AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Karachi, Department of Pharmacy University of Karachi, Pakistan.
Citation: Rehan Haider, Riggs Pharmaceuticals Karachi, Department of Pharmacy University of Karachi, Pakistan.
Copyright: © 2023, Rehan Haider. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 September 2023 | Accepted: 30 October 2023 | Published: 24 November 2023
Keywords: congestive heart failure; cardiac dysfunction; cardiomyopathy; heart disease risk factors; pathophysiology management; lifestyle modifications; medications echocardiography
Congestive heart failure (CHF) is a continual condition characterized by the heart's inability to pump blood efficiently, which is essential for the buildup of fluid within the lungs and distinctive components of the body. It is a critical and regular health problem globally, affecting hundreds of thousands of people, primarily the elderly. CHF can cease owing to several underlying reasons, including coronary artery sickness, excessive blood strain, heart valve troubles, and cardiomyopathy.
This summary aims to define CHF together with its pathophysiology, threat elements, clinical manifestations, analysis, and control. The pathophysiology of CHF includes weakening of the coronary heart muscle, which can also occur because of harm from preceding coronary heart attacks, extended high blood pressure, or special elements affecting coronary heart features. Because the pumping ability of the heart diminishes, blood glide in critical organs becomes inadequate, leading to symptoms, shortness of breath, fatigue, and fluid retention.
Numerous risk factors contribute to the development of CHF, including age, coronary heart sickness, obesity, diabetes, smoking, and a sedentary lifestyle. Early diagnosis of CHF is critical for saving the patient from improving and decorating consequences. Diagnostic methods may additionally include medical records, physical examinations, imaging checks such as echocardiography, and blood tests to evaluate coronary heart characteristics and discover the underlying functionality.
CHF control aims to alleviate signs and symptoms, sluggish sickness development, and enhance the pleasantness of life. Treatment strategies usually involve lifestyle changes such as adopting a coronary heart-wholesome diet, engaging in regular exercise, and quitting smoking. Medicinal pills such as diuretics, ACE inhibitors, beta-blockers, and angiotensin receptor blockers are prescribed to enhance coronary heart characteristics and decrease signs and signs. In severe cases, surgical interventions, such as coronary artery pass grafting or coronary heart transplantation, can be considered.
As CHF is a continual condition, affected individual education and regular compliance with healthcare carriers are vital to display the ailment's improvement and regulate remedies. With improvements in scientific treatment plans and early detection, CHF analysis has advanced over the years. However, it remains a vast public health challenge, necessitating continuous research and cognizance efforts to beautify affected person consequences and decrease the load of this situation on affected human beings and healthcare systems.
The concept that there may be a right-away relationship between diabetes and congestive heart failure (CHF) is not always new. In 1954, Lund beck [1,2] posted an editorial on clinically crucial headaches in patients with diabetes, underlining that heart ailments are not unusual in patients with diabetes; indeed, it is present in one-third of aged subjects. He became the primary to suggest the presence of diabetes-particular cardiomyopathy. 20 years later, Rubler et al. [3] posted helping information, concluding that myocardial disease seemed to be a complication of the diabetic state and now not simply because of coronary artery disorder (CAD). Shortly thereafter, the Framingham look presented epidemiologic evidence of a strong relationship between CHF and diabetes. The latter examination indicated that the relationship between diabetes and CHF was no longer disadvantageous because of conventional threat factors for coronary heart ailment (CHD), but also related to other mechanisms [4]. The prevalence of CHF is growing in Western societies because of the growing older population and accelerated survival following ischemic heart ailment (IHD), especially myocardial infarction (MI) [5]. There are numerous known causes of CHF, including high blood pressure, CAD, valvular disorder, arrhythmias, anemia, renal failure, and thyroid dysfunction [5-9]. Hazard elements for the development of CHF include growing age, valvular coronary heart ailment, and IHD, especially previous MI, electrocardiographic symptoms of left ventricular hypertrophy, cardiomegaly detected using chest X-ray, elevated coronary heart price, hypertension, and decreased pulmonary crucial capability. The Framingham Look used several of those danger factors to assemble multivariate danger components to identify excessive-hazard applicants for CHF [10]. presently, IHD is the leading purpose of CHF in industrialized societies with diabetes as a hastily rising chance issue for each CHF and IHD [8,11]. thinking about the unexpectedly developing occurrence of diabetes [12], this means that the mixture of diabetes and CHF turns into increasingly commonplace in the future. bad glucose control contributes to the development of CHF as pondered by using the relation between an increase in glycated hemoglobin (HbA 1c) and the hazard of growing CHF [13]. In an epidemiologic look at an elderly Italian cohort, 9.5% of the individuals had CHF and 14.7% had diabetes. interestingly, the superiority of diabetes among topics with the CHF was increased by approximately 30%. This association was strengthened. during the follow-up, indicating that CHF predicts the appearance of diabetes [14].
In summary, there is a strong link between CHF and diabetes, and both conditions are becoming increasingly common. The links between these disorders are complex and has not yet been fully explored signs and symptoms and diagnosis.
Analysis and Definition of Congestive Heart Failure
The current diagnosis of CHF is based entirely on a summary of clinical signs and symptoms combined with characteristic signs, symptoms, and signs and symptoms of myocardial disease [5]. In medical physical activities, CHF is commonly divided into systolic and diastolic myocardial disorder. The latter is also known as coronary heart failure with preserved left ventricular characteristics, with systolic disease representing the impaired ability to expel blood from the left ventricle, and diastolic disease is a disorder of ventricular filling due to relaxation abnormalities. Echocardiography is the preferred technique for documenting such a disease, and the left ventricular ejection fraction is the maximum typically used term for impaired systolic dysfunction. Evidence of odd quiescence of the left ventricle reduced diastolic distensibility, or diastolic stiffness is an Echocardiographic signal and symptom of the diastolic disease. Echocardiography along with tissue Doppler imaging (TDI) is beneficial for detecting diastolic myocardial disease in humans with diabetes, similar to the non-diabetic population [15,16]. Plasma concentrations of natriuretic peptides and their precursors are also useful for diagnosing CHF in patients, including those with diabetes [5,17]. The first clinical type of CHF severity was presented through the big-apple coronary heart association (Table 40. 1). This type of therapy was used in all patients with CHF. regardless of visibility in the hospital or ambulatory area and etiology.
Diagnosis and Definition of Glucose Abnormalities
Diabetes and other glucose abnormalities are a collection of metabolic disorders characterized by hyperglycemia due to defects in insulin secretion, insulin motion, or both. Diabetes is associated with harm, dysfunction, and failure of various organs [18]. Metabolic syndrome is an entity that has been defined in numerous ways [19, 20], combining distinct cardiovascular threat factors, including abnormalities in glucose homeostasis.
Epidemiology
Risk Factors for CHF And Diabetes
The most important risk factors for cardiovascular disease (CVD) and MI are family history, smoking, abnormal blood lipids, hypertension, diabetes, obesity, and socioeconomic factors [21]. Many risk factors for CHF are, by necessity, similar to those for CVD, with IHD and hypertension being the leading causes. Other common factors influencing the occurrence of CHF are male sex, smoking, overweight, physical inactivity, and valvular heart disease [5]. Type 2 diabetes mellitus (T2DM) and poor glucose control, observed as high fasting plasma glucose and elevated HbA 1c are also of considerable importance [22–27]. Risk factors for T2DM include family history, age, overweight or increased waist-to-hip ratio, and sedentary lifestyle [28, 29]. The morbidity is known to increase progressively with the number of Existing risk factors [30]. Particular risk factors for CAD in T2DM are lipid perturbations, including small, dense, easily oxidized low-density lipoprotein (LDL) particles and low-density lipoprotein (HDL) cholesterol and increased triglycerides Moreover, poor neuro metabolic control was observed with high fasting plasma glucose and elevated HbA1c contribution [31]. Hypertension is also an important risk factor. The Reykjavik Study showed a strong relationship between fasting and post-load glucose levels and subsequent risk for hypertension, even after adjustment for age, body mass index (BMI), and weight gain, which is interesting because hypertension is one of the main risk factors for CHF [24, 25]. Patients with diabetes and CHF have higher IHD, increased systolic blood pressure (BP), lower diastolic BP, and higher HbA1c than their counterparts without diabetes [26]. Accordingly, many mutual risk factors exist for CHF and glucose abnormalities.
Prevalence of CHF and Glucose Abnormalities
The prevalence of CHF has varied in different studies. partly because of differences in the definition of this disease [5]. The demand that a heart failure diagnosis be supported by evidence of systolic dysfunction on echocardiography may be difficult to obtain in epidemiologic studies. Modern Echocardiographic techniques did not exist when several of the studies still serving as an important source of information have been conducted [4,32]. The prevalence of CHF has been estimated to be 0.6–6.2% in Swedish men with an increase in age [32]. This is similar to the overall prevalence of CHF among both sexes in the Rotterdam population and the Reykjavik Study [33, 34]. The prevalence of CHF is 1–10% in the British outpatient population [35]. It increases considerably when looking at elderly populations, as exemplified by the Italian Campania study, in which the prevalence was 9.5%, underlining the impact of age [14]. It has been estimated that at least 30% of patients with diabetes remain undetected [20]. When screening a Belgian outpatient population with one known cardiovascular risk factor, diabetes was detected in 11% of patients, and an additional 3% had impaired glucose tolerance (IGT) [36]. The prevalence of diabetes was 7.8% in Swedish men and 5.1% in women aged 35 – 79 years, with similar proportions reported in t Finnish middle-aged population [37, 38]. The prevalence of diabetes may be considerably higher in selected high-risk populations, but the lowest among those with CAD. In the Euro Heart Survey, Diabetes and the Heart, patients admitted to the hospital because of acute and stable CAD were investigated for the presence of diabetes and IGT. Only 29% of the 4961 patients had normal glucose metabolism, 31% had known diabetes, and 12% had previously unknown diabetes. The remaining 28% of the patients had IGT [39]. Similar proportions were detected in patients with cerebral and peripheral vascular disease [40]. Thus, the combination of CVD and glucose perturbations is very common but has been understudied in many previous studies because of the lack of diagnostic accuracy in combination with a thorough investigation of the neuro metabolic state.
Considerably less is known about the prevalence of the combination of diabetes and CHF. The most recent and extensive study of the prevalence of diabetes and CHF is that from the In the Reykjavik population [34], the prevalence of the combination of CHF and diabetes was 0.5% in men and 0.4% in women, increasing with age. Diabetes was found in 12% of those with CHF compared to only 3% of the controls without CHF.
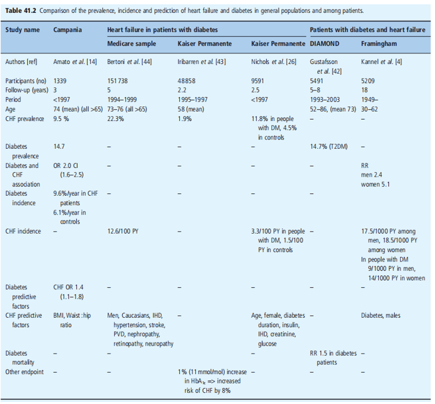
Thus, there was a strong association between diabetes and CHF (Figure 41.1). Based on Framingham data, Rutter et al. [41] noted that the heart is prone to changes in the form of increased left ventricular mass and wall thickness, with worsening glucose tolerance. Kannel et al. [4] and Gustafsson et al. [42] reported on the role of diabetes in CHF from a general and a hospitalized population, respectively. Their findings indicate a strong association between CHF and diabetes. Iribarren et al. [43], Bertoni et al. [44,] and Nichols et al. [26], focusing focus on the role of CHF in patients with diabetes, the prevalence of CHF varies between 1.9 and 22.3%. Finally, Amato et al. [14] found a strong association between diabetes and CHF in orderly population. The outcomes of these studies have been summarized in Table 41.2.
Incidence of CHF and Glucose Abnormalities
Recent results from the Framingham study indicate that the incidence of CHF has declined over the last five decades [45]. However, these data were not supported by other studies [46]. In contrast, hospital admissions for CHF are increasing, resulting in higher healthcare expenditures for patients with this diagnosis [47]. The incidence of CHF has been reported to be 4.4 per 1,000 people in men and 3.9/1000 in women, rising with age in both sexes [48]. The incidence in Finland was similar among men (4.0/1000). person-years, but lower in women at 1.0/1000 person-years [49]. The age-standardized annual incidence of diabetes, reported to be 2.2 and 2.3 per 1000 person-years in Dutch men and women, respectively, are uniform in several European countries [50]. However, when considering an elderly population, as in the Italian Campania study, the incidence was considerably higher at 6.1% per year. This is somewhat different from the observation in the Netherlands, where the incidence decreased in the oldest age group [14, 50] Considerably less is known about the incidence of the combination of diabetes and CHF. Once more, it seems that the most recent and extensive study originated in the Reykjavik population. In this study, the age- and sex-standardized incidences of abnormal glucose regulation were 12.6/1000/year, diabetes 4.6/1000/year, and CHF 5.3/1000/year (Figure 41.2). In addition, there was a strong association between the incidence of glucose abnormalities and CHF [51]. In the Framingham study, the incidence of CHF was twice that among males and five times higher in females with diabetes during the 18 years of follow-up than in patients without diabetes. The excessive risk of CHF remained high even after the exclusion of patients with prior CAD [4]. In the general population of elderly For Italians, the prevalence of diabetes was 9.6% per year in CHF patients [14].
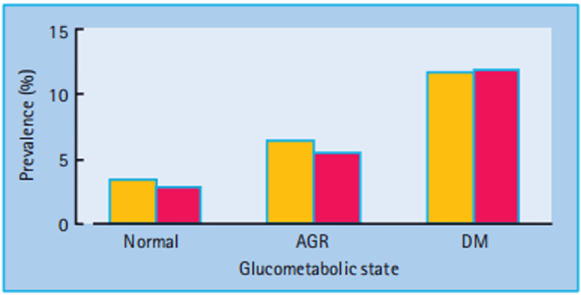
Figure 41.1: Prevalence of congestive heart failure (CHF) in relation to glucose metabolic state. Yellow bars, males; red bars, females; AGR, abnormal glucose regulation; DM, diabetes. Reproduced from Thrainsdottir et al. [34], with permission from American Diabetes Association.
Pathophysiology
Myocardial structural and biochemical alterations can be identical in a failing heart, and many of them seem to be independent of the etiology of myocardial dysfunction. They include Changes in myocardial energy production, altered expression of contractile proteins, de-synchronized
excitation-contraction coupling, adrenergic receptor stimulation, myocytes depletion, and increased activity of several cytokines. Many of these aberrations are found in diabetic hearts. Here, some general features of the pathophysiology are followed by a discussion of additional diabetes-specific factors.
Congestive Heart Failure
CHF is a clinical syndrome originally induced by myocardial damage but is subsequently influenced by the induction of an untoward neuro hormonal response. Thus, norepinephrine, angiotensin II, endothelin, and aldosterone are all linked to the vicious cycle of myocardial remodeling (Figure 41.3), which is unopposed will cause successive deterioration of myocardial performance [52].
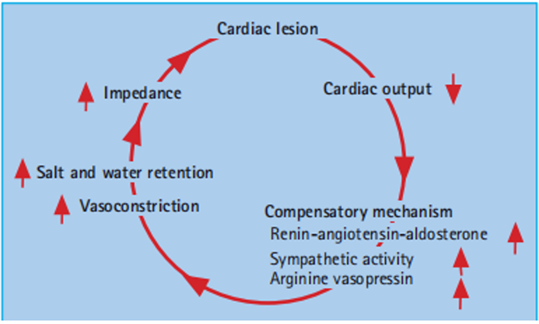
Figure 41.3: Neuro hormonal activation caused by depressed myocardial function leads to a vicious circle further compromising the already compromised myocardial function.
Metabolic conditions play a significant role in cardiac adaptation and remodeling. This leads to an increase of myosin-heavy chain beta, altered troponin T (Tn T) molecules, diminished storage of creatinine phosphatases, and decreased sarcoplasmic ATPase activity, which may result in myocytes hypertrophy associated with impaired contractile function and less effective energy supply [53, 54].
The myocardium has high energy turnover, with ATP as an important source of energy. The two pathways for energy supply are the breakdown of free fatty acids (FFA) and carbohydrates (Figure 41.4). The lipolytic pathway transfers FFA via oxidation to acetyl coenzyme A (ACA), which enters the citric acid or Krebs cycle. The carbohydrate pathway produces pyruvate through glycolysis, glycogenolysis, and lactate oxidation. Pyruvate is decarboxylated via pyruvate dehydrogenase to ACA, which then enters the Krebs cycle. The dominant pathway for myocardial energy production is the oxidation of FFA, but the myocardium is also dependent on glucose oxidation [55].
When the heart is subjected to ischemic stress or exposed to sustained enhancement of intra-ventricular pressure, it tends to change towards more dominant glucose oxidation [56]. This may be counteracted by a reduction of the glucose transporter 4 (GLUT - 4), which becomes reduced in CHF, hampering glucose transport over the cell membrane. At the same time, the heart is subjected to increased FFA concentrations, released via stress influenced by an increased sympathetic tone [57]. It is assumed that prolonged intracellular accumulation of FFA and its metabolites may cause myocardial dysfunction [58].
Besides these mechanisms, alterations in gene expression and inflammatory activity have been suggested to cause metabolic and mechanical disturbances in CHF [59–62] All nucleated cells, including the cardiomyocyte, can produce pro-inflammatory cytokines as a response to injury, such as MI, myocarditis, or when the heart fails. Both tumor necrosis factors α (TNF-) and interleukin-6 (IL-6) levels increase in proportion to the severity and duration of CHF [59,60]. This cytokine release may trigger a cascade of events leading to myocardial structural alterations further deteriorating the clinical picture of CHF.
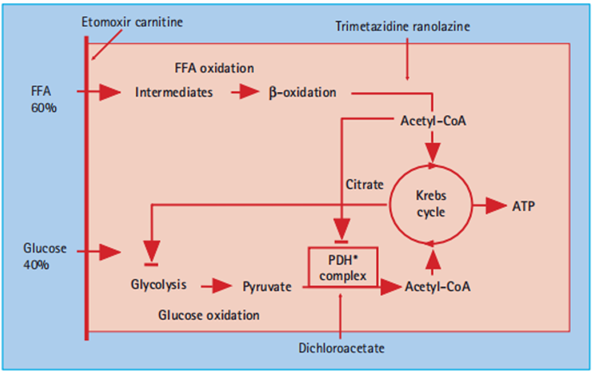
Figure 41.4: Schematic illustration of myocardial energy production of relevance for congestive heart failure (CHF) patients with and without diabetes. The site of action for metabolic modulators are indicated. See text for further information. CoA, co – enzyme A; FFA, free fatty acids; PDH, pyruvate dehydrogenase.
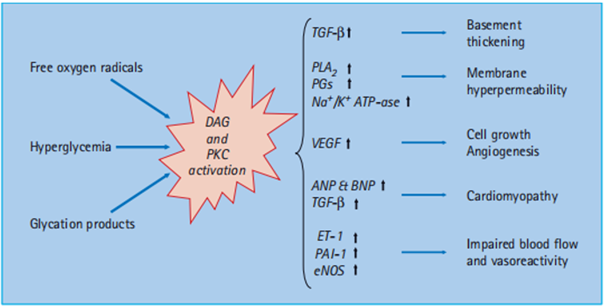
Figure 41.5: Metabolic effects of hyperglycemia induced activation of protein kinase C (PKC) and diacyloglycerol (DAG). See text for further explanation. ANP and BNP, atrial and brain natriuretic peptide; eNOS, endothelial nitrous oxide synthase; ET - 1, endothelin 1; PAI - 1, plasminogen activating inhibitor 1; PG, prostaglandin; PLA 2, phospholipase A 2; TGF - β, transforming growth factor β; VEGF, vascular endothelial growth factor.
CHF and Diabetes
The main myocardial energy production is normally based on the oxidation of FFA (70%) with a smaller contribution from glucose oxidation (30%) and lactate FFA is produced by lipolysis of endogenous cardiac or exogenous stores of triglycerides. Oxidation of FFA is an effective supplier of energy in the form of ATP if the oxygen supply is sufficient. In conditions with limited oxygen availability, glucose oxidation will provide more energy per mole of oxygen and supports more work than FFA [63]. For a person with diabetes, glucose utilization for energy production is substantially lower, about 10% (Figure 41.4). The shift to an even more pronounced oxidation of FFA causes a higher oxygen utilization than under normal circumstances [64]. The major restriction to glucose utilization in the diabetic heart is the slow rate of glucose transport across the sarcolemmal membrane in the myocardium [65, 66]. The impaired glucose oxidation in the diabetic heart can also result from a decreased rate of phosphorylation of glucose, which subsequently limits the entry of glucose into the cell. The depressed phosphorylation is triggered by the increased metabolism of FFA [64]. Insulin deficiency enhances lipolysis, thereby increasing circulating FFA [67].
People with diabetes are also known to increase the risk for other disturbances such as reduced myocardial blood flow and blunted hyper kinetic response to myocardial ischemia, resulting in diminished myocardial function [68–71]. Indeed, CHF is an insulin-resistant state with an increased release of non-esterified fatty acids which are taken up in muscular tissue and downregulate glucose uptake and utilization [72].
Another consequence of hyperglycemia is oxidative stress and activation of processes triggered by an increased level of diacylglycerol and protein kinase C, as depicted in Figure 41.5. Besides, many other unfavorable effects of the increased levels of inflammatory cytokines in heart failure patients may enhance insulin resistance [71,72].
Prognosis
CHF in General
During the past 30 years, mortality from CHD has declined markedly among patients free from diabetes. This decline has been substantially lowering in men but is not seen in women with diabetes [73]. In the presence of CHF, the prognosis becomes poor [74]. In an English population, 1-month survival was 81
Drugs, such as trimetazidine, etomoxir, and dichloroacetate, whose mode of action is to shift myocardial metabolism from oxidation of FFA towards glycolysis have been tested in patients with myocardial dysfunction and diabetes. They act on different parts of the metabolic pathways as indicated in Figure 41.4. Their usefulness must be further explored in clinical trials of appropriate design until their therapeutic role can be considered established despite some.
The research method used for this test was a retrospective evaluation of the scientific records of patients with congestive coronary heart failure (CCHF) over a period of 5–12 months. Information is accumulated from several hospitals and medical institutions, checkbooks, and consultant templates.
The review analyzed scientific data from 500 patients diagnosed with CCHF. Researchers have determined that most cases of CCHF occur in people over the age of 65, with a slightly higher incidence in adult males. The most common comorbidities in patients with CHF were hypertension and diabetes. The evaluation also showed that patients with a history of smoking and obesity had a greater risk of developing CCHF. Additionally, the study found that patients with a family history of coronary artery disease were more likely to develop CCHF. Argument: Results show that CCHF is closely related to distinct lifestyle factors such as age, gender, smoking, and weight problems. The existence of excessive blood pressure and diabetes as common comorbidities underscores the interrelationship between cardiovascular and metabolic diseases. The effect of family history on the risk of CCHF indicates a genetic problem in improving the situation. Moreover, the retrospective method limited the researchers' capability to set up purpose-and-impact dating among risk factors and CCHF. A prospective take a look at with a more extensive and diverse cohorts has to provide more robust proof.
The study highlights essential risk factors related to congestive coronary heart failure (CCHF), together with age, gender, circle of relative’s statistics, smoking, weight problems, hypertension, and diabetes. This information can aid healthcare specialists in figuring out individuals at higher risk for CCHF and imposing preventive measures as a result.
However, further studies are required to discover the mechanisms underlying the relationship between those danger factors and CCHF improvement. Longitudinal tests with larger and more diverse populations may provide a better idea of the progression of CCHF and the effectiveness of prevention and treatment.
This study provides valuable information on the factors involved in CCHF and lays the groundwork for future research on this issue. The data obtained may contribute to the development of targeted interventions aimed at reducing the burden of CCHF and improving patient outcomes, recent promising results.
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project.
We would also like to thank My Mentor Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout the research. Their insights and expertise were instrumental in shaping the direction of this project.
I at this moment declare that, I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Financial support and sponsorship
No Funding was received to assist with the preparation of this manuscript
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
