOS 2 that causes ARDS is not tested. However, evidence on HST suggests it will prove successful if given early, promptly and adequately to ARDS patients while refraining from any further isotonic crystalloid or colloid fluid infusions using saline, HES and/or plasma therapy- just give the normal daily fluid requirement and no more. After giving HST over one hour using the CVP catheter already inserted, the patient recovers from AKI and produces through a urinary catheter massive amount of urine of 4-5 liters as you watch. This urine output should not be replaced. Just observe the patient recovering from his AKI, coma and ARDS and asks for a drink. This is done in addition to the cardiovascular, respiratory, and renal support on ICU. Patients with AKI on dialysis, the treating nephrologist should aim at and set the machine for inducing negative fluid balance.
The HST of 5%NaCl and/or 8.4%NaCo3 is given in 200 ml doses over 10 minutes and repeated. I did not have to use more than 1000 ml during the successful treatment of 16 ARDS patients. Any other hypertonic sodium concentration is not recommended. A dose of intravenous diuretic may be given but it does not work in a double or triple the normal dose. A dose of 200 mg of hydrocortisone is most useful. Antibiotic prophylactic therapy is given in appropriate and adequate doses to prevent sepsis and septic shock. No further fluid infusions of any kind crystalloids, colloids and blood is given. The urinary loss should not be replaced as this defeats the objective of treatment.
A suggested recommended future trial urgently needed
I would recommend a small pilot prospective controlled cohort study on 100 patients as a start to try HST in established ARDS cases that would be something to look forward to reading a report on it, hopefully soon. No multicenter trial or high expenses is needed for that. Not much time is required either. If you cannot do it on a hundred patients, you probably cannot (as Mr. JP Ward put it to me before the start of our prospective study [19]. I can assure the investigators that no harm will come to patients. It is a guaranteed win bit; you may win but you do not lose anything. In the worst-case scenario, the patient may not respond because of chronicity of ARDS or after sepsis complicates ARDS and gets the capillary damage established. As the author of all self-referenced articles here, published in open access journals, and as copyright holder I give open permission to any interested investigator to use any of my articles as template, particularly recommended article [19]- the appropriate permission from the editors of BJUI and authors are given. I strongly recommend that hypertonic sodium therapy should be given a trial in the management of ARDS of both sepsis and Covid-19 as it may prove to be my successful positive contribution to the war against the Covid-019 pandemic.
Conclusion
Both VOS and ARDS are iatrogenic complications that remain overlooked and underestimated. The reason for that is the new VOS complicates the shock being treated with fluid therapy and difficult to detect and recognize. The massive use of FT is not the treating physician’s fault. Hence all physician find it offensive to label as fluid overload. Physicians are being mislead by the faulty rules on FT causing many errors and misconceptions that lead to massive fluid retention during shock resuscitation. This VO induces VOS and cause ARDS.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
