AUCTORES
Globalize your Research

BOOK
*Corresponding Author: Derese Desalegn Buta, University of South Africa.
Citation: Derese D. Buta, Li Zungu, Ayuk Betrand, (2024), Development of Awareness and Prevention Strategies on Pneumonia Among Under Five Children in Sidama Regional State, Ethiopia, J. Psychology and Mental Health Care, 8(1): DOI:10.31579/2637-8892/250
Copyright: © 2024, Derese Desalegn Buta. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 January 2024 | Accepted: 19 January 2024 | Published: 30 January 2024
Keywords: attitude, awareness, ethiopia, knowledge, pneumonia, practice, prevention, sidama regional state, strategies, under-five children,
Purpose: Aim of the study was to develop awareness and prevention strategies on pneumonia among under-five children in Sidama Regional State, Ethiopia.
Methods: Current study used mixed method approach followed with Delphi group comments and suggestions to attain the research goal.
Community based cross sectional study design and multistage sampling method were employed to recruit 843 mothers with under five children in quantitative phase. Strucured questionaries used to collect data. Data were entered in Epi data version 4.2.2 and exported to SPSS version 25; further analysis. Descriptive statistics, binary logistic and multivariate analysis were applied.
Furthermore, 6 FGDs were conducted among 40 mothers. Qualitative data were collected by using FGD guide, audio recorded, field note taken, and voice transcription, verbatim has done, three themes and six sub themes identified. Analysis supported by Atlas ti soft ware.
Result: The over all prevalence of childhood pneumonia was 22.2%. Factors like Medium and large family size, lack of formal education, birth intervals <2 years, age of 7-36 months, history of respiratory disease, disease history among children and history of measles disease last year prior to data collection, absence of latrine, lack of separate house for animal, using charcoal, chimney in the house, absence of window, severely underweight, lack of receiving vitamin A and immunization were found as significantly contributing factors of pneumonia.
Results also showed that 63.6% of respondents had poor knowledge, 38.2% with negative attitude and 42.5% improper practices towards childhood pneumonia prevention and control.
Majority of FGD discussants perceived as pneumonia is dangerous and seek health care, but showed gap of identifying the exact causes of childhood pneumonia, transimision way, sign and symptom as well as prevention mechanism.
Conclusion: Current study confirmed that, there is substainatially high prevalence of child hood pneumonia and remained as public health problem. Likewise poor knowledge and practice of communities’ were also obtained towards pneumonia prevention and control mechanisms. Thus, researcher developed awareness and prevention strategies to assist and strengthen the prevention and control of childhood pneumonia. Health planners and managers recommended to utilise the strategies to reduce child morbidity and mortality.
All authors declare that they have no competing interests.
The financial support for the current study was obtained from University of South Africa and NORAD project of Hawassa University and Derese Desalegn Buta is an author who received an award. The funded agency did not take part in study design, data collection and manuscript preparation process.
I declare that the above thesis is my own work and that all the sources that I have used or quoted have been indicated and acknowledged by means of complete references.
I further declare that I submitted the thesis to originality checking software and that it falls within the accepted requirements for originality.
I further declare that I have not previously submitted this work, or part of it, for examination at Unisa for another qualification or at any other higher education institution.
Signature  Date November 25/2021
Date November 25/2021
DEVELOPMENT OF AWARENESS AND PREVENTION STRATEGIES ON PNEUMONIA AMONG UNDER FIVE CHILDREN IN SIDAMA REGIONAL STATE, ETHIOPIA
STUDENT NUMBER: 62136313
NAME OF STUDENT: DERESE DESALEGN BUTA
DEGREE: DOCTOR OF PHILOSOPHY: DEPARTMENT OF PUBLIC HEALTH,
UNIVERSITY OF SOUTH AFRICA
SUPERVISOR: Prof LI ZUNGU
CO-SUPERVISOR: Dr AYUK BETRAND
First and foremost infinite thanks goes to Almighty God who gave me vision with full strength, without him everything might be meaningless even my life too. His mercy, love and support make me joyful within each ups and downs.
My heartfelt thanks and appreciation goes to my dearest supervisor Professor LI Zungu for her tireless advice, guidance and support as well as understanding without her help this might not be happen really. I am proud of her patience and on time responses through the whole process of my research work.
My especially gratitude goes to my co-advisor Dr Ayuk Betrand for his amazing technical advice and guidance through all thesis chapters which I learnt a lot from his valuable comments and suggestions.
I am also thankful to UNISA for the educational chance, assigning advisor, granting the ethical clearance and the bursary offered. The UNISA staffs at all level including Ethiopian regional office deserve my appreciation and thanks for their unreserved commitment and support they did through each unclear steps and error without their involvement, which might take a time even to understand.
My thanks and love goes to my wife Ms Elsabet Shudura and my lovely daughter Kayo (Kukusha/Buchula/Mare) for your understanding and support during my study time. Dears I knew that my full engagement in the course work precluded you my time but your thoughtfulness and praying make me happier rather thinking the worries. Your understanding and patience supported me to manage and handle the every aspects safely. Much more love!
I would also like to recognize and acknowledge Hawassa University, Sidama development association, former Sidama Zone Administration Office and health department for financial and logistic support.
My thanks and appreciation goes to my friends and colleagues Mr Mengesha Boko, Mr Fitsum Dangura, Teshale Tamirat, Nafkot Birhanu, Mohamed, Getu Mulatu, Tadese Mekuria and Abiyot Fiseha for your unforgettable support and motivation you showed.
My unique and personal thanks goes to data collectors and supervisors as well as study participants for your especially commitment and engagement in my study, without your involvement and contributions this might not be happened.
I would like to appreciate and recognize scholars and experts involved in Delphi panels with sharing their plenty of experiences and practices through strategy development.
My gratitude and thanks goes to Mr Amanuel Yoseph, Dr Dejene Hailu and Dr Hunachew Beyene for your unreserved technical guidance and advice through my research work.
My especially thanks and recognition goes to all my families, brothers, sisters, father in law and mother in law. My father Desalegn Buta and my mother Almaz Echero I never forget your best wishes and praying always, which helped me yet. I pray God for your long live and health too.
Mr Solomon G/Medihin, Ms Rinnie Matlou, Dr Tsegaye Asres and Dr Tsegaye Alemu also deserve my acknowledgement for their unreserved contributions on language edition, formatting and technical assistance work respectively.
I would also like to acknowledge those all my friends who have been encouraging and supporting me in each steps, especially Mr Teklu Birhanu, Gosaye Kebato and Yohanes Esayas.
Last but not least my thanks goes to Tadese enjory, Central and Rori hotels and Gezhegn and Elfinesh resort for their patience and understanding while consuming Wifi services.
This thesis work is dedicated to our son who went to heaven in his 8th day of birth. God is good all the time!
DECLARATION Error! Bookmark not defined.
1.2 BACKGROUND TO THE RESEARCH PROBLEM... 16
1.3 STATEMENT OF PROBLEM... 17
1.4 AIM/PURPOSE OF RESEARCH.. 17
1.8 THEORIES/META-THEORETICAL GROUDING/THEORETICAL FRAMEWORK.. 18
1.8.1 Meta-theoretical assumptions. 18
1.8.2 Theoretical framework. 18
1.9 DEFINITION OF KEY CONCEPTS. 19
1.10 RESEARCH DESIGN AND METHODS. 19
1.10.3 Research population. 19
1.10.4 Data collection procedure. 20
1.10.6 Ethical considerations. 20
1.11 STRUCTURE OF THE DISSERTATION.. 20
2.2 OVERVIEW OF PNEUMONIA.. 21
2.3 BURDEN OF CHILDHOOD PNEUMONIA.. 21
2.4 LITERATURE REVIEW FINDINGS ON FACTORS ASSOCIATED WITH CHILDHOOD PNEUMONIA.. 22
2.4.1 Socio-demographic and economic factors contributing pneumonia among under five children. 22
2.4.1.1 Sex of the child as contributing factors of childhood pneumonia. 22
2.4.1.2 Household economic status as factor for the occurrence of childhood pneumonia. 22
2.4.1.3 Child’s age as pneumonia contributing factors. 22
2.4.1.4 Parental education as factors of childhood pneumonia. 22
2.4.1.5 Family size as factor of childhood pneumonia. 23
2.4.2 Environmental factors associated with childhood pneumonia. 23
2.4.2.1 Solid fuels and indoor air pollution as contributing factors of childhood pneumonia. 23
2.4.2.2 Smoking as associated factors for childhood pneumonia. 23
2.4.2.3 Overcrowding and poor ventilation as contributing factors of pneumonia. 24
2.4.2.4 Housing conditions of households as contributing factors of childhood pneumonia. 24
2.4.2.5 Hygiene and sanitation practices as factors of childhood pneumonia. 24
2.4.3 Nutrition and immunization related factors associated with childhood pneumonia. 24
2.4.3.1 Malnutrition as contributing factors of childhood pneumonia. 24
2.4.4 Immunization and related factors of childhood pneumonia. 24
2.6 THE AVAILED CHILDHOOD PNEUMONIA PREVENTION AND CONTROL STRATEGIES. 26
2.6.1 Protective interventions for childhood pneumonia prevention and control 27
2.6.1.1 Exclusive breastfeeding. 27
2.6.1.2 Adequate complementary feeding and continued breastfeeding. 27
2.6.1.3 Vitamin A supplementation: 27
2.6.2 Preventative interventions for childhood pneumonia prevention and control 28
2.6.2.2 Sanitation and hygiene. 28
2.6.2.3 Reduced household air pollution. 28
2.6.3 Treatment interventions for childhood pneumonia prevention and control 28
2.6.3.1 Improved care seeking and referral 28
2.6.3.2 Timely and accurate diagnosis mechanism to prevent childhood pneumonia deaths. 28
2.6.3.3 Appropriate use of antibiotics. 28
Theoretical FOUNDATIONS OF THE STUDY 29
3.3 THEORETICAL FRAMEWORK.. 29
3.4.1 Health Belief Model (HBM) 29
3.4.1.1 Perceived Susceptibility. 30
3.4.1.2 Perceived Seriousness/Severity. 30
3.4.1.3 Perceived Benefits. 30
3.4.1.4 Perceived Barriers. 30
3.4.1.5 Individual’s perceptions. 30
3.4.1.7 Benefits of taking the preventive measures. 30
3.4.2 Global Action Plan for Prevention and control of Pneumonia Framework. 30
RESEARCH DESIGN AND METHODS 31
4.2.1 Quantitative Research. 32
4.2.1.1 Cross-sectional study design. 32
4.2.2 Qualitative Research. 32
4.2.3 Mixed Research method. 32
4.3.3 Study sample and sampling techniques. 34
4.3.3.1 Sample size calculation. 34
4.3.3.2 Sampling techniques/procedures. 34
4.3.3.3 Eligibility criteria for being a respondent for interview.. 35
4.3.3.3.1 Inclusion criteria. 35
4.3.3.3.2 Exclusion criteria. 36
4.3.3.4.1 Dependent Variables. 36
4.3.3.4.2 Independent Variables. 36
4.3.4 Data collection process and tool 36
4.3.4.1 Data collection approach. 36
4.3.4.2 Research data collection tool 36
4.3.4.3 Training provided for data collectors and supervisors. 37
4.3.4.5 Data collection process. 37
4.3.5 Ethical considerations. 38
4.3.5.1 Protecting the Rights of Institutions. 38
4.3.5.2 Protecting the rights of respondents. 38
4.3.5.3 Scientific integrity. 39
4.3.6 Processing and analysis of data. 39
4.3.6.2.1 Analysis of quantitative part 40
4.3.6.2.2 Analysis of qualitative part 40
4.3.6.2.3 Analysis of Delphi method data. 40
4.3.7 Validity, Reliability and Trustworthiness. 40
4.3.7.2 Reliability of the research instrument 40
ANALYSIS AND PRESENTATION OF THE RESEARCH FINDINGS 41
5.2 DATA COLLECTION, MANAGEMENT AND ANALYSIS. 41
5.3 RESEARCH RESULT FOR QUANTITATIVE PART OF STUDY. 41
5.3.1 Response rate and residence of respondents. 41
5.3.2 Socio-demographic and economic characteristics of respondents. 42
5.3.2.1 Wealth index of households. 43
5.3.3 Socio-demographic characteristics of surveyed child. 43
5.3.4 Environmental and housing characteristics of study respondents. 44
5.3.4.1 Availability of latrine and solid waste management 44
5.3.4.2 Housing characteristics of the respondents’ 44
5.3.4.3 Households energy source. 45
5.3.5 Nutrition related characteristics of surveyed child. 46
5.3.6 Vitamin A supplementation, deworming and immunization status of child. 47
5.3.7 Behavioural and disease status of child’s family. 47
5.3.8 Prevalence of childhood pneumonia and associated factors in Sidama Regional State. 48
5.3.8.1 Prevalence of pneumonia among under-five children. 48
5.3.9.1 Heard about pneumonia and source of information. 58
DISCUSSION OF THE RESEARCH FINDINGS 67
6.2 PREVALENCE OF CHILDHOOD PNEUMONIA AND ASSOCIATED FACTORS. 67
6.2.1 Prevalence of pneumonia among under five children in Sidama Regional State. 67
6.2.4 The association between environmental factors and the occurrence of childhood pneumonia. 68
CONCLUSIONS, RECOMMENDATIONS AND LIMITATIONS 70
7.2 SUMMARY AND INTERPRETATION OF THE RESEARCH FINDINGS. 70
7.2.1 Socio-demographic and economic characteristics of respondents. 71
7.2.2 Socio- demographic characteristics of child. 71
7.2.3 Prevalence of pneumonia among under-five children. 71
7.2.4 Key factors associated with the occurrence of pneumonia among under-five children. 71
7.4.1 Recommendations for woreda health offices, health centers and health posts. 72
7.4.2 Recommendations for Sidama Regional Health Bureau. 72
7.4.3 Recommendations for health sector partners and professional associations. 72
7.4.4 Recommendations to the Federal Ministry of Health. 72
7.4.5 Recommendations for further researchers. 72
7.5 CONTRIBUTIONS OF THE STUDY. 73
7.6 LIMITATIONS OF THE STUDY. 73
8.2 GUIDING PRINCIPLES OF THE STRATEGIES. 73
8.3 VALIDATION MECHANISM... 73
8.4 PURPOSE AND OBJECTIVES OF THE STRATEGIES. 73
8.4.1 Purpose of the strategies. 73
8.4.2 Objective of the strategies. 73
8.5 SCOPE OF THE STRATEGIES. 73
8.6 BASIS FOR THE DEVELOPMENT OFTHE STRATEGIES. 73
8.7 INTEGRATION OF THE FINDINGS WITH THE THEORETICAL FOUNDATION.. 74
8.7.1 Individual’s perceptions. 74
8.7.3 Benefits of taking the preventive measures. 75
8.8.1 Development of strategies. 76
8.8.1.1 Strategy one: Health communication and promotion. 76
8.8.1.1.1 Community mobilization. 76
8.8.1.1.2 Health education. 77
8.8.1.1.4 Social marketing. 78
8.8.1.4 Strategy four: Treating children who become ill with pneumonia. 78
8.8.1.5 Strategy five: Improving the utilization of maternal and child health services. 78
8.9 CONCEPTUAL FRAMEWORK FOR AWARENESS AND PREVENTION STRATEGIES OF CHILDHOOD PNEUMONIA 79
8.9 PRIORITY AREAS FOR ACTION.. 79
8.10 MONITORING AND EVALUATION.. 81
8.11 IMPLIMENTATION STRATEGIES. 83
8.12 STRATEGIES DISSEMINATION PLAN.. 83
Figure 4.1: Map of study site, Ethiopia, 2020. 33
Figure 5.1: Wealth index of households in Sidama Regional State, Ethiopia: 2020 (N=843) 43
Figure 8.1: Diagrammatic presentation of Delphi group data collection and analysis. 74
Figure 8.3: The WHO health system framework/the six building blocks of health system (WHO 2007:3). 79
ANNEXURE A: ETHICAL CLEARANCE GRANTED FROM UNIVERSITY OF SOUTH AFRICA.. 88
ANNEXURE B: LETTER OBTAINED FROM SNNPR HEALTH BUREAU TO CONDUCT RESEARCH.. 90
ANNEXURE C: LETTER OF PERMISSION FROM FORMER SIBAMA ZONE HEALTHDEPARTMENT. 91
ANNEXURE D: INFORMATION SHEET AND CONSENT FORM... 91
ANNEXURE E: DATA COLLECTION TOOL FOR QUATITATIVE PART OF STUDY (ENLISH VERSION.. 92
ANNEXURE G: FGD GUIDE AND CONSENT FORM FOR QUALITATIVE DATA COLLECTION (ENGLISH VERSION) 108
ANNEXURE H: FGD GUIDE AND CONSENT FORM FOR QUALITATIVE DATA COLLECTION (SIDAAMU AFOO VERSION) 109
ANNEXURE I: COMMENT AND FEEDBACK FORM FOR DELPHI GROUP. 110
ANNEXURE J: BIBLIOGRAPHY OF DELPHI TECHNIQUE INDIVIDUALS. 110
AIDS: Acquired immunodeficiency syndrome
AOR: Adjusted odds ratio
ARI: Acute respiratory infections
CHERG: Child health epidemiology reference group
CI: Confidence interval
COR: Crude odds ratio
CSA: Central statistical agency
DPT: Diphtheria, tetanus and pertussis
EDHS: Ethiopian demography and health survey
EPI: Expanded programme on immunization
FGD: Focus group discussion
FIRS: Forum of international respiratory societies
FMOH: Federal Ministry of health
GAPP: Global action plan for pneumonia prevention
GAPPC: Global action plan for the prevention and control
GVAP: Global vaccine action plan
HAD: Health development army
HBM: Health Belief Model
HEW: Health extension worker
HHs: Households
Hib: Homophiles influenza type b
HIV: Human immunodeficiency virus
IMNCI: Integrated management of childhood illness
IVAC: International vaccine access centre
KAP: Knowledge, attitude and practice
LMICs: Lower middle income countries
MCV: Measles vaccine
MDG: Millennium development goal
MNCH: Maternal and child health
MUAC: Mid upper arm circumference
NEB: National Electoral Board
NGO: Non-governmental organizations
OCA: Organizational capacity assessment
ORS: Oral rehydration solution
PCV: Pneumococcal conjugate vaccines
PMTCT: Prevention of mother to child transmission
PPP: Public Private Partnership
RR: Respiration rate
SDG: Sustainable development goals
SNNPR: Southern nation nationalities and people’s region
SPSS: Statistical package for the social sciences
SRS: Simple random sampling
TB: Tuberculosis
UN: United Nations
UNICEF: United Nations Children’s Fund
UNISA: University of South Africa
URI: Upper respiratory infections
USAID: United States Agency for International development
VIP: Ventilated improved latrine
WASH: Water, sanitation and hygiene
WHO: World health organization
Pneumonia is one of the acute lower respiratory tract infections which can be caused by bacteria or viruses or other micro-organisms those cause inflammation of the lungs, that makes difficult for the oxygen breathe in and get into bloodstream. Most of the severe or fatal pneumonia is caused by bacteria (Save the Children 2017:6).
The signs and symptoms of childhood pneumonia can be cough with or with out fever, chills and difficulty in breathing. Its severity could be ranged from mild to severe and might be affected by the factors like type of micro-organisms causing the lung infection, age of persons and their health status. The likely vulnerable groups are under five children and 65 or older people who have co-morbidies (WHO 2019a:1-2)
Globally pneumonia remained as the leading cause of mortality among children under five years old; killing about 2,216 children in a day. In 2017 (WHO 2019b:1) childhood pneumonia accounted nearly 15 per cent of the 5.4 million under-five deaths worldwide and killing around 808,694 children. Most of its vulnerable age groups were less than 2 years old children.
Pneumonia is a major cause of illness and death in under five children in resource Low Countries. In the last decade there have been different improvements and new interventions, resulting in a significantly reduction in pneumonia incidence and improved outcome (WHO 2019a:1). In 2015 countries like India, Nigeria, Indonesia, Pakistan, and China alonenly contributed more than 54% of all global cases of pneumonia. Similarly 49% of global pneumonia deaths occurred in India, Nigeria, Pakistan, Democratic Republic of Congo and Ethiopia McAllister et al 2019: e47).
Although there have been improvements globally; the challenge posed by pneumonia has persisted in the above mentioned five countries where half of all under-five deaths registered in 2018 occurred in these countries (WHO 2019a:1).
Ethiopia is 6th leading country from the top 15 countries those estimated with the highest number of under five deaths due to pneumonia and diarrhoea, with the 15 deaths/1000 live births per year according to international vaccine access centre (2016:6). Pneumonia is a leading cause of under-five children in Ethiopia. It killed more than 32,000 children under-five in 2018 which mean more than 4 children every hour and shares 17% of all causes of deaths. Pneumonia can be prevented easily by different cost effective interventions like proper nutrition, immunizing the children, exclusive breastfeeding, appropriate complementary feeding and hand washing (Save, UNICEF & every breath count 2019:1-2).
According to the annual report of Health Bureau of southern nation, nationality and peoples regional State as well as Sidama zone health department (2018:25-32) pneumonia registered as the first leading cause of both illinesses and deaths in the study area. In the budget year of 2017/18 it caused 339,152 morbidity cases in the southern region and from these 42,830 cases registered in the Sidama zone.
According to the report of Save the Children (2017:34) the early recognition of pneumonia and its danger signs can help caregivers and or health care workers to prevent deaths of children due to childhood pneumonia. Thus, establishing the proper health information and communication systems to provide evidences on childhood pneumonia to the communities, can contribute to control burden of pneumonia. Mothers/caregivers can easily identify signs and symptoms of pneumonia and seek appropriate care for their children as if they got information and empowered very well.
The current research aimed to develop awareness and prevention strategies through assessing the overall prevalence of pneumonia among under five children and its contributing factors like socio-demographic, environmental, behavioural and nutritional as well as immunization related determinants. Additional the study was also explored the level of knowledge, attitude and practice of mothers/caregivers towards childhood pneumonia prevention and control in Sidama Regional State, Ethiopia.
The study gives an insight into the household determinants of childhood pneumonia and assists to recognize the actions to be prioritised and recommends prevention and awareness creation strategies for the better prevention and control of childhood pneumonia in the study area.
Global pneumonia occured as one of the most common infectious diseases which affects millions of life every day. It remained as immediate cause of death for young children in the poorest countries. The World Health Organization and the United Nations Children’s Fund together developed and promoted the approach called Integrated Management of Childhood Illness (IMCI), for the better patient management and significantly reducation of morbidity and mortality those caused by common childhood diseases, including pneumonia. However deaths of children due to pneumonia are declining slowly than the other major killers of diseases, where the high-burden countries in sub-Saharan Africa registering the slowest progress (Save the Children 2017:5; Miller et al 2014:24).
According to the report of UNICEF (2016a:7), deaths of children due to pneumonia concentrated within the poorest countries. Low and lower-middle income countries account more than 90 percent of pneumonia and diarrhoea deaths together. Furthermore the poorest countries share a disproportionate burden of pneumonia deaths; where more than 30% of all pneumonia and diarrhoea deaths are concentrated. Morbidity and mortality due to pneumonia also disproportionately affects the youngest children whose about 80% of deaths associated with pneumonia.
Pneumonia remained a major cause of illinesses and deaths among under five children and deaths due to pneumonia has been declining more slowly than other diseases of child mortality such as malaria, measles and HIV in 2015. Accordingly, reports from UNICEF (2016b:7) and Save the children (2017: vii) revealed that around 735,000 childhood pneumonia deaths may be registered in 2030 if no significant progress is made.
Childhood morbidity due to pneumonia in developing countries can be associated with behavioural, socio-economic and environmental factors. Having a better knowledge on such underlying risk factors of childhood pneumonia is one of the strategy to protect children against pneumonia (Mihrete et al 2014:1; Diaz et al 2013:1). Improper nutritional status (micronutrient deficiency as well as lack of breastfeeding), HIV infection, exposure to indoor air pollution, overcrowding, premature birth, and poor living conditions have also been reported to influence the occurrence of childhood pneumonia (Dadi et al 2014:1; Fekadu et al 2014:1; Ghimire et al 2012:1). However, only limited data exist about the knowledge, attitude and practice of households towards childhood pneumonia prevention and control at the current study.Thus, there is a need for further research to reveal the influence of the above-mentioned factors on childhood pneumonia.
Improvements those showed global to reach the children who are losing their life because of pneumonia are not fast or fair enough across the globe. Children from the poorest countries are two times more likely to die before their 5th birthday compared to those from developed countries. This is because of undernutrition and lack of quality health services including immunizations, diagnosis and treatment of common childhood illnesses. Due to this, iInterventions that may save thousands of lives each year are not reaching children with the greatest need (Save, UNICEF & every breath count 2019:1).
World Health Organization (2013:5-9) reported that pneumonia is a common problem for everybody and its severity can be increased by different factors like medical conditions, health behaviours and environment. Most of the time infants and children below two years of age are at increased risk of pneumonia, because of lack of well developed immune systems.
In 2009 WHO and UNICEF launched the new approach called Global Action Plan for the Prevention and Control of Pneumonia framework (GAPP) global, with the aim to achieve that every child should be protected from pneumonia through a healthy environment and access to preventive and treatment measures. The GAPP brought a better opportunities to integrate activities as well as capture synergies and efficiencies (WHO/UNICEF 2013:5-7&38). It proposed the different interventions for preventing and controlling of pneumonia among under five children; through protecting them by establishing and promoting good health practices, preventing them from becoming ill by ensuring healthy environments and universal coverage of immunization, HIV prevention and treating children who are ill from pneumonia with appropriate treatment.
The GAPP framework also aimed to strengthen the countries to achieve impacts through analysing their local data, intervening on the results and continuously monitor and evaluate their progress towards clear and achievable goals by 2025. These goals helped to reduce child mortality due to pneumonia to less than 3/1000 live births and reduced the incidence of severe pneumonia by 75% compared with 2010 levels. Likewise it also helped to reduce the global burden of stunted children by 40% compared with 2010 levels. Additional targets like 90% full-dose coverage of relevant vaccines, 90
LITERATURE REVIEW
The chapter presents the review of literature accessed from different sources like books, journals, published articles, governmental as well as non-governmental organizations’ reports, EDHS, WHO factsheets and documents, UNICEF reports and global as well as national plans setted regarding childhood pneumonia prevention and control. Researcher reviewed or could access those materials via enternet, google scholar and pubmed, searched with using key words like, childhood pneumonia, prevalence of under five pneumonia, factors associated with childhood pneumonia, childhood pneumonia prevention and control strategies, KAP of mothers/caregivers towards under five pneumonia and other feasible sentences as well as phrases were used. The literature review starts with the general overview of childhood pneumonia, burden and its associated factors like socio-demographic, environmental, and nutritional. It also covers KAP of mothers towards childhood pneumonia prevention and control with its associated factors of and lastly the availed childhood pneumonia prevention and control strategies were also discussed under this chapter.
Pneumonia is one of the infectious disease of the children that can cause infection of the lungs and it can be caused by bacteria, viruses or fungi. The infections of pneumonia may causes the alveoli, to become inflamed and fill up with fluid or pus that can make it difficult for the oxygen we breathe in to and get into our bloodstream. The most common symptoms of pneumonia are cough, fever, chills, and trouble breathing. The severity of pneumonia can be categorised into mild, moderate and severe. The streptococcus pneumonias is one of the most common cause of bacterial pneumonia in children, followed by Haemophilus influenzae type b; whereas respiratory syncytial virus is the among most common viral cause of pneumonia; and pneumocystis jiroveci is responsible for at least one quarter of all pneumonia deaths in infants infected with HIV (WHO 2014:1-4).
Factors like germ causing the lung infection, age of idividuals and their overall health status can determine the overall seriousiness of pneumonia case. Pneumonia can affect the most vulnerable groups of communities those are infants and young children, adults 65 years or older, and people who have co-morbidies (WHO 2019a:1-2).
According to study conducted by Maranu and Zar (2019:4), the pneumonia caused aetiologies have been increasingly ascribed to multiple organisms as detected by molecular testing and they can be categorized as bacteria, virus and fungi. Regarding their classifications, bacteria types are staphylococcus aureus, haemophilus influenza, streptococcus pneumonia, mycobacterium tuberculosis, bordetella pertussis, klebsiella pneumonia. The viral categories are respiratory syncytial virus, rhinovirus influenza, human Meta, adenovirus, para influenza virus, rhinovirus measles virus herpes viruses and those fungal is Pneumocystis jirovecii.
The pneumonia causative infectious agents can be transimitted through airborne droplets such as coughs or sneezes inhaled into the lungs, direct oral contact with someone who has pneumonia through kissing and during or shortly after birth, the babies are also at a higher risk of developing pneumonia from coming into contact with infectious agents through birth canal, or from contaminated instruments if used for delivery (FMOH).
Approaches like integrated management of neonatal and childhood illnesses (IMNCI) and integrated community case management (ICCM) can be used to assess and diagnose the sick children with cough or difficult breathing those with symptoms of pneumonia. It is possible to classify pneumonia as severe or non severe based on presence or absence of danger signs like stridor, chest in-drawing and or inability to feed or drink. Health workers can use standard guidance for monitoring the child’s breathing rate with a timer and observing the child for chest in-drawing. Thus childhood pneumonia can be identified by a breathing rate of 50 or more breaths per minute, for children between the ages of 2-12 months and 40 breaths per minute for those children from 12 months to 5 years. If pneumonia diagnosed the child should be given antibiotics (Amoxicillin) and sent to home, or referred to a health facility for further care, depending on the severity of the symptoms (WHO 2014:2-3; FIRS 2017:17).
According to Ashraf (2014:63); pneumonia can be classified as the following:-
Pneumonia: For child (2 months to 5 years), can be defined as a cough or difficult breathing with or without fever and having only fast breathing, but no other signs and symptoms of severe disease like chest in-drawing, stridor and or unable to eat or drink.
Severe pneumonia/very severe disease: in child can be cough or difficult breathing or fast breathing and with one of the signs and symptoms of severe diseases (stridor, chest in-drawing, unable to feed/drink, lethargy and vomiting).
World Health Organization (2019a:3), proposed that under five pneumonia can be prevented through ensuring proper immunizations, adequate nutrition with exclusive breast feeding, reducing indoor air pollution, accessing good housing conditions, encouraging good hygiene practices and availing cotrimoxazole prophylaxis for children infected with HIV. Likewise engaging the community and encouraging their participation may also help to reduce morbidty as well as mortality of children due to pneumonia.
Early diagnosis and management of childhood pneumonia is one of the critical area which can help the reduction of morbidity and mortality of child. It can be achieved through increased community involvement and awareness. For this the improved diagnostic tests like better sampling procedures and rapid detection of infectious agents are needed which enables the targeted therapy. In contrary unwise use of antibiotics may agravative the situation of emergence and bacterial resistance. However the proper use of antibiotics may decrease the challenge related with antimicrobial drug resistance (FIRS 2017:18).
Of the 2.56 million pneumonia deaths global in 2017, majority of victims were under five children and it is the leading cause of mortality. Although too many children still die today even if there has been a three (03) fold reduction in child deaths due to pneumonia globally since 1990 (Dadonaite and Roser 2019:1).
Pneumonia remained as a leading cause of child illiness and death in low and middle income countries (Marangu and Zar 2019:3). The findings from the study conducted in Philippines showed that childhood pneumonia remained as the public health important issues and the results obtained as incidence rates of pneumonia episodes were 105, the episodes of severe pneumonia 61 and deaths associated with pneumonia were 0.9 per 1,000 person-years (Kosai et al 2015:1).
According to the research findings which was conducted in India, (AwasthiI et al 2019:1) about 24.6% children suffered from community acquired pneumonia within past 12 months preceding the survey and from these 4% of children were hospitalized. Another study conducted in two slums of India revealed that the prevalence of childhood pneumonia was 16.3% (Nirmoliaa et al 2017:1).
According to the missing piece world pneumonia day report (2018:23), almost 2.6 million mortality due to pneumonia were concentrated in sub-Saharan Africa, south Asia, and south East Asia. Sub-Saharan Africa alone share the largest number of pneumonia deaths, followed by South Asia and South East Asia. In sub-Saharan Africa, more than 60% of pneumonia deaths are concentrated among under five children, while in the developed region, 86% pneumonia deaths are concentrated among the older peoples whose age over 70 years. In contrast, South Asia and South East Asia carry a double burden due to pneumonia deaths, with significant deaths among both children and the elders. Furthermore in South Asia under five deaths account 40% and adults over 70 years account 34% of deaths due to pneumonia while in South East Asia 14% of pneumonia deaths were among children and 60% were among the older age group.
The result of systematic analysis conducted globally, regionally, and nationally to identify the causes of under-5 mortality between 2000–2015 showed that pneumonia was the leading cause of deaths among under five children in sub-Saharan Africa (Liu 2016:3027). Similarly the study conducted in Ghana (Osei et al 2018:1) showed that prevalence of under-five pneumonia was found to be 18.4% with a mortality rate of 12.7%.
Ethiopia is among high childhood pneumonia burdened countries. The report of Ethiopian Demography and Health Survey (2016:26) showed that the prevalence of acute respiratory infections was 7% with the significant differences of results across the regions. In addition a study result carriedout in Munesa District, Ethiopia revealed that the magnitude of community acquired pneumonia was 17.7% (Lema et al 2019:1). Another research employed in Northwest, Ethiopia revealed that prevalence of childhood pneumonia was 16.1% (Fekadu and Mamo 2014:1). Similarly, a study conducted in Southwest, Ethiopia showed that the prevalence of childhood pneumonia was 28.1% (Lema et al 2018:1).
Finally, previous findings by Yoseph and Fantahun (2019:2) indicated that the prevalence of Pneumonia was found to be 20.68% among under five children, which is high as compared to study findings from Wondo Genet district, Ethiopia which recorded a prevalence of 33.5% (Abuka 2017:10).
It is known that global morbidity of child as well as mortality due to pneumonia can be contributed by socio-demographic and economic factors like age of child, educational status and occupation of mothers/caregivers, economic status of families, residence and number of family in the household and environmental factors such as housing conditions, availability of toilet and source of water, poor management and disposal of the child’s stool, (Dadonaite and Roser 2019:6-9; Amugsi et al 2015:1).
Evidences from the past studies revealed that different factors like child as well as maternal related, environmental, socio-economic status of households, co-morbid diseases like HIV/AIDS and malaria, lack of breastfeeding and poor nutritional status of the child are important risk factors for childhood pneumonia especially common in low resource countries (Dadi et al 2014:1; Banda et al 2016:153).
Sex of child is one of the contributing factor for several illinesses. However, the contribution of sex for the occurrence of pneumonia remained unclear and no agreement has been reached in the literature (Ramachandran et al 2012:889, Muenchhoff & Goulder 2014:120). According to the literature review study conducted majority of the respiratory tract infections are more common and severe in males than females and also leading to higher deaths too. Commonly obtained that lower respiratory tract infections occurred in males. This was guessed as the greater resistance found in females due to their enhanced Th1 immune response (Muenchhoff and Goulder 2014:124-5; Falagas 2007:1845). Similar result was obtained from the case control study conducted in Urban part of Bangladesh, which revealed that being male was risk factor of childhood pneumonia (Ram 2014:968).
According to facility based study conducted in Sudan childhood pneumonia was more prevalent in male than female children, which revealed a relationship between gender and pneumonia (Gritly et al 2018:60). Another birth cohort research employed in South Africa reported that boys had a greater incidence of pneumonia than girls (Roux et al 2015:e95). The similar results were obtained from the studies done in Germany and Ethiopia which showed that being male increases the risk of having pneumonia (Lema 2019:1; Kolditz 2016:32). On the contrary, findings obtained from the case control study carriedout in Brazil revealed that being a male gender was found as protective factor for the occurrence of childhood pneumonia (Lima et al 2016:1).
Worldwide, poor economic status and living conditions can be taken as risk factors for illnesses and associated with poorly utilization of health care services.
Previous studies revealed that children who from their households’ with poor economic status are more likely affected by pneumonia infections than children living with better economic status (Amugsi et al 2015:1; Hemagiri 2014:47). Over all, a better income may help to have better housing conditions, presence of clean fuel for cooking, better food, media access and health seeking behaviour. But the poor communities are likely to live in poor sanitation and hygienic practices, which might increase their exposure to infectious agents (Cardoso et al 2004:1). It is also stated that communities with poor economic status may have more family size and live in crowded houses where the housing conditions are suitable for the transmission of infectious agents (Amugsi et al 2015:1).
Different previous studies revealed that low economic status can contribute childhood pneumonia. For instance a studies conducted in India reported that children those from low socio economic status are at higher risk of developing childhood pneumonia (Gupta and Bhadrala 2019:949; Nirmolia et al 2017:1). Similar result was also obtained from the case control study conducted in Urban Dhaka, Bangladesh, which revealed that poor economic status was the predictors of pneumonia among under-five children (Ram 2014:968). In addition hospital based case control study conducted in Bellary and another descriptive study from Sudan revealed that poor economic status of the family was predictor of childhood pneumonia (Gritly et al 2018:60; Hemagiri et al 2014:47).
Pneumonia can affect the children regardless of all age. However, the evidences showed that younger age groups of children are at more risk of developing childhood pneumonia than others. For instance, a population based study conducted in Germany and a hospital based study conducted in Sudan revealed that less than one year age children were more affected with pneumonia than children of older age groups (Kolditz et al 2016:32, Gritly et al 2018:60). Similarly facility based research employed in Bellary reported that the younger age was found as contributing factor for childhood pneumonia (Hemagiri et al 2014:47).
In addition, a study done in Oromia zone of Amhara region revealed that children at age range 2-11 months were 85% more likely to suffer from pneumonia as compared to older age. Another facility based research employed in Sidama zone alluded that children aged between 2-12 months were 4 times more likely to develop pneumonia than older age group (Abuka 2017:19; Dadi et al 2014:1).
Parental education is another important risk factors of children’s health. The level of maternal education is inversely related to the occurrence of childhood illinesses as well as deaths, mothers with better educational status are more capable about taking care of their children than their contraries which require all necessary recognition and implementation of simple home care and also early presentation to health-care facilities (Gothankar et al 2018:1).
Education helps to improve the socio-economic lives of the families; hence helping in avoidance of some of the risk factors of acute respiratory infections including pneumonia (Ujunwa and Ezeonu 2014:95). However lack of education and poor awareness of the mothers may have negative impact the reduction both morbidity and mortality of children due to pneumonia which can be also the big challenge for public health interventions. A research carriedout in India revealed that gap of maternal education contribute the prevalence of pneumonia (Nirmolia et al 2017:1).
Well educated mothers relatively can understand the any risk factors of child health and may try to prevent them from the exposures while the reverse is true with uneducated mother or mothers with low level of education. An institution based study conducted in India as well as in Vietnam showed that low literacy status of mothers was the significant contributor for the occurrence of acute severe pneumonia in under five children (Hoang et al 2019:274; Gupta and Bhadrala 2019:949).
The study findings from different countries or areas showed that children with low educational level of mothers have high probability of developing childhood pneumonia. An Institution based case control study conducted in India and another hospital based descriptive study, from Sudan showed that low literacy level of mothers had significant association with childhood pneumonia (Gritly et al 2018:60 Hemagiri et al 2014:47).
The same is true with father’s educational level as that the less educated mother’s positively contributes for the occurrence of childhood pneumonia; where the households with high level educated fathers, there is protective associations. According to the result of study done in Ethiopia showed that the prevalence of pneumonia was significantly contributed with the father’s lower level of education grades (1 - 4) and (5 - 8) as compared to higher educational level (Dadi 2014:1).
A household’s family size is another important risk factors for childhood pneumonia. Three different studies conducted at different areas of India with different study designs and periods revealed that overcrowding, due to large family size, was found as a contributing factor for the occurrence of childhood pneumonia (Gupta and Bhadrala 2019:949, Gothankar et al 2018:1 & Hemagiri et al 2014:47.
A hospital based study which was done in Southeast Nigeria, reported that having large family size obtained as contributing factor for the occurrence of childhood pneumonia than those from small family size (Ujunwa and Ezeonu 2014:95).
Environmental factors are major determinants for different human diseases. According to the literature review study conducted on childhood pneumonia in developing countries; environmental factors like biomass combustion, exposures to wood combustion, tobacco smoking, day care attendance for children, any refugee environment and school resumption, were found as associated factors with pneumonia.
Positive upper respiratory infections, contact history of households and rainy/winter season were also found as contributing factors of pneumonia (Johnson and Abdulkarim 2013:5).
According to the WHO fact sheet (2018a:1), about three billion people has been using solid fuels like; wood, charcoal, crop wastes, coal and dung. Some anothers have been using kerosene in open fires and inefficient stoves for cooking and most of these people are poor and from developing countries. These cooking practices are inefficient use of fuels and technologies that can produce household air pollution which could be the suitable environment for childhood pneumonia transmission.
According to WHO (2018b:2) report of air pollutions and child health, the use of polluting fuels and technologies are common problem for the developing pollution which then contributes respiratorty diseases including pneumonia among under five children. Almost all low and middle income countries are highly burdened about air pollutions. For instanse 83% of the population has been affected in the African region, 59% in the South-East Asia region and 42% in the Western Pacific Region. The evidence obtained from systematic review study carriedout in LMIC countries revealed that solid fuel as a proxy for PM2.5 reported as major contributing factors for childhood pneumonia (Adaji et al 2019:3208).
The findings from four preceding studies conducted in different parts of India using different study designs and time revealed that using biomass fuel, cooking fuel, indoor air pollution and poor indoor household air pollution were strongly associated with the occurrence of childhood pneumonia (Gupta and Bhadrala 2019:949; Nirmolia et al 2018:1; Yeimo et al 2018:307 & Hemagiri et al 2014:47). The same findings were also obtained from a reviewed study done in India, which showed indoor air pollution was found as predictors of childhood pneumonia and recommended as proper attention should be given to minimize the use of such contributing factors (Yadav and Awasthi 2016:83).
A preceding study conducted in South Sudan, around 99% households used solid fuels for cooking and this put the children at risk of pneumonia related mortality, due to household air pollution. To minimize such risks the use of clean or improved stoves for cooking was highly advised in South Sudan (Abd-Elfaraga & Langoyab 2016:36).
As Ethiopian demography and health survey report (2016:11) indicated 95% of households in Ethiopia used the same type of solid fuel for cooking with virtually all of these households using wood. According to cross-sectional studies conducted at public hospitals in Southwest and Northwest Ethiopia, the use of wood and charcoal were the main fuel source for cooking and as the major contributors of childhood pneumonia (Lema et al 2018:25 & Fekadu et al 2014:150).
It is obtained that air pollution and passive smoking can elevate the risk of pneumonia occurrence. Studies revealed that the presence of indoor air pollution can double the probability of a child developing pneumonia and decreases its recovery. In 2017, indoor air pollution estimated to cause 29% childhood pneumonia deaths and outdoor air pollution shared another 18% of all deaths (Dadonaite & Roser 2019:7). Detailed findings reported that passive smoking children are more likely to develop pneumonia than non-exposing children. Furthermore, Dadonaite & Roser (2019:7) reported that exposure to second hand smoke led to 61,000 deaths due to lower respiratory disease among childhoods in 2017. Also, findings of a study conducted by Ujunwa & Ezeonu (2014:95) in Enugu, Southeast Nigeria showed that parental smoking was a risk factor for childhood pneumonia. These findings were inline with the findings of a case control study carried out in Ethiopia that showed parental smoking was contributing factor of childhood pneumonia (Geleta et al 2016:1).
Overcrowding is one of the means that may create fertile opportunities for communicable diseases like pneumonia.
Children living inside the home environment where there were inadequate ventilation conditions could be more susceptible to childhood pneumonia, while toddlers who live in the home environment with adequate room ventilations have a lower risk of the same disease. The findings of a cross sectional study from India and another hospital based case control study from Brazil reported that overcrowding was a contributing factor for childhood pneumonia (Lima et al 2016:1 & Hemagiri et al 2014:47). Similarly, the result of case control study conducted in Urban Dhaka, Bangladesh revealed that overcrowding was a contributing factor to pneumonia (Ram et al 2014:968). An Ethiopian study also confirmed that there was significant relationship between occurrence of pneumonia among under-five children and crowded living space (Fekadu et al 2014:150).
It is known that different housing conditions like lack of separate kitchen and windows in the kitchen, number of rooms, roofing material, general sanitation, rearing cattle inside the main house, latrine availability and lack of proper hand washing can contribute to the occurrence of childhood pneumonia. The finding from case-control study design conducted in Indonesia showed that poor environmental sanitation was predictors of pneumonia among under-five children (Yeimo et al 2018:307). A research result which was carriedout in Urban Bangladesh revealed that a tin roof in the living space was found as the contributing factors for the occurrence of childhood pneumonia (Ram et al 2014:968).
Having separate kitchen with the presence of windows can be protective from the occurrence of pneumonia. For instance, institution based cross-sectional studies carriedout in different areas of Ethiopia revealed that cooking food in living room, lack of separate kitchen and lack of windows in the kitchen were risk factors of childhood pneumonia (Lema et al 2018:25; Abuka 2017:19). Similar result has also been reported in another literature reviewed study carriedout in Ethiopia which alluded that food cooking in the main house was associated for being a factor of pneumonia (Merkeb and Adane 2019:2).
Different preceding studies showed that rearing of cattle inside the main house was the determinant factor of pneumonia. A community based cross sectional and another institution-based unmatched case-control studies conducted at different areas of Northwest Ethiopia showed that rearing of cattle inside the main house found as the contributing factors of childhood pneumonia (Markos 2019:1 & Fekadu et al 2014:150)
Improper hygienic and sanitation practices are major determinants of childhood pneumonia. Study carriedout in Rwanda revealed that household toilet type was one of the associated factors with the occurrence of childhood pneumonia (Harerimana et al 2016:1). Similarly result of study conducted in Ethiopia reported that improper hand washing practice of mothers was one of the contributing factors of the occurrence of childhood pneumonia (Markos 2019:1).
Proper nutrition is essential for the development human life and keeping healthy. The essentiality and necessity of proper and balanced nutrition gets started from the very beginning of foetal development. It is important and necessary for all-rounded growth and development of body organs and physiologic functions (WHO 2000:3).
According to WHO (2005:1), malnutrition (under-nutrition) is one of the health outcomes and contributing factors for disease and which can also escalate the probability of getting illiness and death of children. Malnutrition is determinant factors of childhood pneumonia (Awasthi 2016:83; Srivastava et al 2015:1). Similarly, studies conducted in Bellary and Pakistan revealed that malnutrition to be found as significant risk factor of pneumonia among under-five children (Hemagiri et al 2014:47; Aftab et al 2016:1).
According to a review study conducted in developing countries, malnutrition was significantly associated with pneumonia (Ramezani et al 2015:1173). Similar findings were also obtained in Gambia through a case control study and reported that malnutrition remains important tractable risk factor for pneumonia. In addition, severe malnutrition was found to be the strongest predictor of severe pneumonia (Howie et al 2016:1405). Another cross sectional study design conducted in Southwest Ethiopia, shown that moderate acute malnutrition was significant factor of childhood pneumonia (Lema et al 2018:25).
There were evidences in Indian which showed that inappropriate complimentary feeding, iron deficiency (anaemia), low birth weight and pre-lacteal feeding to be predictors of under five pneumonia (Yadav & Awasthi 2016:83). There was also strong evidence between breast feeding practice and the magnitude of childhood pneumonia. According to the research conducted in different parts of India, poor exclusive breast feeding was found as predisposing factors of childhood pneumonia (Awasthi 2016:63, Srivastava et al 2015:1 & Hemagiri et al 2014:47).
Different studies from developing countries revealed that nutritional factors like micronutrient deficiencies, low birth weight, lack of breast feeding, rickets, anaemia and stunting were found to be the contributing factors of childhood pneumonia (Aftab et al 2016:1 Ramezani et al 2015:1173, Ujunwa and Ezeonu 2014:95 & Fekadu et al 2014:150). Likewise the result of literature review study revealed that suboptimal breastfeeding increase the probablity of children getting pneumonia disease and death in all age groups. Especially the death due to pneumonia was higher among those children did not breastfed compared to those with exclusively breastfed as well as propely breastfed for their ages (Lamberti 2013:1). The similarly findings were obtained from the institution based study employed in Ethiopia, which revealed that mixed breastfeeding was found as significant factor for the occurrence of childhood pneumonia (Lema et al 2018:25).
Improving the vaccination status of children can decrease the related diseases and deaths of children. There are several types of vaccines those can protect against diseases including childhood pneumonia. Commonly utilized vaccines are pneumococcal conjugate vaccines, Haemophilus influenzae type b, measles vaccine, diphtheria, tetanus and pertussis. The evidences showed that around 20 million children did not get immunized, with global coverage of three doses of DPT and one dose of the measles vaccines continuing to stall at 86% in 2018. There were also nearly 39 million children global who did not received the three doses of Hib vaccine and 71 million who did not received the three doses of PCV, putting children at higher risk of pneumonia (Save the Children and UNICEF 2019:5).
Previous Observational studies conducted at different areas of India revealed that the absence or inappropriate immunization was found to be a significant predictors of pneumonia (Gupta and Bhadrala 2019:949; Yeimo et al 2018:307). Incomplete immunization for age was found as determinants of pneumonia (Srivastava et al 2015:1; Gothankar et al 2018:1). This inappropriate immunization was mostly due to the absence of vaccines especially BCG (Gupta and Bhadrala 2019:949; Yeimo et al 2018:307). Likewise, another case control studies conducted in North-eastern Pakistan and Vietnam revealed that lack of immunization was obtained as contributing factor of childhood pneumonia (Hoang et al 2019:274 & Aftab et al 2016:1).
As part of improving child health program; WHO/UNICEF identified three critical steps namely recognizing the sickness of child, timely seeking appropriate care and treating the child with appropriate antibiotics(WHO & UNICEF 2006:2). Knowledge and attitude of the mothers/caregivers towards childhood illiness are important factors to determine child health. The knowledge, attitude and practices of mothers can directly influence the over all health status of the children hence they are the main caregivers for children in almost all societies (Mutalik & Raje 2017:30; Kanté et al 2015:3-5).
A study conducted in India revealed that majority of mothers even those who obtained formal education had poor knowledge as the illiterate counterparts (Mutalik & Raje 2017:30). Two other studies from India showed that knowledge of mothers towards the prevention and control of pneumonia was not satisfactory (Pradhan et al 2016:35 & Jena 2014:25). Similarly a study conducted in Saudi Arabia showed that 54% of the mothers/caregivers had insufficient knowledge towards ARI, including pneumonia (Alluqmani et al 2017:1959).
A comprehensive health education on aetiology or causative agent of childhood pneumonia, its prevention and management can help to establish appropriate contact between the health services provided and the community. This will help the families to identify the danger signs of acute respiratory diseases in children and to encourage appropriate and early care seeking behaviours (Mutalik & Raje 2017:32). A cross sectional study employed in Uttar Pradesh; identified that there was lack of knowledge among mothers/caregivers about under five pneumonia (Minz et al 2019:62). Another community based behavioural trial study conducted in India revealed that the level of recognition of mothers/care givers towards pneumonia and its danger signs was poor (Awasthi et al 2018:1).
Majority of past studies have analysed low knowledge of mothers regarding childhood pneumonia. Studies from Nigeria and Ghana showed that mothers were less knowledgeable towards aetiology and danger signs of childhood pneumonia (Abbey et al 2016:1 & Ukwaja et al 2012:889). Likewise in resource Low Countries, caregivers poorly recognized the symptoms associated with pneumonia.
A qualitative research conducted in Uttar Pradesh, India showed that knowledge of mothers/caregivers towards majority of danger signs of childhood pneumonia were reported to be poor,however chest in-drawing was identified as sign of sever disease (Awasthi et al 2015:1).
Majority of illiterate mothers were found to be less knowledgeable about teaching their children regarding proper hygienic practices, even though they need to care for their families. Age and educational level of mothers’ were found as the determinant factors of their knowledge towards pneumonia. Good knowledge of mothers was associated with ARI including pneumonia. The findings of the study also showed that short duration of marriage, young ages and higher education were significantly associated with better understanding and sufficient knowledge of mothers/caregivers (Alluqmani et al 2017:1959 & Pradhan et al 2016:35).
From the study conducted in Bangladesh, it was reported that majority of mothers could describe that childhood pneumonia as it is critically life costing disease, however they did not identify whether child had pneumonia or not. Different factors like presence of coughing mothers, drinking cold water and engulfing dust particles were found as the causes for childhood pneumonia but mothers did not considered the illness as serious enough. (Ferdous et al 2014:1). Majority of mothers whose children with respiratory infections often did not provide early care for their children and stick to their intention to try herbal medicine or antibiotic before hand or held confidence in traditional healer. The finding of cross sectional study which was conducted in Kenya revealed that most of the mothers/caregivers were using home remedies and only went to health facilities when the case complicated even if they felt that health institution care is the best (Ndungu et al 2018:73).
Signs and symptoms of childhood pneumonia have been perceived differently among different mothers. Report showed that mothers of children with acute respiratory infection perceived cough as ordinary occurrence and felt confident about treating themselves and showed poor ability to differentiate pneumonia, simple cough and colds (UNICEF 2014:3). But in some areas mothers have relatively good attitude towards medical care for children with pneumonia. A study conducted in Pakistan reported that mothers had a positive attitudes towards early consultation with qualified medical practitioner regarding acute respiratory infections (Bham et al 2016:1557).
Different factors contributed the negative attitude of mothers/caregivers towards health care seeking practice about childhood pneumonia. The result of study carriedout in Ethiopia revealed that lack of money, thought that no benefit for such childhood illness and thought that mild or moderate illness were found to be contributing factors for not seeking health care treatment (Awoke 2013:155).
In many countries especially rural communities have a decreased rate of health service utilization including IMNCI (Ndu et al 2015:1). A cross sectional study conducted in Saudi Arabia revealed that practice of mothers regarding childhood pneumonia prevention and control was poor. It was reported that most of them use self-medications at home without consulting doctors about the importance of home remedies rather many of them ask physicians for prescribing antibiotics (Alluqmani et al 2017:1959). Similar result was obtained from the mixed method study conducted in Ghana showed that mothers mostly practice home base care and remedies as well as allopathic care for children with pneumonia (Abbey et al 2016:1). Likewise a result of study carriedout in rural districts of Sierra Leone, showed that majority of children were not given a recommended treatment, rather some of them given traditional treatment. This was justified that most of communities’ prefere for the local availed treatments and the barriers seeking to facility care were remained even after free health care initiative launched (FHCI) (Diaz et al 2013:1).
On time health care seeking from the recognized health institutions is very important and for this to happen, mothers should be familiar with signs and symptoms of childhood pneumonia. A research conducted in Alexandria, Egypt revealed that about 57.2% of children were given home remedies prior to seeking medical advice and also nearly 26% of mothers waited ≥ 2 days before seeking medical advice (Fadl et al 2020:1). Likewise, study carriedout in Tanzania showed that the provision of care due to community acquired pneumonia in most children was delayed. About 26.6% of children were learnt to be given leftover antibiotics at home without prescribing by the physicians (Ngocho et al 2020:56).
Different studies described that factors like limited education of parents, gap of understanding the severity of the illness and or insufficient knowledge about the disease were found to be significantly associated with the delays in care seeking. Factors such as rural residence, low income of households, giving home treatment before seeking medical advice and previous episodes of pneumonia were found to push parents to use traditional treatments or self-medications at home ( Fadl et al 2020:1 and Bham et al 2016:1557). A result of qualitative research employed in Northern India, revealed that mothers consulted local medical practitioners directly; but decisions to visit doctors outside the village required consultation with husband or mother-in-law for health services of children with pneumonia (Awasthi et al 2015:1-2). Similarly, the findings of qualitative, exploratory design employed in South Africa showed that decision making about the health care utilization for a sick child was influenced by different individuals of households in addition to mothers/caregivers. It is assumed that a sick child would be treated at home or can be taken to different places like clinics, private doctors, traditional healers, faith healers and hospitals (Haskins et al 2017:1).
A qualitative study findings from the rural Oromia region of Ethiopia revealed that care givers or mothers of ill children described the cultural, social and community-based resources availablilty to reduce the uncertainty of time and strategies for accessing these resources in order to receive treatment for a sick child. (Shaw et al 2017:1).
Childhood pneumonia is the leading killer and with diarrhoea can contribute almost quarter of all deaths among the under five children in the poorest countries, especially in areas where there with poor access to health services, lack of nutritious foods and basic sanitation as well as poor hygiene and housing conditions. To reduce child deaths due to pneumonia and support countries to do so, WHO and UNICEF iniated the strategies called integrated global action plan for pneumonia (GAPP). The GAPP strategies proposed as a global framework for actions that partners can integrate and allign their efforts to reduce childhood morbidity and mortality due to pneumonia. In order to rise the awareness of communities towards pneumonia, that it is a major cause of child death, there are calls for scaling up the use of interventions of proven benefit and provide guidance on implementation and support of countries. The GAPP framework was envisioned as that every child, should be protected from pneumonia through creating a healthy environment and access to preventive and curretive measures (WHO and UNICEF 2009a:2-4).
The high concentration of pneumonia deaths and illinesses among less developed communities are the indicators, of that there is inequality within countries which also needs additional effort to reach the most vulnerable children. UNICEF established the commitment to address the equity gaps like reaching the basic causes of child mortality and to ensure that all children have the same opportunity to survive as well as reach their full potential. Fighting pneumonia could be one of the important areas which can help to reduce child mortality. The GAPP established a progressive goals for the control of childhood pneumonia and provided a roadmap for national governments as well as calls for integration and active engagement amongst all stakeholders through protect, prevent and treat framework to end childhood pneumonia by 2025.
In this regard, some of pneumonia related goals were; to decrease child deaths due to pneumonia to less than 3/1000 live births and reduce incidence of severe pneumonia by 75% compared to 2010 levels. Similarly, GAPP given the attention on universal access to drinking water in health facilities and homes, adequate sanitation in health inistitutions by 2030 and in homes by 2040 respectively, hand washing facilities (water and soap) in health facilities and homes, clean and safe energy technologies where in both health care facilities and homes by 2030 (WHO and UNICEF 2009a:1-5 and WHO/UNICEF 2013:7).
The following figure 2.1 presents the three focus intervention areas (protect, prevent and threat) of GAPP strategies to control childhood pneumonia.
Figure 2. 1: GAPP framework for protecting, preventing and treating childhood pneumonia (WHO and UNICEF 2009a:4).
It would be possible to protect the children from pneumonia infections through ensuring a safe environment, exclusive breastfeeding for first six months, balanced nutrition and preventing low birth weight, reducing air pollution and improving hand washing practices regularly (WHO/UNICEF 2013:6).
According to WHO recommendations every infants should get only breast milk and nothing else, except those treatment purpose like oral rehydration solution (ORS), medicines, vitamins and minerals if needed. Breastfeeding is global accepted and preferred method for feeding an infant hence it can benefits for the development of children and keeping physical health of mothers. It is important that breastfeeding has to be started within one hour after birth and continued for the first six months of life (Taren and Lutter 2017:361-2).
There is an evidence that breastfeeding can protect from childhood pneumonia. Proper breastfeeding can help to protect children from all infections those may lead to hospital admissions (series/breastfeeding 2017:2). According to the literature review study conducted, a suboptimal breastfeeding can increase the probability of getting pneumonia and deaths across age groups. Furthermore it was shown that pneumonia deaths were higher among those did not breastfed compared to exclusively breastfed infants and among not breastfed compared to breastfed infants and young children (Lamberti et al 2013:1).
According to WHO (2009a:4), adequate and safe complementary feeding can be started from the age of 6 months with continued breastfeeding up to 2 years or beyond. The transition from exclusive breastfeeding to predominant breastfeeding should include the introduction of complementary feeding that can be solid, semisolid or soft foods with full of energy and nutrients those availed in the community or can be provided as supplements for vulnerable infants (Taren & Lutter 2017:362).
Vitamin A deficiency is one of the contributing factors of child mortalities.. Improving Vitamin A status of deficient children can increases their resistance to infections and can reduce deaths from all possible causes by 23%. Vitamin A deficieny can be improved through routinely way or enhanced outreach base supplimetations. Sustaining the improved supplementation of vitamin A is essential, not only to eliminate vitamin A deficiency as a public-health problem, but also as a vital element of the child survival agenda (UNICEF 2007:3). The evidences showed that most of severe childhood infections are related with vitamin A deficiency. (Heidarian & Ansarinezhad 2014:57).
It is possible to prevent children from becoming ill with pneumonia by implementing actions like proper immunization, cotrimoxazole prophylaxis for HIV-infected and exposed children and zinc supplementation for children with diarrhoeal diseases (Save the Children and UNICEF 2019:5-6).
Immunizing the children is a golden strategy to reduce illinesses and deaths of under five children. It is a cost-effective intervention of children across ages including infancy. The greatest improvement of child mortality in 2000 to 2015 was due to significant reductions in vaccine-preventable diseases through immunizations (WHO 2018c:1).
Childhood pneummonia can be prevented via pneumoncocoal vaccine which is more effective than the other prevention strategies, like reduced crowding and indoor air pollutants and nutrition. The use of pneumococcal vaccine would be taken as complementary to the use of other pneumonia control strategies, such as appropriate case management, promotion of exclusive breastfeeding for first six months and the reduction of known risk factors, such as indoor pollutants and tobacco smoke (WHO 2015:44). The pneumococcal conjugate vaccine can protects against severe forms of pneumococcal diseases such are pneumonia, meningitis and bacteraemia. There are two pneumococcal conjugate vaccines those available since 2009; 10-valent (PCV10) and 13-valent (PCV13). World health organization recommends 3 primary doses of pneumococcal conjugate vaccine (WHO 2013:8).
According to WHO (2018d: 4), pure drinking water, proper sanitation and hygiene are essential to the health of human. They are not only a prerequisite to health, but also can contribute to livelihoods school attendance and helps to create resilient communities. WASH interventions include safe water, storage for portable water, latrines for sanitation and soap for hygiene, bath and hand washing practices. It also includes the promotion of key hygiene practices those can contribute in health, economic and social benefits (Gomathi et al 2017:575 and WHO & UNICEF 2013:75).
Most of deaths due to preventable illinesses are subjected to poor WASH conditions throughout the developing world. Globally the burden of disease due to poor WASH falls heavily on under five children. Washing hands with soap can reduce the risk of acute respiratory infections by 20%, thereby addressing one of the major causes of under five deaths (UNICEF 2015:3-4 &7).
According to WHO health fact sheet (2018a:1-4); household air pollution is one of the common global public health problems. The sudden exposure to pollutants in the air can affect the health of communities, across the world. Morely it affects the most vulnerable groups like children. Majority of the populations depend on solid fuels (wood, coal, crop waste and animal dung) to cook and heat their homes that can increase household air pollution which may double the risk of pneumonia. An intervention study conducted in Guatemala revealed that young children who had exposed to household solid fuels were twice more likely develop pneumonia compared to children who were not exposed (Smith 2011:1717).
Pneumonia is one of the most common infectious complications in HIV-infected patients’ leads to illiness and deaths (Seda 2016:11). Similar result was obtained from the reviewed literature study conducted and it revealed that pneumonia is the most associated pulmonary illness and remained as a common cause of illiness and deaths in the HIV-infected population (Breanne 2017:1).
Knowing and identifying the burden of the HIV epidemic is vital for planning, implementing and monitoring any health programs that attempts to tackle the impact of HIV/AIDS. This is also right for the under five children HIV epidemic, for which prevention, care, and treatment efforts lag behind those done for adults (WHO and UNAIDS 2013:3).
Cotrimoxazole prophylaxis is safe and cost effective in decreasing illinesses and deaths among HIV-infected infants and children. It can protect against the the severe opportunistic infections and supports to improve the quality of life of HIV-infected infants (WHO and UNICEF 2009b:1).
Childhood pneumonia can be treated at health centres or hospitals through case management in community (WHO and UNICEF 2009a:4). Possible treatments include improved care seeking and referral, timely and accurate diagnosis, appropriate antibiotics and oxygen therapy provisions (UNICEF 2016a:19).
On time recognition of childhood pneumonia and its symptoms supports to early care seeking and can ensure that children get to a health provider early.That also helps the care providers to assess and treat children effectively according to WHO and UNICEF standards or based on IMNCI and ICCM guidelines (UNICEF 2016a:20).
The GAPP framework considered the faster and effective diagnosis mechanisms of childhood pneumonia as part of interventions. It was planned to ncrease the level of care-seeking for childoood pneumonia by 13% among the community and reduce treatment failure by 40%. Community case management brought 32% reduction in childhood pneumonia specific mortality among community (UNICEF 2016a:43 and Bhutta et al 2013:1417).
Amoxcilline is effective treatment for bacterial pneumonia (UNICEF 2016a:20). According to the revised WHO (2014:6), guideline children with only fast breathing pneumonia and without any general danger signs could be treated with oral amoxicillin: at least 40 mg/kg/dose twice daily (80mg/kg/day) for five days. In areas with low HIV burden, amoxicillin can be given for three days and children with fast-breathing pneumonia who fail on first-line treatment with amoxicillin will better to have the option of referral to a facility where there is appropriate second-line treatment.
Children with severe childhood pneumonia need oxygen therapy to treat hypoxemia (insufficient oxygen in the blood); which is a fatal complication. Improving the access to oxygen can significantly decrease pneumonia deaths among under five children (UNICEF 2016a:20). It is known that the most common sources of oxygen are cylinders, concentrators and pipelines (WHO 2016a:21).
In this chapter, literature was reviewed and analysed on childhood pneumonia concepts, burden and associated factors from the view of worldwide to local concepts. It also discussed about the knowledge, attitudes and practices of mothers or caregivers towards childhood pneumonia prevention and control strategies. Lastly, the existing childhood pneumonia prevention and control strategies including global action plan for prevention and control of pneumonia (GAPP) framework were discussed.
The following chapter 3 presents the research paradigm.
Theoretical FOUNDATIONS OF THE STUDY
3.1 INTRODUCTION
This chapter presents and discusses the concept of framework, theoretical framework, conceptual framework, Health Belief Model and global action plan of pneumonias’ framework for pneumonia control.
3.2 A FRAMEWORK
A framework is the summary or logical structure of meaning that guides development of the study and enables the researcher to link the findings with the core body of knowledge, or it is a combination of concepts that used to explain relationships (Gray et al 2017:1060). A framework for study is a structure that provides guidance for the researcher as study questions or objectives are fine-tuned, ways for measuring variables those selected and analyses are planned (Imenda 2014:188). According to Polit and Beck (2018:550), it is a conceptual underpinning of a study and can be named as theoretical or conceptual framework.
3.3 THEORETICAL FRAMEWORK
A theoretical framework is the way of structuring or networking of different theories that have a relationships on the research topic (Kumar 2011:349). It is the framework with theory-based study or it is a theory that a researcher used to guide in his/her study. Thus, a theoretical framework is the application of theory; or a set of concepts drawn from one and the same theory to give an explanation of an event, or shed some light on a specific phenomena or research problem(Polit and Beck 2018:550, Imenda 2014:189).
3.4 CONCEPTUAL FRAMEWORK
A conceptual framework orginated from the theoretical framework and focuses on specific section that theoretical framework becomes the basis of the study. It is the aspects selected from the theoretical framework to become the basis of the research enquiry and is the basis for research problem (Kumar 2011:332). According to Polit and Beck (2018:550), conceptual framework is a framework with studies based on a specific conceptual model. Conceptual framework focuses on a limited scope, carefully put together in the form of a conceptual model, which would be immediately applicable to a particular study (Imenda 2014:189).
The conceptual framework for the current study was developed based on Health Belief Model (HBM) and global action plan of pneumonia (GAPP) control framework. These were used because of the relative applicability and interpretation of the models throughout the study. The purpose of the current study was to develop the awareness and prevention strategies on pneumonia among under five children by assessing the magnitude and associated factors of childhood pneumonia and knowledge, attitude and practice of mothers/caregivers towards pneumonia prevention and control.
The advantage of HBM is that it specifys an incloherent set of common sense beliefs that happen to explain or mediate the effects of different factors on health behaviours and are amenable to change through educational intervention. The model would be applied in different health behaviours and to provide a framework for adjusting behaviour patterns that are relevant to public health (Mark and Paul 2015:31). According to the literature review study conducted by Elvis and Francis (2015:1), HBM bargains that the readiness of people to take an action to prevent disease and promote health depend on, their level of believe about the severity of disease. However, HBM have some limitations, like it does not consider for a one’s attitude, beliefs and/or the individual determinants that can challenge a person’s acceptance of a health behaviour; it does not consider about behaviours that are habitual which may inform the decision-making process to accept a proposed inteventions; neither does it account for other factors like environmental or economic those may control or encourage the recommended actions and also it assumes that everyone has access to equal amounts of information on the illness or disease (Wayne 2019:2). By considering these limitations, the researcher used HBM jointly with Global Action Plan of Pneumonia (GAPP) control framework to develop the feasible conceptual framework for the current study.
Global Action Plan of Pneumonia control framework is relatively a comprehensive approach to pneumonia control and it includes almost all the interventions that could be implemented as necessary part of child survival that are globally recommended and has been presented with protective, preventive and threating factors for the prevention and control of under-five pneumonia (WHO and UNICEF 2009:4).
Current study tried to address the prevalence of childhood pneumonia and possible determinants with assessing knowledge, attitude and practice of mothers/caregivers that can affect the level of prevention and control of the disease. By using HBM with the GAPP framework makes the following conceptual framework (Figure 3.1), was developed with considering the possible assocated factors of childhood pneumonia, which guides the current study more effectively to develop the awareness and prevention strategies on pneumonia among under-five children.
3.4.1 Health Belief Model (HBM)
The HBM intial developed in United States Public Health Service since 1950s by a group of social psychologists to understand “the widespread failure of people to accept disease preventives or screening tests for the early detection of asymptomatic disease”; and it was later used to patients’ responses to symptoms and to compliance with prescribed medical regimen (Janz and Becker 1984:2).
The importance of the HBM is geared towards minmizing or controlling a disease conditions and aims to justify and forecaste health behaviours. The central assumptions of the HBM is that individuals will act if they feel their personal health is threatened and they perceive the benefit that health promoting activity outweighs the detriment of following through with the behaviour. The assumption is congruent with the model’s focus on health promotion and disease prevention (Tarkang and Zotor 2015:2).
The basic concepts of the original HBM is that health behaviour is determined by personal beliefs or perception about a disease and the strategies available to decrease its burden; and personal perception is influenced by the whole range of intrapersonal factors affecting health behaviour. Primarily, there were four perceptions that serve as the main constructs of the model; namely perceived seriousness, perceived susceptibility, perceived benefits, and perceived barriers (Turner et al 2004:31). Later the model proposes the cues to action which may activate the behaviour when appropriate beliefs are held. These cues include a diverse range of triggers, including individual perceptions of symptoms, social influence, and health education campaigns (Mark and Paul 2015:31-2).
3.4.1.1 Perceived Susceptibility
Individual risks or degree of susceptibility is one of the common perceptions which initiates people to adopt a healthier behaviours. The more perceived risks, the more likelihood of engaging in behaviours to reduce the risk. A person’s perception towards the relevance of health problem can help the individuals to take the required action to prevent the health problem thus there must be activities that improve the individual’s perception of one’s susceptibility to the health conditions (Tarkang and Zotor 2015:5 and Turner et al 2004:32). In the current study, it is thought that people who perceived their children to be susceptible to pneumonia would take more likely the pneumonia protective, preventive as well as management base actions to protect their children from childhood pneumonia.
3.4.1.2 Perceived Seriousness/Severity
Perceived seriousness refers to individual’s belief/trust about the severity of a disease which usually depend on medical information or knowledge that may come from beliefs which a person has about the difficulties of a disease (Turner et al 2004:1).
It assumes that an individual can take the proper actions as him/her understoods the magnitude of the disease and its negative consequences (Tarkang and Zotor 2015:5). In the current study, it was learnt that if mothers/caregivers perceive childhood pneumonia as a serious infection that has severe negative consequences and implications on their physical and social lives, they would then adopt actions to prevent and treat the disease. Thus, knowledge and attitude of mothers or caregivers plays a crucial role in the prevention and control of childhood pneumonia
3.4.1.3 Perceived Benefits
It is the indviduals’ feelings or assumptions of the value or usefulness of a new behaviour that assumed to decrease the probability of getting a disease. People proclivity to accept the new behaviours when they believe that will increase the chances of getting healthier or decrease their chances of getting a disease (Turner et al 2004:32). The person needs to believe or accept that taking a certain action will help to tackle a problem from happening. It is this belief that may give a person’s confidence to take the actions because of the expected outcomes (Tarkang and Zotor 2015: 5). For the current study, the perceived benefits are assumed to be beliefs of parents /mothers or care givers about the effective interventions of childhood pneumonia preventing and controlling health actions.
3.4.1.4 Perceived Barriers
The perceived barrier is an individual’s own evaluation of the challenges in the process of accepting a healthier behaviour. It is the most important in which plays a significant role indetermining the behaviour change. In order for a new behaviour to be accepted/adopted, one needs to accept the benefits of the new behaviour outweighs the consequences of continuing the old behaviour (Turner et al 2004:33). Perceived barriers can also be referred to one’s belief which persons realize that they have the power to challenge with different obstackles and that they would be able to take the interventions (Tarkang and Zotor 2015:5).
The current study identified that decreased level of knowledge, attitude and practices among mothers/caregivers can be a challenge and retards the implementation of pneumonia prevention and control strategies in the communities.
According to Tarkang and Zotor (2015:3-4), there are three different elements of HBM those are individual’s perceptions about new behaviour, modifying factors and benefits of taking preventive measures. Each of these are described as follows:
3.4.1.5 Individual’s perceptions
Individual’s perceptions are opinions towards one’s own susceptibility to a disease plus the seriousness with which one views the perceived threat of the illness (Tarkang and Zotor, 2015:3-4). In the current study, knowledge and attitude of mothers or caregivers on the prevention and control of childhood pneumonia were considered as contributing factors of childhood pneumonia.
3.4.1.6 Modifying Factors
Factors like socio-demographic, socio-psychological and structural are among the modifying factors those may affect one’s perceptions and thus they can influence health related behaviours (Tarkang and Zotor, 2015:4). From the current study, socio-demographic factors, like educational and economic status of the parents can affect a family’s perceptions of susceptibility and severity of suffering of their childrens’ ill effects resulting from childhood pneumonia.
3.4.1.7 Benefits of taking the preventive measures
Perceived benefits and practicing variables affect the likelihood of initiating and maintaining action (Tarkang and Zotor, 2015:5). The current study assessed the knowledge and practices by mothers or caregivers towards prevention and control mechanisms like protective, preventive and to evaluate how they are taking care for their children and implementing childhood pneumonia interventions.
3.4.2 Global Action Plan for Prevention and control of Pneumonia Framework
WHO and UNICEF (2009:2&19), have been developed childhood pneumonia preventionand control approach called GAPP that would support the countries in their efforts for effective management of pneumonia. The GAPP framework proposes strategies of interventions that partners can collaborate their efforts. The GAPP was developed to improve awareness of communities towards childhood pneumonia prevention and control, that it is a possible cause of child death and call for scaling up the use of interventions of proven benefit and provide the way of implimentations.
The GAPP framework has been envisioned with the different areas for controlling pneumonia among under-five year’s children and categorized into three major areas namely; protecting the children through a healthy environment, preventing them not to becoming ill with pneumonia and properly treating children who became ill with pneumonia.
In current study, different interventions on protection, prevention and treatment of childhood pneumonia were assessed and analysed. The protective factors including birth weight, breastfeeding, nutrition, indoor air pollution and hand washing practices were assessed. In addition, knowledge and attitude of respondents towards childhood pneumonia prevention and control were addressed. Regarding the preventive factors, vaccination status, HIV/AIDS status of family members, zinc and Vit A supplementation and deworming status were also assessed. Similarly, the study also assessed the treatment related factors that the mothers/caregivers practiced towards childhood pneumonia prevention and control.
Based on the theories and assumptions of both Health Belief Model (HBM) and GAPP framework, the researcher has developed the conceptual framework for the present study which has been used as the guiding principle for the study and came up with the potential findings. This conceptual framework has also been used as the roadmap for the development of awareness and prevention strategies for childhood pneumonia control.
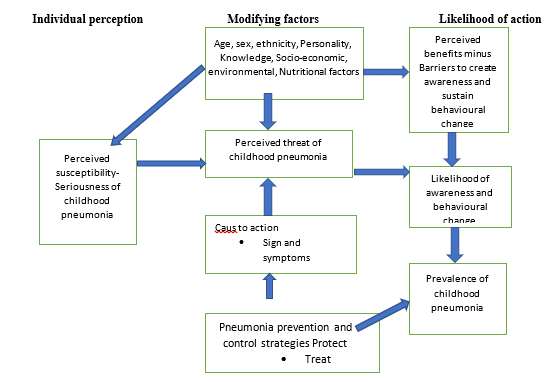
Figure 3. 1: Conceptual framework developed by researcher (adapted and modified from HBM (Turner 2004: 34) and GAPP framework (WHO and UNICEF 2009a: 4).
3.5 CONCLUSSIONS
This chapter presented the framework, theoretical framework and conceptual framework. It also described the HBM and GAPP framework for prevention and control of pneumonia among under five children those are used as the base for newly developed conceptual framework of the current study. Furthermore it was also discusses about the four perceptions of HBM like perceived seriousness, perceived susceptibility, perceived benefits and perceived barriers were discussed in detail. In addition, the three intervention areas of GAPP, namely: protection, prevention and treatment were discussed. The newly developed conceptual framework was also showed in this chapter.
The next chapter will present the methods and materails of the current study.
The chapter presents and discusses about the research design and the methods used to atain the purpose and objectives of the current study. It also describes the type of research design used, study area conducted, population and sample groups selected. Further sample size calculation and sampling methods, method of data collection and analysis as well as ethical considerations and measures taken to ensure validity and reliability were also presented in this chapter.
4.2 RESEARCH DESIGN
According to Polit and Beck (2010:567), a research design is taken as the overall plan for addressing a research objectives for increasing the study’s integrity. Researcher can choose and take the right way to answer a research question considering with different considerations like number of study groups will be included, resources and time of data collection (Gray et al 2017:1054). For the current study, the researcher used a convergent type of mixed method. The use of quantitative and qualitative data as a mixed research method is believed to triangulate the data as well as the findings that will help to create a better understanding of a research problem than using individual approaches (Creswell 2014:32).
In the present study, the descriptive and explorative type of research approaches were applied. A community based cross sectional study design and focus group discussion were employed for the quantitative part and for the qualitative part respectively. This was made so to conduct the study with the objectives of assess childhood pneumonia prevalence and its contributing factors, likewise it was to explore knowledge, attitudes and practices of mothers/caregivers towards of child hood pneumonia prevention and control. Then after to develop awareness and prevention strategies on pneumonia among under five children in Sidama Regional State; in line with the strategy to accelerate the goal of ending preventable pneumonia disease by 2025.
4.2.1 Quantitative Research
Polit and Beck (2010:565), argued that it is the study of phenomena which concede themselves to precise measurement and quantification. It is also described as the systematic study or process that counts or measures formally to answer the research question or objective and usually uses numerical data (Gray2017:1082). In the current study it was used to measure or quantify the prevalence of childhood pneumonia and assocaiated factors numerically. Similary it was used to assess KAP of mothers/care givers towards and its determinants towards pneumonia prevention and control among under five children. The findings also generated with numeric values.
4.2.1.1 Cross-sectional study design
According to Polit and Beck (2013:239), a cross-sectional study design would be used to collect data at one point in time and or multiple times in a short time period. The cross sectional study design is right the approach to describe the status of certain events or phenomena and its relationships at a fixed point of time. In the current study all quantitative data were collected at one point of time or data collection period and which aimed to determine the prevalence of childhood pneumonia and its contributing factors, and also to explore KAP of mothers/caregivers towards childhood pneumonia prevention and control.
4.2.2 Qualitative Research
From the books a qualitative research is defined as, it is an indepth study and rigorous approach used to describe ones’ cultures, life experiences and social processes from the individual perspectives or it is a method of exploring and understanding the meaning of individuals’ or groups’ justifications to a social or human problem (Gray 2017:1081-Creswell 2014:32). In the current study, a qualitative research was basical used to answer objective seven (explore KAP of mothers/caregivers towards childhood pneumonia prevention and control). It was applied to complement quantitative data or findings and to explore the factors related to the life experiences of the communities that may contribute to childhood pneumonia- especially knowledge, attitudes and practices of mothers/caregivers towards childhood pneumonia prevention and control.
4.2.3 Mixed Research method
It is the use of two research designs usually quantitative and qualitative methods together, in order to describe the issues in detail and triagulates the data to create better understanding on the issues (Gray 2017:1070). In the current study quantitative and qualitative approachs (mixed research method) were applied in convergent way of mixed method. Both quantitative and qualitative data were collected concurrently but analysed separately. Finaly the results were merged during interpretation. This helped for better strengthening of data as well as study findings and for vigorous and dependable conclusions. It was used for complementarity, incrementally and enhanced validity. Thus doing so avoids limitations of a single approach and provides an opportunity for testing alternative interpretations of the data. Supported to obtain more complete understanding from two data sets and corroborate results from different methods.
4.3 RESEARCH METHOD
Research is a serious, or systematic assessment or study to re-assure and amend the existing knowledge and effectuate new knowledge. Whereas, research methods are the specific ways that researcher choses to conduct the research, within the sellected design. A research methods could be topic selection, choice of study area, sample size calculation, data collection and analyisis with appropriate statistical tests (Gray 2017:1070 &1085). The current study has used different research methods to achieve the planned goal or proposed objectives and help in the development of the proposed awareness and prevention strategies on childhood pneumonia within the study area. Those methods and approaches are discussed as follows:
4.3.1 Study area/setting
Study area/setting is a place which could be organization, agency or community where a study has planned to conduct or it is the location and conditions in which data collection for the study will take place (Kumar 2011:208 & Polit and Beck 2010:568).
Current study was conducted in five districts and one town administration of Sidama Regional State which has been established newly from SNNPR as of June 2020. They are Dale, Aleta Chuko, Bensa, Bona Zuria and Loka Abaya districts and Aleta Wondo town. The Region found in between 6°14’ & 7°18’ N and 37°92’ & 39°14’ E with the altitude ranging from 1,200 metres to 3,211 metres and is one of densely populated regions in Ethiopia. According to 2019 restructuring, there are 30 rural districts, 6 towns, one city administration with 8 sub-cities. The region has 19 functional governmental hospitals, 135 governmental and 3 non-governmental health centres and 620 health posts (Sidama Zone Health Department 2019:12).
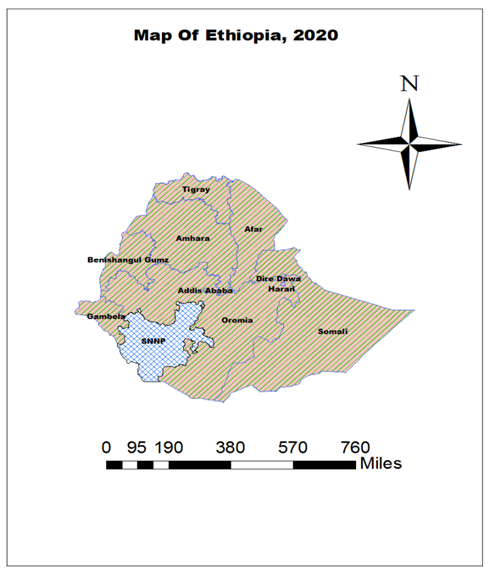
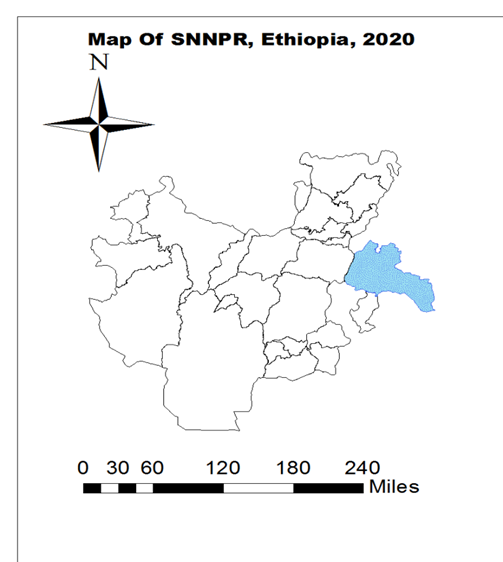
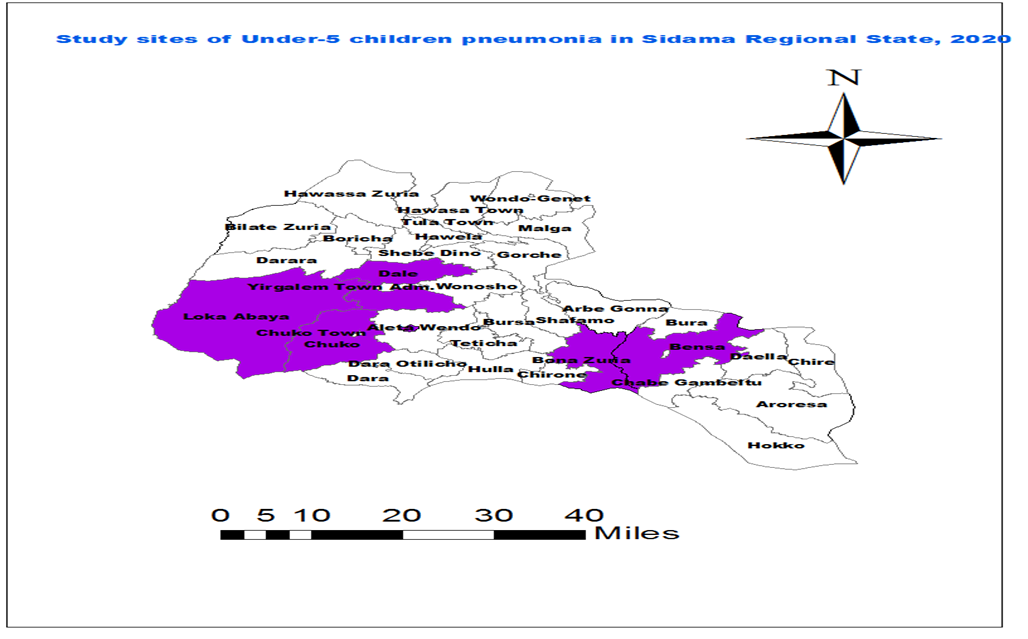
Figure 4. 1: Map of study site, Ethiopia, 2020
4.3.2 Study Population
Study population is the whole aggregation of subjects that a researcher is interested and not restricted to human or respondents can be specified with the reasons that set the study population based on the eligibility criteria (Polit and Beck 2010:306),
Sidama regional state is among the densely populated regions in Ethiopia with having nearly 4.5 million population in 2019. Among these 607,435 are children aged under five years and there are estimated 772,533 women in reproductive age group. Majority of people in the region are rural dwellers and agriculture dependents.
Source population of the current study comprised of all mothers/caregivers with under-five children who living in the six districts of Sidama regional state, namely: Dale, Aleta Chuko, Bensa, Bona Zuria and Loka Abaya districts and Aleta Wondo town in Sidama region, Ethiopia.
4.3.3 Study sample and sampling techniques
Sample is a subset of the accessible group or population that the researcher selects for participation in the study; whereas sampling is the way of taking a portion of the population to represent the entire group. Or it is a way of selecting study participants like groups of people, behaviours or other elements those are appropriate to conduct a study (Polit 2018:243 Gray 2017:1087).
4.3.3.1 Sample size calculation
Sample size is the number of particiapants/respondents to be taken from the universe based sample. A sample size expected to be enough/optimum for the study and needs to fulfil the requirements like efficiency, reliability, representativeness and flexibility (Kothari 2004:56), The sample size was calculated for the quantitative part of current study by considering all necessary estimations of a proportion with specified absolute precision. The prevalence of childhood pneumonia and its contributing factors for the areas covered by the current study site was not known from previous studies. Due to this reason, a 50% prevalence rate was used to calculate the sample size. The sample was calculated by using the formula for estimation of single population proportion.
n=((Z^2 x P (1-P))/d^2 x k
n=((〖1.96〗^2 x 0.5 (0.5)))/〖0.05〗^2 x 2
n=((1.9208))/0.0025
n=768 Respondents
The final sample size was 845 respondents after adding 10% non-response rate.
For the qualitative part of this study, six FGDs were conducted to attain data saturation and 4 FGDs each group included seven (07) mothers while 2 FGDs included 6 mothers with child less than 5 years age purposively selected. The opinions and experiences of respondents were solicited simultaneously and the moderator guided the discussion.
Regarding the Delphi group, 10 expertise based on their previous maternal, neonatal and child health experiences and exposures on the area, who have been working in University, regional health Bureaus, Zonal health department, Hospitals and NGOs were participated. Delphi method is a way of getting informations/judgments from an expert panel about specific issues where experts requested individually in number of rounds, by circulating a summary of the panel’s views between rounds to foster consensus (Polit and Beck 2018:546).
4.3.3.2 Sampling techniques/procedures
The probability sampling approach was applied for the collection of quantitative data from the current study area and purposive or non probability method was used for sampling of FGD participants.
For the quantitative study a multi-stage sampling techniques were used to collect information from the study site. A multi-stage sampling technique is one of the sampling strategies that move on through a set of stages/levels from larger to smaller or higher to lower sampling units (Polit and Beck 2010:560). The researcher has randomly selected a total of 6 districts (5 rural and 1 urban), namely: Bensa, Bona Zuria, Aleta wondo town, Aleta Chuko, Dale and Loka Abaya districts firstly and 21 kebele from these districts. The current study used simple random sampling method through table for random numbers method to select those six districts and 21 kebele accordingly where each element in the population is given an equal and fair chance to be selected.
Cluster sampling method was used to select 845 study samples proportionally from 21 kebele. Each kebele was divided into small villages called “gote” or “limat budin” and randomly selected for data collection. From the selected “gote” or “limat budin” data were collected until the proportional allocated sample size reaches as shown in figure 4.2. According to Kothari (2004:65), cluster sampling can be conveniently taken by grouping the area into smaller non-overlapping areas and then to randomly select some of smaller areas until satuareting the proposed sample size
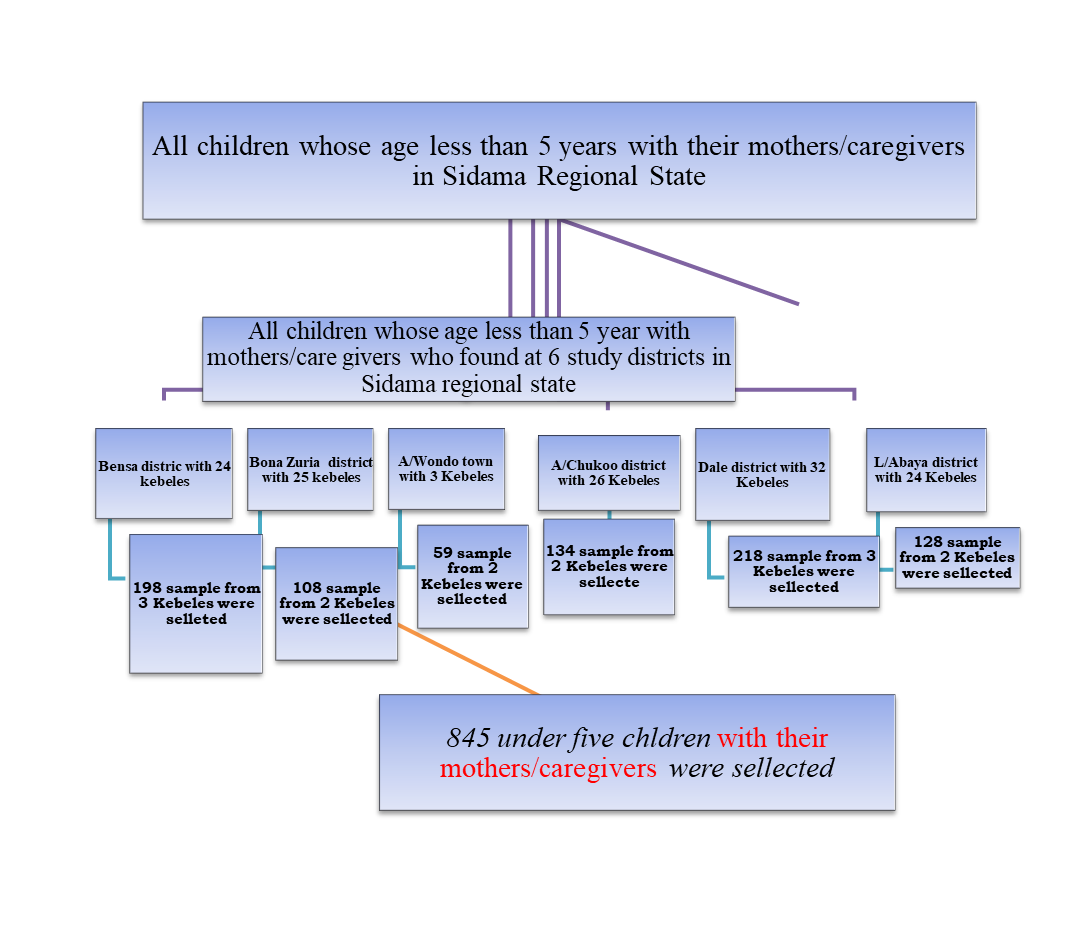
Figure 4. 2: Schematic presentation of how to select sample population for quantitative part of study in Sidama Regional State: 2020
Non-probability or purposive sampling method is the way of sampling by non-random means to select respondents. It is a judgmental way of sampling which involves conscious selection by the researcher of certain respondents to be included in a study (Polit 2018:291; Gray 2017:1081) For the qualitative part of the current study, the purposive or purposeful sampling was used for selection of respondents for collection of data.
The researcher decided on six focus group discussions (FGD) with each FGDs containing seven respondents/discussants (mothers with their child age less than 5 years). The respondents were chosen with the consideration of their past active participation and knowledge on health issues at their village. All six FGDs were selected from three districts namely: Loka Abaya, Dale and Aleta wondo town; hence it was assumed to be representative of the remained three districts as that leaving conditions of communities are more or less similar in different districts. Two FGDs from each districts and one FGD from each kebele were involved in 5 rural districts while 2 FGDs were involved from one kebele at Aleta wondo town. The selection of each discussant from the selected kebele was done with the help of health extension workers who knew households very well and had participated earlier in health issues in their kebele.
4.3.3.3 Eligibility criteria for being a respondent for interview
Polit and Beck (2018:547) defined eligibility criteria as it is the criteria that designated to select the specific target population to be included in a study. Households were selected through cluster base sampling and respondents who were availed at home durng data collection and conseted were made to be included in the current study.
4.3.3.3.1 Inclusion criteria
The study inclusion criteria are measurements identified by the researcher which would be presented for the respondents to be included in the sample (Gray 2017:1063). In the current study the following were considered as inclusion criterias:
4.3.3.3.2 Exclusion criteria
Exclusion sampling criteria are descriptive criteria that eliminate some respondents from the inclusion of study sample for the reason of eliminating sample characteristics that may introduce error (Gray 2017:1057). The following were the exclusion criteria agreed in the current study:-
Variable is abstract ideas that have been made measurable. In quantitative study, variables are studied in order to investigate incidence, the assocaitions that may exist among them and or cause-and-effect relationships (Gray 2017:1096). Thus, study variables can be defined as the components of the indicators which can be measured (Walliman 2011:66). In the current study different dependent and independent variables were considered by reviewing different literatures including Ethiopian Demography and Health Survey.
4.3.3.4.1 Dependent Variables
They are called the outcome variables or the variables hypothesized to depend on which can be caused by another variable. It is a response, behaviour or outcome that is predicted and measured in research (Polit and Beck2018:546, Gray 2017:1053). In our current study, dependent variables were listed as follows: -
4.3.3.4.2 Independent Variables
According to Polit and Beck (2018:552), an independent variable is the variable which is considered to cause an effect or influence the dependent variable.It is the variable or variables that may predict the occurrence of the dependent variable (Gray 2017:1063).
Independent variables considered in current study were categorized into socio-demographic and economic, environmental, behavioural and health status, nutritional and immunization related variables.
Socio-demographic and economic variables included parental education and occupation, religion, maternal age, family size, economic status, ethnicity group, sex of child and age, marital status and residence of the respondents.
Environmental variables like type of household fuel, tobacco smoking, latrine availability, housing conditions, presence or absence of cattle, availability of separate kitchen, presence or absence of ventilation and waste management were addressed.
Nutrition and immunization related variables included feeding practice, immunization status of child, Vit A supplementation and deworming status, duration of breastfeeding, and nutritional status of child were included.
Health status variables like family history of acute respiratory infections, history of HIV/AIDS and disease history of child were assessed.
4.3.4 Data collection process and tool
4.3.4.1 Data collection approach
Data collection is a way of precise and systematic collecting of relevant information to the study purpose and objectives (Gray 2017:1052). For the quantitative part of current study data were collected from home to home survey. Individual interview and observational approaches were applied to collect the relevant informations to the specific objectives of the study. An interview is a way of data collection in which data collector asks questions about respondent, either face-to-face, by telephone, or via the Internet. However observational methods can be used to collect information by observing the conditions of individuals (Polit and Beck 2018:553).
For the qualitative part of the study data were collected via face to face participation of FGD participants. The discussions were conducted at selected kebele.
The Delphi survey was conducted through mail communication to collect inputs for the development of awareness and prevention startegies.
4.3.4.2 Research data collection tool
The structured interview schedule were used to collect the quantitative data of current study. An interview schedule was taken as an arranged instrument which specified the wording of all questions used to ask respondents in a structured self-report studies (Polit and Beck 2018:553). The structured interview schedule of the current study was developed in English language by reviewing the standard survey questions including DHS and previous similar studies. It was translated into Sidaamu Afoo- the local language spoken in the study area. Then by checking the validity of the questionnaire, the interview schedule was translated back into English to avoid possible difference in the meaning.
The questions of the structured interview schedule were grouped into six parts namely: socio-demographic and economic information, Childs’ characteristics, information on environmental factors, nutritional related factors, information on immunization status of the child, and KAP of respondents. There are total of 110 items or questions includeding the questionnaries for wealth index assessement. The major contents included in the current interview schedule were:-
Part one: Socio-economic and demographic information (26 items):
Household socio-economic and demographic data, respondents’ socio-demographic, children’s demographic data and wealth index.
Part two: Child’s characteristics (13 items)
Age, sex, place of delivery, birth interval and order and disease status of child.
Part three: Information on environmental factors (24 items)
Latrine availability, waste management, housing condition, fuel used and charcoal utilization.
Part Four: Nutritional related factors (16 items)
Anthropometric measurements, breastfeeding, additional food initiation, Vit A supplementation and deworming.
Part Five: Information on Immunization status of the child (06 items)
Immunization status, PVC 10 vaccine, measles vaccine.
Part Six: KAP of respondents (25 items)
Knowledge, attitude and practice;
For qualitative part of the current study, data were collected by using FGD guide. FGD guide includes the procedures and guiding questions that could support to explore the KAP of mothers/caregivers towards childhood pneumonia prevention and control. The guiding questionnaire was also translated into local language (Sidaamu Afoo) and then back to English by independent translators to optimize the accuracy of the translation.
The FGD guiding questionnaires included the following basic areas:-
Introduction part or aim of FGD, group consent for the participation, ground rule, knowledge about childhood pneumonia and its causes, common symptoms, prevention as well as treatment methods and their practices towards prevention and control of childhood pneumonia and challenges related with it. The questions were open-ended and non-leading. As the discussion progressed, some of the questions were modified to effectively attain the purpose of the interview.
The researcher considered the above employed methods of data collection based on the factors like nature, scope and object of enquiry; availability of funds, time and precision required (Kothari 2004:112):
4.3.4.3 Training provided for data collectors and supervisors
Researcher developed a training manual which includes the introduction part, aim of training, importance of the manual, short definition of research, sampling, data collection methods and tools, research ethics and data quality issues. The manual was prepared in English language. Data collectors and site supervisors were trained by the researcher for two days on the approach and method of data collection, at the training hall of Yirgalem General Hospital. The detailed explanations were provided about the purpose and objectives of the study, sampling method, way of interviewing, content of the data collection tool, data quality and ethical issues. Furthermore they oriented about research methodology and data collection procedures.
Data colectors and supervisors had been familiarised with each questions of the interview schedule especially on the translated one through reading and discussing. The clarifications of each questions regard to its purpose were made clear. An orientation was given on how to fill out the questions of the structure of the interview schedule, both open and closed-ended questions, the skip patterns, observation questions, questions with one and multiple responses, how to measure weight, height and count pulse rate of the index children. Morely emphasis was also given them about how to establish mutual trust with respondents before asking questions.
Regarding the qualitative data collection, orientation was given for the FGD assistances and health extension workers to equip them with the basic aim of research and selecting participants as well as way of guiding the discussion.
According Polit and Beck (2018:561), pilot study can be taken as a small-scale study conducted in the way of preparing for a main study, usually to assess feasibility data collection tool. Regarding the quantitative section of current study, 10% of actual sample size or about 85 questionnaires were piloted at Tula sub city where outside the study districts before actual data collection. The aim of piloting was to test the data collection tool as well as equip and familarize the data collectors and supervisors with the data collection instruments. Based on the pilot study findings, some changes those related with culture sensitivity, language error and might missed the expected meaning were corrected and modified with more relavant and understandable way of writing. However the qualitative instrument was not piloted rather edited and re-checked by researcher.
4.3.4.5 Data collection process
Quantitative data collection
Twelve data collectors and three site supervisors attained the collection of quantitative data. Six of the data collectors had a bachelor’s degree, six held diploma in nurses and all three site supervisors had a master of public health degree. They were purposeful selected with the consideration of earlier experience in data collection, familiarity with local language and who took IMNCI training.
There were six teams established for those six districts of data collection area, each team with two data collectors in Sidama regional state, to collect data from the households. One site supervisor was assigned for two teams to manage and support them. All data collectors and site supervisors are native for the Sidaamu Afoo language and had earlier experience in research data collection. Furthermore they were also trained on basic IMNCI pneumonia management guideline. Each team was equipped with the interview schedules, weighing scales, MUACs and tape meters. Data were collected from home to home in the selected cluster of the study area, by interviewing mothers/caregivers using interview schedules. The pilot study participants were not included in the main study. During thedata collection measuring the weight, MUAC and height of the index child was carried by data collectors. The immunization status of the child was assessed by referring their immunization cards. Where there was no either of them (mother or caregiver) data collectors made return visits to the households for at least three times for the interview, and enforced to visist and collect data from next household. Respondents’ confidentiality was maintained; and kept records/data confined to them confidential. In addition, the reliability of the weighing scales and measuring tapes checked for accuracy and calibrated after every measurement. Each measurement was done twice, and the average was taken.
Site research data collection supervisors were charged with the supervising of the process of data collection and resolve the problems encountered. They were also responsible to organise the logistics needed for data collection and orient data collectors about the field work in the districts and checked the filled instruments for completeness and correctness. Furthermore they have checked the daily filled interview schedules and took actions if there were inconsistent or incompleteness.
They guided data collectors to re-check those incomplete schedules and made to re-interview the households based on the type of problems identified and reported to the researcher.
The researcher was able to coordinate the whole process of data collection and checking the sample for data quality. Where the filled interview schedules were found to be inconsistent, incomplete or having missing information, the supervisors and data collectors were communicated to re-checked and filled data or made to re-interview the households based on the type of problems identified.
Qualitative data collection
Six FGDs were conducted at three study districts, two FGDs per district. The researcher and assistants together with health extension workers facilitated the discussion according to the FGD interview guide. The discussants had chosen the safe place and confortable way of sitting by themselves. Most of them chose a semi-circular sitting arrangement and used compound of health posts’ where there were shades or sitting facilities for the discussion. FGDs were audiotaped with discussants permission and the researcher and assistants took notes as well. In each FGDs discussants were coded with number; like FGD1 participant 1, 2, 3, 4, 5, 6 and 7 for analysis, while conducting discussion with field note book, they coded and registered with their age. Based on their interest and saturation of needed data 1 hour to 1:30 hours were taken to finalize the discussion within each FGDs.
To ensure the discussants safety from covid-19, researcher provided a facemask for all discussants and ensured social distancing among them while sitting. Discussants also utilized accordingly to keep them selves from Covid-19.
Delphi data collection
In the current study, 10 Delphi panellists were included, who are child and maternal health experts and other relevants from university, RHB, Health departments, NGOs and hospitals. The aim of Delphi method data collection was to gather inputs from experts’ and professionals. Data were collected through electronic mail. Firstly, experts were identified, and telephonic interview was done to introduce the researcher and the purpose of the call. Secondly, the study aim was explained to the experts and consent from each individual was obtained. The envisaged framework was then shared to the experts for their input and had one to two weeks to respond with their comments and suggestions through electronic mail.
The Delphi data validating tool was prepared by researcher which contained 08 (eight) Issues to be considered while panellists have commenting the developed awareness and prevention strategies (Annex I).
4.3.5 Ethical considerations
According to Polit and Beck (2018:548), ethics is considered as a system of moral values which is dealt with the degree to which research/study procedures has followed an ethical, legal as well as social obligations to the study respondents. In the journey of study, the application of ethics begins with properly identifying research topic and continues through publication of the study findings (Gray et al 2017:265). This sub-topic presents the principles, permissions needed and granted by relevant bodies of the study.
4.3.5.1 Protecting the Rights of Institutions
Institutional review is a process of examining the design and methods of a proposed study for ethical considerations, and also for overseeing studies in progress. Institutional review is undertaken by an independent committee of peers at an institution to identify the level to which the proposed study protects the rights of respondents. The peers’ reviews committee of research are responsible to ensure that the researcher is conducting the research in an ethically manner (Gray 2017: 1064). The final research proposal of the current study was submitted and approved by Research Ethics Committee, Department of Health Studies at UNISA (Annex A). The institutional permissions were obatained from the former Regional Health Bureau of SNNPR and Sidama Zone Health Department to carry out the research (Annex B & C).
4.3.5.2 Protecting the rights of respondents
The privacy code for each sample were used during data collection rather than taking name of individuals. Recruitment of study respondents and interview were done in privately, with only the data collectors, supervisors as well as principal researcher and the potential respondents. The respondents were clearly informed that the collected information or data would be disseminated via seminars, conferences or articles in such a way that no one could identify who was interviewed and it would be only in group or percentage form. Both paper base and audiotaped collected data has been locked at the office of the researcher and the key has only been with him so that no third party can access to ensure the confidentiality. Computer base record has been secured by personal password and the computer is used by the researcher only.
The right to protection from exposure: mean not to exposing respondents to conditions or situations for which they have not been informed well and ready. Data collectors and supervisors had introduced themselves to the study respondents and the fact that their role was only data collection. Respondents were informed about the objectives and scope of the study before the interview has been started. (Annex D & G).
The right to freedom from harm and discomfort: Beneficence is one the basic ethical principle which seeks to maximize advantage for study respondents and minimize harm (Polit and Beck 2010:548). Data were collected at the household level and had no known risks which would expose respondents to harm. However there was low risk considered hence the study included direct human participant mean that under five age children and their anthropometric measurements like height, weight and physical examinations (checking bilateral pitting edema, pulse rate count). Parental consent was obtained and sufficient counselling and care were given to minimize the discomfort which mothers/caregivers may felt due physical examinations done for child. To minimise any discomforts related with mis-understanding during interview; the questionnaire were translated to Sidaamu Afoo local language, training was given for data collectors on interviewing skills and way to establish mutual trust with respondents. Furthermore data colectors advised to take only a reasonable time to complete the interview schedule (Annex F & H). Benefits from current study include improved community awareness about the burden of childhood pneumonia and its risk factors and further development of awareness and prevention strategies to prevent and control childhood pneumonia.
Justice
According to Grove et al. (2017:1066), justice is one of ethical principles that states human respondents should be treated fairly, as groups and as individuals. The justice for the current study has been secured by randomly selecting the clusters for study respondents’ enrolment with an equal chance to be included in the study. Moreover the appropriate scientific research methodology were followed in each steps.
4.3.5.3 Scientific integrity
The current study contributed to the improved body of knowledge and study regarding childhood pneumonia and associated factors for its prevention and control through honest finalization, result presentation and publication. The scientific integrity of the study was maintained trough the protecting the intellectuals’ property of the author’s publications that were consulted in the current study by giving proper recognition and citation in the list of references. The reported data/result was collected, analysed and interpreted based on appropriate scientific procedures and evidence in an ethical manner.
4.3.6 Processing and analysis of data
Collected data would be processed that editing, coding, classification and tabulation should done under data processing making them amenable to analysis. The term analysis used to refer the computation of finate measures along with searching for patterns of relationship that exist among data-groups those are subject to statistical tests of significance to determine what validity data can be said to indicate any conclusions (Kothari 2004:122).
4.3.6.1 Data processing
A. Processing the quantitative data
The collected raw data supposed to be edited for the detection of errors and omissions and correct them when possible. Data edition helps to ensure the accuracy and consistent of gathered facts (Kothari 2004:122-23). In the current study editing was carriedout at field level by supervisors and at central level by principal researcher to correct the evident errors like an entry in the wrong place were corrected. For instance entry recorded in year when it should have been recorded in months for the age of index child were corrected and the like also done accordingly.
According to Kothari (2004:123), coding can be done by giving numerals or other symbols to answers that responses can be limited into number of categories or classes. All the necessary coding was done prior to data analysis in the current study. Data were arranged into similar categories or groups based on their common characteristics. For instance, study variables such as age of respondent, income and age of child were classified according to their common characteristics.
B. Processing Qualitative part of data
According to Ranjit and Kumar (2011:248), findings from the qualitative data can be reported through developing a narrative to describe a situations and identifying the main themes that emerge from the field notes. In the current study data from field note and recorded audio were analysed manual with the support of Atlas ti soft ware. The narrative reported prepared, voice transcription and verbatim has done, three themes and six sub-themes were identified.
4.3.6.2 Data analysis
The analysis is an interpretation of data that include comparison of different outcomes of the various interventions upon the several groups to make a decision as to the achievement of the research goals (Singh 2006:150). For the current study data analysis were done as the following ways:-
4.3.6.2.1 Analysis of quantitative part
Before starting data entry, the questionnaires those filled by data collectors were reviewed for completeness and consistency of quantitative data. The missed values were verified against the sources accordingly. After cleaning, the interview schedules were coded numerically with in each districts as well as kebele. Then double data entry was done by using Epi data version 4.2.2 software to minimize the missed values and exported to SPSS version 25 software for analysis. The statisticians and senior researchers were consulted for the proper applications of both Epi data and SPSS software programs as per their experiences and earlier exposures. After exporting the quantitative data, the missed values were checked through each study variables by running them with frequency and rearranging with ascending order. The missed values were rechecked and addressed from hard copy data and cleaned as per its appropriateness.
The analysis were done by using SPSS version 25 software programme. Descriptive, bivariate and multivariate statistics were carriedout for quantitative data.
Descriptive statistics were used to present information using frequencies, tables, graphs, mean and standard deviations.
Bivariate and multivariate analysis were conducted to determine the risk factors of pneumonia among children aged under-five. Bivariate analysis were employed by using Chi-square tests or Fisher's exact tests. However multivariate analyses were carriedout through using binary logistic regression with backward stepwise regression technique in order to identify the childhood pneumonia contributing factors independently, while controlling for confounders.
Independent variables those with a p-value less than 0.25 in the bivariate analysis were checked for multivariable analysis. The crude odds ratio (COR) and adjusted odds ratio with 95% confidence interval (CI), regression coefficient and p-value of the variables were calculated in the logistic regression analysis. Through the analysis, the two-sided tests were applied and a p-value less than or equal to 0.05 was considered as statistically significant.
4.3.6.2.2 Analysis of qualitative part
Qualitative data were analysed manually supported with Atlas ti software. Data were analysed by arranging a thematic content and framework analysis. The thematic content analysis was used in exploring or describing the way of awareness creation and prevention of childhood pneumonia.
Verbatim was done with caution. Firstly the audio taped data were listened careful to transcribe. The thematic content analysis was done secondly with the identification of pertinent information. Then significance of the information categorized or coded from the transcript based on the objectives of the study. The frequency or degree of uniformity of ideas that discussants stated were helped to form code. Those codes that can come together were merged to form a new code. Then final mutuality exclusive codes that could not be reduced to any form were taken as final themes in the current study.
4.3.6.2.3 Analysis of Delphi method data
The Delphi data were analysed based on the feedbacks collected from the individual Delphi panelists via email. The common feedbacks from Delphi panels included editing for typographic errors, additional inputs, questions and comments on the content highlighted in track changes. Researcher then analysed and corrected the comments by incorporating the important inputs and reverted it back to the Delphi Panels for final checking and editing of the developed strategies. Researcher gave additional justification to Delphi panellists when needed.
4.3.7 Validity, Reliability and Trustworthiness
4.3.7.1 Validity
The degree of measurements by possible instruments to what it is supposed to measure is called validity. Polit and Beck (2010:377), put that content validity, face validity and construct are major types of validities.
Face validity focuses what the instrument looks as though it is measuring the appropriate construct. Who will be completing the instrument or it is a subjective assessment, usually by an expert that verifies a measurement instrument appears to measure the content it is purported to measure(Grove et al 2017:1058; Polit and Beck 2010:377). For the current study, questionnaires were developed by the researcher based on modified standard survey questions from WHO, EDHS and previous similar researches. Moreover, comments and suggestions from statisticians and epidemiologists those thought as important were incorporated to improve the validity of the instrument.
Ilk type
Content validity used to assure that the degree of all an appropriate items has been included in an instrument for the construct being measured. It concerns about the adequacy of domained to be covered and it also examines the levels that the measurement covers/addresses relevant elements to the construct being measured (Grove et al 2017:1050 & Polit and Beck 2013:377-78). To address the content validity of the current study, detailed literature was conducted and conceptual framework was done before developing data collection tool. According to the published evidences of related literatures, the data collection tool was developed which contained the common elements those are relevant to the study objectives and conceptual framework. Furthermore the developed instruments were reviewed and checked by supervisors.
4.3.7.2 Reliability of the research instrument
Reliability can be considerd as the consistency of measuremnets that instrument measures the attribute or concerns a measure’s accuracy. Quantitative researchers better to consider the three aspects of the reliability interests like stability, internal consistency and equivalence (Polit and Beck 2013:373). Data collectors as well as supervisors were trained on way of data collection and consistensive use of tool, which was to assure the reliability of the current study. The data collection tool was piloted and the necessary refinement was done accordingly before data collection. The questionnaires were translated to local language as both data collectors and supervisors were local language speakers. The similar questions were used for all respondents and the information was clearly given to them. Field supervisors tried to verify the reliability of sample questions respondents during data collection. The investigator also has done close monitoring and daily follow-up through data collection process and has checked the filled data collection tools for completeness and consistency.
The data entry clerk entered the sample data into Epi Data version 4.2.2 software. Another ten randomly selected questionnaires were entered into Epi Data version 4.2.2 software and checked for consistency. Its completeness was also re-checked during analysis through SPSS software.
4.3.7.3 Trustworthiness
According to Polit and Beck (2013:570), trustworthiness can be defined as the level of confidence that investigators have developed in their data qualitative, through credibility, transferability, dependability, conformability, and authenticity criteria. In the current study the general trustworthiness has been ensured as follows and the following general trustworthiness aspects have been assured in this study.
4.3.7.3.1 Credibility
The confidence of the data truthness and proper interpretations of them refers as credibility. Qualitative investigators supposed to develop confidence in the truth of the findings from each respondents and syntax in their research (Polit and Beck 2013:492). Credibility of the current study were ensured by giving enough time during data collection from FGD discussants to establishing amity with them. The investigator’s earlier exposure/experience as a public health care practitioner and facilitator with childhood pneumonia prevention and control services in Ethiopia has been of a paramount assistance in conceptualising the study. The discussion was conducted in local language and which helped the respondents to understand and give their experience freely. In addition, the principal investigator and assistances have used FGD guide to probe respondents. The field notes and audiotapes were used to capture the data and helps to enable the principal investigator to understand in-depth. The investigator also tried ensure the authenticity of data through member cross checking mechanism as that transcripts were given to senior researcher and expertise.
4.3.7.3.2 Dependability
Dependability is a criterion to be used for checking the integrity in qualitative studies, through the stability of data over situations as well as analogous to reliability in quantitative research (Polit and Beck 2010:568). In the current study the supervisors and copy editors were involved as hearers of the reviewed documents produced during the study. Supervisors and independent qualitative researcher were participated to review the transcripts for analysis.
4.3.7.3.3 Confirm-ability
Confirm-ability is objectivity, which is the potential for congruence between two or more independent people about the data accuracy, relevance, or meaning (Polit and Beck 2013:492). The audit trial was used to ensure the confirm-ability of current study. The principal Investigator used field notes and audio tape recorder in order to keep the original voice of the discussants and properly interview transcripts from individuals. The independent qualitative researcher and supervisors were involved for confirm-ability cehck. Researcher tried to focus on discovering omissions of comments and to verify placement of phrases into themes with the hlp of member check.
4.3.7.3.4 Transferability
According to Polit and Beck (2013:492), transferability is can be taken as a similarity of the generazebility or the extent to which qualitative findings can be transferred to or have an applicability in other settings. In current study transferability has been assured by its methodology that researcher used a mixed type of study which can be applicable in other areas too. Further the study provided adequate information in each study processes like study purpose, objectives, sampling strategies, data collection procedures and data analysis. The researcher also used member check.
4.3.7.3.5 Authenticity
According to Polit and Beck (2013:493), authenticity is the level to which investigator symmetry and faithfully show a range of different realities. It can be emerged in a report when it shows the feeling tone of respondents’ lives as they are lived. The FGDs of the current study were guided by local language and participants can reflect their opinion clearly. The transcription was also done by the most experienced individuals who knew the both languages very well, which helped to capture the multiple perspectives of participants and foster change across them to ensure the authenticity of the study. Additionally the investigator cross checked the transcribed data with original audio and field notes and corrected any differences found.
4.4 CONCLUSSION
This chapter presented the research design and methods used in current study which was -the mixed research approach. It also discussed the study setting, population, sample and sampling procedures, and inclusion and exclusion criteria, determination of sample size. Besides, study variables, data collection tool and process were also described accordingly. The chapter also presented the ethical considerations followed under this study, method of data processing and analysis, mechanism of validity and reliability assurance and trustworthiness of the study.
The the next chapter will present the analysis and research findidngs of the study.
This chapter presents the result of the study that alines with the study objectives. The study findings include the prevalence of pneumonia among under-five years children and its different associated factors like; socio-demographic and economic, behavioural and health related, nutritional and immunization related and environmental risk factors in Sidama regional state of Ethiopia. The study result also includes the level of knowledge, attitude and practice of mothers/caregivers of under-five children towards childhood pneumonia prevention and control and its associated factors in the current study area. Furthermore the qualitative findings also presented in this chapter.
5.2 DATA COLLECTION, MANAGEMENT AND ANALYSIS
Current study includes both quantitative and qualitative data. Quantitative data were collected from 15th March to 20th May 2020 from 13 kebele of six randomly selected study districts in newly established Sidama regional state of Ethiopia.
For the qualitative part of study six (06) FGDs with total of 40 women participants who had under-5 children; meaning that two FGDs with six participants and four FGDs with seven participants were involved and data were collected based on the prepared discussion guideline.
It is true that quality issues of data can affect the analysis and interpretation of research findings. Different quality measures were taken in each steps of quantitative and qualitative data process to ensure its quality.
5.3 RESEARCH RESULTS
5.3.1 Response rate and residence of respondents
Overall 845 study respondents randomly selected from households for the current study, while 843 were involved in the interview and giving a response rate of 99.8%.
Out of the 843 respondents, 217(25.7%) were from Dale, Loka Abaya 128(15.2%), Aleta Wondo town 59(7%), Bona Zuria 108(12.8%), Bensa 197(23.4%) and Aleta Chuko districts 134(15.8%) respectively. Regarding their kebele; 73(8.7%) from Wara, Soyama 73(8.7%), Gane 71(8.4%), Arada Gale 56(6.6%), Chalbessa 72(8.5%), Mesalemia 59(7.0%), Olonso Hore 56(6.6%), Bona Kike 52(6.2%), Chalba 62(7.4%), Hatessa 66(7.8%), Shanta Wene 69(8.2%), Chuko Lamala 64(7.6%) and Rufo Wacho 70(8.3%). Thus majority of respondents 784 (93.0%) were rural dwellers whereas 59 (7.0%) were urban habitats.
5.3.2 Socio-demographic and economic characteristics of respondents
The study result revealed that 707(83.9%) of the respondents were mothers of the children and 136(16.1%) were care givers. Majority of the respondents 801(95.0%) were formally married and living together, 19(2.3%) were single and 23(2.7%) widowed. Regarding the sex of respondents 738(87.5%) were female and 105(12.5%) male.
Majority of the respondents 747(88.6%) were Protestants followed by Apostolic 57(6.8%), Orthodox 32(3.8%) and Muslim 7(0.8%) respectively. Out of 843 respondents 803(95.3%) belongs to Sidama ethnicity, 26(3.1%) Amhara and the others namely Wolaita, Oromo and Silte constitutes the rest 14(1.6%).
The analysis showed that the literacy rate was 657(77.9%) while 186(22.1%) did not have formal education. Most of the participants 522(61.9%) had elementary school level (grade 1-8) and 41(4.9%) had tertiary level of education or graduate certificate and above. Regarding respondents’ occupation, 605(71.8%) responded that they were housewife followed by merchants 92(10.9%), government employees 74(8.8%), farmers 61(7.2%) and 11(1.2%) were daily laborers respectively.
The analysis showed that the mean family size of study respondents at the study area were 5.46 (standard deviation ±1.87). The household family size ranged from three to twelve persons. The result of recoded categorical data of family size showed that 456(54.1%) households had small family size, 251(29.8%) of them had medium family size and 136(16.1%) had large family size. Half of mothers from the surveyed households had only one or two children, followed by 179(21.2%) of mothers who had three, 132(15.7%) had five and above and 120 (14.2%) had four children respectively.
Findings of analysis showed that the age of respondents reached from 16 to 65 years with a mean age of 29.6 years (standard deviation ±7.09). The most frequent age in the current study was 30 years while the median age was 29. The majority of respondents 505 (59.9%) were 25-35 years age followed by 16-24 years 193(22.9%) and 145(17.2%) equal or more than 36 years.
Table 5. 1: Socio-demographic and economic characteristics of respondents in Sidama Regional State: 2020 (N=843)
| Characteristics | Frequency
| Percentage | |
| Relation of respondent to child (N=843) | Mother | 707 | 83.9 |
| Care giver* (father, sister, brother of child or others) | 136 | 16.1 | |
| Total | 843 | 100 | |
| Marital status of respondents (N=843) | Single | 19 | 2.3 |
| Married | 801 | 95.0 | |
| Widowed | 23 | 2.7 | |
| Total | 843 | 100 | |
| Sex of respondent (N=843) | Male | 105 | 12.5 |
| Female | 738 | 87.5 | |
| Total | 843 | 100 | |
| Religion of respondents (N=843) | Protestant | 747 | 88.6 |
| Apostolic | 57 | 6.8 | |
| Orthodox | 32 | 3.8 | |
| Muslim | 7 | 0.8 | |
| Total | 843 | 100 | |
| Ethnicity of respondents (N=843) | Sidama | 803 | 95.3 |
| Amhara | 26 | 3.1 | |
| Others** (oromo, silte and wolaita) | 14 | 1.6 | |
| Total | 843 | 100 | |
| Occupation of respondents (N=843) | Housewife | 605 | 71.8 |
| Merchant | 92 | 10.9 | |
| Government employer | 74 | 8.8 | |
| Farmer | 61 | 7.2 | |
| Daily labourer | 11 | 1.3 | |
| Total | 843 | 100 | |
Educational level of respondents (N=843) | *No formal education/Illiterate | 186 | 22.1 |
| Elementary school (1-8 grade) | 522 | 61.9 | |
| Secondary school (9-12 grade) | 94 | 11.2 | |
| Above secondary school (certificate and above) | 41 | 4.9 | |
| Total | 843 | 100 | |
| Age of respondents (N=843) | 16-24 years | 193 | 22.9 |
| 25-35 years | 505 | 59.9 | |
| >=36 years | 145 | 17.2 | |
| Total | 843 | 100 | |
| Family size of households (N=843) | Small family size (<=5 members) | 456 | 54.1 |
| Medium family size (6-7 members) | 251 | 29.8 | |
| Large family size (>=8 members) | 136 | 16.1 | |
| Total | 843 | 100 | |
| Parity of mothers (N=843) | One | 197 | 23.4 |
| Two | 215 | 25.5 | |
| Three | 179 | 21.2 | |
| Four | 120 | 14.2 | |
| Five and above | 132 | 15.7 | |
| Total | 843 | 100 | |
*Care givers refers fathers, sisters, brothers of child or others who were participated under the study where the mother was absent.
*Formal education= respondents did not attend any education and who cannot read and write also
5.3.2.1 Wealth index of households
Total of 13 questions were used to assess and evaluate the information of wealth index of households in the current study area. Assets of each households’ that information collected were given a weight or factor score made over principal components analysis. The resulting asset scores were uniform in relation to a standard normal distribution with a mean value of zero and a value of standard deviation one. These standardized scores were also used to generate the break points that define wealth quintiles of population which remained presented in five groups with the similar number of individuals in each group as; poorest (lowest), poor (second), middle, rich (fourth), and richest (highest).
Findings of the current study revealed that 156(18.5%) of households were in the poorest/lowest/ and 177(21%) in poor/second/ categories while 173(20.5%) in middle level, whereas 168(19.9%) and 169(20.1%) of them belonged to the rich/fourth/ and richest/highest/ categories respectively. (See Figure 5.1).

Figure 5. 1: Wealth index of households in Sidama Regional State, Ethiopia: 2020 (N=843)
5.3.3 Socio-demographic characteristics of surveyed child
The current study analysis revealed that half of the children 422(50.1%) were male and 421(49.9%) were female children. Majority of surveyed children 626(74.3%) were delivered at health facility and the rest 217(25.7%) were at home. In addition 664(78.8%) of sample children had two years and above birth interval with their older child and the rest 179(21.2%) were delivered with in less than two years’ interval.
The study result showed that age range of children involved in the study were between 1-59 months. The average age of children was 28.9 months (standard deviation ±15.8).
Furthermore, half of the children 429(50.9%) were between the age group of 13-36 months followed by 37-59 months 239(28.4%), 7-12 months 122(14.5%) and 53(6.3%) were less than or equal to6 months (see table 5.2)
Table 5. 2: Socio-demographic characteristics of surveyed children in Sidama regional state: 2020 (N=843)
| Characteristics | Frequency | Percentage | |
| Sex of child (N=843) | Male | 422 | 50.1 |
| Female | 421 | 49.9 | |
| Total | 843 | 100 | |
| Age of child (N=843) | <=6months | 53 | 6.3 |
| 7-12 months | 122 | 14.5 | |
| 13-36 months | 429 | 50.9 | |
| 37-59 months | 239 | 28.4 | |
| Total | 843 | 100 | |
| Where was the surveyed child born (N=843) | Health facility | 626 | 74.3 |
| Home | 217 | 25.7 | |
| Total | 843 | 100 | |
| What is the birth order of sample child (N=843) | 1st | 196 | 23.3 |
| 2nd | 214 | 25.4 | |
| 3rd | 179 | 21.2 | |
| 4th and above | 254 | 30.1 | |
| Total | 843 | 100 | |
| What was the birth interval of surveyed child within its older child(N=843) | < 2> | 179 | 21.2 |
| >= Years | 664 | 78.8 | |
| Total | 843 | 100 |
The availability of latrine and solid waste management analysis revealed that 740(87.8%) of households had latrine. Of those households with latrine, majority 628(84.9%) had simple pit latrine and 112(15.1%) ventilated improved latrine (VIP). Regarding solid waste management, 525(62.2%) of respondents had their households managed solid waste backyard simple system followed with 197(23.4%) blow a fuse and 121 (14.4%) burying system (see table 5.3).
Table 5. 3: Availability of latrine and solid waste management in Sidama Regional State, Ethiopia: 2020 (N=843)
| Household characteristics | Frequency | Percentage | |
Presence of HH latrine (N=843) | Yes | 740 | 87.8 |
| No | 103 | 12.2 | |
| Total | 843 | 100 | |
Type of latrine utilized by HHs (N=740) | Simple pit latrine | 628 | 84.9 |
| VIP | 112 | 15.1 | |
| Total | 843 | 100 | |
Ways of solid waste management at HH level (N=843) | Backyard simple | 525 | 62.2 |
| Blow a fuse | 197 | 23.4 | |
| Bury | 197 | 14.4 | |
| Total | 843 | 100 | |
5.3.4.2 Housing characteristics of the respondents’
Housing conditions were also assessed and half of the houses were roofed with corrugated iron 430(51%) followed with 404(47.9%) roofed with grass and 9(1.1%) were roofed with bamboo. Regarding floor materials 458(54.3%) of houses were with mud and 338(40.1%) and 47(5.6%) floored with cement and wood respectively.
Further analysis revealed that majority of houses from the study area, that means 529(62.8%) had windows for the ventilation purposes whereas 314(37.2%) did not. Three hundred and eighty-four (45.6%) of houses had 2 rooms and 236(28%) had three rooms. In addition, 181(21.5%) had one room and 42(5%) lived in a house with four rooms.
Half of the total respondents’ 432(51.2%) of households shared the living houses with different kind of animals but 411(48.8%) households did not. Three hundred and twelve respondents lived with a cow/bull and 76(22.8%) with sheep, goats, donkey and hens within different proportions (see table 5.4).
Table 5. 4: Housing characteristics of respondents in Sidama Regional State, Ethiopia: 2020 (N=843)
| Characteristics | Frequency | Percentage | |
| Roof materials of living house (N=843) | Grass | 404 | 47.9 |
| Corrugated | 430 | 51.0 | |
| Bamboo | 9 | 1.1 | |
| Total | 843 | 100 | |
| Floor material of living house (N=843) | Mud | 458 | 54.3 |
| Cement | 338 | 40.1 | |
| Wood | 47 | 5.6 | |
| Total | 843 | 100 | |
| Presence of window in the living house (N=843) | Yes | 529 | 62.8 |
| No | 314 | 37.2 | |
| Total | 843 | 100 | |
| Number of rooms in the living (843) | One | 181 | 21.5 |
| Two | 384 | 45.5 | |
| Three | 236 | 28.0 | |
| Four | 42 | 5.0 | |
| Total | 843 | 100 | |
| Animal living with the same house (N=843) | Yes | 411 | 48.8 |
| No | 432 | 51.2 | |
| Total | 843 | 100 | |
| Kind of animal which lived with the same house (N=411) | Cow/Bull | 311 | 75.7 |
| Sheep | 58 | 14.1 | |
| Goat | 33 | 8.0 | |
| Donkey | 5 | 1.2 | |
| Hen | 4 | 1.0 | |
| Total | 411 | 100 | |
Household energy sources were assessed and the analysis revealed that majority of households 686(81.4%) used firewood while 147(17.4%) used charcoal as major energy sources. More than quarter 263(31.2%) of households used charcoal for cooking and other related purposes.
Of 263 households that used charcoal; 107(40.7%) used it twice per day followed with 102(38.8%) once a day, 43(16.3%) three times and above per day and 11(1.3%) used it only once per every two days.
More than half 489(58%) of households used kitchen for cooking and 336(39.9%) cooking in the main house and 18(2.1%) cooked outdoor. Three hundred twenty-two (38.2%) of households had chimney during data collection.
The current study analysis revealed that 12(1.4%) used electricity as source of energy for lighting in their households while 428(50.8%) of households used kerosene lamp (locally known as kuraz), 364(43.1%) used hurricane lamp or lantern (locally known as fanos/masho) and 39(4.6%) wood.
The place of children where they usually stay when their mothers are preparing food was also assessed and 486(57.7%) of respondents responded that the child stays outside of the cooking place while 357(42.3%) carried the child on their back or by the side of mothers (see table 5.5).
Table 5. 5: Households’ energy sources and related characteristics in Sidama regional state, Ethiopia: 2020 (N=843)
| Characteristics of HHs energy sources | Frequency | Percentage | |
Type of firewood (N=843) | Charcoal | 147 | 17.4 |
| Wood | 686 | 81.4 | |
| Electricity | 10 | 1.2 | |
| Total | 843 | 100 | |
| Charcoal use (N=843) | Yes | 263 | 31.2 |
| No | 580 | 68.8 | |
| Total | 843 | 100 | |
| Frequency of charcoal use(N=263)* | Once per day | 102 | 38.8 |
| Twice per day | 107 | 40.7 | |
| Three times and above per day | 43 | 16.3 | |
| Once per every two days | 11 | 4.2 | |
| Total | 263 | 100 | |
Usual place for cooking (N=843) | Main house | 336 | 39.9 |
| Kitchen | 489 | 58.0 | |
| Outdoor | 18 | 2.1 | |
| Total | 843 | 100 | |
| Presence of chimney during data collection (N=843) | Yes | 322 | 38.2 |
| No | 521 | 61.8 | |
| Total | 843 | 100 | |
Source of light at home (N=843) | Hurricane lamp/Masho/Fanos | 364 | 43.2 |
| Kerosene lamp/Kuraz | 428 | 50.8 | |
| Wood | 39 | 4.6 | |
| Electricity | 12 | 1.4 | |
| Total | 843 | 100 | |
| Usual location of child while mothers cook (N=843) | On back or beside of mothers | 357 | 42.3 |
| Outside the cooking area | 486 | 57.7 | |
| Total | 843 | 100 | |
*There were only 263 households those used charcoal
5.3.5 Nutrition related characteristics of surveyed child
Respondents were asked about the status of breastfeeding and complementary feeding practices of child. Majority of mothers 578(68.6%) had initiated their children on breast milk immediately after birth while 159(18.9%) within one hour after delivery, 85(10.1%) after an hour but within 24 hours and 21(2.5%) of them initiated after a day.
Out of 843 mothers’ children aged under 5 years included in this study, 328(38.8%) had breastfed their child for more than two years; followed by 154(18.3%) who breastfed their child up to 2 years, and 63(7.5%) of them did it up to 12 months and 57(6.8%) for less than 6 months. In addition, 242(28.7%) of the respondents include both mothers who did not know for how long they breastfed their children and those who were still breastfeeding during data collection.
Regarding frequency of breastfeeding of children per day, 239(28.4%) had breastfed their children for up to 10 times, 115(13.5%) of them breast fed five times or less and 91(10.8%) for more than 10 times. The remaining 398(47.2%) could not remember how many times they breast-fed their children and were not breast-feeding during the data collection period.
Majority of mothers 763(90.5%) had commence complementary feeding during data collection and only 80(9.5%) did not. For children on complementary feeding, 620(81.3%) started exactly at recommended 6 months while 103(13.5%) had initiated their children for complimentary feeding early (less than six months) and 40(5.2%) did after 6 months. Furthermore, 344(38.4%) of mothers or caregivers used spoons for feeding the children, 210(24.9%) used their hands, 135(16%) used bottles and 94(11.2%) used cups (refer table 5.6)
Table 5. 6: Child breastfeeding and complementary feeding practices among mothers in Sidama regional state, Ethiopia: 2020, (N=843)
| Characteristics of child feeding practices of households’ | Frequency | Percentage | |
Initiation of breast-feeding (N=843) | Immediately after birth | 578 | 68.6 |
| Within an hour | 159 | 18.8 | |
| Between 1 and 24 hours | 85 | 10.1 | |
| After a day | 21 | 2.5 | |
| Total | 843 | 100 | |
Duration for breast-feeding (N=843) | < 6> | 57 | 6.7 |
| 7-12 months | 63 | 7.5 | |
| Up to 2 years | 154 | 18.3 | |
| >2 Years | 327 | 38.8 | |
| Others* | 242 | 28.7 | |
| Total | 843 | 100 | |
Frequency of breast-feeding per day (N=843) | <= 5 times | 115 | 13.6 |
| Up to 10 times | 239 | 28.4 | |
| >10 times | 91 | 10.8 | |
| Others** | 398 | 47.2 | |
| Total | 843 | 100 | |
Had started complementary feeding (N=843) | Yes | 763 | 90.5 |
| No | 80 | 9.5 | |
| Total | 843 | 100 | |
| When had started complementary feeding (N=763), | < 6> | 103 | 13.5 |
| At 6 months | 620 | 81.3 | |
| >6 months | 40 | 5.2 | |
| Total | 763 | 100 | |
| Materials used for feeding the child (N=763) | Bottle | 135 | 17.7 |
| Cup | 96 | 12.6 | |
| Spoon | 321 | 42.0 | |
| Hand | 211 | 27.7 | |
| Total | 763 | 100 | |
Others* = the respondents could not remember the frequency that they breastfed their children
Others** = the respondents did not remember the specific number of times (frequency) they breastfed their children
5.3.6 Vitamin A supplementation, deworming and immunization status of child
The status of vitamin A supplementation and deworming for the children were assessed and verified from the children’s immunization card. The results showed that 545(64.7%) of children received vitamin A, 245(29.1%) did not and 53 (6.3%) were not eligible for vitamin A supplementation. In addition, 365(43.3%) of the children were dewormed while 478(56.7%) were either not dewormed or had exceeded the age for deworming (see table 5.7)
The current study analysis showed that 765(90.7%) of children had received at least one vaccine while 78 (9.3%) had not get vaccinated against any disease. Of those children who received vaccination, 802(85.1%) received three doses of both penta 3 and PCV10, 82(9.7%) received two doses and 18(2.1%) received one dose. About 656 (77.8%) of the children were vaccinated for measles as depicted in table 5.7.
Table 5. 7: Vitamin A supplementation, deworming and immunization status of surveyed children in Sidama regional state, Ethiopia: 2020 (N=843)
| Characteristics of surveyed child | Frequency | Percentage | |
Supplemented with vitamin A (N=843) | Yes | 545 | 64.7 |
| No | 245 | 29.1 | |
| Not eligible* | 53 | 6.3 | |
| Total | 843 | 100 | |
Deworming received (N=843) | Yes | 365 | 43.3 |
| No | 169 | 20.0 | |
| Not eligible** | 309 | 36.7 | |
| Total | 843 | 100 | |
| Received any of vaccine and dose (N=843) | Yes | 765 | 90.7 |
| No | 78 | 9.3 | |
| Total | 843 | 100 | |
Received dose of Penta3 & PCV10 (N=843) | One | 18 | 2.1 |
| Two | 82 | 9.7 | |
| Three | 743 | 88.2 | |
| Total | 843 | 100 | |
Received measles vaccine (N=843) | Yes | 656 | 77.8 |
| No | 98 | 11.6 | |
| Not eligible*** | 89 | 10.6 | |
| Total | 843 | 100 | |
Not Eligible* = Children who were not eligible for Vitamin A (whose age was < 6>
Not Eligible** = Children whose age were not eligible for deworming (<23>
Not Eligible*** = Children who were not eligible for measles (whose age was < 9>
5.3.7 Behavioural and disease status of child’s family
Data on families’ history of smoking, presence or absence of any respiratory disease and HIV/AIDS status were assessed and results in this regard revealed that 19(2.3%) families had history of smoking, 38(4.5%) respiratory disease and 4(0.5%) HIV positive status.
Of those who had the history of smoking, 13(68.4%) were father of the child, 3(15.8%) were mothers and others 3(15.8%) were brothers for the sample child. Similarly, of the 38 families who had reported the history of respiratory diseases, 17(44.7%) were child’s father, 13(34.2%) were mothers and 8(21.1%) were other family members (see table 5.8 below).
Table 5. 8: Behavioural and disease history of child’s family member in Sidama Regional State, Ethiopia: 2020, (N=843)
| Behavioural and disease status characteristics of HHs | Frequency | Percentage | |
| Any smoker among family members (N=843) | Yes | 19 | 2.3 |
| No | 824 | 97.7 | |
| Total | 843 | 100 | |
| If yes who was the smoker (N=19) | Father | 13 | 68.4 |
| Mother | 3 | 15.8 | |
| Brother | 3 | 15.8 | |
| Total | 19 | 100 | |
| The presence of a family member living with HIV (N=843) | Yes (positive for HIV) | 4 | 0.5 |
| No (negative for HIV) | 814 | 96.5 | |
| Unknown status (did not tested for HIV) | 25 | 3.0 | |
| Total | 843 | 100 | |
| Who was positive for HIV (N=843) | Father | 2 | 50.0 |
| Mother | 2 | 50.0 | |
| Total | 4 | 100 | |
| A family members had history of respiratory disease (N=843) | Yes | 38 | 4.5 |
| No | 805 | 95.5 | |
| Total | 843 | 100 | |
| Who had history of respiratory disease (N=38) | Father | 17 | 44.7 |
| Mother | 13 | 34.2 | |
| Others*(brothers & sisters) | 8 | 21.1 | |
| Total | 38 | 100 | |
According to the respondents responses, 203(24.1%) of children had the
history of cough and cold with or without fever for less than two weeks duration. However detailed analysis revealed that 187(22.2%) of the children were further assessed and were confirmed to suffer from pneumonia by counting their respiration rate (RR), (see figure 5.2) which shows the prevalence of childhood pneumonia.
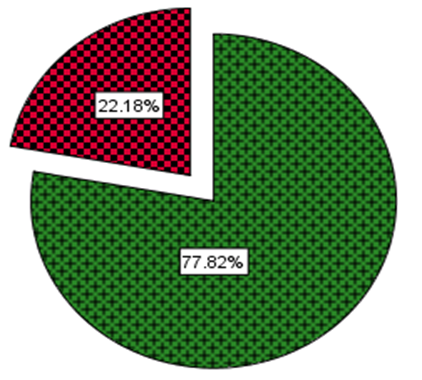
Figure 5. 2: The prevalence of pneumonia among under-five children in Sidama Regional State, Ethiopia: 2020 (N=843)
The bivariate analysis of the current study was done using Chi-square test to investigate the presence of significant association between childhood pneumonia and possible risk factors. The result of the bivariate analysis of the study was presented following the proposed objectives. The variables with p-value less than or equal to 0.25 at the bivariate analysis were included in the multivariate analysis.
5.3.8.2.1 The association between the socio-demographic and economic factors and the occurrence of pneumonia among under-5 year’s children
5.3.8.2.1.1 Households’ socio-demographic and economic characteristics and association with the occurrence of pneumonia among under-5 year’s children
Table 5.12: below presents the results of bivariate analysis amongst the households’ socio-demographic and economic characteristics and childhood pneumonia disease occurrence in the study area. The result showed that the children living in household with medium family size (COR=2.30; 95%CI: 1.58, 3.36) and large family size (COR=4.00, 95%CI: 2.54, 6.30) were more likely to develop pneumonia. Similarly, mothers/caregivers with no formal education (COR= 3.25, 95%CI: 1.42, 7.42) were more likely to develop childhood pneumonia.
Being rural residence (COR=0.54, 95%CI: 0.30, 0.95) was found as the protective factor for the children not to develop pneumonia. However, the rest of socio-demographic and economic characteristics like relation of respondent, sex of the mother/caregiver, marital status of the mother, religion, ethnicity, and residence, age of mother/caregiver and education level of child’s father were found not to influence the occurrence of pneumonia among children aged under 5.
Table 5. 9: Bivariate analysis of mother’s/caregivers’ socio-demographic and economic characteristics of mothers/care givers in Sidama regional state: 2020
| No | Variables | Pneumonia status | COR of 95% CI | p-value | |
| Yes (n %) | No (n %) | ||||
| 1 | Relation of respondent to child | ||||
| Mother | 154(21.8) | 553(78.2) | 1 | ||
| Father | 26(24.8) | 79(75.2) | 1.18(0.73, 1.91) | 0.50 | |
| Care giver | 7(22.6) | 24(77.4) | 1.05(0.44, 2.48) | 0.92 | |
| 2 | Sex of mothers/care givers | ||||
| Female | 161(21.8) | 577(78.2) | 0.85(0.53, 1.36) | 0.50 | |
| Male | 26(24.8) | 79(75.2) | 1 | ||
| 3 | Marital status of mothers/care givers | ||||
| Single | 3(15.8) | 16(84.2) | 1.25(0.22, 7.05) | 0.80 | |
| Married | 181(22.6) | 620(77.4) | 1.95(0.57, 6.62) | 0.29 | |
| Widowed | 3(13.0) | 20(87.0) | 1 | ||
| 4 | Religion of mothers/care givers | ||||
| Protestant | 164(22.0) | 583(78.0) | 1.06(0.54, 2.04) | 0.87 | |
| Orthodox | 10(31.3) | 22(68.7) | 1.71(0.64, 4.55) | 0.29 | |
| Muslim | 1(14.3) | 6(85.7) | 0.63(0.70, 5.70) | 0.68 | |
| Others | 12(21.1) | 45(78.9) | 1 | ||
| 5 | Ethnicity of mothers/care givers | ||||
| Sidama | 175(21.8) | 628(78.2) | 0.65(0.32, 1.31) | 0.26 | |
| Others | 12(30.0) | 28(70.0) | 1 | ||
6 | Residence of mothers/care givers | ||||
| Urban | 20(33.3) | 40 (66.7) | 1 | ||
| Rural | 167(21.3) | 616 (78.7) | 0.54 (0.30, 0.95) | 0.03* | |
7 | Family size of household | ||||
| Small | 57(12.5) | 399(87.5) | 1 | ||
| Medium | 71(28.3) | 180(71.7) | 2.30(1.58, 3.36)* | 0.00* | |
| Large | 59(43.4) | 77(56.6) | 4.00(2.54, 6.30)* | 0.00* | |
8 | Educational status of mothers/care givers | ||||
| No formal education | 82(44.1) | 104(55.9) | 3.25(1.42, 7.42)* | 0.05* | |
| Primary education (1-8) | 77(14.8) | 445(85.2) | 0.71(0.32, 1.60) | 0.41 | |
| Secondary education (9-12) | 20(21.3) | 74(78.7) | 1.11(0.45, 2.79) | 0.82 | |
| Certificate and above** | 8(19.5) | 33(80.5) | 1 | ||
| 9 | Age category of mothers/care givers | ||||
| 16-24 years | 46(23.8) | 147(76.2) | 1 | ||
| 25-35 years | 104(20.6) | 401(79.4) | 0.87(0.59, 1.21) | 0.50 | |
| >=36 years | 37(25.5) | 108(74.5) | 1.31(0.79, 2.16) | 0.30 | |
*Statistical significant at p ≤0.25
5.3.8.2.1.2 Socio-demographic characteristics of child and association with the occurrence of pneumonia among under-5 year’s old children
The result of bivariate analysis showed that being male child (COR=1.23, 95%CI: 0.89, 1.70, p=0.22), children with birth interval of less than two years (COR=1.99, 95%CI: 1.38, 2.87, p<0 COR=2.11, p=0.006 p=0.004)>
Table 5. 10: Socio-demographic characteristics of child and the occurrence of pneumonia among under five children in Sidama Regional State: 2020
| No | Variables | Pneumonia status | COR of 95% CI | p-value | |
| Yes (n %) | No (n %) | ||||
| 1 | Age of child | ||||
| ≤6 months | 8(15.1) | 45(84.9) | 0.97(0.42, 2.23) | 0.94 | |
| 7-12 months | 34(27.9) | 88(72.1) | 2.11(1.24, 3.58) | 0.006* | |
| 13-36 months | 108(25.2) | 321(74.8) | 1.84(1.22, 2.78) | 0.004* | |
| 37-59 months | 37(15.5) | 202(84.5) | 1 | ||
| 2 | Place of birth | ||||
| Health institutions | 137(21.9) | 489(78.1) | 1 | ||
| Home | 50(23.0) | 167(77.0) | 1.07(.74, 1.56) | 0.72 | |
| 3 | Sex of Child | ||||
| Male | 101(23.9) | 321(76.1) | 1.23(0.89, 1.70)* | 0.22* | |
| Female | 86(23.4) | 335(79.6) | 1 | ||
4 | Number of children the mothers had | ||||
| One | 45(23.1) | 150(76.9) | 1.16(0.68, 2.01) | 0.58 | |
| Two | 48(22.3) | 167(77.7) | 1.12(0.65, 1.91) | 0.69 | |
| Three | 45(25.1) | 134(74.9) | 1.31(0.75, 2.26) | 0.34 | |
| Four | 23(18.1) | 104(81.9) | 0.86(0.46, 1.60) | 0.63 | |
| Five and above | 26(20.5) | 101(79.5) | 1 | ||
5
| Birth interval with in the older child | ||||
| < 2> | 58(32.4) | 121(67.6) | 1.99(1.38, 2.87)* | 0.00* | |
| ≥2 years | 129(19.4) | 535(80.6) | 1 | ||
6 | Birth order of the child | ||||
| First | 45(23.0) | 151(77.0) | 1 | ||
| Second | 48(22.4) | 166(77.6) | 0.97(0.61, 1.54) | 0.90 | |
| Third | 45(25.1) | 134(74.9) | 1.13(0.70, 1.81) | 0.62 | |
| Fourth and above | 49(19.3) | 1205(80.7) | 0.80(0.51, 1.27) | 0.34 | |
*Statistical significant at p ≤0.25
5.3.8.2.2 Bivariate analysis of behavioural and disease history of household members and occurrence of pneumonia among under-five year’s children
Findings of bivariate analysis showed that children from households where family member had smoking history (COR=0.41, 95%CI: 0.09, 1.78, p= 0.23) and also history of respiratory diseases (COR=11.38, 95%CI: 5.41, 23.91, p=0.00) were found to more likely suffer from pneumonia than those who were not from such family.
Children who had history of disease during data collection period (COR=1.91, 95%CI: 1.28, 2.86, p=0.00) and those children who had past history of measles within last one year during data collection (COR=8.70, 95%CI: 1.04, 72.77) were more likely to suffer from pneumonia than those who did not have same history. But children who had other chronic disease history were not identified as the factors for pneumonia in current study (see table 5.11) below.
Table 5. 11: Behavioural and disease history and the occurrence of pneumonia among under-five year’s children in Sidama Regional State: 2020
| No | Variables | Pneumonia status
| COR of 95% CI | p-value | |
| Yes (n %) | No (n %) | ||||
| 1 | A smoker among family member | ||||
| Yes | 2(10.5) | 17(89.5) | 0.41(0.09, 1.78)* | 0.23* | |
| No | 185(22.5) | 639(77.5) | 1 | ||
| 2 | The presence of a family member living with HIV | ||||
| Yes | 1(25.0) | 3(75.0) | 1.06(0.09, 12.14) | 0.97 | |
| No | 180(22.1) | 634(77.9) | 0.90(0.35, 2.29) | 0.82 | |
| Unknown status | 6(24.0) | 19(76.0) | 1 | ||
| 3 | A family members had history of respiratory disease | ||||
| Yes | 28(73.7) | 10(26.3) | 11.38(5.41,23.91)* | 0.00* | |
| No | 159(19.8) | 646(80.2) | 1 | ||
| 4 | Had history of current disease during data collection | ||||
| Yes | 44 (32.6) | 91 (67.4) | 1.91 (1.28, 2.86)* | 0.00* | |
| No | 143(20.2) | 565 (79.8) | 1 | ||
| 5 | Child had known disease historical | ||||
| Yes | 77(23.5) | 251(76.5) | 1.07(0.22, 5.28) | 0.93 | |
| No | 108(21.3) | 398(78.7) | 0.95(0.19, 4.64) | 0.95 | |
| Not known | 2(22.2) | 7(77.8) | 1 | ||
| 6 | Have child had measles disease last year | ||||
| Yes | 67(55.4) | 54(44.6) | 8.70(1.04, 72.77)* | 0.05* | |
| No | 119(16.7) | 595(83.3) | 1 | ||
*Statistical significant at p ≤0.25
5.3.8.2.3 Bivariate analysis of environmental characteristics of households and the occurrence of pneumonia among under-five year’s old children
According to the result of bivariate analysis households without latrine (COR=5.81, 95%CI: 3.77, 8.96, p=0.00) were more likely to contribute for the occurrence of childhood pneumonia. Furthermore the absence of a separate house for animals and humans (COR=1.73, 95%CI: 1.25, 2.41, p<0 COR=3.68,>
The other environmental variables that influenced the occurrence of pneumonia among under-five children were household with only one room (COR=2.02, 95%CI: 0.84, 4.83, p=0.12), families using charcoal as main source of energy (COR=3.69, 95%CI: 2.63, 5.18, p<0 COR=2.12,>
The other environmental variables like the usual place of cooking and solid waste management were found to be the protective factors of the childhood pneumonia while roofing materials did not show any significance contribution for the occurrence of pneumonia in the current study area.
Table 5. 12: Bivariate analysis of environmental characteristics of households in Sidama Regional State: 2020
| No | Variables | Pneumonia status | COR of 95% CI | P- value | |
| Yes (n %) | No (n %) | ||||
| 1 | Households had latrine | ||||
| Yes | 130(17.6) | 610(82.4) | 1 | ||
| No | 57(55.3) | 46(44.7) | 5.81(3.77, 8.96)* | <0> | |
| 2 | Solid waste management system of the HHs | ||||
| Backyard simple | 116(22.1) | 409(77.9) | 0.80(0.50, 1.24) | 0.31 | |
| Blow a fuse at anywhere | 39(19.8) | 158(80.2) | 0.69(0.40, 1.47) | 0.17* | |
| Bury | 32(26.4) | 89(73.6) | 1 | ||
| 3 | Separate living house for animals and humans | ||||
| Yes | 76(17.6) | 356(82.4) | 1 | ||
| No | 111(27.0) | 300(73.0) | 1.73(1.25, 2.41)* | <0> | |
| 4 | Roofing material of living house | ||||
| Grass | 112(27.7) | 292(72.3) | 1.34(0.27,6.56) | 0.72 | |
| Corrugated iron | 73(17.0) | 357(83.0) | 0.72(0.15, 3.51) | 0.68 | |
| Bamboo | 2(22.2) | 7(77.8) | 1 | ||
5 | Presence of window in the living house | ||||
| Yes | 69(13.3) | 448(86.7) | 1 | ||
| No | 118(36.2) | 208(63.8) | 3.68(2.62, 5.17)* | <0> | |
6 | Number of rooms of the living house | ||||
| One | 52(28.7) | 129(71.3) | 2.02(0.84, 4.83)* | 0.12* | |
| Two | 83(21.6) | 301(78.4) | 1.38(0.59, 3.22) | 0.46 | |
| Three | 45(19.1) | 191(80.9) | 1.18(0.49, 2.82) | 0.71 | |
| Four and above | 7(16.7) | 350(83.3) | 1 | ||
7 | Usually place for cooking | ||||
| Main house | 63(18.7) | 273(81.3) | 0.36(0.14, 0.97) | 0.04* | |
| Kitchen | 117(23.9) | 372(76.1) | 0.16(0.19, 1.30) | 0.16* | |
| Outdoor | 7(38.9) | 11(61.1) | 1 | ||
| 8 | Use of charcoal | ||||
| Yes | 102(38.8) | 161(61.2) | 3.69(2.63, 5.18)* | <0> | |
| No | 85(14.7) | 495(85.3) | 1 | ||
| 9 | Presence of chimney | ||||
| Yes | 98(30.4) | 224(69.6) | 2.12(1.52, 2.95)* | 0.00* | |
| No | 89(17.1) | 432(82.9) | 1 | ||
*Statistical significant at p ≤0.25
5.3.8.2.4 Bivariate analysis of nutritional and immunization characteristics of child and the occurrence of pneumonia among under-five year’s old children
Table 5.13 presents the result of bivariate analysis of nutritional and immunization status of child and the association with the occurrence of pneumonia among under-five children. The result showed that severely malnourished children (COR=2.33, 95%CI; 1.43, 3.81, p=0.001) and initiation of breastfeeding after a day of delivery (COR=2.82, 95%CI; 1.00, 7.97, p=0.03), were found to be contributing factors of childhood pneumonia occurrence in Sidama Regional State. Similarly lack of receiving vitamin A and deworming within last six months preceding to data collection, and not receiving any dose of vaccine and measles were also obtained as significant contributing factors of childhood pneumonia in study area with the [(COR=5.81, 95%CI: 4.06, 8.31, p<0 COR=1.50, p=0.06); COR=8.74, COR=4.30,>
However, type of materials used to feed the child were found to be the protective factors while receiving PCV10 vaccine did not show any significant association with the occurrence of pneumonia among children in the study area (see table 5.13).
Table 5. 13: Bivariate analysis of nutritional and immunization related status of children and the occurrence of pneumonia among under-five year’s children in Sidama Regional State: 2020
| No | Variables | Pneumonia status | COR of 95% CI | P-value | |
| Yes (n %) | No (n %) | ||||
| 1 | Nutritional status of children (weight for age) | ||||
| Normal | 130(20.5) | 505(79.5) | 1 | ||
| Under weight | 27(21.1) | 101(78.9) | 1.04(0.65, 1.66) | 0.87 | |
| Severe under weight | 30(37.5) | 50(62.5) | 2.33(1.43, 3.81) | 0.001* | |
| 2 | Initiation of breast feeding | ||||
| Immediately at birth | 124(21.5) | 454(78.5) | 1 | ||
| Within one hour after birth | 37(23.3) | 122(76.7) | 1.11(0.69, 1.76) | 0.68 | |
| Between first 1 and 24 hour | 17(20.0) | 68(80.0) | 0.86(0.46, 1.62) | 0.65 | |
| After a day | 9(42.9) | 12(57.1) | 2.82(1.00, 7.97) | 0.03* | |
| 3 | Materials used to fed the child | ||||
| Bottle | 51(37.5) | 85(62.5) | 1 | ||
| Cup | 25(26.0) | 71(74.0) | 0.59(0.33, 1.04) | <0> | |
| Spoon | 66(20.6) | 254(79.4) | 0.43(0.28, 0.67) | <0> | |
| Hand | 31(14.6) | 181(85.4) | 0.29(0.17, 0.49) | <0> | |
| Not eligible | 14(17.7) | 65(82.3) | 0.36(0.18, 0.70) | 0.003* | |
| 4 | Received vitamin A last 6 month | ||||
| Yes | 68(12.5) | 477(87.5) | 1 | ||
| No | 111(45.3) | 134(54.7) | 5.81(4.06, 8.31)* | <0> | |
| Not eligible | 8(15.1) | 45(84.9) | 1.25(0.56, 2.76) | 0.59 | |
| 5 | Dewormed with in last 6 months | ||||
| Yes | 71(19.5) | 294(80.5) | 1 | ||
| No | 45(26.6) | 124(73.4) | 1.50(0.98, 2.31) | 0.06* | |
| Not eligible | 71(23.0) | 238(77.0) | 1.23(0.85, 1.79) | 0.26 | |
| 6 | Any vaccine and dose given | ||||
| Yes | 136(17.8) | 629(82.2) | 1 | ||
| No | 51(65.4) | 27(34.6) | 8.74(5.29, 14.43)* | <0> | |
| 7 | Received measles vaccine | ||||
| Yes | 122(18.6) | 535(81.4) | 1 | ||
| No | 48(49.5) | 49(50.5) | 4.30(2.76, 6.70)* | <0> | |
| Not eligible | 17(19.1) | 72(80.9) | 1.04(0.59, 1.82) | 0.90 | |
| 8 | PCV10 given | ||||
| Yes | 173(21.6) | 628(78.4) | 1 | ||
| No | 2(40.0) | 3(60.0) | 1.34(0.47, 3.80) | 0.59 | |
| Not eligible | 12(31.6) | 25(68.4) | 0.84(0.48, 1.49) | 0.56 | |
*Statistical significant at p ≤0.25
5.3.8.4 Multivariate analysis of factors and association with the occurrence of pneumonia among under-five year’s old children
The multivariate analysis were employed by using the binary logistic regression with conditional backward stepwise method. Likwise Hosmer and Lemeshow Test was performed in order to recognise the risk factors that are self-sufficiently associated with childhood pneumonia though controlling for confounders. The same controlling variables for binary logistic regression were kept for multivariate analysis also. Independent variables those were significantly associated with childhood pneumonia at a p-value less than 0.25 in the bivariate analysis while using Chi-square tests were included in the multivariable analysis. The association of risk factors with the occurrence of pneumonia were recognised based on p-value less than 0.05 and considering 95% confidence interval also.
5.3.8.4.1 Multivariate analysis of socio-demographic and economic factors and the occurrence of pneumonia among under-five children
From binary logistic regression there were five different socio-demographic and economic factors found to influence the occurrence of childhood pneumonia with p-value less than 0.25. Those potential risk factors were checked under multivariate analysis for proper identification as risk factors of pneumonia with controlling the likely confounders. From the backward stepwise method used for the analysis, the Omnibus Tests of Method coefficients analysed for the socio-demographic factors and childhood pneumonia occurrence, to check that the model significantly elucidated the relationship (see table 5.15).
Table 5. 14: Omnibus Test of model coefficients for the socio-demographic and economic variables and the occurrence of childhood pneumonia, in Sidama Regional State, Ethiopia: 2020
As the result from multivariate analysis indicate: that family size, educational level of respondents, age of child and birth interval of sample child with its older child were found to be associated factors for the occurrence of pneumonia among under-five children.
Both medium and large family size were significantly associated with the occurrence of childhood pneumonia with p-value less than 0.001 for both categories. Children from large family size were 4.34 times and children from medium family size were 2.39 times more possible to suffer from pneumonia with (AOR: 4.34; 95%CI 2.65, 7.10; p<0>
The result of multivariate analysis revealed that mothers or caregivers who never had formal education were found to be one of the causal factors for the occurrence of pneumonia among under five children. Children from mothers or caregivers who did not have formal education were 4.10 times more likely to develop pneumonia as compared to their counterparts of educated mothers/caregivers (AOR: 4.10; 95%CI; 1.65, 10.00; p=0.002).
Birth interval of the surveyed child with its older child was also significantly associated with the occurrence of pneumonia in children, p=0.01. Detailed analysis showed that children who had birth intervals of less than 2 years were 1.65 times more likely to develop pneumonia than those that had birth intervals of more than 2 years with their respective older siblings (AOR:1.65: 95%CI: 1.10, 2.48; p=0.02).
There was a momentous association among the age category of children and pneumonia occurrence. The finding of multivariate analysis revealed that the middle age group (7-36 months) children were affected more than children in the rest age group. Children from age group 7-12 months were 2.63 times affected and those 13-36 months were 2.20 times more likely to develop pneumonia than the others, with (AOR: 2.63; 95%CI: 1.46, 4.74; p=0.001 and AOR:2.20; 95%CI: 1.40, 3.46; p=0.001) respectively.
However, the sex of the child and their residence did not show any significant association for the occurrence of pneumonia in the current study area as the result of multivariate analysis revealed (see table 5.15).
Table 5. 15: Multivariate analysis of household’s socio-demographic and economic factors and occurrence of pneumonia among under-five children in Sidama Regional State, Ethiopia: 2020
| No | Variables | Pneumonia status | COR of 95% CI | AOR of 95% CI | P-value | |
| Yes (n %) | No (n %) | |||||
1 | Family size | |||||
| Small | 57(12.5) | 399(87.5) | 1 | 1 | ||
| Medium | 81(26.8) | 221(73.2) | 2.30(1.58, 3.36)* | 2.39(1.60, 3.59) | <0> | |
| Large | 49(38.9) | 77(61.1) | 4.00(2.54, 6.30)* | 4.34(2.65, 7.10) | <0> | |
2
| Educational status of respondents | |||||
| No formal education | 82(44.1) | 104(55.9) | 3.25(1.42, 7.42)* | 4.10(1.65, 10.00) | 0.002* | |
| Primary education (1-8) | 77(14.8) | 445(85.2) | 0.71(0.32, 1.60) | 0.89(0.37, 2.18) | 0.81 | |
| Secondary education (9-12) | 20(21.3) | 74(78.7) | 1.11(0.45, 2.79) | 1.33(0.50, 3.56) | 0.57 | |
| Certificate and above | 8(19.5) | 33(80.5) | 1 | 1 | ||
3 | Age of child | |||||
| ≤6 months | 8(15.1) | 45(84.9) | 0.97(0.42, 2.23) | 1.15(0.47, 2.80) | 0.76 | |
| 7-12 months | 34(27.9) | 88(72.1) | 2.11(1.24, 3.58)* | 2.63(1.46, 4.74) | 0.001* | |
| 13-36 months | 108(25.1) | 321(74.8) | 1.84(1.22, 2.78)* | 2.20(1.40, 3.46) | 0.001* | |
| 37-59 months | 37(15.5) | 202(84.5) | 1 | 1 | ||
4 | Sex of Child | |||||
| Male | 101(23.9) | 321(76.1) | 1.23(0.89, 1.70)* | 1.23(0.84, 1.73) | 0.31 | |
| Female | 86(23.4) | 335(79.6) | 1 | 1 | ||
| 5 | Birth interval within older | |||||
| < 2> | 58(32.4) | 121(67.6) | 1.99(1.38, 2.87)* | 1.65(1.10, 2.48) | 0.02* | |
| ≥ 2 years | 129(19.4) | 535(80.6) | 1 | 1 | ||
| Residence of respondents | ||||||
| Urban | 20(33.3) | 40 (66.7) | 1 | 1 | ||
| Rural | 167(21.3) | 616 (78.7) | 0.54 (0.30, 0.95) | 0.75(0.38, 1.45) | 0.39 | |
1 indicates reference category, * indicates, Significant association at p<=0.05 and ** indicates highly significant association at p< 0>
5.3.8.4.2 Multivariate analysis of behavioural and disease history of households and the occurrence of pneumonia among under-five children
Four different behavioural and disease related variables those presented a significant association in binary logistic regression were performed in multivariate analysis to check the association with childhood pneumonia occurrence. From these variables like children who had family member/s with the history of respiratory disease and children had suffered from measles disease in the previous one year prior to data collection showed high significant association (p<0 p=0.03).>
The value of chi-square with degree of freedom and p-value of Omnibus Test of model coefficients were checked to identify the association (see table 5.16).
Table 5. 16: Omnibus Test of model coefficients for the behavioral and disease history of households’ family member and the occurrence of childhood pneumonia, in Sidama Regional State, Ethiopia: 2020
Similarly the p-value and X2 with degree of freedom of Hosmer and Lemeshow Test was also assured. See table 5.17:
Table 5. 17: Hosmer and Lemeshow Test for the socio-demographic variables and the occurrence of childhood pneumonia, in Sidama Regional State, Ethiopia: 2020
History of respiratory disease among family member was found as risk factor for the occurrence of childhood pneumonia with p- value less than 0.001. Children who had family member/s with the history of respiratory disease were 5.63 times more likely to suffer from pneumonia than their counterparts who lived with family members without the history of respiratory disease (AOR: 5.63; 95%CI 2.74-11.57; p<0>
The history of any disease among children during data collection was found to significantly influence the occurrence of pneumonia p=0.03. Children with any of disease history during data collection were 1.63 times more likely to develop pneumonia (AOR: 1.63; 95%CI: 1.04, 2.53; p=0.03). Detailed analysis revealed that children had suffered from measles disease in the previous one year prior to data collection were 5.96 more likely to develop pneumonia with (AOR: 5.96; 95%CI: 3.91, 9.07; p<0>
However, having the history of HIV virus among family members did not show significant association after controlling the confounders (see table 5.18).
Table 5. 18: Multivariate analysis of behavioural and disease history of households and the occurrence of pneumonia among under-five children in Sidama Regional State, Ethiopia: 2020 (N=843)
| No | Variables | Pneumonia status | COR of 95% CI | AOR of 95%CI | P- value | |
| Yes (n %) | No (n %) | |||||
| 1 | A smoker among family member | |||||
| Yes | 2(10.5) | 17(89.5) | 0.41(0.09, 1.78)* | 0.32(0.07, 1.47) | 0.14 | |
| No | 185(22.5) | 639(77.5) | 1 | 1 | ||
| 2 | A family members had history of respiratory disease | |||||
| Yes | 22(57.9) | 16(42.1) | 5.63(2.74, 11.57)** | <0> | ||
| No | 165(20.5) | 640(79.5) | 1 | 1 | ||
| 3 | Had history of current disease during data collection | |||||
| Yes | 44 (32.6) | 91 (67.4) | 1.91 (1.28, 2.86)* | 1.63(1.04, 2.53) | 0.03* | |
| No | 143(20.2) | 565 (79.8) | 1 | |||
| 4 | Have child had measles disease last year | |||||
| Yes | 67(55.4) | 54(44.6) | 6.20(1.12, 9.34)* | 5.96(3.91, 9.07) | <0> | |
| Unknown | 1(12.5) | 7(87.5) | 0.71(0.09, 5.86) | 0.41(0.04, 3.78) | 0.43 | |
| No | 119(16.7) | 595(83.3) | 1 | 1 | ||
1 indicates reference category, * indicates, Significant association at p<=0.05 and ** indicates highly significant association at p< 0>
5.3.8.4.3 Multivariate analysis of environmental factors of households and the occurrence of pneumonia among under-five children
Table 5.19 below presents environmental factors that influence occurrence of childhood pneumonia at the study area at multivariate analysis. Five factors namely presence or absence of latrine in the household, living in the same household with domestic animals, the use of charcoal as the main source of energy, presence of chimney during the time of data collection and living in house without window were found to influence the occurrence of pneumonia.
There significant association were found between the absence of household latrine and the occurrence of childhood pneumonia at the study area. Children from households that did not avail latrine were 4.32 times more likely to develop pneumonia than those who were accessed for latrine (AOR: 4.32; 95%CI: 2.61, 7.15; p<0>
Children whose family did not have separate house for the animal and human being were 1.51 times more likely to develop pneumonia than those whose family had separate shelter for animals and human beings (AOR: 1.98; 95%CI: 1.30, 3.01; p=0.001). Also, children living in household that used charcoal as the main source of energy were 3.55 times more likely to suffer from pneumonia compared to their counterparts living in households who did not use charcoal (AOR=3.55; 95%CI 2.36, 5.35; p<0>
Analysis also revealed that having house with windows was found as the protective factor from pneumonia occurrence; as children who lived in houses without windows were found to be 4.60 times more likely to develop pneumonia than those who lived in houses with windows (AOR: 4.60; 95%CI: 2.93, 7.15; p<0 p=0.003).>
Table 5. 19: Multivariate analysis of environmental factors and the occurrence of pneumonia among under-five children in Sidama Regional State, Ethiopia: 2020 (N=843)
| No | Variables | Pneumonia status | COR of 95% CI | AOR of 95%CI | p- value | |
| Yes (n %) | No (n %) | |||||
| 1 | Households had latrine | |||||
| Yes | 130(17.6) | 610(82.4) | 1 | 1 | ||
| No | 57(55.3) | 46(44.7) | 5.81(3.77, 8.96)* | 4.32(2.61, 7.15) | <0> | |
| 2 | Separate living house for animal and human being | |||||
| Yes | 76(17.6) | 356(82.4) | 1 | 1 | ||
| No | 111(27.0) | 300(73.0) | 1.73(1.25, 2.41)* | 1.98(1.30, 3.01) | 0.001* | |
| 3 | Solid waste management system of the HHs | |||||
| Backyard simple | 116(22.1) | 409(77.9) | 0.80(0.50, 1.24) | 1.91(1.25, 2.91) | 0.90 | |
| Blow a fuse at anywhere | 39(19.8) | 158(80.2) | 0.69(0.40, 1.47) | 0.76(0.40, 1.48) | 0.42 | |
| Bury | 32(26.4) | 89(73.6) | 1 | 1 | ||
| 4 | Presence of window in the house | |||||
| Yes | 69(13.3) | 448(86.7) | 1 | 1 | ||
| No | 118(36.2) | 208(63.8) | 3.68(2.62, 5.17)* | 4.60(2.93, 7.15) | <0> | |
| 5 | No of rooms of the living house | |||||
| One | 52(28.7) | 129(71.3) | 2.02(0.84, 4.83)* | 2.20(0.80, 6.04) | 0.13 | |
| Two | 83(21.6) | 301(78.4) | 1.38(0.59, 3.22) | 1.20(0.46, 3.13) | 0.71 | |
| Three | 45(19.1) | 191(80.9) | 1.18(0.49, 2.82) | 1.25(0.47, 3.36) | 0.66 | |
| Four and above | 7(16.7) | 350(83.3) | 1 | 1 | ||
| 6 | Usually place for cooking | |||||
| Main house | 63(18.7) | 273(81.3) | 0.36(0.14, 0.97) | 0.39(0.12, 1.22) | 0.11 | |
| Kitchen | 117(23.9) | 372(76.1) | 0.16(0.19, 1.30) | 1.58(0.51, 4.89) | 0.42 | |
| Outdoor | 7(38.9) | 11(61.1) | 1 | 1 | ||
7 | Use of charcoal | |||||
| Yes | 102(38.8) | 161(61.2) | 3.69(2.63, 5.18)* | 3.55(2.36, 5.35) | <0> | |
| No | 85(14.7) | 495(85.3) | 1 | 1 | ||
8
| Presence of chimney | |||||
| Yes | 98(30.4) | 224(69.6) | 2.12(1.52, 2.95)* | 1.91(1.25, 2.91) | 0.003* | |
| No | 89(17.1) | 432(82.9) | 1 | 1 | ||
1 indicates reference category, * indicates, Significant association at p<=0.05 and ** indicates highly significant association at p< 0>
5.3.8.4.4 Multivariate analysis of nutritional and immunization related factors and the occurrence of pneumonia among under-five children
The result of the multivariate analysis revealed that being severely underweight child for its age, a child who did not take vitamin A in the last six month during data collection, a child who did not take any dose of vaccine for their age and children who did not receive measles vaccines were found to be the contributing factors for the occurrence of pneumonia in the study area.
Detailed analysis revealed that children who were severely underweight for their age were 2.43 times more likely to develop pneumonia than those with proportional weighed children (AOR: 2.43, 95%CI; 1.35, 4.37 p=0.003).
Children who did not receive vitamin A were 5.27 times more likely to develop pneumonia than those who received (AOR: 5.27; 95%CI: 3.41, 8.15; p<0 p=0.002);>
However using hand to fed the children was less likely to develop childhood pneumonia (AOR=0.22, 95%CI: 0.09, 0.55; p<0>
Table 5. 20: Multivariate analysis of nutritional and immunization related factors and the occurrence of pneumonia among under-five children in Sidama Regional State, Ethiopia: 2020 (N=843)
| No | Variables | Pneumonia status | COR of 95% CI | AOR of 95% CI | P-value | |
| Yes (n %) | No (n %) | |||||
| 1 | Nutritional status of children (weight for age) | |||||
| Normal | 130(20.5) | 505(79.5) | 1 | 1 | ||
| Under weight | 27(21.1) | 101(78.9) | 1.04(0.65, 1.66) | 1.06(0.62, 1.83) | 0.82 | |
| Severe under weight | 30(37.5) | 50(62.5) | 2.33(1.43, 3.81)* | 2.43(1.35, 4.37) | <0> | |
| 2 | Initiation of breast feeding | |||||
| Immediately at birth | 124(21.5) | 454(78.5) | 1 | 1 | ||
| Within one hour after birth | 37(23.3) | 122(76.7) | 1.11(0.69, 1.76) | 1.30(0.82, 2.11) | 0.29 | |
| Between first 1 and 24 hour | 17(20.0) | 68(80.0) | 0.86(0.46, 1.62) | 0.90(0.46, 1.75) | 0.75 | |
| After a day | 9(42.9) | 12(57.1) | 2.82(1.00, 7.97) | 2.35(0.82, 6.71) | 0.11 | |
| 3 | Received vitamin A last 6 month | |||||
| Yes | 68(12.5) | 477(87.5) | 1 | 1 | ||
| No | 111(45.3) | 134(54.7) | 5.81(4.06, 8.31)* | 5.27(3.41, 8.15) | <0> | |
| Not eligible | 8(15.1) | 45(84.9) | 1.25(0.56, 2.76) | 1.30(0.40, 4.22) | 0.67 | |
| 4 | Dewormed with in last 6 months | |||||
| Yes | 71(19.5) | 294(80.5) | 1 | 1 | ||
| No | 45(26.6) | 124(73.4) | 1.50(0.98, 2.31) | 0.67(0.39, 1.15) | 0.15 | |
| Not eligible | 71(23.0) | 238(77.0) | 1.23(0.85, 1.79) | 0.74(0.45, 1.21) | 0.23 | |
| 5 | Any vaccine and dose given | |||||
| Yes | 136(17.8) | 629(82.2) | 1 | 1 | ||
| No | 51(65.4) | 27(34.6) | 8.74(5.29, 14.43)* | 8.03(4.24, 15.22) | <0> | |
| 6 | Received measles vaccine | |||||
| Yes | 122(18.6) | 535(81.4) | 1 | 1 | ||
| No | 48(49.5) | 49(50.5) | 4.30(2.76, 6.70)* | 2.27(1.34, 3.86) | 0.002* | |
| Not eligible | 17(19.1) | 72(80.9) | 1.04(0.59, 1.82) | 0.70(0.30, 1.64) | 0.41 | |
| 7 | Materials used to fed the child | |||||
| Bottle | 51(37.5) | 85(62.5) | 1 | |||
| Cup | 25(26.0) | 71(74.0) | 0.59(0.33, 1.04)* | 0.52(0.27, 1.02) | 0.06 | |
| Spoon | 66(20.6) | 254(79.4) | 0.43(0.28, 0.67)* | 0.61(0.37, 1.02) | 0.06 | |
| Hand | 31(14.6) | 181(85.4) | 0.29(0.17, 0.49)* | 0.28(0.15, 0.55) | <0> | |
| Not eligible | 14(17.7) | 65(82.3) | 0.36(0.18, 0.70)* | 0.22(0.09, 0.55) | ||
1 indicates reference category, * indicates, Significant association at p<=0.05 and ** indicates highly significant association at p< 0>
5.3.9 Knowledge, attitude and practice of mothers/caregivers towards pneumonia prevention and control and associated factors with integration of qualitative finding
Knowledge, attitude and practice of mothers/ caregivers were assessed based on prepared questionnaires and analysed separately for each of the three variables for quantitative part of this study.
The qualitative part of the data were analysed manually with the support of Atlas ti software. A total of 40 mothers with under five children were participated in 6 different FGDs. Their age ranged from 24 to 42 years, with mean age 28.7 and the mode 30. The detail biblograph of FGDs preseted with the following table.
Table 5.21A: Biblograph of FGD participants in Sidama regional state, Ethiopia 2020
| List of FGDs | Age of participants (P) | Their district | Kebele | Remark |
| FGD 1 | P1=26, P2 36, P3 40, P4 34, P5 35, P6 30 & P7 31 | Dale | Soyama | |
| FGD2 | P1 38, P2 26, P3 28, P4 26, P5 31 P6 26 & P7 33 | Dale | Gane | |
| FGD3 | P1 32, P2 40, P3 29, P4 37, P5 30, P6 38 &P7 27 | Aleta wondo town | Mesalemia | |
| FGD4 | P1 40, P2 32, P3 39, P4 28, P5 34 & P6 30 | Aleta wondo town | Mesalemia cluster 2 | |
| FGD5 | P1 24, P2 41, P3 42, P4 38, P5 27, P6, 32 & P7 30 | Loka Abaya | Arada gale | |
| FGD6 | P1 40, P2 25, P3 37, P4 35, P5 29 & P6 30 | Loka Abaya | Chalbesa |
FGD: Focus group discussion, P: Participants
Three themes and six sub-themes were obtained from the analysis of qualitative data that was aligned with the proposed objectives (See table 21B below).
Table 5.21B: Themes and sub-themes identified from qualitative data analysis in Sidama regional state, Ethiopia 2020
|
The results of each sub-themes were used to support the findings of quantitative part of study, as discussed below.
The knowledge of mothers or caregivers related to identification of sign and symptoms, causes, mode of transmission and prevention of pneumonia was assessed. Results of descriptive analysis in this regard revealed that 634(75.2%) of mother/caregivers had heard of childhood pneumonia while about quarter 209(24.8%) of them did not know. Of those who had heard, almost half of respondents got the information from health extension workers and 146(17.3%) from older people or community leaders while 25(3%) and 13(1.5%) directly from health workers and TV/Radio respectively.
Table 5. 21C: Knowledge and source of information of mothers/caregivers about childhood pneumonia in Sidama Regional State, Ethiopia: 2020
| No | Characteristics | Frequency (n) | Percent (%) | |
1 | Heard childhood pneumonia (N=843) | Yes | 634 | 75.2 |
| No | 209 | 24.8 | ||
| Total | 843 | 100 | ||
2 |
Source of information (N=634) | Health extension workers | 450 | 53.4 |
| Health workers | 25 | 3.0 | ||
| TV/Radio | 13 | 1.5 | ||
| Older people/community leaders | 146 | 17.3 | ||
| Total | 834 | 100 | ||
The results from focus group discussions analysis also confirmed that most participants agreed that they had heard about pneumonia as common childhood disease and got the information from health extension workers and health professionals when they took their children to the health facilities for postnatal consultation.
A 26-year-old mother from Soyama kebele said that “Health professionals have informed me that my child had get pneumonia and I have to properly handle him. They also gave me a syrup to treat… it” (FGD1 participant).
Nine different questions about signs and symptoms of childhood pneumonia were asked and tried to assess knowledge of mothers/care givers. Majority of them 497(59.0%) knew that fever is one of the signs and symptoms of childhood pneumonia. Almost half of the respondents 412(48.9%), 443(52.6%), 444(52.6%), 432(51.2%) and 443(52.6%) responded that they are knowledgeable on chills, chest in-drawing, fast breathing and stridor for being signs and symptoms of pneumonia respectively.
Most of the FGD discussants mentioned that pneumonia may cause fast breathing, chills and sign of stridor among under-five children while they get pneumonia.
One 26-year-old mother from Gane kebele said “My child had fast breathing and sign of stridor [Afale udulinosi, sheengarsannosi], while he was diseased with pneumonia…” (FGD2 participant).
Another 32-year-old mother from A/wondo town reflected “Childhood pneumonia caused shortness of breathing and that my child became very weak with difficulty of breathing…” (FGD3 participant).
As the result revealed two third of mothers/caregivers 622(73.8%); knew cough as sign and symptom of pneumonia while 374(44.4%) and 323(38.2%) of them knew that weakness and loss of appetite as signs and symptoms of pneumonia respectively.
Majority of FGD participants argued that cough is typical sign and symptom of pneumonia among under-five children.
A 40-year-old woman from Aleta wondo town showed her feeling saying, “Cough is the most typical sign and symptom of pneumonia that children can show when they had diseased with it. Once up on time my child got pneumonia and was challenged with cough critically [mudde mudde buusiisinosi], till I took him to health facility…” (FGD4 participant.
Another 24-year-old mother from Arada Gale kebele believed “Children became weak [dalaganno] and unable to eat and drink when they got pneumonia…” (FGD5 participant).
However, except cough, almost half of the respondents did know that the other signs and symptoms of pneumonia properly as shown in table 5.22.
Table 5. 22: Knowledge of mothers/caregivers on sign and symptom of pneumonia in Sidama Regional State, Ethiopia: 2020
| No | Variables for assessing knowledge of respondents on sign and symptom of pneumonia | Right answer | Wrong answer | ||
| Frequency (n) | (%) | Frequency (n) | (%) | ||
| 1 | Knew that fever as sign and symptom of pneumonia | 497 | 59.0 | 346 | 41.0 |
| 2 | Knew that chills as sign and symptom of pneumonia | 412 | 48.9 | 431 | 51.1 |
| 3 | Knew that cough as sign and symptom of pneumonia | 622 | 73.8 | 221 | 26.2 |
| 4 | Knew that chest in drawing as sign and symptom of pneumonia | 443 | 52.6 | 400 | 47.4 |
| 5 | Knew that difficulty in breathing as sign and symptom of pneumonia | 444 | 52.7 | 399 | 47.3 |
| 6 | Knew that Stridor as sign and symptom of pneumonia | 443 | 52.6 | 400 | 47.4 |
| 7 | Knew that fast breathing as sign and symptom of pneumonia | 432 | 51.2 | 411 | 48.8 |
| 8 | Knew that weakness as sign and symptom of pneumonia | 374 | 44.4 | 469 | 55.6 |
| 9 | Knew that appetite loss as sign and symptom of pneumonia | 323 | 38.3 | 520 | 61.7 |
Table 5.23 presents the knowledge of mothers/caregivers on causes of childhood pneumonia. Three hundred eighty-eight of mothers/caregivers (46.0%) knew that bacteria are a cause of childhood pneumonia; while, 357(42.3%) and 223(26.5%) of them knew that dust or germs and virus respectively might be the causes of pneumonia.
However, from almost six (06) FGDs, none of the discussants showed that pneumonia can be caused by bacteria, virus or germs. Rather they perceived that childhood pneumonia can be caused by poor handling and the sudden clash of cold and hot temperature or due to weather change.This can be inferred from a 40-year-old mother from Chalbesa kebele who was quoted for saying: “Childhood pneumonia can be caused by poor handling practices of mothers, starting from the very beginning of birth; that means poor wearing practice, exposing the child to cold weather and poor hygienic practice…” (FGD6 participant).
Another 36-year-old mother from Soyama kebele perceived, “The childhood pneumonia can occur within the sudden interaction of hot and cold weather condition. When mothers did not dress their children and probably those exposing the chest of child to cold weather, the child may get pneumonia…” (FGD1 participant).
Surprisingly, 550(65.2%) and 137(16.3%) of the mothers/caregivers responded that childhood pneumonia might be caused by weather change and witchcraft respectively which was wrongly perceived.
One 38-year-old mother reacted, “Health professionals told me that I did not have to expose my child to cold weather and rather I have to keep doors properly closed. While I did not properly close the door and expose my child to cold weather, he could be diseased with pneumonia. I understood that the cause for pneumonia was interaction of hot and cold temperature…” (FGD2 participant).
But regarding witchcraft as cause of childhood pneumonia none of FGD participants confirmed it confidently.
Two different FGD participants (one 25-year-old and the other 34-year-old mothers) said, “The cause for childhood pneumonia cannot be witchcraft, rather it could be poor handling practice that community showed…” (FGD6 and FGD1 participants respectively).
Table 5. 23: Knowledge of mothers/caregivers on causes of pneumonia in Sidama Regional State, Ethiopia: 2020
| No | Variables for assessing knowledge of respondents on causes of pneumonia | Right answer | Wrong answer | ||
| Frequency (n) | (%) | Frequency (n) | (%) | ||
| 1 | Knew that dust/germs may cause pneumonia | 357 | 42.3 | 486 | 57.7 |
| 2 | Knew that bacteria may cause pneumonia | 388 | 46.0 | 455 | 54.0 |
| 3 | Knew that virus may cause pneumonia | 235 | 27.9 | 608 | 72.1 |
| 4 | Knew that fungi may cause pneumonia | 156 | 18.5 | 687 | 81.5 |
| 5 | Thought that weather change may cause pneumonia | 293 | 34.8 | 550 | 65.2 |
| 6 | Thought that witchcraft may cause pneumonia | 706 | 83.7 | 137 | 16.3 |
From the total of 843 interviewed mothers/caregivers 544(64.5%) knew that pneumonia can be transmitted through air droplet; while 234(27.8%) responded that pneumonia can be transmitted by personal contact.
The findings from qualitative part of study also revealed that childhood pneumonia can be transmitted through air droplet. A 40-year-old mother said, “Pneumonia can be transmitted via air droplet; hence it is the disease of interaction between cold and hot temperature…” (FGD1 participant). But another discussant aged 41 reflected, “Pneumonia can be transmitted from the older child to the smaller one; if there was the child or children who had experienced with history of being diseased with childhood pneumonia, it can be transmitted during coughing…” (FGD5 participant).
There was also an idea raised from discussants that pneumonia can be transmitted through poor personal hygiene of children which their mothers practiced. One 28-year-old mother said, “Pneumonia can be transmitted when mothers had not washed their child properly including their clothes.
Some mothers did not change the clothes for their children in timely manner and that dirty clothes may aggravate the transmission of childhood pneumonia…” (FGD2 participant).
Some discussants told the researcher that pneumonia can be transmitted by poor sanitation and poor feeding that parents practiced. One 32-year-old mother said that “Open defecation can contribute or the transmission of pneumonia among under-five children. If community defecate in open space, there might be flies those can facilitate the transmission of pneumonia. Additional pneumonia can be transmitted if children drink milk without boiling…” (FGD4 participant).
Table 5. 24: Knowledge of mothers/caregivers on transmission method of pneumonia in Sidama regional state, Ethiopia: 2020
| No | Variables for assessing knowledge of respondents on transmission method of pneumonia | Right answer | Wrong answer | ||
| Frequency (n) | (%) | Frequency (n) | (%) | ||
| 1 | Knew that pneumonia can be transmitted through air droplet | 544 | 64.5 | 299 | 35.5 |
| 2 | Knew that pneumonia can be transmitted through personal contact | 234 | 27.8 | 609 | 72.2 |
| 3 | Knew that pneumonia can be transmitted through dirty hands | 229 | 27.2 | 614 | 72.8 |
From the total of respondents only quarter of mothers/caregivers of this study were knowledgeable on most of the prevention methods of pneumonia. However, 573(68.0%) of them were able to identify that pneumonia can be prevented by vaccine.
As the findings obtained from FGDs discussion indicated, some of the discussants witnessed that childhood pneumonia can be prevented via immunization, even if they did not know that there is pneumococcal vaccine, most of them agreed that they have had their children immunized until nine months.
One 35-year-old mother said, “We have to immunize our children properly to prevent them from different diseases including childhood pneumonia. Some mothers may delay immunizing their kids and those children can be challenged with diseases...” (FGD1 participant).
Other discussants argued that breastfeeding can prevent pneumonia. Two different mothers (one 26 and another 31 both from FGD2) said, “Properly breastfeeding of the children may help families to protect their children from being pneumonia diseased and other diseases. So, we have to breastfeed our children continuously even if they are diseased…”
Majority of discussants from different FGDs raised that pneumonia can be prevented with proper clothing and they argued, “Pneumonia can be prevented with proper clothing of the child [Du’mu uduunichinni gagasosi seekkine funge amada hasiisanno/qiidu afirannosiki gede/] since from the time of delivery. If the children are exposed to the cold temperature pneumonia cab be occurred, but if we can wear them properly, we can prevent them from the suffering of the disease. Some mothers may expose their children with cold and hot temperature or vice versa, but this might harm their children. So, mothers should take care of their children to prevent them from pneumonia…” (FGD1, FGD2, FGD4, FGD5 & FGD6 participants).
There were also perceptions like childhood pneumonia can be prevented only through treatment after children getting it. Some of the discussants assumed that pneumonia can be continued and it can be controlled with on time treatment only.
One 42-year mother argued, “Pneumonia may happen suddenly within children and the parents should took them to health facility or purchase the syrup to treat them. Once my daughter got sick and I took her to health centre, and health professional told me that she had pneumonia and gave me a syrup for seven days with advising me that I have to administer it properly…” (FGD5 participant)
Table 5. 25: Knowledge of mothers/caregivers on prevention methods of childhood pneumonia in Sidama regional state, Ethiopia: 2020
| No | Variables for assessing knowledge of respondents on prevention method of pneumonia | Right answer | Wrong answer | ||
| Frequency (n) | Percentage (%) | Frequency (n) | Percentage (%) | ||
| 1 | Knew that pneumonia can be prevented through vaccine | 573 | 68.0 | 270 | 32.0 |
| 2 | Knew that pneumonia can be prevented through proper nutrition | 252 | 29.9 | 591 | 70.1 |
| 3 | Knew that pneumonia can be prevented through Exclusive breast feeding | 276 | 32.7 | 567 | 67.3 |
| 4 | Knew that pneumonia can be prevented through proper clothing within weather conditions | 303 | 35.9 | 540 | 64.1 |
| 5 | Knew that pneumonia can be prevented through proper house ventilation | 253 | 30.0 | 590 | 70.0 |
| 6 | Knew that pneumonia can be prevented through washing hands before feeding child | 225 | 26.7 | 618 | 73.3 |
A total of 25 questions were used to assess knowledge of mothers/caregivers in the current study. These include one (01) question about general information, nine (09) questions about signs and symptoms of pneumonia six (06) questions about causes of pneumonia and three (03) questions were about ways of transmission and the remaining six (06) questions were about prevention methods of pneumonia. Every correct response received a score of 1 and wrong response received a score of 0. The knowledge score ranged from 0 to 25 and rank as knowledge percentile into three levels namely poor knowledge <50>=75%.
The study results revealed that the respondents’ average knowledge score was 11.44 with standard deviation ± 4.27 and a range between 4 and 23. Majority of mothers/ caregivers 536(63.6%) had poor knowledge, 237(28.1%) had moderate/fair knowledge and 17(8.3%) of mothers/caregivers had good knowledge towards childhood pneumonia prevention and control as indicated in figurer 5.3.
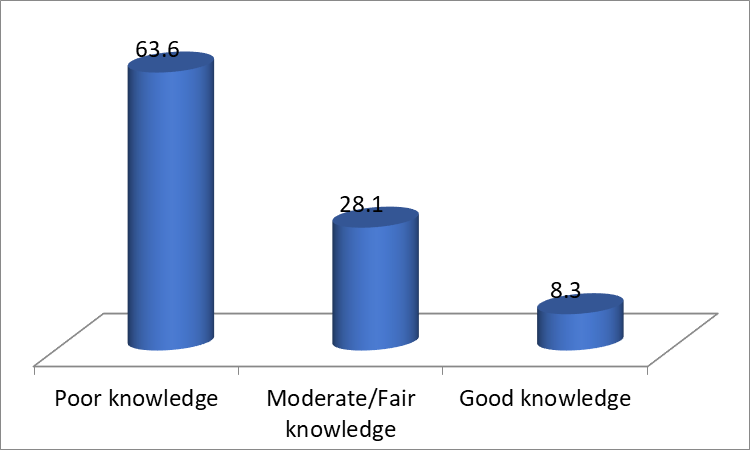
Figure 5. 3: Knowledge of mothers/caregivers towards childhood pneumonia prevention and control in Sidama Regional State, Ethiopia: 2020
Table 5.26 presented the attitude of mothers/care givers towards pneumonia prevention and control in Sidama Regional State. About 717(85.1%) of mothers/care givers agreed, 105(12.4%) disagreed and 21(2.5%) were indifferent that pneumonia can harm children. Similarly, 783 (92.8%) of respondents agreed that a child suffering from pneumonia should be taken immediately to a health facility, 42(5.0) disagreed and 18(2.1%) were indifferent. Regarding the mothers/care givers’ attitude towards pneumonia preventive methods, 726(86.1%) agreed reducing indoors smoke and dust may help to prevent pneumonia, 85(10.0%) of them disagreed and 32(5.3%) were indifferent.
The majority of FGD discussants reported that they have thought pneumonia as risky on the health of children. One 35-year-old mother said, “Pneumonia is highly dangerous which can disturb the health of our children badly. I never forget the history when my child had diseased with pneumonia while his father was far away from us and I had been through a lot of challenges. The child had become critical, he could not eat and even he could not breathe properly and become lethargic until I took him to health facility. So, I believe that pneumonia is the worst disease for children…” (FGD1 participant).
Majority of respondents showed negative attitude towards buying antibiotics from the shop without visiting health facilities. About 602(71.4%) of respondents reported that they did not like to buy drug from shop for their child without consulting health professionals or visiting health facility when they feel that their child showed sign and symptom of pneumonia.
The findings from the qualitative part of study also supports the above evidences. One 30-year-old mother said, “We have to take our children to health professionals or health facility if they showed any sign and symptom of disease. In the past, most of communities purchase the drug or medication from anywhere even from shop when they thought that their children seem sick of pneumonia as well as other health problems. But nowadays there is a good progress as community members no longer buy road side drugs or use drugs without consulting health professionals or visiting health facilities which is a good practice that I am also following…” (FGD3 participant).
Table 5. 26: Attitude of mothers/caregivers towards pneumonia prevention and control in Sidama Regional State, Ethiopia: 2020
| Characteristics | Strongly disagree | Disagree | Indifferent | Agree | Strongly agree |
| Attitude towards risk of pneumonia | 50(5.9) | 55(6.5) | 21(2.5) | 380(45.1) | 337(40.0) |
| Attitude towards taking pneumonia infected child to health facility immediately |
30(3.6) |
12(1.4) |
18(2.1) |
303(35.9) |
480(56.9) |
| Reducing indoor smoke and dust may help to prevent pneumonia |
40(4.7) |
45(5.3) |
32(3.8) |
436(51.7) |
290(34.4) |
| EBF and EPI may help to prevent pneumonia |
34(4.0) |
78(9.3) |
42(5.0) |
360(42.7) |
329(39.0) |
| Mothers can treat cough or common cold at home |
79(9.4) |
192(22.8) |
54(6.4) |
416(49.3) |
102(12.1) |
| Attitude towards getting antibiotics for child without visiting health facility |
238(28.2) |
364(43.2) |
36(4.3) |
130(15.4) |
75(8.9) |
| Traditional healers sometimes can treat pneumonia |
62(7.4) |
117(13.9) |
94(11.2) |
331(39.3) |
239(28.4) |
Another 7 questions were used to assess and evaluate the attitude of mothers/care givers towards pneumonia prevention and control in the current study area. The responses of those all 7 questions were labelled into 5 categories (strongly disagree, disagree, indifferent, agree and strongly agree). The questions were computed with SPSS version 25 and checked for its mean, standard deviation, minimum and maximum values. Then the attitude score was recoded into different variables and categorized into negative and positive attitude. Those whose attitude with mean value and below were categorized into negative attitude while whose attitude with more than mean value were grouped into positive attitude.
The mean attitude score value was obtained as 25.9% with SD 3.237 and 11 minimum and 35 maximum value scores. As the study finding showed the majority of respondents 521(61.8%) were with positive attitude and 322(38.2%) were with negative attitude.
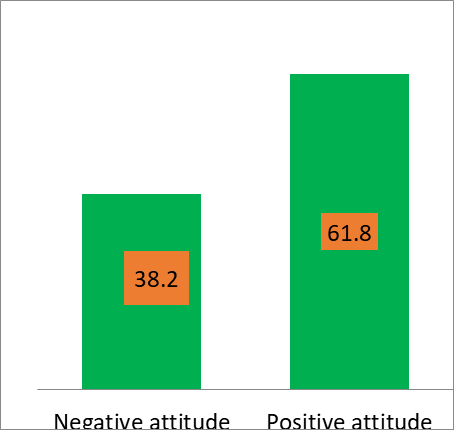
Figure 5. 4: Attitude of mothers/caregivers towards childhood pneumonia prevention and control in Sidama Regional State, Ethiopia: 2020
5.3.9.9 Practices of mothers/caregivers towards pneumonia prevention and control with integration of qualitative findings
The following table 5.26 presents respondents’ practices which were exercised to prevent and control children from pneumonia in Sidama Regional State. Majority of mothers/caregivers 683(81%) responded that they took their child to health facility when the child seems sick of pneumonia; while 160(19.0%) did not. Similarly, 656(77.8%) showed that they did not purchase the drug without consulting health professionals.
The discussion result showed that most of the FGD participants also supported the above findings. One 40 year old mother said, “I personally took my children to health facility while they seemed sick. I can witness that most of my neighbours also take their sick children to health facility early as much as possible...” (FGD3 participant).
Regarding breastfeeding practices, current findings revealed that only half of, (47.6%) mothers/caregivers agreed that they breastfed continuously even if their child was sick of pneumonia as compared to 442(52.4%) who did not do so.
From the qualitative findings of the current study, discussants raised their feeling differently of the above result. A 25-year-old mother reflected, “I personally do not agree with the idea of giving food or breastfeeding to a child sick of pneumonia. This is because I feel that the breast milk may suffocate the sick child. Due to this I do not support the idea that giving food for the children while they are ill…” (FGD2 participant).
About 523(62%) of mothers/caregivers responded that they have been practicing proper clothing for their children to manage childhood pneumonia during data collection. This was taken as that they have been practicing proper dressing based on weather conditions.
Most of the FGDs discussants’ findings also supported the above quantitative result positively. They argued that properly clothing of the child may help to reduce/manage/ childhood pneumonia. One 36-year-old mother said, “Childhood pneumonia can be managed by proper clothing of the children when they became sick. I believe that most of the pneumonia cases among under-five children could happen when their mothers did not follow the proper clothing approach, especially when there might be the interaction of hot and cold weather. So, to minimize or manage challenges such like this, it is better to dress children with right clothes according to the weather conditions…” (FGD1 participant).
Table 5. 27: Mothers’/caregivers’ practices towards prevention and control of childhood pneumonia in Sidama Regional State, Ethiopia: 2020, (N=843)
| No | Variables for assessing practice of respondents towards pneumonia prevention and control | Yes | No | ||
| Frequency (n) | (%) | Frequency (n) | (%) | ||
| 1 | Took child to the nearest health facility immediately when child seems sick of pneumonia | 683 | 81.0 | 160 | 19.0 |
| 2 | Took child to the traditional healers when child seems sick of pneumonia | 155 | 18.4 | 688 | 81.6 |
| 3 | Purchase drug from pharmacist without consulting health professional when child seems sick of pneumonia | 187
| 22.2
| 656
| 77.8
|
| 4 | Took child to the religious leaders when child seems sick of pneumonia | 214
| 25.4
| 629
| 74.6
|
| 5 | Purchase drug from any shop when child seems sick of pneumonia | 196
| 23.3
| 674 | 76.7 |
| 6 | Taking child to Health facility within 24 hours when child seems sick of pneumonia | 524 | 62.2 | 319 | 37.8 |
| 7 | Breast fed continuously when child seems sick of pneumonia | 401 | 47.6 | 442 | 52.4 |
| 8 | Vaccinating the children to prevent pneumonia | 732 | 86.8 | 111 | 13.2 |
| 9 | Using ventilation to prevent pneumonia | 494 | 58.6 | 349 | 41.4 |
| 10 | *Proper clothing the child to manage pneumonia when seems sick of pneumonia | 523 | 62.0 | 320 | 38.0 |
*Proper clothing= wearing children as per their body temperature and weather conditions
5.3.9.10 Overall level practice of mothers/caregivers towards childhood pneumonia prevention and control
There were ten different questions used to evaluate and check the practice of mothers/care givers towards pneumonia prevention and control whether it was proper or improper practice. The response of each individual was labelled as “0” and “1” where “0” for improper practice and “1” for proper practice.
The responses were computed with SPSS version 25 and checked for its mean. The value of respondents practice level below mean practice score value were categorized as improper practice and those practice level was equal to mean score value and those above were categorized as proper practice.
The findings indicated that mean practice score value was 7.1 with minimum and maximum value of 0 and 10 respectively. About 486(57.5%) of mothers/caregivers had practiced the childhood pneumonia prevention and control ways properly while 358(42.5%) showed improper practice.

Figure 5. 5: Practice of mothers/caregivers towards childhood pneumonia prevention and control in Sidama Regional State, Ethiopia: 2020 (N=843)
To assess the associated factors with the level of KAP of mothers/caregivers, the three-level category of knowledge was recoded into dichotomous namely adequate and inadequate knowledge from which below mean score value was inadequate while equal and above mean value labelled as adequate knowledge. For attitude and practice the variables already dichotomized (positive and negative attitude; and proper and improper practice) towards childhood pneumonia prevention and control.
Both bivariate and multivariate analysis were conducted with the socio-demographic and economic characteristics and level of KAP of mothers to identify the contributing factors.
5.3.9.11.1 Factors associated with knowledge of mothers/caregivers towards childhood pneumonia prevention and control
Table 5.28 presents factors associated with level of knowledge of mother/caregivers on pneumonia prevention and control at the current study area. At the bivariate analysis, 12 variables were investigated for association and variables with their p-value <0>
The presence of a functional radio was found as one of the positively associated factors for having adequate knowledge among mothers/caregivers at the current study area (AOR: 1.28; CI, 0.94, 1.75; p=0.047). In addition, the increased level of educational status of child’s father was found to be significant contributing factor for having adequate knowledge among mothers/care givers (AOR=1.88; CI: 0.86, 4.08; p=0.005). Mothers who had two children also found to be positively associated factor with having adequate knowledge among mothers/caregivers (AOR=1.86; CI: 1.20, 2.89; p=0.005).
Table 5. 28: Socio-demographic and economic factors associated with knowledge of mothers/caregivers towards pneumonia prevention and control in Sidama Regional State: 2020, (N=843)
| No | Characteristics | Status of knowledge | COR of 95%CI | AOR of 95%CI | P-value | |
| Adequate | Inadequate | |||||
| 1 | Number of children mothers had | |||||
| One | 74(37.9) | 121(62.1) | 1 | 1 | ||
| Two | 95(44.2) | 120(55.8) | 1.29(0.87, 1.92) | 1.41(0.93, 2.14) | 0.10 | |
| Three | 92(51.4) | 87(48.6) | 1.73(1.14, 2.61)* | 1.86(1.20, 2.89) | 0.005** | |
| Four | 49(38.6) | 78(61.4) | 1.03(0.65, 1.63) | 1.13(0.70, 1.84) | 0.64 | |
| Five and above | 49(38.6) | 78(61.4) | 1.03(0.65, 1.63) | 1.20(0.74, 1.95) | 0.45 | |
| 2 | Place of delivery | |||||
| Health Institution | 281(44.9) | 345(55.1) | 1.45(1.05, 1.99)* | 1.34(0.96, 1.88) | 0.90 | |
| Home | 78(35.9) | 139(64.1) | 1 | 1 | ||
| 3 | Presence of TV | |||||
| Yes | 79(52.7) | 71(47.3) | 1.64(1.15, 2.34)* | 1.11(0.74, 1.66) | 0.61 | |
| No | 280(40.4) | 413(59.6) | 1 | 1 | ||
| 4 | Presence of radio | |||||
| Yes | 157(49.2) | 162(50.8) | 1.54(1.17, 2.05)* | 1.28(0.94, 1.75) | 0.047** | |
| No | 202(38.5) | 322(61.5) | 1 | 1 | ||
| 5 | Educational level of child’s father | |||||
| Illiterate/no formal education | 37(34.6) | 70(65.4) | 1 | 1 | ||
| 1-8 grade | 189(38.7) | 300(61.3) | 1.19(0.77, 1.85) | 1.08(0.69, 1.71) | 0.73 | |
| 9-12 grade | 88(50.0) | 88(50.0) | 1.89(1.15, 3.11)* | 1.64(0.97, 2.79) | 0.07 | |
| Certificate and above | 37(62.7) | 22(37.3) | 3.18(1.64, 6.16)* | 1.88(0.86, 4.08) | 0.005** | |
| 6 | Educational level of respondents | |||||
| Illiterate/no formal education | 74(39.8) | 112(60.2) | 1 | 1 | ||
| 1-8 grade | 211(40.4) | 311(59.6) | 1.03(0.73, 1.44) | 0.93(0.65, 1.34) | 0.71 | |
| 9-12 grade | 44(46.8) | 50(53.2) | 1.33(0.81, 2.20) | 0.99(0.57, 1.75) | 0.99 | |
| Certificate and above | 30(73.2) | 11(26.8) | 4.13(1.95, 8.74) | 2.11(0.86, 5.18) | 0.10 | |
1 indicates reference category, * indicates, Significant association at p<=0.25 on bivariate analysis and ** indicates significant association at p< 0>
5.3.9.11.2 Factors associated with attitude of mothers/caregivers towards childhood pneumonia prevention and control
Different factors were considered and checked through both bivariate and multivariate analysis to identify weather there was significant association within the positive or negative attitude of mothers/care givers towards childhood pneumonia prevention and control at the study area.
Ten socio-demographic and economic variables were included in the bivariate analysis to investigate the influence on the attitude of mothers/caregivers towards childhood pneumonia prevention and control at the study area. Six variables were found as candidate variables for multivariate analysis with a p-value of <0>
Mothers/caregivers who had adequate knowledge towards childhood pneumonia prevention and control were significantly associated with positive attitude of mothers/caregivers towards the prevention and control of pneumonia (AOR: 0.64; 95%CI: 0.48, 0.86; p=0.003). Furthermore, mothers/caregivers age older than or equal to 36 years had positive attitude than the other age groups (AOR=0.64; CI: 0.48, 0.86; p=0.003). Lastly, having five and more children was positively associated with mothers/care-givers’ positive attitude towards pneumonia prevention and control with p-value 0.01 and (AOR=1.96; CI: 1.15, 3.35) as indicated in table 5.29.
Table 5. 29: Factors associated with attitude of mothers/caregivers towards pneumonia prevention and control in Sidama Regional State: 2020, (N=843)
| No | Characteristics | Attitude status | COR of 95%CI | AOR of 95%CI | P-value | |
| Positive | Negative | |||||
| 1 | Knowledge status of respondents | |||||
| Adequate | 279(57.6) | 205(42.4) | 0.66(0.49, 0.87)* | 0.64(0.48, 0.86) | 0.003** | |
| Inadequate | 242(67.4) | 117(32.6) | 1 | 1 | ||
| 2 | Age of respondents | |||||
| 16-24 | 125(61.9) | 77(38.1) | 1 | 1 | ||
| 25-35 | 325(64.0) | 183(36.0) | 1.09(0.78, 1.53) | 1.07(0.74, 1.52) | 0.71 | |
| >=36 | 71(53.4) | 62(46.6) | 0.71(0.45, 1.10)* | 0.51(0.30, 0.87) | 0.01** | |
| 3 | Number of children mothers had | |||||
| One | 119(61.0) | 76(39.0) | 1 | 1 | ||
| Two | 129(60.0) | 86(40.0) | 0.96(0.64, 1.42) | 0.94(0.62, 1.42) | 0.78 | |
| Three | 106(59.2) | 73(40.8) | 0.93(0.61, 1.40) | 0.94(0.60, 1.46) | 0.97 | |
| Four | 80(63.0) | 47(37.0) | 1.10(0.69, 1.72) | 1.27(0.77, 2.08) | 0.34 | |
| Five and above | 87(68.5) | 40(31.5) | 1.40(0.87, 2.23)* | 1.96(1.15, 3.35) | 0.01** | |
| 4 | Job of respondent | |||||
| Housewife | 364(60.2) | 241(39.8) | 1 | 1 | ||
| Government employer | 44(59.5) | 30(40.5) | 0.97(0.5, 1.59) | 0.94(0.53, 1.66) | 0.83 | |
| Merchant | 66(71.7) | 26(28.3) | 1.68(1.04, 2.72)* | 1.62(0.98, 2.66) | 0.06 | |
| Daily labourer | 7(63.6) | 4(36.4) | 1.16(0.34, 4.00) | 1.32(0.36,4.81) | 0.68 | |
| Farmer | 40(65.6) | 21(34.4) | 1.26(0.73, 2.19) | 1.39(0.78, 2.47) | 0.26 | |
5 | Educational level of respondent | |||||
| Illiterate | 113(60.8) | 73(39.2) | 1 | 1 | ||
| 1-8 grade | 313(60.0) | 209(40.0) | 0.97(0.69, 1.36) | 0.86(0.60, 1.23) | 0.42 | |
| 9-12 grade | 69(73.4) | 25(26.6) | 1.78(1.04, 3.07)* | 1.50(0.84, 2.66) | 0.17 | |
| Certificate and above | 26(63.4) | 15(36.6) | 1.12(0.56, 2.26)* | 0.95(0.42, 2.13) | 0.90 | |
1 indicates reference category, * indicates, Significant association at p<=0.25 on bivariate analysis and ** indicates significant association at p< 0>
5.3.9.11.3 Factors associated with the practice of mothers/caregivers towards childhood pneumonia prevention and control
From multivariate analysis four variables (knowledge of mothers/care givers, age of respondents, and presence of radio and educational level of respondents) were obtained as significantly associated factors with practice of mothers/caregivers towards pneumonia prevention and control in study area.
Mothers/caregivers with fair knowledge showed proper practice towards pneumonia prevention and control (AOR=1.56; 95%CI: 1.12, 2.17; p=0.008). Also the presence of functional radio (AOR=1.53; 95%CI: 1.11, 2.11; p=0.009) and mothers/caregivers between the age group of 25-35 years (AOR=1.52; 95%CI: 1.08, 2.16; p=0.02) were positively associated factors with the proper practice of mothers/caregivers to prevent and control pneumonia among under-five children respectively. Similarly, mothers/caregivers with both primary (AOR=1.72; 95%CI: 1.20, 2.48; p=0.004) and secondary educational level (AOR=3.01; 95%CI: 1.70, 5.34; p=0.001) were found to show more proper practice towards childhood pneumonia prevention and control than the rest with different level of education (see table 5.30).
Table 5. 30: Factors associated with practice of mothers/caregivers towards pneumonia prevention and control in Sidama Regional State: 2020, (N=843)
| No | Characteristics | Practice status | COR of 95%CI | AOR of 95%CI | P-value ≤0.05 | |
| Proper | Improper | |||||
| 1 | Wealth index | |||||
| Poorest | 75(48.1) | 81(51.9) | 1 | 1 | ||
| Poor | 102(57.6) | 75(42.4) | 1.47(0.95, 2.26)* | 0.52(0.32, 0.82) | 0.06 | |
| Middle | 107(61.8) | 66(38.2) | 1.75(1.23, 2.72)* | 0.91(0.58, 1.43) | 0.68 | |
| Rich | 104(61.9) | 64(38.1) | 1.75(1.23, 2.73) | 1.03(0.65, 1.62) | 0.91 | |
| Richest | 97(57.4) | 72(42.6) | 1.45(0.94, 2.25) | 0.96(0.60, 1.51) | 0.85 | |
| 2 | Knowledge status of respondents | |||||
| Poor | 286(54.4) | 250(46.6) | 1 | 1 | ||
| Fair | 155(65.4) | 82(34.6) | 1.65(1.20, 2.27)* | 1.56(1.12, 2.17) | 0.008** | |
| Good | 44(62.9) | 26(37.1) | 1.48, 0.88, 2.47) | 1.45(0.84, 2.50) | 0.18 | |
| 3 | Age of respondents | |||||
| 16-24 | 105(52.0) | 97(48.0) | 1 | 1 | ||
| 25-35 | 310(61.0) | 198(39.0) | 1.45(1.04, 2.01)* | 1.52(1.08, 2.16) | 0.02** | |
| >=36 | 70(52.6) | 63(47.4) | 1.03(0.66, 1.59) | 1.53(0.84, 2.18) | 0.21 | |
| 4 | Presence of radio | |||||
| Yes | 210(65.8) | 109(34.2) | 1.74(1.31, 2.35)* | 1.53(1.11, 2.11) | 0.009** | |
| No | 275(52.5) | 249(47.5) | 1 | |||
| 5 | Marital status of respondents | |||||
| Single | 8(42.1) | 11(57.9) | 1 | 1 | ||
| Married | 467(58.3) | 334(41.7) | 1.92(0.76, 4.83)* | 2.00(0.77, 5.22) | 0.15 | |
| Widowed | 10(43.5) | 13(56.5) | 1.06(0.31, 3.61) | 1.16(0.32, 4.26) | 0.82 | |
| 6 | Educational level of respondents | |||||
| Illiterate/no formal education | 84(45.2) | 102(54.8) | 1 | 1 | ||
| 1-8 grade | 306(58.6) | 216(41.4) | 1.72(1.23, 2.41)* | 1.72(1.20, 2.48) | 0.004** | |
| 9-12 grade | 67(71.3) | 27(28.7) | 3.01(1.77, 5.13)* | 3.01(1.70, 5.34) | 0.001** | |
| Certificate and above | 28(68.3) | 13(31.7) | 2.61(1.27, 5.36) | 1.93(0.88, 4.22) | 0.10 | |
1 indicates reference category, * indicates, Significant association at p<=0.25 on bivariate analysis and ** indicates significant association at p< 0>
5.4 CONCLUSSIONS
This chapter presented the result of the study following the research objectives. The prevalence of childhood pneumonia in the current study was reported and the associated factors namely: socio-demographic and economic, behavioural and disease related, environmental and nutritional and immunization related were also clearly justified and presented. This chapter also presented with level of knowledge, attitude and practice of mothers/caregivers towards childhood pneumonia prevention and control and also its associated factors.
The next chapter will present with discussion of result.
This chapter presents the discussion of the study results linked with the stated study objectives. The research findings are also discussed in relation to different previous studies conducted on similar topics or concepts.
Findings were discussed under sub topics of prevalence of childhood pneumonia, different categories of associated factors of pneumonia, level of knowledge, attitude and practice of mothers with aged under five children towards childhood pneumonia and factors associated with KAP of mothers/caregivers towards childhood pneumonia prevention and control were discussed here.
6.2 PREVALENCE OF CHILDHOOD PNEUMONIA AND ASSOCIATED FACTORS
6.2.1 Prevalence of pneumonia among under five children in Sidama Regional State
Understanding the burden and associated factors of childhood pneumonia is important for the management and development of proper prevention strategies. The result of current study indicates that the prevalence of pneumonia among children aged under-five years in study area is 22.2%. The prevalence of the current study is higher than that of conveyed from the studies carriedout in northwest Ethiopia and Ghana which were 16.1% and 18.40% respectively (Osei 2018:1 & Fekadu et al 2014:150). However, the result of current study is lower than the results obtained from the studies conducted in southern and southwest Ethiopia which were 33.5% and 28.1% respectively (Lema 2018:25 and Abuka 2017:19). This difference might be due to study setting, periodic variations and the difference of implementation of health extension program especially on child health management. Most of the above listed studies whose values are higher than the value of current study were conducted at facility base and this might also makes the difference.
6.2.2 The association between socio-demographic and economic factors and the occurrence of childhood pneumoni
Different socio-demographic and economic factors like medium and large family size, respondents with no formal education, the middle age group of children (7-36 months) and less than or 2 years of birth interval of children were found as associated factors for the occurrence of childhood pneumonia in the current study area. The educational level of mothers/caregivers significantly influenced the occurrence of pneumonia (p=0.002). This implies that children who had mothers/caregivers with no level of education were likely to suffer from Pneumonia. The same results were reported from studies done in Vietnam and India that showed the low literacy level of mothers were significantly associated with the occurrence of pneumonia (Hoang 2019:277 & Gupta 2019:951).
Current findings revealed that having medium and large family size were found to be significantly associated with the occurrence of under-five pneumonia with p-values less than 0.001. This implies children who lived in households with large family sizes were more likely to suffer from pneumonia than their counterpart in small family sizes. These findings are in line with findings obtained from a study carriedout in southeast Nigeria which revealed that children with large family size can develop pneumonia than the others (Ujunwa and Ezeonu 2014:95). These might be due to the overcrowding; hence overcrowding is suitable means for the transmission of communicable diseases. For instance, a study conducted in Bellary and India showed that overcrowding was found to significantly influence the occurrences of childhood pneumonia (Srivastava et al 2015:1 & Hemagiri et al 2014:47).
Findings showed that age of children can also contribute to the occurrence of childhood pneumonia. Children with age group 7-12 and 13-36 months were found for being significantly associated with childhood pneumonia occurrence (p=0.001). That implies children who were in the age group of 7-36 months were more likely to suffer from pneumonia than the most lower and upper age groups of children. Similar findings were obtained from the study conducted in Ethiopia which showed that children in the age group of 2-12 months were found to be determinant factor for the occurrence of pneumonia. Also, the same findings were obtained from a study conducted in Rwanda which revealed that children in the age of 0-11 months and 24-59 months being found as negatively associated with the occurrence of pneumonia. On the contrary, the risk of suffering from pneumonia reduced among children aged 2-11 and 12-23 months in urban areas of Ethiopia (Abuka 2017:19, Harerimana et al 2016:1 and Dadi et al 2014:1). These differences might be due to the environmental exposure of children with age and the degree of the care that mother/caregiver offer to their children. Younger children have the opportunity of always being carried by the mothers/caregivers. Hence, they have not started walking. Being constantly with/on mothers/caregivers’ carriage may prevent them from the exposure to move on their own, and that might contribute to the occurrence of any illness including childhood pneumonia.
The study findings revealed that birth interval of children which is less than two years was found as contributing factor of childhood pneumonia (p=0.02). This implies that children whose birth interval is less than 2 years from their older ones were likely to suffer from pneumonia. This might be due to that children who had less than 2 years birth interval may lack proper care from their mothers/caregivers for they could be busy.
6.2.3 The association between behavioural and history of disease related factors and the occurrence of childhood pneumonia
From multivariate analysis, different behavioural and history of disease related factors were found to be meaningfully associated with the occurrence of childhood pneumonia in the current study area. Presence of family members with history of respiratory disease was found as one of the associated factors for the occurrence of pneumonia with (p<0>
Children having any disease history during data collection period were also obtained to be significantly associated with the prevalence of pneumonia among under-five children (p=0.03). That is to mean children who were with any other illness during the time of data collection were more likely to suffer from pneumonia than those to the contrary. These results are supported with previous results obtained from research done in different parts of Ethiopia, which showed that children with the history of diarrhea were at higher likelihoods of developing pneumonia compared to those who did not (Markos et al 2019:1 and Dadi et al 2014:1). This might be due to that children suffering from any disease can be immune compromised and susceptible for any other infections including pneumonia.
The study findings reported that children with the history of measles disease in the previous year preceding to data collection were found to be contributing factors of childhood pneumonia (p<0>
6.2.4 The association between environmental factors and the occurrence of childhood pneumonia
Five different environmental factors namely; households with no latrine, not having separate house for animal and human, absence of window in the living house, charcoal use and presence of chimney during the time of data collection were found to be positively associated factors with the occurrence of childhood pneumonia in the current study area. Children who lived in a household that did not have separate shelter for animal and human being were at a higher degree of suffering from pneumonia (p=0.001). Current findings concur with results obtained from a study carriedout in northwest Ethiopia which shown that keeping cattle inside the main house was associated with childhood pneumonia (Fekadu et al 2014:150). This might be due to poor sanitation which then can create suitable transmission opportunity for the pneumonia causative agents and children could be easily affected with pneumonias a result.
Results from multivariate analysis revealed that the use of charcoal as the main source of energy in the household significantly influenced the prevalence of childhood pneumonia in the current study area (p<0>
Absence of window in the living house was another positively associated factor with the occurrence of childhood pneumonia in the current study (p<0>
Household without latrine was also found as significantly associated factor of childhood pneumonia (p<0>
Presence of chimney inside the house during data collection was also found as the significantly associated factors of pneumonia among under-five children (p=0.003) in Sidama Regional State. Children who lived with the house where there was chimney were more likely to develop pneumonia than those who did not reside in a household where there was no chimney. Similar result was obtained from the study conducted in Ethiopia, which revealed that children leaving in a household with a chimney were found to increase the odds of childhood pneumonia (Mesafint et al. 2020:9).
6.2.5 The association between nutritional and immunization related factors and the occurrence of childhood pneumonia
Findings in the current study showed that nutritional as well as immunization related factors were also found to be major contributing factors of childhood pneumonia in the current study area. Severely underweight was one of the positively associated factors with pneumonia in under-five children (p=0.003). Malnutrition can weaken the body’s disease fighting ability by affecting the immunity. Hence the severely malnourished children are the vulnerable group for any diseases. These results, are aligned with the results obtained from India, Gambia and Ethiopia, and showed that malnutrition was one of the determinants of childhood pneumonia (Lema et al 2018:25, Howie et al 2016:1405 and Srivastava et al 2015:1). In addition, a literature review study carriedout in Pakistan also showed that malnutrition was a major factor of childhood pneumonia (Aftab et al 2016:1, Ramezani 2015:1173 and Hemagiri et al 2014:47).
Lack of immunization was also found to positively influence the occurrence of childhood pneumonia. Children who, did not get measles vaccine were more likely to develop pneumonia than those who were vaccinated, according to the current findings (p=0.002). Immunization is a way of preventing the infectious disease thus children who are not immunized are at risk of being infected. It is known that immunization can prevent different diseases in children including pneumonia. These findings align with results from studies conducted both in Ethiopia and Pakistan which revealed that lack of vaccination was one of the major risk factors of pneumonia (Lema et al 2018:25 and Aftab et al 2016:1). Similarly, incomplete immunization per one’s age was also significant risk factor for pneumonia among under-five children in India (Gupta and Bhadrala 2019:949, Srivastava et al 2015:1 and Hemagiri et al 2014:47).
A statistically significant association exists between lack of vitamin A supplementation and the occurrence of childhood pneumonia (p<0>
However, feeding child with hand was obtained as one of the negatively associated factors with the occurrence of pneumonia (p<0>
6.2.6 Level of knowledge, attitude and practice of mothers/caregivers towards pneumonia prevention and control
Current findings indicated that majority of respondents (63.6%) had overall poor knowledge while 28.1% had fair and only 8.3% had good knowledge towards pneumonia prevention and control. This indicates that the majority of mother/caregivers lack basic knowledge about pneumonia prevention and control where having such knowledge is one of the fundamentals that must be presented to build a positive health. These findings coincide with previous findings conducted in Nigeria and Bangladesh which revealed mothers for having poor knowledge on the severity of childhood pneumonia (Pradhan et al 2016:35 & Ferdous et al 2014:1). On the contrary, findings from studies conducted in India reported that 41.3% of mothers had fair knowledge (Yahaya et al 2018:35). This difference might be due to study setting, way of implementing health education program and it might be also socio-economic status variations within each study area.
In the current study, the majority of mothers/caregivers (61.8%) had positive attitude compared to 38.2% of mother/caregivers who had negative attitude towards childhood pneumonia prevention and control as such they feel better to prevent and control pneumonia among under five children. The current findings are higher than that of research findings obtained from the studies conducted in Saudi Arabia and India which reported that more than half of the mothers had poor attitude towards childhood pneumonia prevention and control (Alluqmani et al 2017:1959 & Pradhan et al 2016:35). The difference might be attributed to the level of understanding of the severity of childhood pneumonia and rate of exposure to pneumonia among the mothers/caregivers.
The current study revealed that more than half of the mothers/caregivers (57.5%) reported that they practice measures of prevention and control of pneumonia. Contrarily, research findings obtained from a study conducted in Saudi Arabia revealed that practice of mothers towards ARI including pneumonia was poor (Alluqmani et al 2017:1959). In addition, results from a cross sectional survey conducted in Pakistan reported that 58% of mothers practiced self-medication (Bham et al 2016:1557), which is an improper practice. This might be due to the difference among mothers/caregivers’ perception towards health seeking behaviour and understanding of benefits of visiting health facility or consulting health professionals.
6.2.7 The association of factors with knowledge of mothers/caregivers towards pneumonia prevention and control
The current study analysis indicated the determinants of adequate knowledge towards pneumonia prevention and control in under five children. Mothers/caregivers who owned a functional radio had better knowledge than those who did not possess one (p=0.05). This implies households with functional radio could easily access information related to child health including pneumonia. The presence of a radio in households might also indicate a higher economic status or wealth index of the family and positively correlate with the knowledge of mothers/caregivers. These findings coincide with results obtained from India which reported that maternal socioeconomic status have an important role in knowledge towards respiratory disease (Mutalik and Raje 2017:29).
Respondents’ level of education was significantly associated with maternal/caregivers’ adequate knowledge of childhood pneumonia prevention and control measures. Increased level of education was positively associated with having knowledge on pneumonia prevention and control among under five children (p=0.005). This might be due to the fact that mothers with better literacy can understand issues than those who did not have formal education. Similar findings were found from a cross‑sectional study done in India and showed the increased level of mothers’ education; and this was significantly associated with the increased knowledge of childhood pneumonia among mothers (Pradhan et al 2016:36). Furthermore, studies conducted in Pakistan and Saudi Arabia revealed that having better literacy or high educational level to be positively associated with good knowledge towards pneumonia in under five children (Alluqmani et al 2017:1959 & Bhamet al 2016:1557).
Number of children mothers had also was found to be significantly associated with adequate knowledge in current study area. Mothers who had two children (p=0.005) were obtained to be associated with adequate knowledge. Mothers/caregivers who had two children were likely to have adequate knowledge than the others. This might be due to the fact that as number of children increases, there might be increasing experience for mothers also; and this may support them to understand or acquire knowledge about childhood pneumonia. The current findings are consistent with those of Keter (2015:34) that reported mothers in Kenya with more than three children were more likely to have knowledge of pneumonia.
6.2.8 The association of factors with attitude of mothers/caregivers towards pneumonia prevention and control
From the current study, majority of mothers/caregivers showed positive attitude towards pneumonia prevention and control among under five children. Adequate knowledge of respondents about pneumonia was found to have a significant association with having positive attitude towards childhood pneumonia prevention and control (p=0.003). Mothers/caregivers who had adequate knowledge were more likely to have positive attitude than their counterparts. These findings are also aligned with the results of a cross sectional study carriedout in India that revealed the existence of substantial association between the level of knowledge and insight of mothers on childhood pneumonia (Pradhan et al 2016:35). The reason might be the difference in understanding of childhood pneumonia. Mothers who are knowledgeable about childhood pneumonia may think more positively than those who did not recognise the severity of pneumonia among under five children of theirs.
The older age of respondents was found to be negatively associated with the attitude towards pneumonia prevention and control in under five children. Mothers/caregivers of aged >=36 years were less likely to have positive attitude towards pneumonia prevention and control than the younger ones (p=0.01). Similarly, findings obtained from a study conducted in Saudi Arabia showed that better thoughtful and adequate knowledge was significantly associated with young ages (Alluqmani et al 2017:1959). The reason might be that younger mothers/caregivers may have better literacy and understanding than the older age groups of respondents and this may lead them to have positive attitude.
Having five and above children was also found to be another factor for the contribution of mothers/caregivers to have positive attitude towards pneumonia prevention and control. Mothers/caregivers with >=5 children have positive attitude (p=0.01). The proper justification for this might be that mothers/caregivers may have positive attitude as their experience increases as the number of their children increases.
6.2.9 The association of factors with practice of mothers/caregivers towards pneumonia prevention and control
The current study results indicate that majority of mothers/caregivers had proper practice towards childhood pneumonia prevention and control at the study area. Mothers/caregivers with fair knowledge had proper practice than those who did not (p=0.01). The result of a cross sectional study carriedout in Kenya showed that mothers who had better knowledge showed good practice (Keter 2015:51). The reason might be that pre information or being knowledgeable about childhood pneumonia may support to do the right thing regarding pneumonia prevention and control.
The study result showed that mothers/caregivers living in households with a functional radio had positive practice towards the prevention and control of pneumonia (p=0.01). This implies that respondents who had functional radio had proper practices than those who did not have the devise. The reason might be that household with radio may get information timely and that may support them to practice positively.
Current findings revealed that mothers/caregivers with 1-8 grade (p=0.004) and 9-12 grade level of education (p=0.001) had better practice towards pneumonia prevention and control. Mothers/caregivers who grew on their education further had good practice than those with lower education. Similar studies conducted in India, Pakistan and Nigeria showed that better education of mothers/caregivers can influence them positively to practice pneumonia prevention and control measures effectively (Mutalik and Raje 2017:29, Bham et al 2016:1557 and INdu et al 2015:1). This might be due to the fact that educated mothers/caregivers can understand the severity of childhood pneumonia in detail and may take positive actions towards pneumonia prevention and control measures.
6.3 CONCLUSSION
This chapter presented the discussion of results of the current study. The chapter commenced through the introduction and study findings in the current study area which included the prevalence of childhood pneumonia and its socio-demographic, economic, environmental, behavioural, disease, nutritional and immunization related factors. Additionally, it presented the level of knowledge, attitude and practice of mothers/caregivers towards childhood pneumonia prevention and control and its association with the socio-demographic factors. The chapter also included the utilization of different available and valued research findings that are used for the comparison of the current study findings following with the scientific reference using approach.
The next chapter will present the conclusions, recommendations and limitations.
This chapter presents key findings, conclusions based on the study findings, major contributions and its limitations. Furthermore the chapter presents the recommendations, issues for further research and concluding remarks.
7.2 SUMMARY AND INTERPRETATION OF THE RESEARCH FINDINGS
The purpose of the study was to develop awareness and prevention strategies on pneumonia among under-five years’ children in Sidama regional state, Ethiopia in line with the strategy to accelerate the goal of ending preventable pneumonia disease by 2025, through assessing the prevalence of childhood pneumonia and associated factors, and also assessing knowledge, attitude and practice of mothers/caregivers towards childhood pneumonia prevention and control and its associated factors. The study addressed issues to develop awareness and prevention strategies aligned with the integrated Global Action Plan for Pneumonia (GAPP).
The data were collected from 843 respondents at household level for the quantitative part of the study making the response rate of 99.8%; and six (06) FGDs were conducted with a total of 40 mothers of under-five children for qualitative part as well.
The quantitative data were analysed using descriptive and analytic statistics; while the qualitative data analysis followed a process of data reduction, presentation, and conclusion drawing. The original records in Sidaamu Afoo were transcribed verbatim into English language by the researcher from the tape-recorded interviews, field-notes and then the researcher organised the data thematically. Both qualitative and quantitative data were analysed concurrently.
7.2.1 Socio-demographic and economic characteristics of respondents
Majority of respondents were mothers of the children, formally married and living together with their husbands or wives. The vast majority of respondents belonged to Sidama ethnicity and were Protestants religion followers.
Almost a quarter of respondents did not have formal education or could not read and write. Whereas, the rest of respondents had different level of education. The majority of respondents were between 25-35 years of age and had an average small family size (≤5 members).
7.2.2 Socio- demographic characteristics of child
The age of surveyed children ranged from 1 to 59 months with the mean age of 28.85 months (Standard deviation ±15.83). Most children were delivered at health facilities, more than one-quarter of them were the first child of the family and most children had two years and above birth interval.
7.2.3 Prevalence of pneumonia among under-five children
The current findings reported that the prevalence of pneumonia among under-five children in Sidama Regional State is 22.2%.
7.2.4 Key factors associated with the occurrence of pneumonia among under-five children
7.2.4.1 Findings related to socio-demographic and economic factors and association with the occurrence of childhood pneumonia
According to these findings increased family size, lower level of maternal education, middle age of children (7-36 months) and below two years of birth interval were the socio-demographic and economic factors that influenced the occurrence of childhood pneumonia at the current study area.
7.2.4.2 Findings related to behavioural and disease related history of households and the occurrence of pneumonia among under-five children
Findings from multivariate analysis of the current study indicated that children who had a history of any disease during data collection were more likely to develop pneumonia than those who did not. Similarly, those children who had history of measles disease for the past one year before data collection were more likely to develop pneumonia than those without the history of measles.
Additionally, children whose family members had a history of respiratory disease were more likely to develop pneumonia than those who did not.
7.2.4.3 Findings related to environmental factors and occurrence of pneumonia among under-five children
Multivariate analysis shows that absence of household latrine, window, and separate house for animal and human being, presence of chimney in the house during data collection period and use of charcoal were environmental factors that contributed for the occurrence of childhood pneumonia in the current study area.
The study result showed that children from family without latrine were more likely to develop pneumonia than those who lived in a house with latrine. Also, absence of separate house for animals and human being; and living in households without window, presence of chimney in house and use of charcoal as the main source of fuel for cooking were significantly associated with the occurrence of pneumonia among under-five children than the cases where the reverse is true.
7.2.4.4 Findings related to nutritional and immunization related factors and occurrence of pneumonia among under-five children
The current result showed that children who were severely underweight for their age were more likely develop pneumonia than their counterparts who weigh normal considering their age. Similarly, children who were with lack of vitamin A and did not receive the required vaccines including measles preceding to data collection were likely to developed pneumonia than their counterparts who received vitamin A supplementation and vaccines required for their age. Contrary of this children who were fed with hands were less likely to develop pneumonia than those bottles were used to feeding.
7.2.5 Knowledge, attitude and practice of mothers/caregivers towards childhood pneumonia prevention and control
The current study findings reported that majority of mothers/caregivers had poor knowledge but had positive attitude and showed proper practice regarding childhood pneumonia prevention and control.
7.2.6 Factors associated with knowledge, attitude and practice of mothers/caregivers towards pneumonia prevention and control
7.2.6.1 Factors associated with knowledge of mothers/caregivers towards pneumonia prevention and control among under five children
The finding showed that mothers/caregivers from households with a functional radio were more knowledgeable about childhood pneumonia prevention and control than those who did not have. Mothers/caregivers from households who had two children were knowledgeable than the others. Similarly, mothers/caregivers with better level of education had more adequate knowledge than their counterparts towards pneumonia prevention and control in under five children.
7.2.6.2 Factors associated with attitude of mothers/caregivers towards pneumonia prevention and control among under five children
The current study findings showed that mothers/caregivers with adequate knowledge and who had five and above children had positive attitude towards childhood pneumonia prevention and control than the other groups. However older age group of respondents were fund to show less positive attitude than younger age groups.
7.2.6.3 Factors associated with practice of mothers/caregivers towards pneumonia prevention and control among under five children
From the present study mothers/caregivers with fair knowledge towards pneumonia prevention and control among under five children showed proper practice than the others. Similarly, respondents’ age and educational level were found to be positively associated with proper practice towards pneumonia prevention and control in under five children. Likewise, mothers/caregivers who had a functional radio in the household were positively associated with proper practice on childhood pneumonia prevention and control measures.
7.3 CONCLUSIONS
The present study was designed to develop evidence based awareness and prevention strategies on pneumonia among under five children in Sidama Regional State in line with the goal of ending pneumonia by 2025. The conceptual framework for this study was developed based on health belief model and global pneumonia prevention and control framework. A high prevalence of childhood pneumonia was obtained in a current study that pointed the need for the implementation of good strategy to curb further increase in the prevalence. The study also identified relevant socio-demographic and economic factors, behavioural and disease history related factors, environmental factors, nutritional and immunization related factors associated with the occurrence of childhood pneumonia. Gaps related to the knowledge, attitude and practice of mothers/caregivers towards pneumonia prevention and control and its associated factors were reported.
7.4 RECOMMENDATIONS
Based on the study findings obtained, the following recommendations are proposed to each of the responsible bodies in different levels.
7.4.1 Recommendations for woreda health offices, health centers and health posts
As part of the governmental administrative structures, these levels (administrative Institutes) are taken as the implementers of any health programs because they are closer to the community. Besides, these institutions, integrated with concerned partners/stakeholders, are expected to identify and address gaps seen in the community regarding study objectives.
Due to this the following recommendations are made: -
As health bureau is principal owner and monitoring institution of health system implementation at mid-level; the following recommendations are proposed: -
The work of health sector can be effective if partners work collaboratively and in supportive fashion with each other.
Considering this, the following recommendations are proposed for all responsible government as well as non-government health organizations: -
Different policies and programs including implementing strategies and guidelines of health programs have been designed and developed under the Ministry of Health Ethiopia. Considering this the following recommendations are proposed: -
The succeeding recommendations are proposed for future researchers: -
The current study contributes additional supportive evidences for the body of knowledge (BOK) in the area of study. The study establishes the prevalence of childhood pneumonia and its associated factors in Sidama Regional State. The study also contributes the findings on level of knowledge, attitude and practice of mothers/caregivers and associated factors towards pneumonia prevention and control among under-five children in the current study area.
Based on findings and reviewed literature, an awareness and prevention strategies on pneumonia among under five children was developed. The developed awareness and prevention strategies will thus be used by policy developers, program designers, health program implementers and scientific researchers in the field as references and guiding principles.
As the current study was conducted at community level, the findings may help to develop and follow the community base implementing strategy approach which will also help to bring the required change within a limited time; and it will also help to strengthen community participation and involvement in core decision making process on the issue of their own health.
7.6 LIMITATIONS OF THE STUDY
Basically the current research used community based cross-sectional study design for quantitative part integrated with FGD for qualitative part. Furthermore, Delphi method was applied to collect comments and opinions of experts on development of proposed awareness and prevention strategies on pneumonia among under five children. Hence it may share the limitations of any cross-sectional and Delphi methods studies.
There might be calibration error while anthropometric measurements are taken to assess nutritional status of children.
7.7 CONCLUDING REMARKS
The chapter presents a summary of the major findings of the study, conclusions and recommendations drawn as well as the limitations of the study. The subsequent chapter will present the proposed awareness and prevention strategies on childhood pneumonia in Sidama Regional State.
DEVELOPMENT OF AWARENESS AND PREVENTION STRATEGIES ON PNEUMONIA AMONG UNDER-FIVE CHILDREN IN SIDAMA REGIONAL STATE
8.1 INTRODUCTION
This chapter presents the proposed awareness and prevention strategies on childhood pneumonia in Sidama regional state, Ethiopia in line with the strategy to end preventable pneumonia disease by 2025. The chapter further details the major components of the strategies those are guiding principles of the strategies, validation mechanism, purpose and objectives of the strategies, scope of the strategies and basis for the the strategies development. The chapter also discusses the integration of the findings with the theoretical foundation, methodology, implementation strategies, monitoring and evaluation and strategies dissemination plan.
8.2 GUIDING PRINCIPLES OF THE STRATEGIES
The following guiding principles were used for the development of the proposed awareness and prevention strategies.
The developed awareness and prevention strategies were sent to different potential experts on the area of child health and to experienced university lecturers; as well as to health leaders who have been working in different governmental or non-governmental institutions. All panelists gave their comments and feedbacks based on prepared form. This was made to ensure the feasibility, acceptability and practicability of the proposed strategies in their implementation and to check their scientific integrity.
8.4 PURPOSE AND OBJECTIVES OF THE STRATEGIES
8.4.1 Purpose of the strategies
These awareness and prevention strategies aimed to help policy and programme planners and health care leaders as well as implementers to formulate intervention measures to tackle illnesses and deaths of children due to pneumonia in Sidama Regional State.
8.4.2 Objective of the strategies
The objective of the strategies is to develop and validate awareness and prevention strategies on childhood pneumonia in order to support the implementation of ending preventable pneumonia deaths and illness at local as well as national levels.
8.5 SCOPE OF THE STRATEGIES
These strategies are intended to be used at the study area. However, they can provide some common policy issues of child health programs to fight childhood pneumonia with implications for both national and other regional states. The Federal Ministry of Health (FMOH), Regional Health Bureaus, different level health facilities, governmental and non-governmental organizations can also use these strategies for they have been proposed for implementation based on relevant and available evidences and expertise’ opinions.
8.6 BASIS FOR THE DEVELOPMENT OFTHE STRATEGIES
The current study findings and reviewed relevant literatures were used used as the initial basis for the development of these awareness and prevention strategies.
Additional the conceptual framework and Delphi method were also used to develop the current awareness and prevention strategies on pneumonia among under-five children in the study area. Thus the proposed strategies were formulated based on the literatures reviewed to find the existing baseline evidence as discussed in chapter 2 of the current study, and linked to the current research findings. Furthermore, the integrated Health Belief Model (HBM) and global action plan of pneumonia prevention and control framework (GAPP) as discussed in chapter 3 of this study provided the structure for the strategies; and the Delphi method was used to strengthen the proposed strategies.
8.6.1 Delphi method
The Delphi method was also used to develop and strengthen the awareness and prevention strategies. Delphi survey is a technique for obtaining inputs(comments or suggestions) from a panel of experts about specific issue of concern; experts were consulted individually in two rounds via e-mail with a summary of the panelists’ views distributed to attain agreement, (Polit 2018:546). Experts included and consulted for the development of these proposed strategies were university lecturers, health leaders and professionals. The panelists were selected from different working institutions and diverse disciplines; and were believed for acquiring a wide range of experience and exposures in the area of study. The participants in the panel were knowledgeable on the area and helped for the decision reached and conclusions made thereafter.
Two rounds of Delphi panelist’s comments and suggestions were collected from experts and the collected data were analyzed based on their importance. The following diagrammatic presentation shows the two rounds of communications and activities conducted with the Delphi panelists.
Delphi panellists.
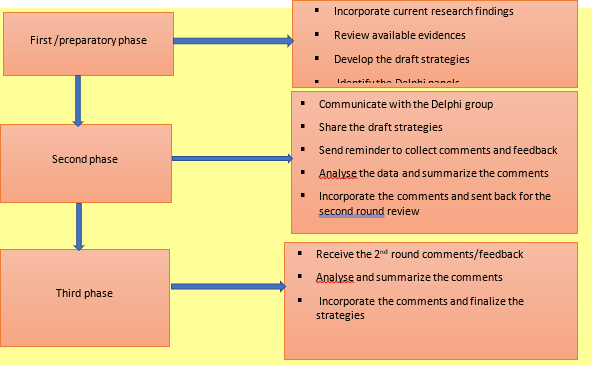
Figure 8. 1: Diagrammatic presentation of Delphi group data collection and analysi
8.7 INTEGRATION OF THE FINDINGS WITH THE THEORETICAL FOUNDATION
The conceptual framework of the current study was developed based on the integration of HBM and global action plan of pneumonia prevention and control (GAPP) framework. The common components of Health Belief Model like, individual’s perceptions, modifying factors and benefits of taking the preventive measures were considered. Under each elements of HBM; the three components of GAPP framework (protective, preventive and treatment) were also addressed to develop the new conceptual framework which is more integrative and helpful for the development of awareness and prevention strategies on childhood pneumonia in Sidama Regional State, Ethiopia.
8.7.1 Individual’s perceptions
From the current study, knowledge and attitude of mothers/caregivers towards pneumonia prevention and control among under-five children were obtained as the individual’s perceptions that can influence level of disease prevention and control in the community. Most of the current study respondents had poor knowledge towards pneumonia prevention and control measures. Regarding their attitude, majority of them believed that childhood pneumonia is a dangerous disease even though they had poor knowledge on the how of the prevention and control of it.
It is known that if mothers/caregivers are knowledgeable about the causes, mode of transmission, preventive measures and management of pneumonia among under-five children, they can keep their children safe from the disease or may seek medical assistances on time.
8.7.2 Modifying factors
The modifying factors under the current study include socio-demographic and economic factors; environmental and nutritional factors of childhood pneumonia; and also factors like behavioral and knowledge of mothers/caregivers towards childhood pneumonia prevention and control. From the present study, different findings were obtained as the contributing factors of under-five pneumonia that can be categorized under modifying factors.
Having medium and large family size, respondents without formal education, age of surveyed children, two and less than two years’ of birth interval between children and number of children mothers have, absence of household latrine, living with animal(s) in the household, absence of window in the living house, using charcoal as source of fuel, children with severe under-weight, lack of any immunization, feeding with a bottle and lack of vitamin A supplementation were among the contributing factors of childhood pneumonia under this category.
8.7.3 Benefits of taking the preventive measures
Perceived benefits (attitude) and taking the proper measures towards childhood pneumonia prevention and control were considered under the category of the benefits of taking the preventive measures. From the current study majority of respondents showed positive attitude towards pneumonia prevention and control; but the gap was seen on properly practicing those prevention and control mechanisms. Behavioral and health status of household members were addressed; and findings were also obtained. Having history of respiratory disease among family members, the child’s past measles disease history and the child’s current disease history during data collection period were found to be the associated factors for the occurrence of childhood pneumonia.
8.8 AWARENESS AND PREVENTION STRATEGIES ON PNEUMONIA AMONG UNDER-FIVE CHILDREN IN SIDAMA REGIONAL STATE
Table 8.1: Summary of major findings of the research in Sidama Regional State, Ethiopia: 2020
| No | Areas of gap addressed | Major findings obtained |
| 1 | Pneumonia prevalence among under-five children |
|
| 2 | Socio-demographic and economic determinants of childhood pneumonia |
|
| 3 | Behavioral and health status related factors associated with childhood pneumonia |
|
| 4 | Environmental factors contributing the occurrence of childhood pneumonia |
|
| 5 | Nutritional and immunization related contributing factors of childhood pneumonia |
|
| 6 | Knowledge of mothers/caregivers towards pneumonia prevention and control |
|
| 7 | Factors associated with knowledge of mothers/caregivers towards pneumonia prevention and control |
|
| 8 | Attitude of mothers/caregivers towards pneumonia prevention and control |
|
| 9 | Factors associated with attitude of mothers/caregivers towards pneumonia prevention and control |
|
| 10 | Practice of mothers/caregivers towards pneumonia prevention and control |
|
| 11 | Factors associated with practice of mothers/caregivers towards pneumonia prevention and control |
|
These awareness and prevention strategies were developed primarily from the current study findings and the reviewed existing national policies, guidelines and strategies. Then strengthened by inputs from Delphi group analysis and aligning with ending preventable pneumonia death by 2025. The researcher believed that the strategies will help as baseline reference for related policy makers and programme planners, governmental and non-governmental implementers with due consideration of other available options to improve child health, preventing morbidity and mortality of children caused due to childhood pneumonia. These strategies were basically organized into seven categories and each of them further includes different focus areas as listed here below:
Increasing knowledge, attitudes and practices of mothers or caregivers towards pneumonia prevention and control in Sidama Regional State should be taken as vital and that needs continuous and effective health communication and promotion work. Communication is the method of distributing the information, ideas, knowledge and experience among individuals or groups by using different communication channels; whereas health promotion can be taken as it is a combination of educational and environmental supports for interventions and situations of living in a suitable environment for health (Meseret and Yihenew 2004:5).
Health promotion is concerned with improving health through seeking improved lifestyles, health services and environments which are not merely restricted to the physical environment but includes cultural and socioeconomic status that substantially determine health conditions. The effective health promotion can be done through community mobilization, health education, advocacy and social marketing, (WHO 2012:15). Update and/or develop IEC/BCC materials and related tools to promote use of high impact MNCH services as per the national health communication material development and implementation guidelines. Community empowerment and demand creation can be done through conducting regular home to home visits to deliver continous counseling on high influence about reproductive health, maternal-newborn and child survival interventions and care as needed through strengthening 1-to-5 HDA network by training network leaders on key MNCH behaviors and practices for awareness creation to support issues related to maternal newborn and child survival, conduct regular mass media activities (FMOH 2015:46).
8.8.1.1.1 Community mobilization
Community mobilization involves convincing the community members to attend or engaged in any activity arranged by health educator to improve awareness on a specific issue at the public level (Sharma and Romas 2012:32). As research findings obtained from the current study indicate, community should be mobilized and guided to be aware of childhood pneumonia prevention and control mechanisms. Health sector integrated with partners can select the suitable approaches and arrange the community mobilization to improve the knowledge of mothers/caregivers those with children under-five age in Sidama Regional State towards pneumonia prevention and control.
For community mobilization activities like organizing a talk in the community, arranging a health fair and bringing together key community leaders for a panel discussion can be used, (Sharma and Romas2012:32). And also it would be useful to follow the local base realistic approaches to screen the participants for the mobilization at the study area.
8.8.1.1.2 Health education
To enhance awareness of community in Sidama Regional State on childhood pneumonia prevention and control strategies, proper health education should be designed and given. Majority of the study respondents had poor knowledge towards the causes and prevention methods of under-five pneumonia. This requires special attention to improve. Health education is a communication of activities aimed with enhancing good health and through averting or reducing of ill-health among individuals and groups by influencing the beliefs, attitudes and behavior of those with influence and of the community at large (Sharma and Romas 2012:18).
According to WHO, health education is not restricted to the distribution of only health-related information, rather it is also an activity to influence the motivation, skills and confidence that necessary to take an action to improve health, as well as the communication of information about the underlying social, economic and environmental conditions those impacting on health. Likewise health education is essential to communicate about the individual risk factors and behaviors to use the health care system (WHO 2012:13). The researcher proposed that health sector and the respected responsible bodies have to provide effective health education to the community in Sidama Regional State utilizing the proper health education materials and approaches considering cultural issues and norms.
8.8.1.1.3 Advocacy
Advocacy has been planned and considered under the current childhood pneumonia awareness and prevention strategies to assure it as prospect. Advocacy can be the communication strategies especially focusing on policy makers and planners, community and opinion leaders to be engaged and attain commitment and support. Moreover it helps for the higher-level commitment and participation in fulfilling a set program agenda, (Meseret and Yihenew 2004:6). Advocacy in health is about shifting a public opinion and mobilizing essential resources to support any issue or policy that affects the health of a community (Sharma and Romas 2012:242). Global and national advocacy campaigns are needed to improve the investments those help to end preventable child pneumonia deaths by 2030 through increasing awareness among all stakeholders about mortality of child due to pneumonia (Every Breath Counts 2017:2).
8.8.1.1.4 Social marketing
Social marketing is the use of marketable marketing techniques to help in attaining of a behavior that is advantageous for the health of a target population (Sharma and Romas 2012:250). It is proposed that social marketing is one of the vital concepts to be used to increase the awareness of community towards childhood pneumonia prevention and control mechanisms.
8.8.1.2 Strategy two: Protecting children from being diseased from pneumonia through adequate nutrition
Protecting children from childhood pneumonia by creating and promoting a good health practices is one of the key areas of pneumonia prevention and control proposed under the strategy of GAPP, (WHO and UNICEF 2013:7). The responsible bodies should work on critical services that may support the community to protect their children from pneumonia. The GAPPD identified that it is possible to protect children from pneumonia by establishing and sustaining a good health practices since starting from birth and by taking proper actions on activities like exclusive beast feeding for the first 6 months, providing adequate complementary feeding and timely supplementation of vitamin A (WHO and UNICEF 2013:6). The researcher identified that lack of vitamin A supplementation can contribute for the occurrence of childhood pneumonia. According to Farhad and Taheren (2014:57), vitamin A deficiency was one of the significantly associated factors with severe childhood infections.
In addition severe malnutrition was also found to be among the associated factors with childhood pneumonia in the current study area. It is known that poor knowledge and practices on food security and complimentary feeding, as well as exclusive breastfeeding can cause the children to be malnourished. A long term regulation and balance of energy in life can be attained through critical periods of life development and basically through the age of intrauterine life, infancy and childhood. For the prevention of malnutrition it is important to promote a healthy and balanced diet from early childhood (WHO 2016:2). Adequate and balanced nutrition during infancy and early childhood is one of the essential for the growth, health and development of children with their full potential. In contrary poor nutrition or malnutrition can agravate the risk of illness and could be responsible, for the mortality of children in many areas directly or indirectly (WHO 2009:3).
Community should have access for information on the different nutritional factors and timely supplementation of vitamin A; these could influence the occurrence of childhood pneumonia in the study area.
8.8.1.3 Strategy three: Preventing children from being diseased by pneumonia through timely immunization and healthy environment
The integrated global action plan for the prevention and control of pneumonia (GAPP) proposed that it is possible to prevent childhood pneumonia through ensuring world-wide coverage of immunization, HIV prevention and by availing healthy environments (WHO 2009:4). Result of the current study also showed that lack of immunization, absence of latrine, lack of separate house for animals and human being, absence of windows, presence of chimney in the house during the time of data collection, using charcoal as main source of fuel and presence of disease history among children as well as family member contributed for the occurrence of pneumonia among under five children. Community should be sensitized on the benefit of timely vaccination of their children, good housing conditions, safe use of fuel and proper health care seeking for family members when they show any sign and symptom of respiratory diseases. The later action should also be taken if a child is sick of any illnesses- including measles.
The Global Vaccine Action Plan (GVAP), recommended by the World Health Organization meeting in 2012, calls for delivery of vaccines as part of the package of interventions for diseases control including childhood pneumonia (WHO and UNICEF 2013:12). Health sector should ensure the accessibility of vaccine for the eligible children along with effective vaccine management.
The GAPP proposed that reducing indoor air pollution and proper sanitation and hygiene can protect the children from pneumonia (WHO and UNICEF 2009:4). It was reported that minimizing household air pollution through uzing improved stoves can reduce severe childhood pneumonia (WHO and UNICEF 2013:14). Evidence from the previous study conducted by Gedefaw, Mamo and Getahun (2014:150) showed that the use of charcoal as main source of fuel, mothers carrying a child on back during cooking, rearing of cattle inside the main house and living in crowded house were the factors those significantly contribute the occurrence of childhood pneumonia.
Healthy housing conditions, proper hygiene and sanitation are essential for maintaining good health of a community. Poor housing conditions can expose people for several risks factors of health including indoor air pollution that may cause respiratory problems, crowded housing which rises the risk of exposure to communicable diseases; and insufficient water supply and sanitation facilities that affect food safety and personal hygiene (WHO 2018:2-4).
Community can exercise good health for their own as well as for their children if they have been empowered and familiarized with the preventable challenges of childhood pneumonia. The current awareness and prevention strategies can substansially support in ways that they can be familiarized with the issues of good housing conditions, proper hygiene and sanitation, safe fuel utilization and timely initiation of childhood immunization. 8.8.1.4 Strategy four: Treating children who become ill with pneumonia
Enhancing the community awareness creation approaches may help for timely health seeking and treating of sick child with pneumonia. The current study findings reported that 42.5% of study respondents showed poor practice towards childhood pneumonia prevention and control including timely treating of the sick child. One of the focus areas of GAPP is the treatment of children who are ill from pneumonia with proper treatment. Increased access to proper care, through community based case management of pneumonia, can reduce 35% mortality in children, (WHO & UNICEF 2013:13-15). World Health Organization has recommended that case management is one of the critical pillar strategies of childhood pneumonia control. It involves classifying the severity of disease by using clinical signs and symptoms like fast breathing, chest in-drawing and presence of general danger signs. Likewise it also guides the professionals to apply appropriate treatment which could be home care advice, antibiotics for home therapy and or referral to a higher-level health facility (WHO 2014:4).
8.8.1.5 Strategy five: Improving the utilization of maternal and child health services
Quality and skill care for woman and newborn during and after delivery like all-inclusive family planning and integrating care for HIV/AIDS (PMTCT), malaria and others were among services that can contribute to the prevention and control of pneumonia, (WHO & UNICEF 2013:12). From the current study, findings showed that having large family size, birth interval of less than two years and age of children between 7-36 months were found to be significantly contributing to the occurrence of childhood pneumonia in Sidama Regional State. The accessing and utilizing of maternal health services within the right time has been proposed and community should be sensitized about the integration and utilization of maternal health services and its contribution on the decrease of childhood pneumonia disease and death.
Provision of modern contraceptives to all woman who want to avoid pregnancy; and continuum of care through adolescence, pregnancy, childbirth, postnatal and newborn periods and into childhood based on WHO standards can support to achieve the goal of improving child health. Delivering good quality of care at child birth, timely immunization, initiation of breastfeeding and proper nutrition can help to improve child health (Every woman Every Child 2015:19; FMOH 2015:5-6).

Figure 8. 2: Continuum of care approach: time of care giving and place and approach of care giving (FMOH 2015:36).
8.8.1.6 Strategy six: Engaging multi-sector partnership to facilitate and contribute pneumonia prevention and control
Engaging and involving different partners and sectors can galvanize support to put pneumonia under control. Areas of partnership can be overall child health and nutrition in societies and the wider communicable disease control, ensuring clean air, safe water supply, sanitation and hygiene, and development of financing communities. The possible engaged partners can be governmental, private sectors and non-governmental organization (Save the Children, UNICEF and Every Breath Counts 2019:7-8).
The Ethiopian health care delivery system is enhanced by the rapid growth of private-for- profit and NGOs sector that have been playing crucial role in expanding the health service coverage and utilization. To catalyze the envolvement of the private sector in health service delivery and increase partnership between the public and private sectors, the FMOH launched the public private partnership (PPP) strategy and supposed to bring significant change (FMOH 2015:18).
Health sector in Sidama Regional State should collaborate with woman, child and youth, education and agriculture sectors to create awareness and exchange experiences. The current study found out that being mothers/caregivers with no formal education to be one of the factors that contribute to childhood pneumonia in Sidama Regional State. These new strategies advise that both inter and intra sector collaboration can help for the proper and timely combat of childhood pneumonia.
8.8.1.7 Strategy seven: Strengthening health system to deliver strong health care in order to combat pneumonia
Health system consists of those organizations, products, manpower and actions whose primary aim is to promote, restore and/or maintain health. The progress towards universal health coverage and improve the quality of primary health care services need the expansion of the coverage of quality and essential health services with an emphasis reducing unfairness and strengthening health care facilities. Likewise the strong and impartial health systems are needed to effectively prevent, diagnose and treat pneumonia and deliver children with their fundamental human right with good-quality healthcare (Save the children, UNICEF & Every Breath Counts 2019:3, FMOH 2015:17-8).
Health systems can be strengthened through improving one or more of the functions of the health systems that leads to access better health service coverage with improved quality and or efficiency (USAID & Abt associate 2015:4). World health organization proposed six possible building blocks to strengthen the health systems. These are ensuring good leadership and governance, good health service delivery, a well performing and competant health workforce, a well-functioning health information system, equitable access to essential medical products, vaccines, technologies and a good health financing, (Anwer 2017:21-3 and WHO 2007:3).
Within the strengthened health systems, neonatal and prenatal mortality can be lowered through availing improved health services and training of health workers. Similarly, under-five mortality can also be decreased by empowering the communities and provide engagement through strengthening of health services in communities, (USAID & Abt associate 2015: ix-x).

Figure 8. 3: The WHO health system framework/the six building blocks of health system (WHO 2007:3).
8.9 CONCEPTUAL FRAMEWORK FOR AWARENESS AND PREVENTION STRATEGIES OF CHILDHOOD PNEUMONIA
The conceptual framework has been developed for the implementation of proposed awareness and prevention strategies of pneumonia among under-five children in Sidama Regional State aligning with GAPP framework and also by using current study findings and the existing relevant literatures that are also aligned with the currently proposed strategies.
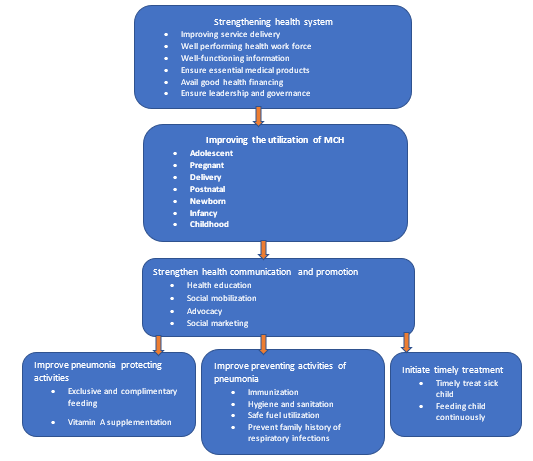
Figure 8. 4: Conceptual framework developed for implementation of proposed awareness and prevention strategies on childhood pneumonia in Sidama Regional State: 2020
8.9 PRIORITY AREAS FOR ACTION
The results of the current study indicated that there are some areas of interventions that can support on the effort of pneumonia prevention and control. The selected priority areas are summarized as below in table 8.2.
Table 8.2: Priority areas of action of awareness creation and prevention strategies on pneumonia prevention and control in Sidama Regional State: 2020
| Ser. No | Areas of action | Purpose | Activities | Outcome |
| 1 | Addressing determinant factors of childhood pneumonia | Creating awareness and empowering the community |
| Increased use and implementation of maternal, neonatal and child health services which might indirectly improve child health |
| 2 | Improve the KAP of mothers/ caregivers towards childhood pneumonia prevention and control | Increasing the level of KAP among mothers/ caregivers towards in the community towards pneumonia prevention and control |
| Improved level of KAP among mothers/ caregivers towards in the community towards pneumonia prevention and control |
| 3 | Improve health seeking behavior in the community | Prevent and treat possible health outcomes |
| Increased awareness and practice of community towards early health seeking |
| 4 | Nutritional intervention to child | Prevent malnutrition and improve child health |
| Well-nourished children with enabled disease preventing immunity |
| 5 | Hygiene and sanitation practice | Improve hygiene and sanitation |
| Improved hygiene and sanitation practice in the community and supported to prevent disease |
| 6 | Demand creation and community participation | Improve community participation on the decision of health issue |
| Demand created in the community with improved participation on the health issues |
| 7 | Health system strengthen | Improve health service delivery |
| Improved health service delivery to all community |
| 8 | Demand creation and capacity building of health staffs | Improve capacity of health work force |
| Improved capacity building within health workforce |
8.10 MONITORING AND EVALUATION
The progressive efforts to prevent and control childhood pneumonia need integrated attention. World Health Organization recommends that countries should have primary responsibility for ensuring that data are available and used for action, and for measuring progress (WHO and UNICEF 2013:31).
Only having strategies may not bring the needed changes in awareness creation and prevention for childhood pneumonia. Rather it is essential to establish and availe the monitoring and evaluation systems in place. Current strategies also proposed that putting a strong monitoring and evaluation system in place will be the cornerstone for the success of planned strategies. Monitoring and evaluation is taken as the foundation for national health sector strategic planning as it covers all major disease programs and health systems activities. Thus, the following leading GAPP indicators are adapted and modified to be used to monitor and evaluate the improvement of awareness and prevention strategies on childhood pneumonia. (WHO and UNICEF 2013:32-3 & WHO 2009:6&10).
Table 8.3: Indicators to evaluate progress in achieving key operational targets for awareness and prevention strategies on childhood pneumonia
| Indicators | Definitions | Interventions category |
| Immunization coverage/fully immunized | Percentage of 12-23 months children who received all doses of vaccines | Prevent |
| Measles immunization coverage | Percentage of 12-23 months children immunized with measles | Prevent |
| Penta3 immunization coverage | Percentage of 12-23 months children who received 3 doses of pentavalent vaccines | Prevent |
| PCV10 immunization coverage | Percentage of 12-23 months children who received 3 doses of PCV10 | Prevent |
| Exclusive breast feeding for 6 months | Percentage of 0-5 months infants who are exclusively breastfed | Protect |
| Continued breast feeding at 1 year | Proportion of 12–15 months children who fed breast milk | Treat |
| Complementary feeding | Percentage of 6-23 months children who received a minimum acceptable diet | Protect |
| Vitamin A supplementation coverage | Percentage of 6 -59 months children who received vitamin A 2 annual doses | Protect |
| Care seeking for pneumonia | Percentage of 0-59 months children with suspected pneumonia taken to an appropriate health provider | Treat |
| Antibiotic treatment for pneumonia | Percentage of 0-59 months children with suspected pneumonia receiving appropriate antibiotics | Treat |
| Hand washing with soap | Percentage of households and health care facilities with soap, water and a hand washing facility | Prevent |
| Hygienic sanitation facility/latrine, waste management facilities/ | Percentage of households with a hygienic sanitation facilities | Prevent |
| Household air pollution | Percentage of households using clean fuels for cooking | Prevent |
| Antiretroviral prophylaxis among HIV-positive pregnant women to prevent vertical transmission of HIV | Percentage of HIV-infected pregnant women who received antiretroviral to reduce the risk of mother- to-child transmission | Prevent |
| Reduced number of smokers among family members | Percentage of smokers among family members | Prevent |
| Community awareness about the prevention and control of childhood pneumonia | Number of men and women who are aware of the methods of childhood pneumonia prevention and control | Prevent |
| Health seeking behavior | Percentage of households seeking health care for respiratory related issues | Treat |
| Having well-ventilated and separate house for animal and human being | Percentage of households with well-ventilated and separate houses for animal and human being | Prevent |
| Availability of information on childhood pneumonia | Percentage of community members who have information on childhood pneumonia | Prevent |
Source: GAPPD framework WHO/UNICEF 2013
Monitoring is the
systematic design of information collection
on an ongoing basis to aid in improving the
implementation or operational process for
delivering a quality service or a product
Monitoring is the
systematic design of information collection
on an ongoing basis to aid in improving the
implementation or operational process for
delivering a quality service or a product
Monitoring is the
systematic design of information collection
on an ongoing basis to aid in improving the
implementation or operational process for
delivering a quality service or a product.
Monitoring is the
systematic design of information collection
on an ongoing basis to aid in improving the
implementation or operational process for
delivering a quality service or a product.
Monitoring is the
systematic design of information collection
on an ongoing basis to aid in improving the
implementation or operational process for
delivering a quality service or a product.
8.11 IMPLIMENTATION STRATEGIES
The main aim of developing the ’Awareness and prevention strategies on pneumonia among under-five children in Sidama regional state’ is to help policy makers, programme planners and implementers formulate respected actions to reduce child morbidity and mortality due to pneumonia through increased community awareness on the focus of strategies of childhood pneumonia prevention and control. .
8.12 STRATEGIES DISSEMINATION PLAN
The strategies will be published in a peer reviewed, reputable, scientific and open access journal and on the UNISA library website for ease of access. All stakeholders involved in the health sector will have unrestricted access to these strategies. The dissemination will also be through presentations at health seminars, workshops, and national and international conferences.
8.13 CONCLUSIONS
This chapter presented proposed awareness and prevention strategies on prevention and control of pneumonia among under-five children in Sidama Regional State, Ethiopia. The study brings together evidences from the current study, reviewed literatures, existing policies, guidelines and strategies. The strategies have been developed aligning with the goal of GAPP, and are hoped to contribute as reference to achieve the goal of ending preventable death of children due to pneumonia. The respective bodies under FMOH of Ethiopia, especially Sidama regional health bureau including woreda health offices and health facilities are advised to use these strategies as additional resources to formulate appropriate measures, interventions and actions in order to reduce childhood morbidity and mortality due to pneumonia.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
