AUCTORES
Globalize your Research

Research article
*Corresponding Author: Si Ahmed Hakim, Neurology department, University Hospital of Tizi-Ouzou, Algeria
Citation: Si Ahmed Hakim, Daoudi Smail (2023) Dysimmune Encephalitis: Study of An Algerian Population. J. Brain and Neurological Disorders. 6(2): DOI:10.31579/2642-973X /048
Copyright: © 2023 Si Ahmed Hakim. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 January 2023 | Accepted: 18 February 2023 | Published: 27 February 2023
Keywords: limbic encephalitis; anti-nmda; anti-caspr2; anti-lgi1
Introduction
Autoimmune encephalitis is a new and little-known entity targeting CNS antigens. It often causes inflammatory limbic encephalitis, for which immunotherapy is effective.
Objective
The main objective of the study is to determine the clinical and paraclinical characteristics of encephalitides associated with NMDAr, CASPR2 and LGI1 antibodies.
Materials and methods
It is a descriptive, prospective and retrospective study, which started from January 2016 to December 2018.
Results
Our cohort included 30 patients with a mean age of 44 ± 18.05 years. The limbic encephalitis was acute in 73.3%. The patients presented mainly psychiatric and vigilance disorders, epileptic seizures, dysautonomia, and memory disorders. A temporal hyper signal (± extra limbic) was often found on MRI, with non-specific abnormalities in the EEG and an inflammatory CSF profile. FBDS, dyskinesias, and neuromyotonia were the discriminating signs. Neoplasia was found in 16.7% of the cases. Immunotherapy led to good results.
Conclusion
This study aimed to know how to identify these entities in our country and establish an early and effective treatment for better outcomes. A study with large samples would be more beneficial.
Autoimmune or dysimmune encephalitis is a rare entity, and its precise incidence and prevalence are unknown [4]. Autoantibodies bind antigens in the neuronal cell-surface of the central nervous system (CNS) and unlike intracellular antibodies, they are often responsible for inflammatory neurological damage [1, 28]. They can be seen at any age and affect both sexes, however, the age of onset and the sex distribution differ according to the type of the implicated antibody [28].
The most frequent are encephalitis with anti-NMDAr (N-methyl-D-aspartate receptors) and anti-VGKC (Voltage-Gated Potassium Channel) antibodies, the antigenic targets of which are the CASPR2 (Contactin-associated protein-like 2) and LGI1 (Leucine-rich Glioma-Inactivated 1) [18, 23]. Their clinical presentation is better individualized and often stereotyped [7,14,22,26].
The clinical manifestations are heterogeneous and depend on the type of antibody involved, even though the most common clinical presentation is an acute or subacute limbic encephalitis, which manifests with neuropsychiatric symptoms, and sometimes extra limbic manifestations, such as signs of dysautonomia, abnormal movements, dyskinesias, and ataxia [4, 16]. Some clinical signs make it possible to evoke the diagnosis and guide the search for the type of antibody involved (Faciobrachial dystonic seizures (FBDS), dyskinesias, neuromyotonia...etc.).
Their diagnosis is supported by laboratory and radiological examinations, such as the presence of inflammatory lesions on cerebral magnetic resonance imaging (MRI), an immune reaction in the cerebrospinal fluid (CSF) and an electrical pattern on the electroencephalogram (EEG). Nevertheless, it is confirmed by the detection of antibodies in the blood and/or the CSF [3,37].
Their management requires early and adapted therapeutic protocols, sometimes aggressive, involving immunomodulatory or immunosuppressive treatments [16, 50]. The response to immunotherapy is most often favourable [16, 48]. Some of these inflammatory autoimmune encephalitides can associate with tumours, and their removal is essential for better clinical outcomes [17].
We conducted a descriptive, longitudinal, prospective and retrospective study, that included thirty patients who presented a dysimmune encephalitis with antibodies against neuronal cell surface proteins (NMDAr, LGI1 and CAPSR2), within the Neurology department of the University Hospital of Tizi-Ouzou, during the period from January 2016 to December 2018.
This work aimed to depict the clinical and paraclinical features of patients presenting autoimmune encephalitis associated with antibodies against extracellular epitopes of neuronal cell-surface (anti NMDAr, anti LGI1, anti CASPR2), and to assess their therapeutic response.
It is a multivariate descriptive, longitudinal, prospective and retrospective study about patients who presented dysimmune encephalitis (to anti-NMDAr, anti-LGI1 and anti-CAPSR2) in the neurology department of the Tizi-Ouzou university hospital from January 2016 to December 2018. Our study included a total of thirty patients (30).
We included patients who presented anti-NMDAr and anti-VGKC dysimmune encephalitis (CASPR2, LGI1). They have presented limbic encephalitis associating, to varying degrees, neuropsychiatric symptoms. The signs onset was either acute or subacute (in several weeks or months).
All the study patients had suggestive paraclinical examinations, namely cerebral MRI, EEG, CSF analysis, as well as anti-NMDAr, anti CASPR2, and anti LGI1 antibodies in the CSF and/or the serum.
We included patients with confirmed diagnosis (definite diagnosis) or with seronegative forms (probable diagnosis) with suggestive clinical characteristics (dyskinesias, brachio-facial dystonias, neuromyotonia, hyponatremia and dysautonomia), as well as paraclinical results (EEG patterns, MRI abnormalities, and CSF abnormalities).
Other differential diagnoses, such as herpetic encephalitis and paraneoplastic encephalitis, have been ruled out. A psychiatric evaluation was carried out in collaboration with the psychiatrists (based on the DSM-V).
From January 2016 to December 2018, we identified thirty patients with one of the three types of dysimmune encephalitis (anti-NMDAr, anti-LGI1, or CASPR2). The mean duration of follow-up was 18 months, with a minimum of 06 months due to death in one patient (3.3%) and a maximum of 30 months in two patients (6.7%). These thirty patients included 16 women and 14 men, with a slight female predominance (53.3%), with a sex ratio of 0.87.
73.3 % of patients had an acute onset, while 26.7 % had a subacute onset. Prodromes were present in one-third of the patients, mainly headache, asthenia, vomiting, and photophobia. The mode of entry was psychiatric in 66.7% of cases and neurological in 33.3% of cases dominated by seizures. Vigilance disturbances were found in 66.7% of cases, to varying degrees, and 10% of patients needed tracheal intubation. Different types of seizures were found in 83.3% of cases. Faciobrachial dystonic seizures (FBDS) were observed in 26.7 % of the patients. Dyskinesias were observed in a third of cases, dysautonomic signs in 76.7% of cases and insomnia in 53.3% of cases. Many unusual symptoms have been reported including central signs, such as mutism, catatonia, aggravation under neuroleptics, pruritus, and peripheral symptoms, namely cramps, paresthesias, and fasciculations.
However, in 30% of cases, the examination revealed objective neurological signs (cerebellar ataxia, hemiparesis, extrapyramidal signs, signs of peripheral involvement), and even neuromyotonia in 20% of cases. Besides, fever was only observed in 23.3% of cases.
MMSE score showed slight memory impairment in 86.2% of cases. Biologically, a third of the patients presented with hyponatremia. Brain MRI revealed abnormalities in 86.7% of cases.

Figure 1: 17-year-old female patient with anti-NMDAr encephalitis (seropositive). Cerebral MRI, FLAIR sequence: left temporo-insular hyper signal.

Figure 2: 65-year-old patient with anti-LGI1 encephalitis (seropositive). Cerebral MRI, FLAIR sequence: bilateral amygdalo-hippocampal hyper signal.
Cerebrospinal fluid analysis showed abnormalities in 86.7% of cases. 73.3% presented hyperproteinorachia, and only 23.3% had lymphocyte-type hypercellularity with an average of 45.86 lymphocytes / mm3. The CSF immunology was pathological in 53.35% of cases.
On the initial EEG, 76.7% of cases presented generalized or focal nonspecific cerebral abnormalities including background slowing, theta or delta activity, and only 23.3% presented with epileptic abnormalities. Furthermore, no patient presented Extreme Delta Brush, but other abnormalities were rarely observed (fast rhythms, slow rhythmic waves, and periodic complexes).

Figure 3: EEG of a patient with anti-NMDAr encephalitis: Rhythmic slow waves especially on the right.
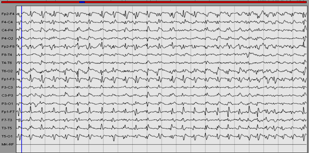
Figure 4: of a patient with anti CASPR2 encephalitis: Periodic complexes.
The specific immunological examination, which consists of measuring membrane antibodies (NMDAr, VGKC, LGI1, CSAPR2), showed that 63.3% of cases presented positive antibodies. 36.84% of patients presented anti CASPR2 antibodies, 26.32% anti-NMDAr antibodies, and 26.32% anti-LGI1 antibodies. 5.26% of cases displayed a combination of CASPR2 and anti LGI1 antibodies, and 5.26% of cases showed a combination of anti LGI1 and anti VGKC antibodies. It is worth noting that they were found in 63.2 % of cases in the CSF, 26.3% in the blood, and 10.5 % in both.
The search for associated neoplasia revealed the presence of tumour in 16.7% of cases. The mean age of the patients with the tumour was 46.6 ± 11 years. The anatomopathological study found mainly thymomas (stage B1 or B2 / B3) and adenocarcinoma of the colon.
All patients received first-line treatment, with 93.3% receiving intravenous (IV) methylprednisolone (1g/day for three to five days), 96.7% receiving IV immunoglobulin (0.4 mg/kg for 05 days) at a rate of one to six cures, and 6.7% receiving plasma exchanges at a rate of three courses). A switch to oral corticosteroids (1 mg/kg/day) was used in 30% of cases. Second-line treatment was started in 46.7% of cases. Rituximab and Cyclophosphamide were used in severe forms, while Azathioprime was initiated in the less severe cases to prevent relapses or as a relay to prior treatment in conjunction with a specific treatment of the existing tumour.
One-third of patients have completely recovered, 63.3 percent have recovered significantly, and one patient has died as a result of tumor complications. Treatment improved the major symptoms (psychiatric conditions, vigilance disorders, epileptic seizures, and memory disorders) (p = 10-3). However, in 63.4 percent of cases, sequelae were observed, with memory impairment being the most common. In 80% of cases, patient autonomy was regained, with just 6.7 percent of cases experiencing a single episode of relapse.
This work aimed to analyse the clinical and paraclinical features of autoimmune encephalitis due to antibodies targeting neuronal cell membrane antigens, namely anti-NMDAr, anti LGI1, and anti CASPR2, in order to better recognize these entities. Therefore, our findings were compared to data from the literature after an average follow-up of 18 months. In our cohort, there was a slight female predominance (sex ratio of 0.87). However, this sex-based distribution did not accurately reflect the various types of antibodies. Some types of encephalitis, such as anti-NMDAr encephalitis [28], have a significant female predominance, while others, such as anti-CAPR2 and anti-LGI1 encephalitis, have a significant male predominance. [5, 38].
In our study, the mean age was 44 ± 18 years, with a vast majority of patients over the age of 45 years. We found an autoimmune history in 26.7% of cases, favouring the disease onset, particularly in the pediatric population [12]. It was a disease that was thought to be uncommon but was likely underdiagnosed. The recent rise in the number of cases reported in the literature [4] is likely due to the availability of biological markers as well as a greater understanding of suggestive clinical presentations. Regardless of the antibody involved, the clinical presentation in our series was relatively stereotyped, with some clinical homogeneity, similar to what has been described in the literature. Limbic encephalitis is the most common presentation with mainly an acute onset (73.3 % of cases) or subacute (26.7 % of cases). It is characterized by a psychiatric (60.7%) or neurological (33.3%) entry mode in the majority of cases. The psychic manifestations include behavioural disorders, such as aggression, agitation, irritability, panic attacks and hallucinations. They are associated with neurological manifestations, such as impairment of antegrade memory (100% of cases), epileptic seizures (83.3% of cases), dysautonomia signs (76.7% of cases) and vigilance disorders (66.7% of cases) [41]. Prodromes were found after a thorough examination (33.3% of cases), although few studies were interested in this parameter, which is most commonly seen in anti-NMDAr encephalitis (70% to 86% of cases) [9].
Patients can seek treatment in psychiatry first because of the psychiatric manifestations (depression, anxiety, and psychotic manifestations), which may mislead the diagnosis [52]. On the other hand, epileptic seizures (inaugural in 23.3% of cases) dominated the neurological onset manifestations, emphasizing the importance of maintaining a critical approach in the face of a first epileptic seizure in order to avoid being satisfied with a simple antiepileptic treatment, which can be inefficient. Epileptic seizures were found in 83.3% of our patients (at the onset or in the acute phase), which was consistent with the literature [33,50]. These are mostly temporal, which is in line with previous findings [8].
Our study found vigilance disturbances ranging from simple obnubilation to coma, with 30% of our patients falling into a coma. Because of certain complications, such as infections, these disorders of consciousness may worsen the vital and functional prognosis, and may even prevent the initiation of certain immunosuppressive treatments [10].
Extra limbic symptoms have been observed in our patients, which makes the name limbic encephalitis debatable in favour of autoimmune or dysimmune encephalitis as some authors have suggested, so as not to underdiagnose certain atypical forms or purely extra limbic encephalitis [4]. As a result, Lai et al. proposed, in 2010, the term autoimmune synaptic encephalitis to replace the term limbic encephalitis [38]. Some signs and symptoms are highly suggestive of autoimmune encephalitis, and it is essential to recognize them. FBDS (26.7% of cases), dyskinesias (33% of cases), orofacial or diffuse with choreic movements and opisthotonos attitude, are considered to be the most suggestive signs. Dysautonomia signs were present in 76.7% of our patients, which approaches the data reported in the literature (69%) [10, 12]. Neuromyotonia and sometimes even paroxysmal ataxia have also been reported [28, 32, 34, 36,40]. Dysautonomia signs were one of the most defining features of these entities, which could result in cardiac and/or respiratory decompensation [10]. Many of those signs were observed in our series, namely sweating, salivation, temperature and blood pressure fluctuations. Neuromyotonia was of capital importance for the diagnosis since it was typical in certain types of antibodies (anti CASP2), allowing the search for the type of tumour that could be involved (thymoma) to be guided [34.39].
We found sleep disorders, such as insomnia, in 53.3% of cases, and it is often identified as a suggestive symptom of some dysimmune encephalitis [2, 32, 44, 49]. It is worth noting that sleep disturbances have been reported in paraneoplastic limbic encephalitis associated with anti Ma2 antibodies [11], and that was ruled out by onconeuronal antibodies testing in our cohort. Paraclinical examinations not only rule out other differential diagnosis but they also contribute to confirm the diagnosis by pointing out certain typical characteristics.
Hyponatremia should be looked for systematically because it can worsen vigilance disturbances, and it requires appropriate correction and the use of some therapies with caution. It was found in a third of our study population. It is rarer in other aetiologies of limbic encephalitis, such as limbic paraneoplastic encephalitis (anti-Hu) compared to what has been reported in autoimmune encephalitis [20, 30, 50].
The scalp EEG was an easy, non-invasive, and cost-effective exam to perform. It was essential for the differential diagnosis (herpetic encephalitis, metabolic encephalopathies, Creutzfeld-Jacob disease). In the literature, no electrical pattern common to all antibodies has been identified. It often showed a diffuse or focal non-specific slowing (up to 90% of cases) and sometimes epileptic abnormalities [19, 31, 48]. On the other hand, an "extreme delta brush (EDB)" pattern has been described only in anti NMDAr encephalitis, which is very suggestive, and even fast rhythms or slow rhythmic waves [15, 35,47]. In our study population, the initial EEG was often pathological (76.7% of cases), often displaying the non-specific abnormalities described above [19]. Inter-critical epileptic anomalies were also uncommonly recorded. The reported EDB pattern was not found in our series, which could be explained by its transient character [19].
Brain MRI often objectified parenchymal abnormalities (86.7% of cases), which were similar to those reported in the literature [25, 51], including isolated temporal lesions (36.6% of cases). They were more bilateral than unilateral. Extra limbic radiological abnormalities were found in half of the cases. The most affected localisations are mainly the frontal lobe, the basal ganglia, and rarely other structures, such as the insula, parietal lobe, occipital lobe, meninges and white matter are affected. These extra limbic anomalies have been reported in the literature at a lower frequency than ours (40% of cases) [51]. Graus et al. included bilateral temporal involvement (in T2 and FLAIR) in the criteria for defined autoimmune encephalitis [23]. Unilateral temporal impairment would be possible. However, in this case, Graus et al. required the presence of antibodies to classify it as autoimmune encephalitis because other etiologies, such as glioma, seizures, and HSV1, could cause a unilateral temporal hyper signal [23].
The cytological and biochemical analysis of the CSF was essential, and it was primarily pathological (86.7% of our cases), which is consistent with the literature data [6,24]. CSF bacteriological analysis was essential in order to rule out infectious causes. In some series, the CSF profil was normal [38,50], which is not against the diagnosis of dysimmune encephalitis. The CSF abnormalities were mainly hyper proteinorachia (73.3% of cases, often the level did not exceed 01g/l), lymphocytic pleocytosis (23.3% of cases, with an average of 45,86 lymphocytes/mm3), and especially the presence of oligo-clonal bands (OCBs) in 46.6% of cases, which demonstrates the existence of an inflammatory mechanism, particularly for seronegative forms. These results are close to those reported by certain authors who found slight to moderate lymphocytic pleocytosis (generally less than 100 cells/mm³) in 60 to 80% of patients and oligoclonal bands in approximately 50% of cases [24, 27].
The specific antibodies testing confirmed the diagnosis, but the determination of the type of antibody to look for and the interpretation of the results had to be chosen according to the clinical presentation and the results of the paraclinical examinations and required a specialized centre with adapted techniques. Some authors have suggested that the presence of antibodies targeting CNS cell membrane was not necessary for the diagnosis of autoimmune encephalitis and that their negativity should in no way delay the initiation of an early treatment if the clinical manifestations and the para-clinical data are suggestive [4, 21]. This was the case in our study, where one-third of the patients had seronegative encephalitis and responded well to immunotherapy.
In our cohort, 63.3% of cases were seropositive (indirect immunofluorescence, immunohistochemistry, and a specific test on transfected HEK cells). Other tests were also necessary, such as the assay of onco-neuronal antibodies (antibodies targeting intracellular antigens) to rule out paraneoplastic encephalitis. We have diagnosed a significant number of patients with this latter (anti-Yo, Ma2, Ri, anti Sox1, CV2/CRMP5, anti-Tr). We also assayed the antibodies directed against intracellular synaptic antigens, which made it possible to diagnose one case of anti-GAD65 encephalitis and one case of anti-amphiphysin encephalitis.
Further exams were performed to look for associated neoplasia, namely abdominal, pelvic and thoracic CT-Scan, pelvic and scrotal ultrasound, as well as tumour markers and PSA assays. Therefore, we found a paraneoplastic syndrome in some patients (16.7% of cases) associated with thymoma or adenocarcinoma confirming the possibility of the existence of paraneoplastic encephalitis among these cases without them being purely autoimmune [1].
In terms of management, we proposed some treatment plans based on prior experiences because there were no therapeutic consensus or well-codified protocols. There was no data from randomized controlled clinical trials of immunotherapy use, the order in which they should be administered or the duration of treatment [10,13, 29,45]. Therefore, we used IV bolus of methylprednisolone as first-line treatment, which was typically followed by oral corticosteroids relay and IV immunoglobulins (Ig) [13, 29, 45]. Some experts defended plasma exchanges, which we used in just 6.7% of cases, while others prefered IV Ig [43,46], despite the lack of compelling evidence of superiority [45]. IV Ig seemed to be more manageable than plasma exchanges due to frequent agitation, epileptic seizures interfering with plasmapheresis progress, and dysautonomia signs which could be worsened by the latter [12,50]. The molecules chosen were rituximab (375mg/m2) and cyclophosphamide (750mg/m2 IV) and have been given shortly after first-line treatment to avoid having a therapeutic window [45]. In patients with less serious manifestations, azathioprine (1mg/Kg/d) was also used to minimize the risk of relapse. This second-line therapy has been implemented in 46.7% of our patients, with no significant side effects recorded. Rituximab, a monoclonal anti-CD20 antibody, is becoming more widely used in the treatment of autoimmune diseases [42]. In parallel, tumour specific management was started with either ablation of the tumour (60% of cases) or by chemotherapy combined with radiotherapy (40% of cases). Depending on the seriousness of the clinical presentation and the therapeutic response, a second-line treatment was added. This proved the importance given to this entity that is sometimes paraneoplastic, allowing us to treat tumours at an early stage.
Finally, after an average of 18 months of follow-up (a minimum of 06 months and a maximum of 30 months), we evaluated the treatment response. One patient was lost to follow-up after 08 months. We found that 33.3% of patients recovered completely, while 63% recovered partially but significantly. Just one patient died as a result of tumour complications. According to the literature data, autoimmune encephalitis is a potentially treatable condition that may be fatal. Adequate, prompt, and sometimes aggressive treatment is essential because it often results in a significant improvement or complete recovery [28]. During the study period, we noticed a few non-disabling sequelae (66.7% of cases). Therapeutic efficacy was reflected by the patient's autonomy, which was assessed by questioning him and those around him about his daily activities without using a specific rating scale. In our sample, 80% of patients regained their autonomy.
This study aimed to identify the clinical and paraclinical characteristics of the most common dysimmune encephalitis types: anti-NMDAr, anti-LGI1 and anti-CASPR2. For a long time, it was confused with other limbic encephalitis causes. The majority of the previous studies described the different subtypes of dysimmune encephalitis without grouping them into a single clinical and paraclinical entity to make clinical diagnosis easier without waiting for specialized examinations. This study proposed a rapid diagnostic approach based on some discriminative clinical features, namely FBDS, dyskinesias, typical psychiatric manifestations and peripheral signs. These characteristics differ depending on which antibody is involved, and the diagnosis is supported by suggestive paraclinical findings such as a temporal hyper signal, which is usually bilateral and often associated with extra limbic lesions on brain MRI, oligo-clonal bands and EEG abnormalities.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
