AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Amanda Jane Thomas, Clinical Specialist Physiotherapist, Critical Care Outreach Team, The Royal London Hospital, Barts Health NHS Trust, UK.
Citation: Jake Causon, Robyn Cary and Amanda Jane Thomas (2021) Decannulation Failure following Tracheostomy for COVID-19: A Single Case Report J. Clin Case Rep and Stu 2(6); DOI: 10.31579/2690-8808/082
Copyright: © 2021 Amanda James Thomas. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 June 2021 | Accepted: 24 August 2021 | Published: 08 September 2021
Keywords: tracheostomy, decannulation, laryngeal stenosis, tracheomalacia
The incidence, aetiology and long term outcomes of laryngotracheal complications secondary to Tracheostomy insertion in patients ventilated for COVID-19 critical Illness are currently unknown. We report a single case from our COVID-19 institutional series who developed early subglottic stenosis and subsequent traceomalacia preventing permanent tracheostomy removal despite three decannulation attempts. We consider the known risk factors for laryngotracheal complications following endotracheal intubation and tracheostomy, in combination with the potential impact of COVID-19 pathological features. Clinical indicators from the case presentation are explored in relation to the early identification of tracheomalacia in the patient with Tracheostomy, and the mechanisms underlying these presenting features are proposed.
List of Abbreviations
OMFS: Oro-maxilla facial surgery; OWV: One way valve;FEES: Fibreoptic endoscopic evaluation of swallow; FNE: Fibreoptic nasendoscopy;CT: Computerised tomography; HFOT: High flow oxygen therapy; CPAP: Continuous positive airway pressure; HDU: High dependency unit; TM: Tracheomalacia; GORD: Gastro-oesophageal reflux disease; OSA: Obstructive sleep apnoea, MDT: Multi-disciplinary team; SBT: Spontaneous breathing trial.
The COVID-19 pandemic in the United Kingdom (UK) resulted in a large number of patients dependant on mechanical ventilation who subsequently required tracheostomy insertion. Outcomes of patients with tracheostomy following a COVID-19 diagnosis have thus far been concerned with reporting temporal characteristics such as time from insertion to decannulation and successful decannulation percentages [1, 2]. The incidence of tracheal complications and failure to decannulate in a COVID-19 cohort is currently unreported, although a small Italian sample reported a 47% incidence of full thickness tracheal lesions following Tracheostomy for COVID-19 related illness [3]. We report a single case from our institutional series who experienced more than one
tracheal complication secondary to Tracheostomy insertion following COVID-19 critical illness and subsequently failed to decannulate over several attempts
Our patient was a 71 year old female admitted with a history of fever, cough and generalised weakness, on a background of type II diabetes, hypertension, hyperlipidaemia, cardiomyopathy, obstructive sleep apnoea (awaiting trial of home CPAP ), ischaemic stroke, and depression. COVID-19 pneumonitis and an acute kidney injury were diagnosed and the patient was transferred to the critical care unit.
Initial support via facemask CPAP was poorly tolerated resulting in respiratory arrest, cardiopulmonary resuscitation and emergency intubation (Grade 2b via bougie). Four days post intubation an endotracheal cuff leak required subsequent endotracheal tube change (Grade 2b). Supra-glottal instrumental assessment at this time identified bilateral oedematous arytenoids. Noticeable oedema of the lips and tongue were also observed which appeared to be exacerbated by prone positioning. Oro-maxilla facial surgical (OMFS) input recommended intra venous dexamethasone and chlorphenamine, but tongue swelling persisted.
29 days after intubation, a surgical tracheostomy was inserted (size 7 TRACOE® twist plus, cuffed, non-fenestrated). During weaning from mechanical ventilation the patient was consistently able to tolerate cuff deflation but unable to tolerate placement of a one way valve (OWV) in line with the ventilator tubing. Once liberated from mechanical ventilation, intolerance to finger occlusion or OWV placement persisted. A fibreoptic endoscopic evaluation of swallow (FEES) at this time revealed a patent supraglottic airway (Figure 1) and mild oro-pharangeal dysphagia, a short course of dexamethasone was prescribed for assumed airway oedema. The patient was subsequently able to tolerate the OWV all day and progressed to normal diet and fluids.

30 days after the Tracheostomy was initially placed, the patient was decannulated but deteriorated over the next hour demonstrating increased work of breathing, anxiety and arterial desaturation to 70% with audible stridor. A size 6 TRACOE® twist cuffed, non-fenestrated tracheostomy tube was re-inserted over bougie into the existing stoma and specialist referral for airway investigation initiated. A third short course of dexamethasone was prescribed.
Following this first attempt, the patient was weaned to continuous cuff
deflation but was consistently unable to tolerate the OWV demonstrating increased work of breathing and minimal airflow through the upper airway on digital tracheostomy occlusion. Fibreoptic Nasendoscopy (FNE) revealed a crowded oropharynx with prominent tonsils and base of tongue, normal vocal cord movement, glottic gap and minimal arytenoid oedema. A contrast CT neck (Figure 2) at this time demonstrated narrowing of the subglottic airway caudal to the tracheostomy site with a minimum cross-sectional diameter of 58mm2 (compared to 168mm2 at the same level in 2010).

Micro-laryngoscopy revealed a 60% subglottic stenosis with anterior granulation proximal to the tracheostomy and a cartilaginous ring loose at the tracheostomy site. The subglottic stenosis was managed with tracheoplasty, laser ablation of the granulation tissue, cruciate cuts and balloon dilatation. Post-operatively, the patient was tolerant to cuff deflation but remained intolerant of OWV insertion. OWV intolerance was attributed to post-operative swelling and recurrent reduced subglottic patency, however repeat FNE on post-operative day 3 demonstrated a collapsing posterior tracheal wall on expiration.
Despite these findings a second decannulation attempt was made approximately 60 days following the initial tracheostomy insertion. The patient was stable initially, however the voice was noted to be significantly asthenic. Seven hours after decannulation the patient was stridulous with an increased work of breathing. FNE revealed a patent upper airway, however to avoid the risk of overnight deterioration a size 6.0 TRACOE® twist uncuffed, fenestrated tube was re-inserted into the existing stoma. Lansoprazole and dexamethasone were prescribed.
Following this second failed decannulation, trials of digital tracheostomy occlusion elicited a low pitch, rough strained vocal quality, immediate back pressure, cough, discomfort, desaturation and tachycardia. Several days later the patient experienced a respiratory arrest due to a plugging of the right main bronchus. FNE, microlaryngoscopy and bronchoscopy performed during and following the resuscitation event (and concomitant tracheostomy change) demonstrated a patent mid trachea to carina although mild malacea of the posterior trachea wall was noted. Proximally, the laryngeal appearances were normal although a haematoma on the right vocal cord was identified and a left vocal cord posterior polyp was removed with suction. Minimal granulation tissue and minimal stenosis of the sub-glottic area were reported.
Over the next few days the patient’s respiratory function deteriorated requiring high flow oxygen therapy (HFOT) delivered via the Tracheostomy. Although continuous cuff deflation was well tolerated, placement of the OWV or digital tracheostomy occlusion resulted in immediate distress, increased work of breathing, and forceful coughing. Vocalisation attempts with the OWV in situ elicited a rough strained voice quality and short phrase speech. Application of the OWV in line with the HFOT appeared to increase valve tolerance but only to a maximum of 10mins. Repeat FNE revealed a clear view to the carina and main bronchi although mild malacia of the posterior tracheal wall was again noted.
In an effort to promote OWV tolerance a further tracheostomy change was performed (size 6 TRACOE® twist uncuffed non-fenestrated). Over the next 2 weeks tolerance to OWV (in line with the HFOT) progressed to greater than 4 continuous hours, although during these periods, the valve was repeatedly coughed off and replaced. Vocal trials remained dysphonic, strained and breathy, with short phrase speech. Interestingly, tolerance to OWV in the supine posture was limited (10secs) and associated with desaturation and increased work of breathing in comparison to OWV application in the upright posture which was consistently tolerated.
In preparation for a third decannulation attempt the patient was weaned to cold humidification and subject to a capping trial. Capping was poorly tolerated with immediate increased work of breathing and intolerance. Facial CPAP (CPAP-Vivo -Breas®) with incremental pressures to 10cmH2O were trialled in an attempt to splint the airway during further capping attempts. Although the patient was tolerant of facial CPAP, simultaneous use with the tracheostomy cap did not improve tolerance.
The third decannulation was planned with the agreement of the multi-professional team, 29 days after the second failed attempt. To ensure appropriate safety netting in the event of poor outcome, the patient was transferred to the high dependency unit (HDU) for the procedure. FNE immediately prior to the procedure demonstrated glottic opening and a distant view of the sub-glottis above the tracheostomy revealed no stenosis. Upon decannulation, the patient immediately desaturated, became bradycardic and visibly distressed with notable inspiratory retraction of the stoma site. A trial of facial CPAP failed to alleviate these features, and a size 6 TRACOE® twist cuffed non-fenestrated tube with subglottic port was reinserted. Three days later, some 90 days following initial tracheostomy insertion, the tube was changed (Size 6 TRACOE® twist un-cuffed fenestrated), and discharge planning for long-term Tracheostomy was initiated.
In the case presented, an early 60% sub-glottic tracheal stenosis identified on micro-laryngoscopy prevented Tracheostomy removal. Since the patient was unable to tolerate placement of a one way valve (which directs expiratory airflow through the glottis) “in line” with the ventilator [4], this stenosis may have been present at a very early stage. Laryngeal stenosis has been reported to occur in 2% of patients whose trachea is intubated for 2-5 days, and 5% when intubation is between 6 and 10 days [5]. Results of surgical intervention for stenosis is usually good, although two thirds of patients with iatrogenic stenosis may eventually require long term tracheostomy [6].
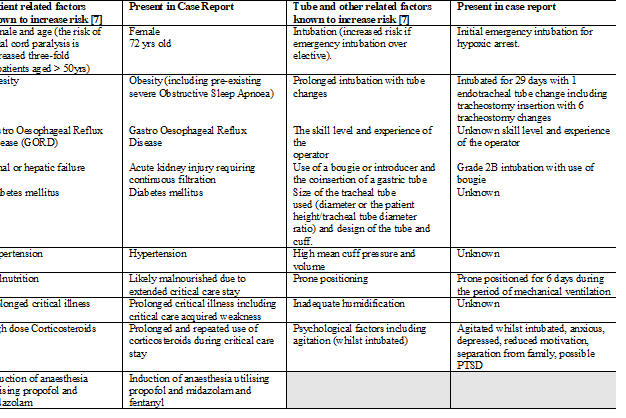
It is well understood that prolonged tracheal intubation or subsequent tracheostomy may damage or impair the larynx in a non-COVID-19 population. Wallace and McGrath, 2021 [7] classify laryngeal complications after tracheal intubation and tracheostomy, as early (including laryngeal oedema, vocal cord palsy or paresis); late (including anterior glottic web, arytenoid cartilaginous trauma); and very late (including glottic and subglottic stenosis) events. While there is limited data exploring the aetiology, type and extent of laryngeal injury following intubation, there are known risk factors that appear to influence complication incidence. Some patient characteristics are thought to adversely affect tissue perfusion and healing, or predisposition to neuropathy. Other risk factors are associated with physical interventions such as intubation, tracheal tube type and patient positioning [7]. In Table 1 we compare the known risk factors for laryngotracheal complications (post intubation or tracheostomy) with our case, and suggest that these features may have predisposed complications without the additional contribution of COVID-19 illness.
To our knowledge, the incidence of laryngotracheal complications and failure to decannulate in a COVID-19 cohort is currently unreported. Fiacchini et al, 2020 [3] report 46.7% of their COVID -19 cohort developed full thickness tracheal lesions and or trachea-oesophageal fistulas after invasive ventilation compared to 1% in matched non-COVID-19 controls. These authors propose several causative mechanisms relating to COVID-19 treatments and pathophysiology, for example the use of prone positioning that may increase pressure on the tracheal wall and exacerbate tracheal necrosis; the pro-thrombotic and anti-fibrinolytic state of patients with COVID- 19 which predisposes micro vascular injury; and corticosteroid use resulting in mucosal atrophy and delayed healing [8].
Although tracheoplasty to manage subglottic stenosis in our case was successful, the patient was unable to be decannulated. Repeated inability to decannulate from tracheostomy in this case was attributed to a diagnosis of Tracheomalacia (TM), which has been defined as diffuse or segmental tracheal weakness due to the softening of the tracheal cartilage. Tracheobronchomalacia exists when this weakness extends into one or both of the main stem bronchi. Both conditions cause narrowing of the airway during expiration [9, 10].
Although TM can be congenital [10], endotracheal intubation or tracheostomy can elicit an acquired cause. These tubes can damage the tracheal cartilage or membrane at the level of the cuff or stoma site weakening the tracheal wall. Acquired TM is usually segmental and associated with prolonged intubation, concurrent high dose steroids and cuff pressures in excess of 25cmH2O [11]. The mechanism eliciting these features is uncertain but may include pressure necrosis, impaired blood flow, recurrent infection, mucosal friction and mucosal inflammation. Early COVID-19 research [3] suggests the virus itself may increase the incidence of micro vascular injury and necrosis of the tracheal mucosa. The prevalence of TM in the COVID-19 Tracheostomy cohort may be further increased through high viral replication in the tracheal epithelium [3].
The prevalence of TM in adults post translaryngeal intubation or tracheostomy is currently unknown. Kandaswarmy et al, 2013 [12] report severe TM (complete tracheal collapse on expiration when PEEP is removed) in 22% of patients who failed extubation after a successful spontaneous breathing trial (SBT). The prevalence of GORD (gastro-oesophageal reflux disorders), prolonged critical care stay and obesity was higher in the severe TM group compared to matched controls, suggesting these features may increase risk. Similar risk factors for TM have been reported [13] and the effect of tracheal mucosa exposure to digestive enzymes on tensile tracheal strength has been previously postulated [14]. Potential risk factors for the development of Tracheomalacia in our case are listed in Table 1, including features of the critical care stay which may have exacerbated the problem. Of interest, Kandaswarmy et al, 2013 [12] suggests that pre-existing TM in the critical care setting can be misdiagnosed as obstructive sleep apnoea (OSA), and may exist with a higher incidence than expected, particularly since endotracheal intubation and ventilation delay the early recognition of substantial tracheal collapse. Our case had a diagnosis of OSA prior to admission and was waiting assessment for CPAP, raising the possibility that TM existed pre-morbidly and progressed secondary to events post admission.
Subtle features of the clinical presentation may have alerted the multidisciplinary team (MDT) to the potential for TM to limit decannulation from Tracheostomy. For example, the patient was never consistently able to tolerate a OWV with comfort, despite the fact that after resolution of the initial subglottic stenosis, the glottic and supraglottic structures were consistently reported as normal or near normal on FNE. Application of the OWV is known to increase subglottic tracheal pressure [15] due to restoration of expiratory glottic flow; however the increases in expiratory dead space, flow rate and pressure change elicited by the OWV may exacerbate both inspiratory and expiratory tracheal diameter changes when the trachea itself lacks structural integrity.
Tolerance to the OWV was improved with the application of HFOT via the Tracheostomy, which may generate an increase in dynamic positive pressure within the trachea limiting both inspiratory and expiratory tracheal collapse. Tolerance to the OWV was also improved in the upright compared to the supine posture where chest wall and abdominal resistive loads may have widened the dynamic tracheal pressure change exacerbating tracheal collapse. Despite patency of the upper airway, the patient was unable to tolerate Tracheostomy capping, suggesting that increasing both inspiratory and expiratory dead space and the associated increase in tracheal pressure changes exacerbated intolerable dynamic tracheal collapse. We presume that the Tracheostomy tube itself was acting as a “splint” within an airway with variable integrity [16], which when removed elicited symptomatic dynamic tracheal collapse.
The extent to which morbidity related to both COVID-19 and a prolonged critical care stay influenced the presenting features in this case are difficult to differentiate. Extreme breathlessness on exertion, critical care acquired weakness, radiological evidence of lung fibrosis, post-traumatic stress disorder (PTSD), high level anxiety and poor motivation have been frequently reported consequences in critical care survivors following a COVID-19 admission. In addition, failure to decannulate over several attempts may have increased patient anxiety and overall engagement with the weaning process. These physical and psychological factors are likely to have prolonged the process of achieving the potential for decannulation and therefore cannot be excluded from a causative discussion.
Our case was unable to be decannulated from Tracheostomy following a prolonged critical care stay elicited by COVID-19 pneumonitis. The patient initially developed a subglottic stenosis which was surgically managed but failed to enable the tracheostomy to be removed. Further decannulation attempts, select investigations and interpretation of the clinical presentation resulted in a diagnosis of Tracheomalacia and long term Tracheostomy. The long term outcomes and prevalence of tracheal complications in patients ventilated and tracheostomised for COVID-19 are currently unknown. On-going review and surveillance of this cohort may allow the early identification and management of morbidity and a greater understanding of complication prevalence.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
