AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Leticia Raysa Schiavon Kinasz, Universidade Estadual de Campinas (UNICAMP), Campinas, São Paulo, Brasil. Telephone: +55 41 998158181.
Citation: Leticia Raysa Schiavon Kinasz, Rebecca Maunsell, Melissa Avelino, Debóra Bressan Pazinatto, Luciahelena Prata, Miguel Angelo Corrales Coutinho, Lais Botacin, Tiago Henrique de Souza, Marcelo Barciela Brandão, (2023). Congential tracheal stenosis: from diagnosis to surgical treatment, what the airway surgeon must know. Journal of Clinical Otorhinolaryngology 5(1); DOI: 10.31579/2692-9562/054
Copyright: © 2023 Leticia Raysa Schiavon Kinasz. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 December 2022 | Accepted: 10 January 2023 | Published: 23 January 2023
Keywords: tracheal; stenosis; tracheoplasty; congenital tracheal stenosis; children
Congenital tracheal stenosis (CTS) is a rare pathology characterized by complete tracheal rings and may be associated with cardiovascular and pulmonary malformations. Despite its rarity otolaryngologists that perform airway endoscopy and airway surgery must be aware of this malformation since endoscopic manipulation and tracheostomy in these children are of great risk and may jeopardize definite treatment and trigger emergency fatal situation. Meticulous sizing of the airway and recognition of malformations is crucial for diagnosis, staging and surgical planning. Slide tracheoplasty has been described as the gold standard treatment for long segment CTS with low mortality and complications. We report two cases of long segment CTS in toddlers that were surgically treated with emphasis on precise diagnosis and the possibility of concomitant airway malformations in children.
Congenital tracheal stenosis (CTS)
Neonatal Intensive Care Unit (NICU)
Microlaryngobronchoscopy (MLB)
Pediatric Intensive Care Unit (PICU)
Non-invasive ventilation (NIV)
Próton pump inhibitors (PPI)
Computed tomography (CT)
Congenital stenosis (CTS) is a rare pathology representing 0,3-1% of all laryngotracheal stenosis in children[1]. It is characterized by the presence of complete tracheal rings, that is, a tracheal circumference consisting of 360º cartilage instead of the normal 270o [1-4]. Despite its rarity CTS is still more common than acquired tracheal stenosis that may also be encountered in children due to intubation, infections, surgeries (tracheostomies) or aspiration of caustic substances [1,4-6]. This condition is frequently associated with other cardiovascular anomalies and some authors have described that only 10-25% of the cases tracheal are not associated with other malformations. The most common malformation encountered is left pulmonary artery sling and tracheomalacia [1,4,7,8]. Otolaryngologists must be trained to recognize airway malformations and be aware of the possibility of the presence of concomitant lesions. Due to its rarity CTS may be difficult to recognize and inadvertent manipulation of the trachea in this situation can lead potential airway obstruction and seriously compromise further treatment.
The need for treatment is determined by degree of stenosis and clinical symptoms. Some cases may be managed conservatively and tracheal lumen may be sufficient with childs growth [4,9,10]. Since the 80’s various surgical procedures have been reported but in the past 20 years slide tracheoplasty has been elected as the gold standard treatment [1,2,4,5,7-9,11-15]. A resection with end-to-end anastomosis may be considered for short length stenosis nevertheless, when more than a third of the trachea is involved a slide tracheoplasty is nowadays considered the safest procedure.
The authors report two cases with initial diagnosis of more common airway malformations but associated CTS successfully treated with slide tracheoplasty with emphasis to the challenging diagnosis, surgical planning and pos operative care of such cases.
A 17-month-old girl with a history of prolonged stay in the Neonatal Intensive Care Unit (NICU) at birth due to respiratory distress and persistent biphasic stridor since birth was referred to the airway clinic. The child had never been intubated but described recurrent “laryngitis” requiring numerous admissions to emergency services. At initial evaluation a nasofibroscopy reavealed an apparently narrow subglottis (Figure 1a). A congential subglottic stenosis was suspected and a microlaryngobronchoscopy (MLB) was scheduled. Before the MLB 7 months later the child was admitted with fever, coughing, respiratory distress and was intubated in the Pediatric Intensive Care Unit (PICU) with a 4.0 cuffless tracheal tube. After 12 days of intubation a MLB was performed and revealed signs of acute laryngotracheitis with edema and hyperemia and mucosal laceration. Sizing of the airway revealed a grade II subglottic stenosis (Figure 1b) but also an unexpected finding of complete tracheal rings extending through the entire trachea in a “funnel-type” fashion with only two normal rings distally (Figure 1c and d). A computerized tomography was performed and no associated vascular or pulmonary malformations were encountered. After persistent endoscopic and systemic treatment for the secondary laryngeal and tracheal inflammation due to intubation with topical corticoesteroids, systemic corticoesteroids, antibiotics and non-invasive ventilation (NIV) the patient could not be kept more than 12 days without ventilatory support. After team discussion, a slide tracheoplasty was planned despite persistence of mild-moderate airway inflammation.
The slide tracheoplasty was performed in cardiopulmonary bypass as technique revised by Rutter and Manning [16]. The trachea was assessed through a cervicotomy associated with a sternotomy and the airway was exposed from the cricoid to the Carina. After the child was put in bypass a 0degree 4mm and 2.2mm telescopes were used to mark the middle and distal limit of the tracheal stenosis. The trachea was then transected at the midpoint of the stenosis in an oblique fashion, the cranial segment of the airway was split open at the midline of the anterior wall all the way through the anterior cricoid ring to include the subglottic stenosis in the slide, and the distal airway was open posteriorly up to the distal end of the stenosis two rings above the Carina (Figure 1e). The distal segment of the trachea was then slided into the cranial segment and 5.0 PDS running sutures were used for the anastomosis as previously described (Figure1f). At the end of the procedure endoscopic control of the suture as performed and the child was intubated with an age appropriate cuff less tracheal tube. The patient was extubated four days after the procedure and kept on NIV for 10 days. Two control endoscopies were performed on post operative days 7 and 14. On both occasions airway was cleared of secretions, sutures were revised and proven to be adequate, airway was gently calibrated with age appropriate tubes smeared with corticoid ointment and the child was not reintubated. Two weeks after the procedure there was considerable improvement of mobilization of tracheal secretions and intermittent respiratory noise. Antibiotics and a feeding tube were used for 10 days and the child was discharged from the hospital with very mild stridor and no respiratory distress 20 days after surgery. Follow-up 8 months after surgery can be appreciated on Figure 1 g and h, the airway shows no sign of restenosis neither at the subglottic level or trachea, the child is completely asymptomatic with no dysphonia.
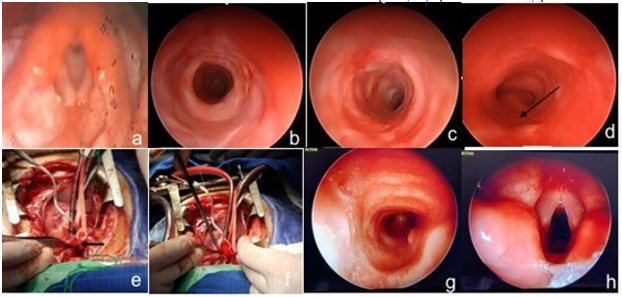
Figure 1 - Case 1: a - nasofibroscopy with the view of a reduced subglottic lumen; b – subglottic stenosis under 4mm telescopic view; c – endoscopic view of the trachea with complete tracheal rings at proximal limit of the CTS with a 4mm telescope; d - endoscopic view of the trachea at the inferior limit the CTS with view of the membranous portion of the adjacent distally normal tracheal rings (black arrow) above Carina; e – Intraoperative view showing the posterior midline incision of the distal trachea (arrow); f – intraoperative view suturing the slided trachea; g- post operative view of the trachea with 4mm telescope at 8 months; h- post operative view of the larynx with 4mm telescope at 8 months.
A female newborn full term was delivered with no complications and developed respiratory distress with retractions and stridor in the delivery room and was put on a 30% oxygen hood. Two days later after no improvement, a nasofibroscopy was performed revealing short ariepiglottic folds and an ômega shaped epiglottis with supraglottic collapse consistent with laryngomalacia. The child was started on próton pump inhibitors (PPI) with no success and continued to present difficulty feeding so at 21 days a MLB was performed. A suprglotoplasty was performed to treat the laryngomalacia but examination of the trachea revealed a long segment CTS with complete tracheal rings in a funnel-shape that did not allow progression of a 4mm telescope nor a 2.5mm tube through its narrowest portion at the midtrachea. A computed tomography (CT) was performed and no other malformations were detected, a new MLB with a 2.7mm telescope was performed confirming a long segment funnel-shaped CTS with two normal distal rings above Carina.
When the child was 4 months old a slide tracheoplasty was performed in cardiopulmonary bypass. The child was extubated three days later after an endoscopic evaluation. Twenty-six days after the surgery a new MLB was performed because the child had persistent mild to moderate retractions and stridor. A slight narrowing was noted at the superior limit of the anastomosis and balloon dilation was performed twice with a three-week interval in an attempt to improve lumen at this point. Two months after the slide tracheoplasty the child still showed signs of mild respiratory distress and a laryngotracheal reconstruction with an anterior cartilage costal graft was performed to address the residual stenosis at the cranial segment of the slide tracheoplasty. The patient was extubated after 3 days with improved respiratory symptoms.
Eighteen months after slide tracheoplasty cartilage graft the child has occasional mild exertional stridor but endoscopic examination reveals no residual stenosis.

Figure 2 – Case 2: A - endoscopic view of complete tracheal rings seen from level of vocal cords; B – intraoperative view of slide tracheoplasty; C – endoscopic view of immediate postoperative aspect of inferior limit of suture with two normal distal tracheal rings; D – immediate endoscopic postoperative view of tracheal suture line; E – endoscopic view of restenosis at superior limit of suture line 26 days after surgery; F – endoscopic view of anterior tracheal costal cartilage graft.
Tracheal stenosis is a rare entity and is of high risk if not diagnosed. CTS is classified into four main types following Grillo [10]. generalized tracheal hypoplasia (type I), funnel-shape tracheal narrowing (type II), segmental tracheal stenosis (type III) and bridge-bronchus stenosis (type IV). Patients may be asymptomatic or mildly symptomatic symptoms may be present and significant in the first days/weeks of life, and as in the case 2, or later as in case 1 [2,10,18]. The most characteristic manifestations include: biphasic stridor sometimes described as “washing-machine noise”, coughing, repeated acute respiratory events, cyanotic spells and respiratory distress [2,4,18,19]. Diagnosis as always in cases of persistent or recurrent stridor is confirmed with airway endoscopy. When complete tracheal rings are identified on endoscopy, imaging is important to exclude associated cardiac, vascular and lung malformations that may occur roughly in 50% of cases [2,12,18-20]. In some cases, bronchography may be useful to fully evaluate the segment distal to the narrowing particularly if an endoscope cannot progress. Concomitant airway anomalies such as congenital subglottic stenosis and laryngomalacia as described in the case reports are much more frequent than CTS. The importance of adequately and skillfully evaluating the pediatric airway cannot be stressed enough, this requires training, documentation and repeated exposure to a good number of cases considering the rarity of some of these malformations.
In a minority of cases surgery may not be needed and the patients may be followed with reevaluations to check on the expansion of the tracheal lumen with growth and worsening of symptoms. A recent study by Yamoto et al has proposed follow up with CT reconstruction that might help define which cases are candidates for surgery [21]. These authors suggest that, if the diameter of the narrowest part of the airway is not smaller than 40% and symptoms are not significant there may not be a need for surgical repair. Another criteria for conservative management according to these authors would be a trachea with a lumen not less than 2.7mm at its narrowest point.
The first surgical approach proposed for CTS in 1982 by Idriss et al was a pericardial graft to perform an enlargement tracheoplasty [2,8,9,18,22]. Since then several techniques have been used such as primary resection and anastomosis, tracheoplasty with autologous and homologous grafts, balloon dilation and stenting and laser sectioning [2-6,12,14,20]. In 1989 Tsang et al described the slide tracheoplasty that was then popularized by Grillo et al [2,4,8,12-18,20]. This has been the gold standard surgery for long segment CTS due to its versatility, use of the patients tracheal tissue and low rate of complications, reinterventions and mortality (less than 5%) [1,2,4-8,11,14]. The slide tracheoplasty doubles the trachea’s circumference, quadruples its diameter and reduces its length by half [24]. Complication rates are low but consist of: granulation tissue in the suture sites an “eight-shape” deformity, suture dehiscence and restenosis [2,4,7]. In 2003 Rutter and Manning [25] reported that after two years using this technique as there first choice for CTS it could be considered superior to other techniques they had used previously. Mortality rates have been decreasing as reported my large series from Cincinatti and London from 30% to 5%. Zenner et al reported that when CTS is associated to Syndromes such as Down, VATER/VACTERL and Apert repairing is more challenging [4,26].
When cardiac malformations are associated these should be corrected preferably at the same time as the slide tracheoplasty [19,21] reinforcing the need of an airway team where otolaryngologists and or dedicated airway and cardiovascular surgeons are integrated. Elliot et al, described association of left pulmonar artery sling in 60% of their cases [27]. In 2016, the Cincinnati group described lung malformations in 18 (13,8%) of their 130 patients submitted to slide tracheoplasty amongst these unilateral pulmonary agenesia was the most frequent finding (61%) followed by unilateral lung hypoplasia (39%).
Tracheostomy should be avoided since it increases the risk of complications, compromises surgical repair of the stenosis and increases risk of granulation tissue, obstruction and death [19,26]. This is why the importance of airway endoscopy cannot be underestimated when considering a tracheostomy for children with respiratory symptoms. As described in both cases there may be coexisting airway pathologies and/or malformations (congenital subglottic stenosis in case 1 and laryngomalacia in case 2) therefore it is essential that the airway endoscopist and /or surgery be familiar with all possible anomalies. Airway endoscopies may need to be repeated with smaller endoscopes as was done in case 2. More narrow stenosis may require bronchographies to further “map” the airway and plan the best surgical approach. In case 1 surgical planning to include the cricoid in the slide was essential or the child would have been left with subglottic stenosis after the slide. In case 2 sizing of the airway post operatively was also essential in recognizing the need for further expansion of the airway after the slide tracheoplasty.
Due to its rarity, large case series of CTS are limited to major international pediatric airway reference centers that have reported over 100 cases [4,6,8,11,24]. Large case series have not been reported in Latin America. Terra et al in 2000 published their results in 7 children surgically treated for CTS but only one was a slide tracheoplasty28. The interest in reporting these two cases is particularly an alert to this probably underdiagnosed pathology. Surgeons must bare this diagnosis in mind, take great care when manipulating complete tracheal rings and particularly when considering a tracheostomy. Airway surgeons must be mindful of the appropriate airway size for the child and size the airway even when treating other airway conditions and ideally be exposed and trained to be familiarized with these rare anomalies.
Surgical success of airway malformations is a result of: precise diagnosis, surgical technique and post-operative management and this is why team evaluation and discussion is paramount: from the otolaryngologist to the thoracic and cardiac surgeon, anesthesiologist and intensive care staff [6,9,12,17,21,24].
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
