AUCTORES
Globalize your Research

Mini-Review Article
*Corresponding Author: Ossama Tawfik. Department of Saint Luke’s Health System, USA.
Citation: Ossama Tawfik , and Jwan Alallaf. Current Approaches to Diagnosis and Treatment of Breast Cancer and Future Directions. Women Health Care and Issues. Doi:10.31579/2642-9756/007
Copyright: ©2019. Ossama Tawfik. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 December 2018 | Accepted: 11 January 2019 | Published: 18 January 2019
Keywords: endometrial cancer, cancerogenesis
Breast cancer is the most common cancer in women worldwide (GLOBOCAN 2012) It is estimated that over 2 million new breast cancer (BC) cases are diagnosed worldwide and over 600,000 women would die of the disease annually
Breast cancer is a heterogeneous disease encompassing various entities with distinct morphologic features and clinical behaviors. This diversity is the result of distinct genetic, epigenetic, and transcriptomic alterations. In order to categorize this heterogeneity and standardize the language, BC classification systems have been developed. These classification schemes have evolved over many decades into a valuable tool that is used to aid in treatment and prognosis. Breast cancer can be broadly categorized into non-invasive (in-situ) and invasive (infiltrating) carcinomas [12-15]. Breast carcinoma in situ is further sub-classified as either ductal or lobular. Cell types, growth patterns and cytological features form the basis to distinguish between the two types. Ductal carcinoma in situ (DCIS) is considerably more common than lobular carcinoma in situ (LCIS) and encompasses a heterogeneous group of tumors. DCIS has traditionally histologically been further sub-classified based on the architectural features of the tumor which has given rise to at least five well recognized subtypes including Comedo, Cribriform, Micropapillary, Papillary and Solid variants [12,13]
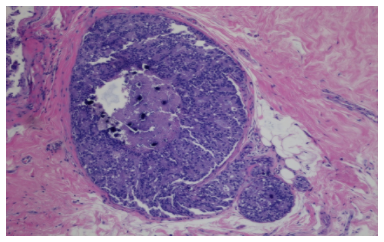
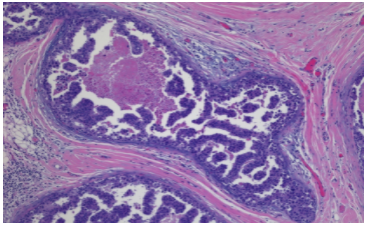


Representative examples of ductal carcinoma in-situ.
Figure 1A shows a cribriform DCIS with calcification and central necrosis. B show a micropapillary pattern. Solid pattern is identified in C and high-grade DCIS with Comedo necrosis in D (Hematoxylin and eosin, magnification x10).
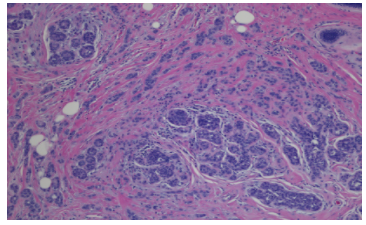
Similarly, invasive carcinomas are as complex and as heterogeneous as their DCIS counterparts. They are differentiated into various histological subtypes, some with well characterized histologic features while the majority remain to be of no special type [12-15]. The major invasive tumor types include infiltrating ductal, lobular, mucinous (colloid), tubular, cribriform, medullary, squamous and papillary carcinomas (Figures 2 and 3). Examples of rare types include apocrine, metaplastic, secretory, hypersecretory, glycogen-rich, lipid-rich, adenoid cystic and small cell neuroendocrine carcinomas. Of these, infiltrating ductal carcinoma (IDC) is, by far, the most common subtype accounting for 70–80% of all invasive lesions (Figure 2).
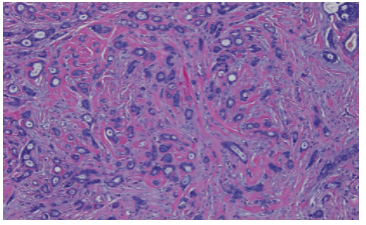

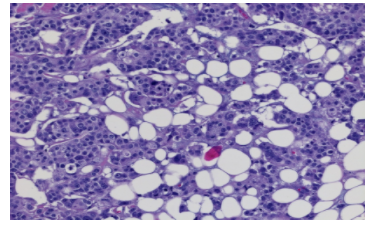
Representative examples of invasive ductal carcinoma with different histologic grades.
A well differentiated ductal carcinoma in A, moderately differentiated carcinoma in B and poorly differentiated carcinoma in C (Hematoxylin and eosin, magnification A: 10x, B and C: 20x).

where lobular carcinoma in situ is negative for the marker (Immunostain, magnification x10).
Representative examples of lobular carcinoma. Figure 3A shows lobular carcinoma in situ and Figure 3B shows invasive lobular carcinoma next to foci of lobular carcinoma in situ (Hematoxylin and eosin, x10). E-cadherin immunostain is shown in Figure 3 C where lobular carcinoma in situ is negative for the marker (Immunostain, magnification x10).
Breast cancer are graded into three grades (I-III) according to the Nottingham modification of Bloom-Richardson system (SBR) based on the cytologic features evaluating nuclear size and degree of nuclear hyperchromasia and pleomorphism, growth pattern evaluating the extent of glandular/tubule formation and mitotic activity (16-18). Each of these three elements is assigned a score on a scale of 1 to 3 with a final grade determined by the sum of the three scores: where grade 1 well differentiated tumors have a score of 3-5, grade two have a score of 6-7 and grade 3 have a score of 8-9.
Unfortunately, the above described system, albeit it is the only accepted grading system accepted, lacks precision in assessing all three parameters including nuclear grade, mitosis and tubular formation, leading to an element of subjectivity with significant interobserver variability. Furthermore, it was not suited for grading in situ lesions or the other non-ductal invasive carcinoma types. Several investigators have attempted to improve the accuracy of grading BC for better correlation with prognosis and survival. Our group has recently proposed a new grading system including the routine evaluation of nuclear features combined with automated proliferation index (N+P) system], using a digital imaging system, eliminating the growth pattern of tumor for better representation of tumor biology. Similar to the SBR grading system, each of the nuclear and automated proliferation index components was assigned a score on a scale of 1 to 3 with the final grade determined by the sum of the two scores. The automated MIB-1 count was likewise scored into three categories: score 1:≤9%, score 2:10-25%, and score 3:> 25%. This system has the advantage of being used for not only invasive ductal carcinomas, but for all other invasive carcinomas, including lobular, other special type carcinomas and non-invasive carcinomas [19-21].
Our studies compared the N+P system with the SBR grading system and correlated them with a variety of clinicopathological parameters including patient’s overall survival, tumor size, angiolymphatic invasion, LN status, and biomarker status including estrogen receptor (ER), progesterone receptor (PR), p53, epidermal growth factor receptor, BCL-2 and Her-2. Although there was an agreement between the two systems with histologic and prognostic parameters studied, there was 37% disagreement when grading individual tumors. Fifty- three percent of SBR grade II tumors were “downgraded” to N+P grade I, and 7% were “upgraded” to N+P grade III. Distinction among the different histologic grades for overall survival curves was better indicated by N+P than SBR grading systems [19-21].
The underlying basis for the development of malignancy is a series of genetic mutations resulting in dysregulation of normal cellular replication resulting in the ability of uninhibited cell growth and tumor formation. In BC, a number of important genetic mutations have been discovered that characterize tumor biology. This molecular characterization confers information about how aggressive a tumor is, which has important prognostic implications. Further, knowledge of the mechanisms that provide a survival advantage for the tumor has led to the development of agents targeted to these pathways resulting in tumor cell death. Most notable in the case of BC are the development of drugs against the ER and Her2 receptors, which are overexpressed in some tumors. The estrogen receptor was the first molecular marker discovered to have a role in breast cancer. This receptor became important clinically with the discovery of the therapeutic benefit of selective estrogen receptor modulators (SERMs), such as tamoxifen and raloxifene in reducing BC recurrence in tumors with ER positivity. Aromatase inhibitors were later introduced after SERMs as another effective therapy for decreasing estrogen in postmenopausal women.
Recently, proposed classification schemes used gene expression microarray analysis, to categorize BC phenotypes based on their molecular features. The purpose of these classification systems is to facilitate identification of tumor markers that may serve as indicators of prognosis and potentially as therapeutic targets. Breast cancers are categorized into at least five major molecular subtypes: luminal A, luminal B, normal breast like, Her2, and basal-like (BL)
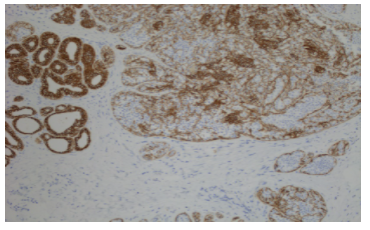
Figure 4. Representative examples of immunostains for invasive breast carcinomas positive for estrogen receptor in A, progesterone receptor in B and Her2 in C (magnification, x10).
(Figure 4) [22-31]. However, the utility of such assignments of molecular subtyping, especially the BL subgroup, also known as triple negative tumors (ER, PR and Her2 negative), has generated much interest and has been called into question by scientists, pathologists, and oncologists alike.

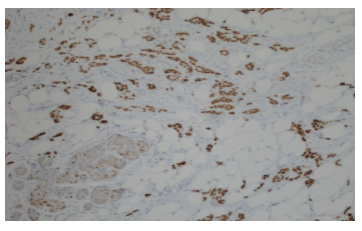
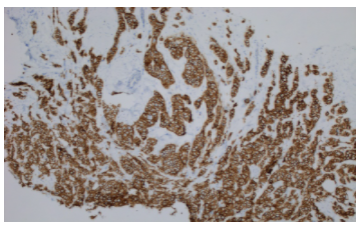
Representative examples of immunostains for invasive breast carcinomas positive for estrogen receptor in A, progesterone receptor in B and Her2 in C (magnification, x10).
Triple-negative (TN) tumors are highly aggressive, rapidly growing, hormone-unresponsive tumors that tend to be diagnosed at a later stage, affect younger women, and are associated with shorter overall survival. TN tumors have recently been shown to be molecularly, pathologically, and clinically a heterogeneous subgroup, although the majority are BL [24,29].
Treatment of breast cancer has evolved over the years. Currently treatment strategies are tailored for each patient based on her clinical status and the characteristics of that particular patient and her tumor. Options varying from using a single treatment modality to various combinations of surgery, chemotherapy, radiation, hormonal therapy and/or immunotherapy [31,32]. Factors such as patient’s age and general health status, as well tumor characteristic including type, histologic grade, burden, location, size, number of lesions, extent of nodal involvement and biomarker and genetic status should be taken into consideration before recommending treatment options.
Surgical options have undergone tremendous changes over the last several decades. Since its introduction by Halstead, radical mastectomy was the only treatment option provided. Later on, breast conserving surgeries were introduced such as simple mastectomy, modified radical mastectomy, partial mastectomy, segmental mastectomy, quadrantectomy, lumpectomy and skin-sparing and nipple-sparing mastectomies allowing for reconstruction with artificial implants [33-35]. Metastatic involvement of LNs is the single most important prognostic factor in BC exclusion and inclusion criteria are essential for diagnostic precision, accurate prediction and overall improvement of patient care. The traditional axillary LN dissections were quickly replaced by sentinel node procedures significantly reducing morbidity and treatment cost for early stage BC patients.
Radiotherapy is used in early BC after breast conservation surgery and in locally advanced BC patients post mastectomy. Breast radiation is an integral part of breast conserving surgery. Postoperative radiotherapy is strongly recommended following surgical excision [36-38]. Whole breast radiation therapy alone reduces the 10-year risk of locoregional and distant recurrence by 15% and the 15-year risk of breast cancer-related mortality by 4%. Boost irradiation gives a further 50% relative risk reduction. Many radiation techniques are currently utilized to treat patients with the goals of maximizing treatment of the targeted lesions and minimizing risks to surrounding organs. Three-dimensional conformal radiation therapy (3DCRT) with/without wedges or field-in-field method, intensity modulated radiation therapy (IMRT), volumetric modulated arc therapy (VMAT), hybrid technique, helical tomotherapy, and Tomo direct are examples of proposed radiation treatment options for BC patients in the literature.
Similar to surgical and radiation modalities, major advances in chemotherapy for BC has led to a significant decrease in mortality rate from BC in the last decade. Many challenging factors such as tumor stage and characteristics including hormonal status, Her2 status and molecular type dictate among others the choice of specific chemotherapeutic agents. Luminal BCs, also known as hormone receptor positive represent the vast majority (60-70%) of BC cases.
Endocrine therapy with agents such as tamoxifen, aromatase inhibitors is the mainstay for treatment. Additional agents such luteinizing hormone-releasing hormone analogs and selective estrogen receptor degraders (fulvestrant) could be used for patient’s refractory to the other hormonal therapies. Anti-Her2 monoclonal antibodies such as trastuzumab, epratuzumab are targeted therapeutic agents for treatment of Her2 positive BC either alone or in combination with other traditional chemotherapeutic agents.
Unlike hormone positive and/or Her2 positive BCs, the TN molecular type is the most difficult to treat. For years standard chemotherapy with conventional cytotoxic agents such as taxanes, anthracycline, alkylating agents such as cyclophosphamide and platinum drugs remained as the only therapeutic options for such aggressive form of the disease. Over the past few years, with the better understanding of the biologic heterogeneity of BC, recent advances have been made in the discovery of new targeted drugs that are very promising. Many clinical trials are underway investigating several promising agents. Drug combination such as poly(ADP-ribose) polymerase (PARP) inhibitors tor carboplatin to standard chemotherapy, anti-angiogenic agents, EGFR inhibitors and src inhibitors are promising cancer therapeutic agents. Perhaps nothing as intriguing as the concept of immunotherapies nowadays.
Programmed cell death ligand 1 (PD-L1) encoded by the CD272 gene on chromosome 9, is a 40kDa transmembrane protein that is expressed on a variety of normal cells including NK cells, macrophages, dendritic cells, B cells, epithelial cells and endothelial cells. Recent data suggest that the PD-1 pathway may be an active immune checkpoint in a variety of cancers [39-43]. Normally when the immune system detects cancer cells it activates cytotoxic T cells. Once the T cells are activated, they infiltrate the tumor microenvironment, recognize the tumor cells and starts killing them. Targeting the PD-1/PD-L1 pathway may prevent inhibitory T-cell signaling and reactivate T cells to mediate tumor killing. A growing body of evidence has clearly shown that certain "immunogenic" tumors that overexpress PD-L1 can evade destruction by the immune system. PD-L1 has been reported to be expressed on tumors cells and stromal tumor-infiltrating immune cells (ICs). Few studies have evaluated the expression of PD-L1 in BC [44-46]. While BC is one of the less immunogenic cancers, some data suggest that the PD-1 pathway might be active in certain subtypes. PD-L1 expression was shown to be increased in TN/BL breast cancer cells. Breast cancers infiltrated by PD-1 positive ICs was associated with worse survival in Luminal B and triple negative BC types. Recent studies suggest that PD-L1 positive BCs were associated with more aggressive features including younger age at diagnosis, large size cancers, LN positivity, ER negativity and distant recurrence. Paradoxically the PD-L1 positive BCs were associated with significantly improved survival.
While this is an exciting time for immunotherapy, we are still far from understanding the exact relationship between PD-L1 expression by ICs and cancer cells and other immunologic features of the breast tumor microenvironment. We, and others, have previously shown that the value of PD-L1 detection by immunohistochemistry as a valuable marker is confounded by many unresolved issues such as different detecting antibodies, different staining protocols and platforms and different cutoff points in addition to variable tissue preparations and variable tumors with different characteristics. Our recently published study has shown an excellent agreement between the three PD-L1 antibodies, including Dako (22C3), Ventana (SP263) and BioCare antibodies, with highly significant Kappa values (p≤0.001) (47). PD-L1 expression was more likely to be associated with higher tumor grade, TN molecular subtype, hormone negative and highly proliferative tumors (p <0.001) (9). Given the high concordance, it is not surprising that all three antibodies demonstrated the same associations with all pathologic and clinical parameters studied. Thus, as in the case with quantitation of PD-L1 in lung cancer and melanoma, pathologists might have the option of utilizing less expensive reagents for the evaluation of this marker in BC. It is inconceivable to perform a unique FDA-cleared assay for each marker and disease following the recommendation of certain biopharmaceutical-sponsored or investigator-driven study. Indeed, many investigators have recently recommended an urgent need to harmonize approaches for PD-L1 testing independent of biopharma for realistic economic and practice expectations in PD-L1 assessment for targeted therapy.
In our second manuscript we explored the expression of PD-L1 in tumor cells along with the expression of CD3, CD4, CD8, CD20 and CD68 markers in tumor microenvironments of a cohort of patients with matched primary BC and metastatic disease in regional LNs (48). Expression of the different markers was be correlated with several clinical and pathological parameters. There was 100% agreement for PD-L1 expression on tumor and ICs between BC and matched LN. PD-L1 is differentially expressed in primary BC and regional nodal disease. Expression correlated with higher grade, hormone receptor negativity and highly proliferative tumors (p <0.001). In LNs, the high positivity rate was driven by TN status (70% vs 5%) (P<0.0001). In contrast, there was significantly near total absence PD-L1 expression in distant metastatic lesions compared to BC and LNs (2-4% in Mets vs 17-20% in BC and LN, p=0.009). ICs density varied in BC and metastatic tumors with predominance of CD3 and CD68 and near total absence of CD20 cells. PD-L1 expression was mainly associated with CD68 cells. There were consistent higher numbers of CD3 (CD8 > CD4) than CD20 cells in primary and metastatic tumors. Correlation of PD-L1 expression in BC and its microenvironment may be useful for development of new treatment strategies. Most of the previous studies focused in evaluating PD-1 expression in the different types of lymphocytes including CD3, CD4, CD8, CD19, CD20 and surprisingly ignoring the evaluation of PD-L1 expression in macrophages. Tumor-associated macrophages play an important role in tumor progression, metastasis and recurrence after treatment. Recent evidence suggests that macrophages are key players in PD-1/PD-L1 cytotoxic T cell signaling and activation. The potential role of macrophage derived paracrine signaling is a critical factor for effective immunotherapy. Correlating the regulatory role of macrophages and overall treatment response could lead to potential targets that could overcome resistance to immunotherapy. Our study is one of the very few that has focused on evaluated PD-L1 expression in the macrophages and correlating it’s with the different histopathologic and clinical parameters.
In conclusion, we as well other investigators have successfully categorized breast cancers depending on the PD-L1 expression in tumor cells and infiltrating ICs. It might be important to test tissue for PD-L1 positivity in primary, locally metastatic and distant metastatic disease separately since there is a differential expression between the same tumors. There is tremendous potential for development of treatment strategies based on the PD-L1 expression in tumors and their microenvironment. It is hoped that we would able to identify certain types of breast cancer that has the potential of evading the immune surveillance and become successful in metastasizing. Successful identification of such aggressive primary and/or metastatic cancers would be very helpful in selecting patients for appropriate immunotherapy as well as accurate prediction and overall improvement of patient care.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
