AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Hayder A Giha, Medical Biochemistry and Molecular Biology, Khartoum, Sudan.
Citation: Osman Al-Sayed Osman Alamin, Sara Osman AbdAllah Hassan, Hayder A Giha (2022) Disparity of risk factors and concordance of NLR with Gensini score in acute coronary syndrome in an Afro-Arab multiethnic nation J. Cardiology Research and Reports 4(2); DOI: 10.31579/2692-9759/038
Copyright: © 2022, Hayder A Giha, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 December 2021 | Accepted: 25 December 2021 | Published: 05 February 2022
Keywords: ACS; ECG; angiography; gensini score; NLR
Background: Acute coronary syndrome (ACS), is ischemic heart disease of varying risk factors and clinical pattern and with immense health burden worldwide. Inflammation is believed to be an etiological factor in ACS, and neutrophil to lymphocyte ratio (NLR), to be a biomarker.
Objectives: To describe the clinical pattern and risk factors of ACS in Afro-Arabs of Sudan and to evaluate the NLR as a severity marker.
Method: In a total population, cross-sectional study, conducted in Al-Shaab Hospital- Sudan, clinical, laboratory and ECG data were used for ACS grouping into unstable angina (UA), non-ST-segment elevation myocardial infarction (NSTEMI) and STEMI. All patients underwent coronary angiography (CAG) and their Gensini score and NLR were calculated.
Results: A total of 130 patients (62.3% men) of a median age of 58.0, 50.0-65.0 yrs., (range 32.0-82.0), were diagnosed with ACS; 44.6% STEMI, 37.7% NSTEMI and 17.7% UA. The median Gensini score was higher in STEMI (42.5, 12.0-71.0) and NSTEMI (40.0, 15.8-60.5) compared with UA (10.0, 5.0-23.0), p 0.002, similarly, was the NLR; 3.5, 1.6-4.6; 2.9, 1.5-3.8 and 0.9, 0.8-1.1, respectively p<0.001. Furthermore, the NLR in concordance with CAG findings p<0.001. Finally, hypertension, diabetes mellitus and dyslipidemia, respectively, were stronger ACS risk factors in women than in men unlike smoking, and family history imposed the least risk.
Conclusion: While the ACS clinical pattern was in-line with literature, the risk factors order was different, and it was different between sexes. Importantly, the NLR strongly associated with ACS severity, but failed to distinguish between NSTEMI and STEMI.
ACS Acute coronary syndrome
MI Myocardial infarction
CAD Coronary artery disease
CAG Coronary angiography
CVD Cardiovascular disease
DM Diabetes mellitus
HDL High density lipoprotein
HTN Hypertension
LDL Low density lipoprotein
NLR Neutrohil lymphocyte ratio
NSTEMI Non-ST-segment elevation myocardial infarction
STEMI ST-segment elevation myocardial infarction
UA Unstable angina
Cardiovascular diseases (CVD) are one of the major causes of death worldwide. The World Health Organization declared that CVD are responsible of about 17.9 million death/year, which was 31% of the world deaths in 2016, of which 7.5 million are due to ischemic heart disease (IHD), mainly acute coronary syndrome (ACS) and sudden death [1]. The incidence of IHD increases with age, and it is responsible for more than half of all CVD in the ages < 75>
The ACS refers to a spectrum of clinical presentation ranging from ST-segment elevation myocardial infarction (STEMI) to non–STEMI (NSTEMI) and unstable angina (UA) according to the presence or absence of ST-segment elevation on initial ECG, in addition to measurement of myocardial biomarkers, such as troponin or creatine kinase, however in both condition there is myocardial necrosis [4, 5]. The UA is different from stable angina, which develops during physical activity or stress and resolves at rest, still there is no myocardial necrosis in UA [4, 6].
For ACS patients, coronary angiography (CAG) is usually conducted and assessed by specialized cardiologists. Significant CAD is assumed as a lumen diameter stenosis of ≥50% in the major coronary arteries e.g. left main, anterior descending or circumflex artery coronary arteries, right coronary artery, or one of their major branches [7].
The IHD is caused by atherosclerosis of the coronary arteries, which leads to development of unstable plaque as a result of chronic inflammatory mechanism [8, 9]. The rupture of the plaque is accompanied by a cascade of platelet reactions culminating in formation of thrombus, followed by occlusion of the affected coronary artery then ischemia/necrosis of the underlying myocardial tissue, leading to ACS [9]. Thus, inflammation plays is an important factor in both initiation and progression of atherosclerotic process [10], and increased neutrophil count is known to be associated with the development and severity of coronary atherosclerosis [11]. Neutrophil to lymphocyte ratio (NLR), is a combination of inflammatory markers in which the neutrophils are nonspecific markers of inflammation and lymphocytes are regulatory cells [12]. The association between NLR and various CVD, is well documented, thus there is propensity of the former to evolve into an accurate, inexpensive, and independent prognostic marker for diagnosis of ACS and predictor for its short and long-term mortalities [13]. In a recent study, NLR was found to be associated with severity and plaque morphology in patients with CHD [14], and the high NLR compared to low NLR at admission was found to be associated with higher mortality in STEMI and NSTEMI patients [15]. Furthermore, the NLR is significantly elevated in patients with low HDL-cholesterol and negatively correlated with high-density lipoprotein (HDL) which has anti-inflammatory activity [16]. However, which NLR value is correlated with a higher risk for developing atherosclerosis, which cut-off value will differentiate normal from abnormal results are still debatable. Different values of NLR, with different methods, in different populations are cited, with no universal value is currently available [17].
There is an extreme need for a reliable, accessible, less invasive prognostic marker in ACS that would help in early identifications of patients with high cardiovascular risk. The goal of this study is to describe the ACS risk factors and clinical spectrum in the biggest cardiology center in Sudan and included subjects with different ethnic decent (Afro-Arabs) to evaluate the potential use of NLR as a quick, reliable and affordable biomarker for grading the ACS severity in a country with limited resources. Moreover, the NLR have racial differences, thus it’s a necessity that data to be collated from all over the world.
Study design: Total-population, cross-sectional hospital-based study.
Study area. The study was conducted in Alshaab Teaching Hospital (ATH) in Khartoum, the main cardiac center in Sudan.
Study population: All patients with ACS admitted to ATH in the period from September to December 2020, with confirmed ACS and underwent coronary angiography, were included while active inflammation, infection, malignancy, hematological disorder, autoimmune disease, and immunosuppressive treatments, were the exclusion criteria. The patients were derived from different ethnic backgrounds of varying degrees of African and Arab race crossing.
Data collection: The personal, demographic, clinical and laboratory investigation data were collected from each participant with inclusion of information about potential cardiovascular risk factors e.g. hypertension (HTN), diabetes mellitus (DM), smoking history, dyslipidemia and family history of CAD.
Blood test: Hemoglobin (Hb), total and differential white blood cells (WBC), and platelets count were done using Sysmex XP 300 machine
Neutrophil / lymphocytes Ratios (NLR): The absolute neutrophil count was divided by the absolute lymphocyte count to calculate the NLR.
The ACS diagnosis:
The following investigations were doneto patients on arrival in the emergency room i. Electrocardiogram (ECG); the resting 12-lead ECG, ii. Cardiac biomarkers: measurement of cardiac troponin (cTn) T or I.
iii. Coronary angiography was done by expert interventional cardiologists.
Based on the clinical data in addition to the cardiac markers and ECG, patient were grouped into, STEMI, NSTEMI and UA [4]. The STEMI is suspected in patients presented with a consistent clinical history and ECG showed persistent (>20 minutes) ST-segment elevation (measured at the J-point) in at least two contiguous leads of ≥ 2.5mm in men < 40>
Assessment of coronary angiography
Coronary angiography (CAG) was conducted and assessed by experienced specialized cardiologists. Significant vessel disease (stenosis) was defined as a lumen diameter narrowing of ≥50% in the major coronary arteries; left main coronary artery, left anterior descending artery, left circumflex artery, right coronary artery, or one of their major branches. The CAD results categorized as; one-vessel disease (1-VD), two-vessel disease (2-VD; or left main trunk disease without right coronary artery stenosis) or three-vessel disease (3-VD; or left main trunk disease with right coronary artery stenosis).
Gensini score: Calculation of the Gensini score was initiated by giving a severity score to each coronary stenosis as follows: It defined narrowing of the lumen of the coronary arteries as 1 for 1 to 25% stenosis, 2 for 26 to 50%, 4 for 51 to 75%, 8 for 76 to 90%, 16 for 91 to 99%, and 32 for total occlusion. The score was then multiplied by a factor representing the importance of the lesion location in the coronary artery system. For the location scores, 5 points were given for a left main lesion; 2.5 for the proximal left anterior descending (LAD) or left circumflex (LCX) artery; 1.5 for the mid-segment LAD and LCX; 1 for the distal segment of the LAD and LCX, first diagonal branch, first obtuse marginal branch, right coronary artery, posterior descending artery, and intermediate artery; and 0.5 for the second diagonal and second obtuse marginal branches [18]. Finally, Gensini score of >25 was used to draw a cutoff point for the NLR atherogenic risk, using Receiver Operating Characteristics (ROC) program.
Ethical consideration
Ethical clearance was obtained from the research ethics committee at Sudan medical specialization board. Permission was obtained from A-Shaab Hospital management staff as a site for the study. Written and verbal consents were obtained from study participants. Confidentiality and anonymity of individual identity is maintained.
Statistical analysis
Sigma-Stat software was used for statistical analysis. T-test and One Way of Analysis of variance (ANOVA) were used for comparisons of normally distributed data (mean ± SD), while Mann-Whitney Rank Sum Test (MW) and Kruskal-Wallis One Way Analysis of Variance on Ranks (KW) were used for analysis of the data which was not normally distributed. The rates and proportions were analyzed by Chi-square test (χ2). The Pearson Product Moment Correlation was used for running the correlations.
Description of the study subjects
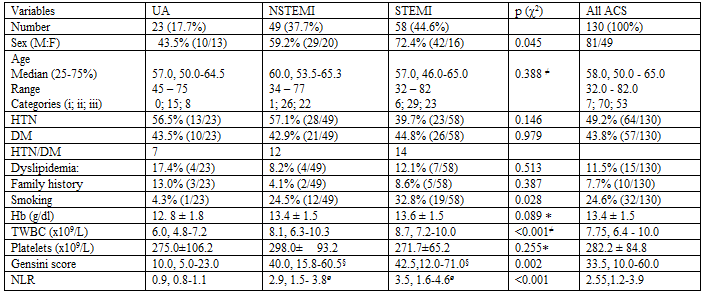
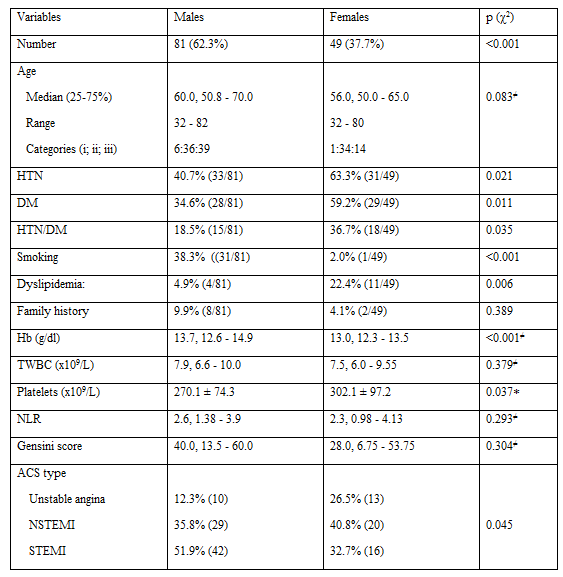
As shown in (Table 1), the total study subjects were 130 patients with ACS, of whom 81 were males and 49 females, aged between 32 and 82 years with a median age of 58.0 (50.0 - 65.0) years. As risk factors, the frequency of diseases associated ACS were as follows; hypertension (HTN) 49.2%, diabetes mellitus (DM) 43.8%, HTN/DM, 25.4% (33/130) and dyslipidemia 11.5%. While frequency of family history of ACS was 7.7% and of smoking was 24.6%. The average hematological indices for all subjects were; hemoglobin (Hb), 13.4 ± 1.5 g/dl, total white blood cells count (TWBC), 7.75, 6.4 - 10.0 x 109/L and platelets 282.2 ± 84.8 x 109/L. However, the female patients had significantly lower Hb (p<0>p 0.037) compared to males, but had comparable TWBC (p 0.379), (Table 2).
Acute coronary syndrome pattern:
The frequencies of the three clinical types of ACS, the unstable angina (UA), non-ST-segment elevation myocardial infarction (NSTEMI), and STEMI, were 17.7%, 37.7%, and 44.6%, respectively (Table 1). While the vast majority of the STEMI were males (72.4%), majority of the UA were females 56.5% and of the NSTEMI were males (59.2%). Although the NSTEMI patients were slightly older, the 3 groups of patients were comparable in age, p 0.388, KW. Notably, all the UA patients were ≥ 45 yrs. Furthermore the Hb and platelet count were comparable between the three groups with slightly lower Hb in UA and platelet in STEMI, p 0.089 and p 0.255, respectively, however, the TWBC was significantly higher in STEMI, followed NSTEMI compared to UA, p <0>
Acute coronary syndrome risk factors and sex:
The potential risk factors, HTN, DM, combined HTN/DM, dyslipidemia and family history of ACS were comparable between the 3 clinical groups, UA, NSTEMI and STEMI except for cigarette smoking which was significantly higher in STEMI, followed by NSTEMI compared to UA, p 0.028, as shown in (Table 1). However, most of the risk factors were significantly different between the male and females patients. Females compared to males had significantly more frequent HTN (p 0.021), DM (p 0.011), HTN/DM (p 0.035) and dyslipidemia (p 0.006), on the contrary males were significantly more frequent smokers (p<0>
Concordance of the coronary angiography (CAG) findings, Gensini score and the neutrophils/ lymphocytes ratio (NLR)
The Gensini score is a numerical estimation of the overall degree of ischemia and thus ACS severity, which was worked out from the visible angiographic findings, it was calculated based on the numbers and locations of stenosis in coronary arteries. The CAG showed, single vessel disease in 43 (33.1%) patients, three vessels disease in 38 (29.2%) patients, two vessels disease in 26 (20%) patients and non-significant CHD in 23 (17.7%) patients (data not shown).
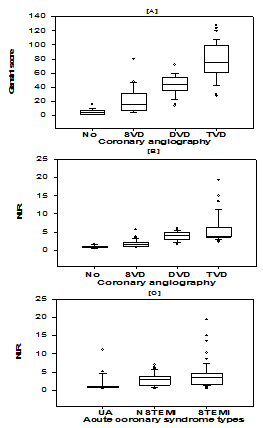
As shown in (Fig. 1A), the Gensini score was markedly significantly different between patients with no (5.0, 2.25-6.75) or with single, (16.0, 7.25-30.0) double (44.0, 36.0-54.0) or triple (75.5, 62.0-99.0) coronary artery lesion regardless of the degree or location of stenosis, or the affected artery, p<0>
Figures legends:
Figure 1. Grouping of patients with acute coronary syndrome (ACS), based on cardiac angiography (CAG), into patients with; no significant stenosis (No), single vessel disease (SVD), double vessel disease (DVD) and three vessel disease (TVD). A. Comparison of the median Gensini score showed marked difference between the four CAG groups, p<0>p<0>p<0>
Interestingly, the NLR was similarly markedly significantly different between the patients in the same above 4 angiographic groups, patients with no stenosis (0.8, 0.78-1.08), single (1.5, 1.13-2.05), double (4.0, 2.9-4.9) or triple (3.9, 3.6-6.2) coronary artery lesion, p<0>
Finally, the ROC curve defined NLR cut-off value of atherosclerosis to be 2.2, with 88.89% sensitivity, and 91.38% specificity (data not shown).
The association of the NLR with the acute coronary syndrome types
The median NLR values were significantly different between the ACS clinical types, it was highest in STEMI (3.5, 1.6-4.6), followed by NSTEMI (2.9, 1.48-3.8) and lowest in UA (0.9, 0.8-1.1), p<0>p<0>p 0.255 (Table 1).
The correlations of Gensini score with NLR and individual hematological parameters
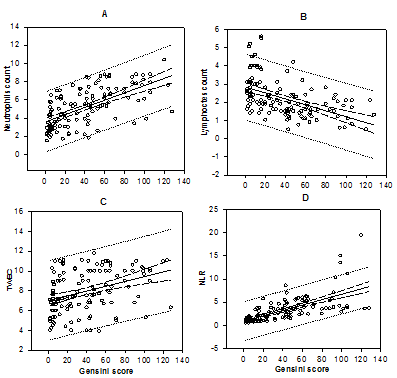
As shown in (Fig. 2) there was statistically significant positive correlation between the NLR and Gensini score, i.e., as the Gensini score increased the NLR was equivalently increased, CC 0.671, p<0>p<0> p<0>p<0>p 0.368 - data not shown).
in the main cardiac center in Sudan, and furthermore to evaluate the NLR as simple affordable non-invasive indicator for disease severity as compared to Gensini score.
Age and sex are two important variables in ACS, in this study most of the patients (62.3%) were males, with an overall average age of presentation of 58 years, nevertheless, 53.8% of the patients were aged between 40-60 years, an age related to structural changes in arteries [19]. As expected, women present earlier (median age of 56 yrs.), compared to men (60 yrs.), and as small as 32 yrs. old patients were seen among both men and women (Table 2), as noticed somewhere else [20]. Unexpectedly, while the median age for NSTEMI was 60 yrs., the median age in both STEMI and UA was 57 yrs., but a large sample study was previously declared that older people are more likely to develop NSTEMI than STEMI [21].
This study disclosed the fact that the vast majority (82.3%) of patients diagnosed with ACS were had myocardial infarction (USTEMI and STEMI) i.e., cardiac necrosis, while the remainders had myocardial ischemia due to UA. Additionally, the more sever MI, the STEMI, was the more frequent (45%), which was consistent with what was reported before [22]. Furthermore, all patient were underwent cardiac angiography (CAG), almost half of the patients had 2 or more coronary arteries with significant stenosis. As seen in (Fig. 1A), the Gensini score of 5.0, 16.0, 44.0 and 75.5, was reflecting angiographic classification; no significant stenosis, single (SVD), double (DVD) and three (TVD) vessel diseases, respectively, p<0>p 0.002, the Gensini score failed to distinguish between NSTEMI and STEMI, p 0.639, (Table 1).
The role of inflammation in atherosclerosis pathology and CVDs, and characterization of the latter as a chronic low-grade inflammatory conditions are now largely accepted [23, 24]. Of the markers of inflammation, the leukocytes (WBCs), namely neutrophils and lymphocytes [14]. In this study we noticed increased numbers of circulating TWBC and neutrophils on the contrary decreased lymphocytes, in patients with severe ACS (Table 1), as well as there were positive correlations of the TWBC and neutrophils and negative correlation of the lymphocytes with Gensini score, the ACS severity marker (Fig. 2). The NLR, which integrates the neutrophils and lymphocytes into a single biomarker, was found to be strong predictor for the ECG-dependent ACS clinical severity, in the present study. The NLR increment was more pronounced in the STEMI followed by NSTEMI compared to UA, in line with previous studies [13, 14). The NLR like the Gensini score, was also failed to distinguish between the NSTEMI and STEMI, p 0.154, (Table 1). However, the NLR was markedly positively correlated with the Gensini score (Fig. 2D), as reported before [11, 25]. The parallel increase of both markers as indicators for increased ACS severity was recognized in different sites [26, 27]. Although healthy control subject were not included in the present study, a previous study showed that, NLR was significantly higher in CVD patients than in normal subjects, as well as it varied according to ethnicity [28].
Despite the well established relationship between NLR and atherosclerosis, the association between NLR and complexity of the coronary arteries stenosis is rarely investigated [29]. In this study, the NLR was also varied significantly with the CAG findings, as the NLR was almost 4 times higher in patients with double (DVD) or three (TVD) coronary arteries stenosis/disease as compared to patients with non-significant arterial stenosis, and around three times higher compared to patients with single artery stenosis (SVD), Fig. (1B). Similar results were reported before [29, 30], although another study, debated this relationship [31].
However, of the limitations of the NLR use as a biomarker for ACS is the versatile non-specific nature of the inflammatory markers in general. A systematic review and meta-analysis showed that high NLR was significantly associated with all CVD outcomes including CAD, ACS, stroke, and composite CVEs [32]. Thus, for use in ACS the NLR need to be coupled with other investigations and suggestive clinical evidences.
In the present study seven risk factors for IHD, including sex were tested. The higher incidence of ACS in men compared with women over the study period was evident (Table 2), which is a well-known testimonial [33]. In this study, HTH was found to be the most common risk factor (49.2%) followed by DM (43.8%), smoking (24.6%), then dyslipidemia (11.5%) and finally family history of IHD (7.7%). However, in a large European study dyslipidemia was found to be the highest risk factor followed by HTN [22], however, in another study, smoking was found to be the commonest risk factor [33]. Chronically, HTN is implicated in atherosclerosis by damaging the blood vessel walls and possibility of plaque deposition. Alternatively, the high prevalence of HTN in general population in different regions including Sudan [34, 35], which is by far overweighing the ACS prevalence, gives false impression that HTN is the predominant IDH risk factor. Although, the above variables are well established risk factors for ACS [36], in the present study the frequency of these factors, except smoking, were not significantly different between the clinical types of ACS, the UA, NSTEMI and STEMI (Table 1). Interestingly, when splitting the patient into males and females, the above factors, except the family history, were found to show differential frequencies between men and women and probably being stronger risk factors for ACS in one sex more than the other (Table 2). Thus, HTN, DM, HTN/DM and dyslipidemia were likely to derive towards ACS in women more than in men, while smoking derive oppositely. As it stand, men probably bears an unidentified stronger risk factor/s than the mentioned ones since the prevalence of the IHD is significantly higher in men.
Finally, in the present study, the calculated NLR cut-off point for atherosclerosis was found to be >2.2. However there are several different approaches e.g. Interactive Dot Plot, were used to define the cu-off points for different goals with different values [11, 37]. In this setting, the NLR cut-off value of 2.2 was set to be used as a predictor of severity of atherosclerosis. Of the limitations of this study, the relatively small sample size and lack of healthy controls, as well as, other acute inflammation markers such as CRP, hs-CT, serum amyloid A, were not tested.
In conclusion, this study described the clinical pattern of ACS and highlighted the differences of the order of the traditional risk factors of IHD between the local and global orders and between sexes. The vast majority of patients had STEMI and NSTEMI, most of them were males with a median age for ACS of 58 years. HTN, DM and dyslipidemia, in this order, were more strongly associated with ACS in women while smoking was the main risk factor in men. The NLR was in strong concordance with the ECG-dependent clinical diagnosis, CAG findings and Gensini score, and proved to be a reliable indicator for ACS severity. The NLR cutoff value for ACS severity was found to be 2.2.
The authors highly appreciate the willingness of all patients and their families in participation and collaboration in this study. Many thanks are extended to the medical doctors, nurses and chemistry labs managers in Al-Shaab Teaching Hospital - Khartoum, for the unlimited assistance
Funding: No fund
Conflicts of interest/Competing interests: No conflict of interest for all authors to declare
Availability of data and material: The data is available upon genuine request
Code availability: 'Not applicable'
Authors' contributions (optional): 'Not applicable'
Ethics approval: The studies were ethically approved by the ethical committee of Sudanese medical speciation board (no reference number).
Consent to participate: An informed consent was obtained from each patient before inclusion in the study. The data was confidentially maintained
Consent for publication: Consent for publication was obtained.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
