AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Z. Pawlak, Kazım Dirik Mah. Mustafa Kemal Cad. Hakkıbey apt. No: 45 D.10 35100 Bornova-İzmir, Turkey.
Citation: Volkan S. Erikci. (2021). Etıology and Management of Lower Gastroıntestınal Bleedıng ın Neonates: A Revıew Artıcle. J. Clinical Research and Reports, 9(4); DOI:10.31579/2690-1919/210
Copyright: © 2021, Volkan Sarper Erikci. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 October 2021 | Accepted: 30 November 2021 | Published: 13 December 2021
Keywords: lower gastrointestinal bleeding; neonates; etiology; LGIB; epidemiology; NEC
Lower gastrointestinal bleeding (LGIB) in neonates is occasionally encountered in clinical practice. There are various causative factors prodicing LGIB in neonates and the babies are usually managed with regard to the underlying pathology that produces LGIB. Although majority of these bleeding episodes is self limited, certain neonates with LGIB may necessitate prompt management including urgent surgical intervention. In this review article it is aimed to review the etiology, epidemiology, clinical manifestations and principles of treatment of LGIB in neonates under the light of relevant literature.
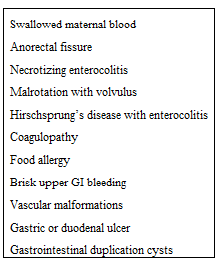
Gastrointestinal tract is highly vascularized organ with a large surface area. Different pathological states can produce gastrointestinal bleeding. LGIB refers to bleeding distal to the ligament of Treitz which is located at the duodenojejunal junction [1]. LGIB in neonates and infants is commonly encountered in clinical practice [2-6]. In a previos report, of the patients presenting to emergency department with a complaint of rectal bleeding, approximately one-third have LGIB and the remainder have an upper gastroinestinal bleeding [7]. Annual incidence of LGIB in children is 6.8 cases per 10.000 hospital discharges in the USA [8]. According to qualitative characteristics of the stool LGIB can be seen as hematochezia, melena or occult gastrointestinal bleeding. Hematochezia refers to bright red blood in stool and is commonly regarded as a suggestive finding of LGIB. Melena is a black and tar-like stool and is usually a finding of upper gastrointestinal bleeding. Occult gastrointestinal bleeding is not visible by eye and usual etiological factor in these children is iron deficiency anemia. In this report it is aimed to review the causes of lower gastrointestinal bleeding and management strategies in neonates with LGIB and a brief literature review is given. In the following parts of the article the most common diagnoses to consider in newborns presenting with LGIB are given in table-1 together with management options.
This is a common etiological factor in neonates presenting to hospital with complaint of LGIB. The rectal blood in these cases comes from mother. Usual reason for this is the swallowing of mother’s blood by neonates during delivery or ingestion of mother’s blood coming from cracked nipples during breast feeding. Apt test (hemoglobin alkaline denaturation test) is helpful in the diagnosis of swallowed maternal blood. The test depends on the chemistry rule that infant HbF resists denaturation with alkali better than adult HbA. Indicative finding in this test is that adult Hb changes in color from pink-red to brown-yellow within 2 minutes while fetal HbF resists denaturation and preserves its pink color. If the Apt test is inconclusive for swallowed maternal blood, a spectrophotometric assay can be used to measure the color change and HbF ˃ 50 percent is indicative for fetal blood and HbF ˂ 10 percent for maternal blood [9]. If the LGIB is determined to be swallowed maternal blood no additional investigation or treatment is required [10].
Although during the first 2 years anal fissure is the most important source of rectal bleeding, it is less common in neonates. If a neonate presents with anal fissure trauma secondary vigorous wiping, rectal interventions such as glycerin suppository insertion, thermometer related injury or rectal irrigations should be considered. The lesion in anal fissure is usually located below the dentate line posteriorly. Sitz baths with topical therapy including local antibiotics and analgesics is all that is needed during the management of these neonates.
Necrotizing enterocolitis (NEC) is an acute illness associated with various etiological factors end result of which may be intestinal necrosis leading to catastrophic outcomes and even death. If a neonate with LGIB presents with systemic signs like apnea, respiratory failure, lethargy, poor feeding or temperature instability, abdominal signs of distention, gastric retention, vomiting and diarrhea NEC should be kept in mind for the causative factor for LGIB. Most of these infants are prematures with low birth weights. Characteristic features of NEC in direct roentgenograms include abnormal gas pattern and ileus. Pneumatosis intestinalis is the hallmark finding of NEC showing intestinal subserosal gas collection. Depending on the stage of NEC, medical treatment should be commenced immediately including iv fluid and electrolyte replacement together with systemic antibiotics. In advanced disease states surgical intervention may also be necessary.
These neonates typically present with abdominal distention, emesis and LGIB in the form of melena or hematochezia. Emergent evaluation and treatment is important for avoidance of life-threatening consequences of the disease itself. LGIB is occasionally seen in these cases (10-20 percent of cases). Upper gastrointestinal series and especially in experienced hands color Doppler ultrasonography may be helpful in diagnosing these children with malrotation. The treatment of LGIB due to malrotation in neonates necessitates to treat underlying pathology, namely malrotation with volvulus. Urgent treatment is life saving because this entity is one of the etiological factors of small bowel syndrome which is frequently seen especially following extensive intestinal resection for midgut volvulus with malrotation.
Most of these neonates frequently have delayed passage of meconium longer than 48 hours after birth. Some other present with acute obstruction associated with bilious or feculent vomiting. Bleeding in the stool may be occult but if the disease worsens due to delayed treatment melena or hematochezia may also be seen. If a neonate with Hirschsprung disease has significant blood in the stool with abdominal distention, Hirschsprung associated enterocolitis should be considered and an emergent medical therapy including decompression of rectum by rectal tube insertion for evacuation and irrigation of rectosigmoid colon, intravenous fluid and electrolyte replacement with appropriate antibiotics should be promptly commenced. In advanced cases emergency surgical interventions should also be necessary.
Most of these neonates present with bleeding symptoms including large cephalohematoma, oozing from umbilical stump, prolonged bleeding after circumcision or blood sampling or intracranial hemorrhage in a term infant [11]. As also called hemorrhagic disease of the newborn coagulopathy results from a lack of vitamin K. Since routine vitamin K administration after birth is usually performed, hopefully this condition is rarely seen today. Other causes of coagulopathy that result with LGIB in neonates include hematological disease states like hemophilia, von Willebrand disease. These neonates should be managed by treating underlying disease that ends up with coagulopathy.
This is one of the most common causes of LGIB in neonates and infants [12]. Etiological factors responsible for LGIB in these infants with food allergy include food-induced enterocolitis syndrome, food-induced colitis and allergic eosinophilic gastroenteritis [13]. The classic symptoms of infants with cow’s milk allergy include protracted vomiting, bloody diarrhea. In severe cases protein-loosing enteropathy and failure to thrive may be observed. The disease is usually self-limited and resolves within 6-18 months of age.
Other causes of LGIB in neonates are brisk upper gastrointestinal bleeding, vascular malformations, gastric or duodenal ulcers and gastrointestinal duplication cysts. As mentioned before LGIB related to any of these illnesses should be managed by getting rid of causative factors that produce blood in the stool.
In conclusion, LGIB in neonates can be sudden but more often subtle requiring extensive evaluation to identify causative factor. LGIB can cause stress for parents, care givers or even physicians dealing with these babies. Although most of these bleeding episodes is self-limited, a systematic approach for focusing the underlying source and a prompt management including surgical intervention may be life saving in these children. Physicians should keep causative factors in their minds when they face infants with LGIB and a rapid pediatric surgical consultancy is recommended. The neonates with LGIB should be treated accordingly.
The author certifies that he has no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
During this study, no financial or spiritual support was received neither from any pharmaceutical company that has a direct connection with the research subject, nor from a company that provides or produces medical instruments and materials which may negatively affect the evaluation process of this study.
Idea/concept, design, control and processing, analysis and/or interpretation, literature review, writing the article, critical review, references and materials by Volkan Sarper Erikci.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.









































