AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Gómez Barriga Maria Dolores, Cardiology Unit Supervision, Hospital Clínico San Carlos. San Carlos Research Foundation, San Carlos Health Research Institute (IDISSC). Calle Martín Lagos s/n (no number), 28040 Madrid, Spain. ORCID: 0000-0001-5973-0823
Citation: Gomez Barriga, MD, Pacheco Del Cerro, E., Fernández Del Palacio, E., Vila Costa, I., (2024), Empowerment Analysis in Patients with Acute Coronary Syndrome and Heart Failure in Hospitalization Units: A Cross-Sectional Study, J Clinical Cardiology and Cardiovascular Interventions, 7(6); DOI: 10.31579/2641-0419/377
Copyright: © 2024, Gómez Barriga Maria Dolores. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 April 2024 | Accepted: 23 May 2024 | Published: 31 May 2024
Keywords: empowerment; chronic diseases; heart failure; acute coronary syndrome; nursing; healthcare context; share experiences; managing disease; emotional issuses; social spheres
Aim: To evaluate the empowerment of patients diagnosed with Acute Coronary Syndrome (ACS) and Heart Failure (HF) admitted to a Level III hospital.
Material and Methods: An observational cross-sectional study conducted over a sufficient period to collect the sample. The study population includes patients admitted to a Level III hospital in cardiology units, diagnosed with Heart Failure or Acute Coronary Syndrome. Inclusion criteria consist of diagnosis of Heart Failure or Acute Coronary Syndrome and consent to participate in the study. The main variable used is the CEPEC questionnaire (Chronic Patient Empowerment Questionnaire), in its shortened version with cross-cultural validation, developed by Dr. Garcimartín.
Results: The Chronic Patient Empowerment Scale (CEPEC) was used. The data indicated a total of 81 men and 39 women, with 37 patients having HF and 84 with ACS. The age range was 50 to 55 years, with more patients below 65 years. The CEPEC scale had a Cronbach's alpha of 0.764. There was a significant age difference (p <0.05) between the two units under study. For each diagnosis, scale items were compared, revealing statistical differences in items P-5, P-15, and P-24.
Conclusions: The scale has proven to be valid and reliable, providing indicators of poor or inadequate patient progress. These circumstances enable the development of precise actions to enhance the situation and quality of life for hospitalized patients.
Höfer et al contributed to the assessment of the quality of life in patients with cardiac diseases, based on concepts relevant to their study and ours. The measurement of health includes not only an indication of changes in the frequency and severity of the disease but also in the patients' perception of health before and after treatments. They assert that the patient's perspective is as legitimate and valid as that of the clinician in monitoring outcomes. [1]
Discussing chronic diseases is relatively clear for healthcare professionals, but the inclusion of conditions considered chronic that influence morbidity and mortality can be more delicate. In order to provide more appropriate management and healthcare for each individual, various types of studies have been conducted. In a comprehensive literature review, it is evident that terms with significant variability are used, depending on the location, type, person, and disease.[2]
Chronic conditions could be defined as having an expected duration of at least six months, understanding that the definition of time alone is not the sole criterion for classifying a health condition as chronic.[2] Other factors include an unfavorable prognosis, consequences or sequelae impacting the quality of life, and a recurrent or worsening pattern. .[2]
Studies have also been published on lifestyle-related diseases, including chronic conditions that are accompanied by changes in the patient's daily lifestyle and habits. Within lifestyle factors, the primary focus is on physical inactivity, poor nutrition, insufficient sleep, high levels of stress, substance use, and social isolation. .[3]
Empowerment has been studied in numerous patients with different diseases and characteristics. The research suggests that empowerment improves the quality of life, particularly in patients with chronic heart failure, enhancing autonomy, self-esteem, satisfaction levels, and reducing healthcare costs. Due to these findings, it is recommended to use validated instruments for measuring patient empowerment. .[4]
Indeed, understanding patient empowerment is considered a valuable aid for patients in managing their health effectively and achieving better outcomes. However, assessing empowerment requires specific empowerment measures, which, in the case of chronic diseases, have not been fully developed. One approach to addressing this gap is to establish systems for measuring empowerment.[5] Small et al. have developed an empowerment questionnaire that covers all the necessary aspects for patients to actively participate in their own health situations. .[5]
Previously, Varekamp et al. in 2009 noted that in healthcare, empowering patients with chronic diseases aims to increase their knowledge and skills. This empowerment enables patients to define objectives and take on responsibilities for their treatment. .[6]
Patient empowerment is a key concept embedded in various models of chronic care. Providing care to a chronic patient necessitates empowerment, with the patient taking responsibility for their own healthcare. This empowerment is crucial for improving health status, preventing complications, and enhancing overall quality of life.[7]
The concept of empowerment has extended to the community level. Increasing community empowerment aims to interconnect health promotion, social change, building social capital, and the distribution of power. These factors are reflected in the overall quality of health in the population.[8]
In 2019, a transcultural adaptation of Small et al.'s empowerment scale was conducted, following a clear and precise methodological process, conceptually very appropriate. The questionnaire derived from the "Empowerment of the Patient in Chronic Conditions" is semantically and conceptually equivalent to the original tool, with the acceptance of the original version's author.[9]
This brief overview of the elements that constitute the situation of patients admitted with Cardiovascular Diseases (CVD), along with the theoretical and clinical aspects of a measure of the patient's situation encompassing all circumstances influencing their quality of life, has led us to formulate the following objective: To assess the empowerment of patients diagnosed with Acute Coronary Syndrome and Heart Failure, admitted to a Level III hospital.
An observational cross-sectional study conducted over a sufficient period to collect the sample.
Study population consists of patients admitted to a Level III hospital in the cardiology units, diagnosed with Heart Failure or Acute Coronary Syndrome.
Whether a patient is admitted to one unit or the other depends on bed availability. Therefore, the medical professional deciding to admit a patient will choose one unit over the other based on the availability of free beds.
The total number of patients, based on the reference from the previous year at the same time, calculated for a 95% confidence interval and a precision of ±2, is a total of 120 patients. Given the unit characteristics, the patient ratio is 3:1, three in the second-floor unit to one in the seventh-floor unit.
Inclusion criteria for patients are a diagnosis of Heart Failure or Acute Coronary Syndrome and having given consent to participate in the study.
The variables used, primarily the CEPEC questionnaire (Chronic Patient Empowerment Questionnaire), in its shortened version with cross-cultural validation, by Dr. Garcimartín [9], It can be seen in Table I.
| 1 | I continue to engage in interesting activities in my life despite my health problems. | 1
| 2 | 3 | 4 | 5 |
| 2 | I am capableof taking chargeof my illness. | 1 | 2 | 3 | 4 | 5 |
| 3 | I am optimistic about my illness. | 1 | 2 | 3 | 4 | 5 |
| 4 | I have helpedpeople with similarillnesses as mineto find different ways to cope with the situation. | 1 | 2 | 3 | 4 | 5 |
| 5 | My health problems prevent me fromenjoying life. | 1 | 2 | 3 | 4 | 5 |
| 6 | I can decrease the impact of symptoms on my dailylife. | 1 | 2 | 3 | 4 | 5 |
| 7 | I have sharedmy experience of taking chargeof my illness with other peoplewith health problems. | 1 | 2 | 3 | 4 | 5 |
| 8 | I know whereto go to determine more about my illness. | 1 | 2 | 3 | 4 | 5 |
| 9 | I have plansto do enjoyable things despite my illness. | 1 | 2 | 3 | 4 | 5 |
| 10 | I have a sense of control overmy illness. | 1 | 2 | 3 | 4 | 5 |
| 11 | Despite my healthproblems, I feel that I have a good quality of life. | 1 | 2 | 3 | 4 | 5 |
| 12 | I have information to handle difficulties related to my illness. | 1 | 2 | 3 | 4 | 5 |
| 13 | I have sharedwith others whatI do to stay well. | 1 | 2 | 3 | 4 | 5 |
| 14 | I have the skills that help me feel in control of my illness. | 1 | 2 | 3 | 4 | 5 |
| 15 | I feel usefulin my daily life despite my illness. | 1 | 2 | 3 | 4 | 5 |
| 16 | I can talk to my doctor if I changemy mind aboutmy treatment. | 1 | 2 | 3 | 4 | 5 |
| 17 | I can livea normal lifedespite my illness. | 1 | 2 | 3 | 4 | 5 |
| 18 | I feel confident in choosing withmy doctor amongdifferent options relatedto my illness. | 1 | 2 | 3 | 4 | 5 |
| 19 | I feel actively engaged in lifedespite my healthproblems. | 1 | 2 | 3 | 4 | 5 |
| 20 | I have sharedmy knowledge aboutmy illness with people who have similar conditions. | 1 | 2 | 3 | 4 | 5 |
| 21 | I participate in decisions that affect my health care. | 1 | 2 | 3 | 4 | 5 |
| 22 | I know how to handledifficulties related to my illness. | 1 | 2 | 3 | 4 | 5 |
| 23 | I try to make the most of my lifedespite my illness. | 1 | 2 | 3 | 4 | 5 |
| 24 | I understand my illness. | 1 | 2 | 3 | 4 | 5 |
| 25 | I have a positive outlookon my illness. | 1 | 2 | 3 | 4 | 5 |
| 26 | There are peoplewith a similar illness who ask me for advice. | 1 | 2 | 3 | 4 | 5 |
| 27 | I have all the knowledge I needto take chargeof my illness. | 1 | 2 | 3 | 4 | 5 |
| 28 | I know how to managemy health problems. | 1 | 2 | 3 | 4 | 5 |
| 29 | I have sufficient knowledge about my illness. | 1 | 2 | 3 | 4 | 5 |
| 30 | I feel thatmy life haspurpose and meaning despite my healthproblems. | 1 | 2 | 3 | 4 | 5 |
1- StronglyDisagree, 2 – Disagree, 3 – Neutral,4 – Agree, 5 - Strongly Agree
Table I. Chronic Illness Empowerment Scale (CEPEC); N. Small (Garcimartín Cerezo 2018a) (Garcimartin et al. 2019) developed a scale to measure empowerment in chronic patients; In Spain,Garcimartín, P. validatedthe cross-cultural adaptation of Small's scale (Garcimartín et al. 2019).
According to Garcimartín's data, a score on the questionnaire below 50 points indicates very low patient empowerment, while a score equal to or higher than 130 identifies good patient empowerment. The maximum score on the questionnaire is 146. Each scale item has five response options: 0-Strongly Disagree, 1-Disagree, 2-Neutral, 3-Agree, 4-Strongly Agree.
In the original scale developed by Small [5], In the original scale developed by Small, it had 47 items and three factors. In the reduced and transculturally validated scale, it has two factors and 30 questions. The dimensions are defined as follows: Factor 1: "Positive Attitude and Sense of Control" refers to changes experienced by patients in terms of self-perceptions after diagnosis and how patients reduce the impact of the disease on their lives, resulting in increased self-control. Factor 2: "Knowledge and Confidence in Decision Making" is related to patients reporting having enough knowledge and understanding to manage their condition and participate adequately in decision-making with healthcare professionals. Factor 3: "Enabling Others" refers to a set of elements related to involvement and integration with other individuals.
In the study, secondary variables related to the patient and hospitalization were collected. These variables included the patient's name, gender, age, hospital identification number (medical record number), date of admission to the hospital unit, discharge date, length of stay in the hospital, and the medical diagnosis at admission. The latter variable is related to the inclusion criteria in the study and the definition of the chronic disease condition.[5]
The age variable has been grouped into seven ranges, each covering a five-year period, with the first range being 45 to 50 years old and the last range being 70 to 75 years old.[5]
The data, measuring the variables for each patient, from both the second north hospitalization unit and the seventh north unit, were collected by the same person to ensure consistency in data collection and criteria.
Statistical Analysis:
The data were analyzed by presenting values and frequencies for all variables. Means and standard deviations were calculated for parameters with a normal distribution, while the median and interquartile range were calculated for those without a normal distribution. The chi-square test was used to assess associations in categorical variables, and paired t-tests were used for continuous variables. A multivariate factor analysis was conducted on the CEPEC questionnaire. The data were analyzed using IBM SPSS Statistics (Version 29). Missing data lead to the exclusion of the patient from the study, and according to the sample size calculation, a new patient meeting the inclusion criteria will be included.
The Red-Cap® system is used to collect data, which includes health, biometric, and personal data such as age and gender. The data will be pseudonymized to comply with legislation. Each patient will receive an identification code. Only the Principal Investigator (PI) and authorized collaborators will have access to the data. Data ownership belongs to the PI. The data will be deposited in the institutional repository of the Health Department of the Community of Madrid. Compliance with ethical and legal requirements is ensured, including approval from the Clinical Research Ethics Committee of the Hospital Clínico San Carlos and compliance with the GDPR and Organic Law 3/2018. Participants have rights to access, rectify, oppose, and delete data, as well as data portability and processing limitation. The study protocol has been reviewed and has received a favorable report from the CEIm of the Hospital.
The study was conducted from October 1 to December 31, 2022, based on the defined inclusion criteria and a 3:1 ratio in the hospitalization units of the second north and seventh north, related to the number of beds in the two hospitalization units and therefore the number of patients in each. The patient admission tree to the hospitalization units, the application of the criteria, and thus the evolution of the number in each hospitalization unit can be seen in Figure 1.
The data for secondary variables can be seen collectively in Table II.

A total of 120 patients were recruited during the last quarter of 2021, with a distribution of 90 cases (74.4%) admitted to the second north unit and 30 admitted to the seventh north unit. Of the total, 81 were male (66.9%) and 39 were female (32.2%). Regarding the admission diagnoses included in the study, 37 patients had Heart Failure (30.6%), and 84 patients (69.4%) suffered from Acute Coronary Syndrome.
The age range with the most admitted patients is 50 to 55 years, accounting for 28.9% of the total. The percentage of patients admitted aged 65 years or younger is 64.6%, and patients aged over 65 years is 35.7%.
A factor analysis of the CEPEC scale is conducted to confirm or deny its validity and reliability. A principal component analysis is performed, resulting in a Cronbach's alpha of 0.794. The removal of each item does not substantially alter the Cronbach's alpha value, with the lowest being 0.764. The intraclass correlation of average values is 0.779 (CI: 95%, 0.716-0.833). The most significant difference obtained is the definition of 10 components, factors, whereas in the original table, there were 2. These 10 components explain 66.942% of the variance.
The mean score for the overall assessment of the scale is 77.02 empowerment points, with a standard deviation of 10.581.
In the grouping of questionnaire factors, the elements are distributed in Factor 1 with elements 2, 6, 8, 10, 12, 14, 16, 18, 21, 22, 24, 27, 28, and 29; in Factor 2 with elements 1, 3, 5, 9, 11, 15, 17, 19, 23, 25, 30; and in Factor 3 with elements 4, 7, 13, 20, 26. (see Table I for element identification)
The distribution of each element in the scale, as seen in Table I, can be observed in Table III.
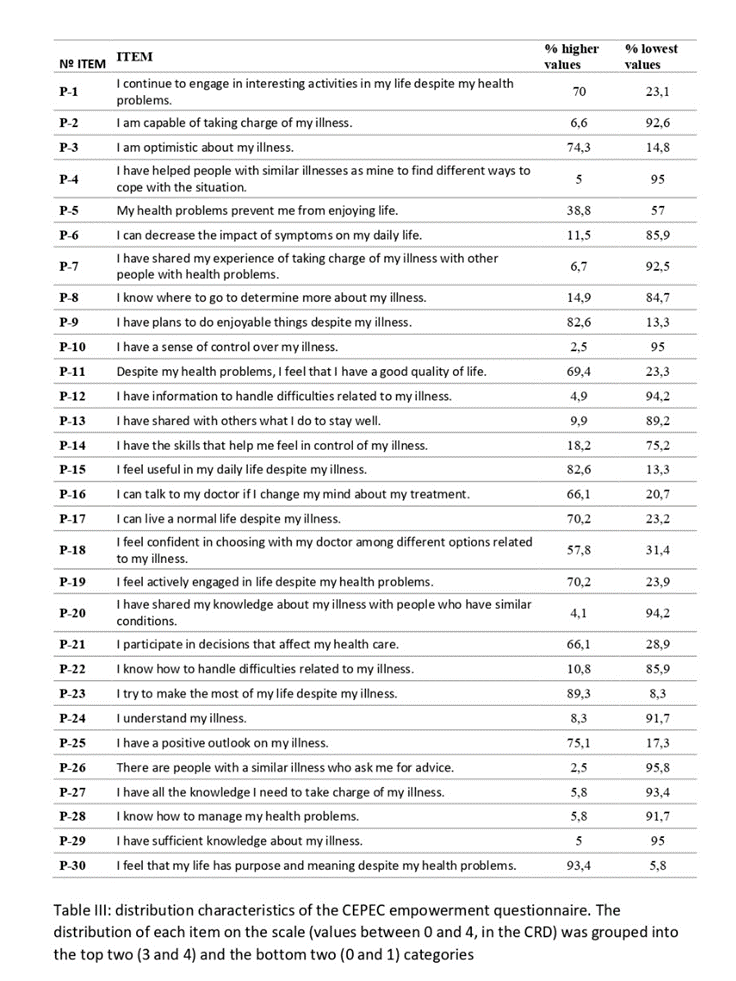
The elements of the scale that have a low score (values between 0 and 1) and higher values (3 and 4) are grouped. In Table III, the percentage of responses after grouping into high and low ratings can be observed. The shaded elements in the low-value percentage column have a percentage equal to or greater than 70% of the patients, indicating that these elements are deficient in the studied patients.
As observed, most elements of Factor 1 and all elements of Factor 3 have a low or very low rating in the majority of patients.
The relationship between variables was analyzed using the Chi-Square test. Differences in age between the two admission units in the study were analyzed, resulting in a p-value <0>
Differences in the distribution of patient diagnoses at admission were analyzed, identifying a higher number of patients with Acute Coronary Syndrome than patients with Heart Failure. The statistical analysis using the Chi-Square test provides a p-value <0>
The comparison of sex with the diagnosis did not show a statistically significant difference between the two variables (Chi-square 2.814, p <0>
Each unit was compared with the items of the CEPEC scale, and statistically significant differences were found with items P-2 (p <0>
The total score of the CEPEC scale was compared between patients admitted to the two comparison units, and no statistically significant difference was found.
Admission diagnoses were analyzed with each element of the scale, revealing statistically significant differences with item P-5 (p <0>
Sex was also compared with each item of the scale, and a statistically significant difference was found with item P-2 (p <0>
Age ranges were compared with the items of the scale, and a difference was found in item P-30 (p <0>
The combination of admission diagnosis and age ranges was compared with the items of the scale, revealing a statistically significant difference between Acute Coronary Syndrome, age range, and item P-7 (p <0>).
For many years, there has been a focus on studying the possibility of having a tool capable of identifying the situation and progression of patients with chronic diseases and their quality of life.
The author who conducted the transcultural adaptation of the scale used[7], she stated that managing chronic conditions requires an empowered patient who actively participates and takes responsibility for their care with the goal of improving health outcomes, preventing complications, and enhancing their quality of life.
It is necessary to analyze the coincidence and development of knowledge about chronic diseases, as there has been a significant evolution and alignment. Articles have been published that highlight the lack of clarity in the concept of chronic diseases in the primary care setting[2] Haga clic aquí para escribir texto., leading to confusion in patient monitoring. However, some authors already incorporate clinical situations related to lifestyle, such as chronic diseases, which share common risk factors[3], like physical inactivity, poor diet, insufficient sleep, high levels of stress, substance use, and social isolation.
The aspects of chronic diseases can be related to the cost of care, as indicated by the study by Conthe[7], which shows a 70% increase in this cost, mainly due to patient rehospitalizations. We can deduce that patients in our study, with heart failure and acute coronary syndrome, who are chronic patients, have impaired quality of life and may be caught in a cycle of rehospitalizations.
All these aspects must be related to therapeutic adherence. Everyone agrees that adherence is a public health issue, and its lack has a prevalence of 50% in patients with chronic diseases [11].
Starting from scientific results, both healthcare professionals and policymakers agree that empowerment is a mechanism to assist patients with chronic diseases in managing their health and achieving better outcomes[5]. Many studies have been conducted to measure empowerment and identify altered situations in patients.
Several questionnaires are developed to measure patient empowerment, utilizing different approaches or lines of development. However, they all agree on the multifactorial nature of empowerment [12] as reflected in the factors (components) of each questionnaire.
In our study, we used the transculturally adapted questionnaire developed by Garcimartín[9]. The validity obtained was 0.794; however, the author's data was 0.9. When compared to HECQ[12] they obtained a value of 0.83, and the data from the MacNew 1 questionnaire is 0.92 in the English version and 0.88 in the Spanish version.
In our case, it may be due to the fact that the main objective of the study was not to analyze the validity and reliability of the questionnaire. We started with a sample size that was not excessively large and was not assessed based on the disease leading to admission, including both patients with Heart Failure and Acute Coronary Syndrome. However, in all cases, including ours, very consistent validity data were obtained, allowing for the effective use of the questionnaire.
The factorial analysis indicates that the grouping into three factors (components) is explained by a variance ranging between 63% for Factor1, 68% for HECQ1[2], and 67% for the one we utilized. However, the factors cover distinct domains. The MacNew questionnaire follows the original approach, resulting in factors related to the physical, emotional, and social spheres. The HECQ questionnaire defines three factors: Decision-making involvement, Interaction involvement, and Degree of control. The one we used yields the same factors as Small's extended original scale[5], namely: changes experienced by patients after diagnosis, the impact of the disease on their life, and shared decision-making. The second factor relates to the impact of the disease on their life, while the third pertains to the ability to seek information outside the healthcare context, share experiences, and strategies for managing the disease with other patients. This presentation of factors suggests that the one we used essentially separates the factors influencing a patient with a chronic disease. However, it also maintains a degree of interrelation between them, as reflected in the defined factors.
Studies have been conducted, focusing on the unique characteristic of the population: healthcare professionals with chronic diseases [6], In these studies, seven themes have been identified as areas where actions should be taken to empower healthcare professionals for their well-being.
Studies have been conducted on patients, focusing on partial aspects to identify their influence on quality of life, adherence, or, as in our case, empowerment. It is clear that cardiac rehabilitation provides patients with a level of knowledge, self-esteem, and self-confidence not achieved by other methods. However, specific aspects have been studied, [13] such as the incorporation of a psychoeducational intervention alongside exercise. Patients subjected to this scheme showed significant improvements. Similarly, but with differences in interventions, studies have included individual education, both hospital-based and primary care-based. Excellent results were observed in patient satisfaction, reflected in high motivation and adherence, as well as increased knowledge and self-care capacity [14]. Cardiac rehabilitation affects physical, social, and emotional dimensions, and nursing plays a role by applying tools to modify the perception of quality of life[15].
It is important to highlight psychological studies, interventions, or psychological issues related to patients with cardiovascular disease. Psychological well-being and its relationship to participation in secondary prevention actions have been examined 16], It was observed that patients with positive relationship alterations were less likely to engage in secondary prevention programs. The effects of cognitive-behavioral therapy on morbidity and mortality in cardiovascular patients were studied, revealing that these actions decrease the risk of disease recurrence [17]. Positive psychological effects have also been studied, indicating that optimism and positive affect improve engagement in physical activity and healthy eating [18]. The influence of using coaches with patients has been investigated, showing that they have a higher likelihood of achieving clinical goals and improving analytical results of hemoglobin A1c and LDL in coach-assisted groups.[19]
Psychological aspects derived from cardiovascular disease have also been studied. Cognitive impairment in patients with coronary syndrome has been examined, defining that these patients experience mild cognitive decline, which may worsen if associated with depression or anxiety [20]. Similarly, it has been confirmed that patients with coronary syndrome presenting to the emergency department may develop symptoms of post-traumatic stress. The presence of these symptoms may lead to a heightened perception of cardiac threat[21].
Similarly, engaging in exercise has proven to be highly effective in the progression of a patient with cardiovascular disease. A study on running and its association with mortality in cardiovascular patients concluded that running even just once a week is better than not running at all [22]. The impact of physical limitations has also been studied in a similar manner. Patients with acute coronary syndrome experiencing physical limitations influence their perception of quality of life, vitality, emotional role, and social adaptation [23].
The identification of questionnaire elements and their relation to factors has a direct connection to the actions to be taken to improve the patient's situation. Various types of interventions have been identified to enhance the patient's empowerment level, including educational, cognitive-behavioral, and combined interventions [4]. Nursing staff has already utilized educational interventions that partially impact the quality of life. In a heart failure nursing consultation, 78% of patients showed improvement in risk factors, except for hyperglycemia and overweight, where the impact was less pronounced [24].
The remaining analyses, including weight, gender, and age, do not reveal differences compared to the already known data.
Methodological Biases exist:The sample size is limited for the intended purpose of the study; a preliminary sample survey should have been conducted, followed by a definitive calculation of the sample size. Other variables, as suggested by cardiology studies, should have been incorporated, such as whether it is the patient's first admission, length of stay, among others.
The CEPEC scale for patient empowerment with chronic diseases, validated by Garcimartín in 2018, has undergone further validity and reliability analysis in our context. Its validity has been confirmed with a Cronbach's alpha of 0.794. The scale, with its factors, precisely profiles us, indicating aspects where the patient and their disease are not perceived favorably.
There are no conflicts of interest among the authors of the work
The study has not received any funding
The data has been obtained following the data protection and patient privacy law and endorsed by the Ethics Committee for Research at the Hospital Clínico San Carlos, with the approval of the study protocol.
Of the authors, two have specialized training in statistics. Specifically, Professor Pacheco del Cerro, Enrique, has conducted the analysis.
Affirm that methods used in data analyses are appropriately applied within the study design. Agree to take responsibility for the statistical approach's appropriateness, conduct, and interpretation.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
