AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Vivek Kumar, Indraprastha Apollo Hospitals, New Delhi, India.
Citation: V Kumar, V Arora. (2022). Conduction system pacing: basis and scope. Cardiology Research and Reports. 4(1); DOI: 10.31579/2692-9759/030
Copyright: © 2022 Vivek Kumar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 November 2021 | Accepted: 08 December 2021 | Published: 03 January 2022
Keywords: right ventricular pacing; heart failure; heart failure hospitalization
Long-term right ventricular pacing (RVP) is associated with more cardiovascular death, atrial fibrillation (AF), thromboembolic complications and heart failure(HF). RVP often results in prolonged QRS duration(QRSd) and ventricular desynchronization.
The ventricular desynchronization as a result of RVP leads to an increased risk of heart failure
hospitalization (HFH) and AF, and this effect is dependent on cumulative percent ventricular paced ( % VP). In the sub-study from the MOST trial, it was evident that % VP >40% was associated with a 2.6-fold increased risk of HFH compared with pacing < 40% of the time despite preserved atrioventricular synchrony. Moreover this adverse effect of RVP induced ventricular desynchrony was more pronounced in patients with left ventricular ejection fraction( LVEF) of 40% or less resulting in increased death or HFH.
AF = Atrial fibrillation
AV = atrioventricular
BBB = Bundle branch block
BVP = Bi-ventricular pacing
CRT = Cardiac resynchronization therapy
CSP = Conduction system pacing
HBP = His bundle pacing
HF = Heart failure
HFH = heart failure hospitalisation
HFrEF = Heart failure with reduced ejection fraction
HOT-CRT = His -Optimised CRT
HPS = His Purkinje system
HPCD = His-Purkinje conduction disease
HV = His to ventricular electrogram interval
LBBB = left bundle branch block
LBBAP = Left bundle branch area pacing
LOT-CRT = LBBP optimised CRT
LV = left ventricle/ventricular
LVEF= Left ventricular ejection fraction
LVSP = Left ventricular septal pacing
NS-HBP = Non selective HBP
PGR = Pulse generator replacement
% VP = Percent ventricular paced
QRSd = QRS duration
RBBB = right bundle branch block
RV = Right ventricle
RVP = Right ventricular/ventricle pacing
SND = SA nodal disease
S-HBP = Selective HBP
Long-term right ventricular pacing (RVP) is associated with more cardiovascular death, atrial fibrillation (AF), thromboembolic complications and heart failure(HF) [1]. RVP often results in prolonged QRS duration(QRSd) and ventricular desynchronization.
The ventricular desynchronization as a result of RVP leads to an increased risk of heart failure hospitalization (HFH) and AF, and this effect is dependent on cumulative percent ventricular paced ( % VP). In the sub-study from the MOST trial, it was evident that % VP >40% was associated with a 2.6-fold increased risk of HFH compared with pacing < 40>
Alternate RV sites, like mid septal or right ventricular outflow tract (RVOT) septal pacing have so far shown conflicting data in terms of QRSd narrowing as well as hemodynamic and clinical outcomes [4]. Strategies to reduce the percentage of RV pacing include algorithms that promote AAI(R) mode permitting first degree or Mobitz Type 1 heart block to occur. But it may not be effective in reducing %VP in patients for whom VP is inevitable (e.g.complete heart block, AF with bradycardia). Even programming a long fixed AV delay above baseline PR interval though promotes intrinsic AV conduction to occur, but still results in % VP > 50% to occur in 88% of patients due to PR prolongation on exercise [5].
These considerations have led to the recommendation of cardiac resynchronization therapy (CRT) in patients needing pacemaker if there is left ventricular (LV) dysfunction.6 But the patients with normal LV function and indication for pacing are predominantly offered conventional pacing strategy with RVP. Of late conduction system pacing (CSP) has come up as a promising pacing strategy gaining acceptance worldwide. CSP involves implanting pacing lead targeting at various levels in the conduction system that includes His bundle and left bundle branch area. The idea is to circumvent AV block and achieve synchronized biventricular activation.
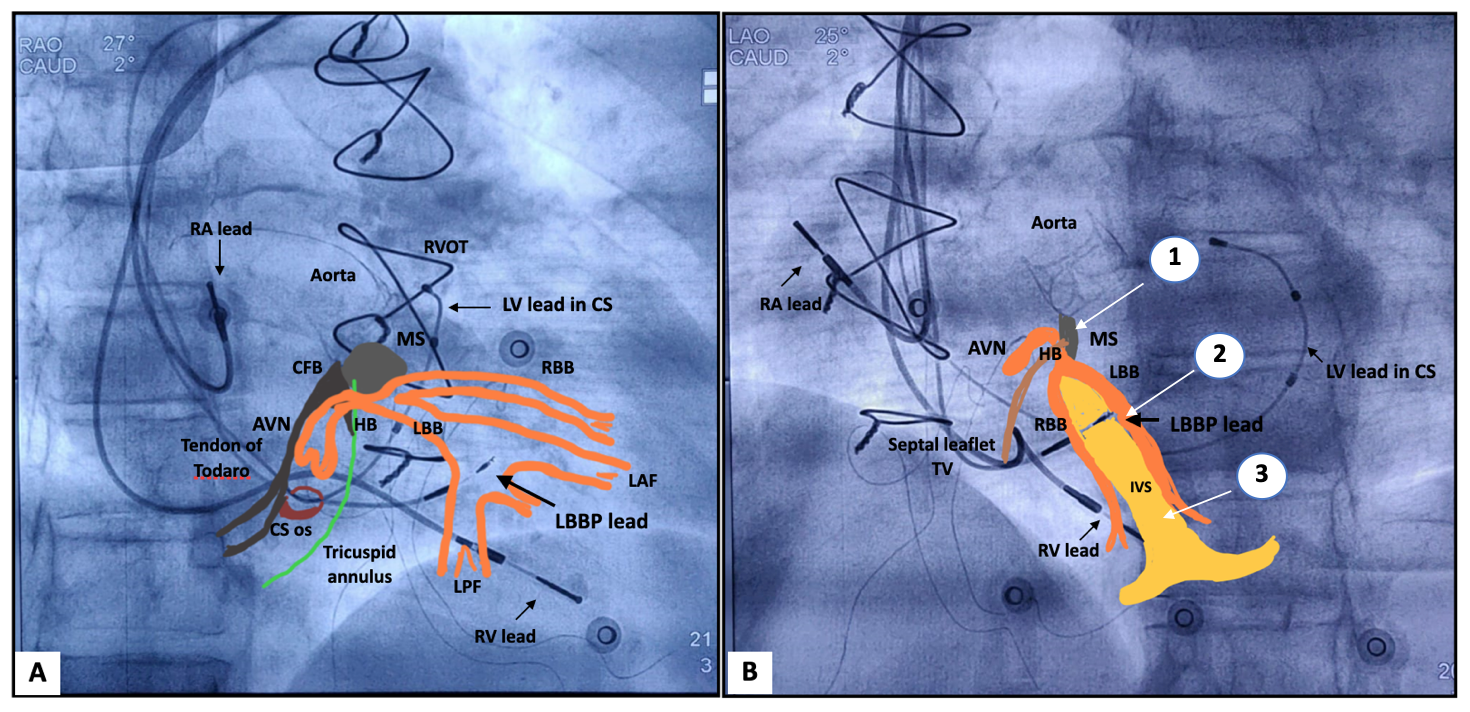
The compact AV node lies in the superficial paraseptal endocardium of the inferior right atrium. It is located along the septal portion of the tricuspid valve annulus towards the apex of the triangle of Koch. The His bundle arises as an anterosuperior extension from the compact AV node and passes into the central fibrous body of the septum. As It emerges out of the central fibrous body, it lies along the posterior and inferior margins of the membranous interventricular septum. Anatomical variations are common as the penetrating part of His bundle courses, commonly it is on the right-side of the membranous septum, but can be on the left side or course under the membranous septum just below the endocardium. 7 After a short course (5-10 mm), the His bundle bifurcates into the right bundle (RBB) and the left bundle (LBB) at the crest of the muscular septum. The RBB is thin and compact, and courses down the right side of the interventricular septum anteriorly. RBB does not divide throughout most of its course until it approaches the base of the right anterior papillary muscle at the distal septal surface.
The left branch traverses the membranous septum and appears between the non-coronary and right coronary aortic cusps. The Left bundle is compact in the proximal 1 to 2 cm and it courses down in the subendocardium of the septal surface of the left ventricle. It then fans into an anterior (superior) fascicle (LAF) and a posterior (inferior) fascicle (PAF). The LAF courses towards the anterior-superior papillary muscle, and the LPF toward the posterior-inferior papillary muscle. Variably the proximal LBB also gives rise to Purkinje fibers to the septum, called the Septal fascicle.8 As the tricuspid valve is more apical than the mitral valve and septal leaflet of the tricuspid valve is attached to the membranous septum. The proximal part of the His bundle rests on the right atrial–LV portion of the membranous septum, and the distal His lies along the RV-LV portion of the membranous septum (Figure 1).
The targets for conduction system pacing are the His bundle (Both the atrial and ventricular portions of the His bundle) and the Left bundle branch area. In SA nodal disease (SND) where the AV node -His bundle Purkinje system is relatively disease-free, it is obvious that if His bundle is paced it will result in QRS morphologically identical to the baseline QRS. Interestingly in early experiments, it was shown that His bundle pacing (HBP) can even result in correction of bundle branch block(BBB) [9]. This was considered as a proof of concept for the proposed hypothesis of Longitudinal dissociation in the His bundle. It was Kaufmann and Rothberger who first postulated the idea of functional longitudinal dissociation in 1919 [10] The theory proposes that fibers destined for respective bundle branches are prefixed and bundled in the proximal His bundle. In the majority of cases, the bundle block manifestation is not a result of conduction delay in the anatomical bundle distally but as a result of conduction delay in proximal fibers. So pacing distal to the block result in normalization and narrowing of QRS morphology [11]. The anatomical basis to this hypothesis was given by James and Sherf in 1971 [12]. They observed that cells in His bundle were mainly arranged longitudinally and separated by fine collagen with minimal cross-connection. They gave an impression of parallel insulated channels for conduction and the bulk of cells were destined for the left bundle.
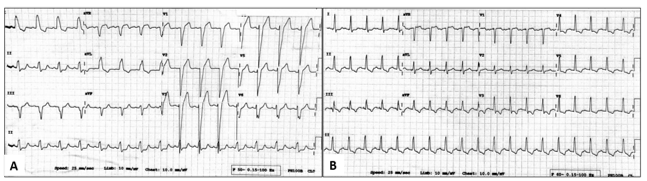
Interestingly it is observed that even in presence of evident distal block (LBBB with left axis deviation) [13].HBP can result in correction of block indicating additional mechanisms at play. It has been observed that there is some degree of output dependence during distal HBP. High output stimulus in the His area corresponds with a larger area of capture, thereby reaching beyond the block.14 It can recruit normal conducting fibers adjacent to abnormal myocardium causing the functional block. This will
give an impression of non-selective HBP and the result would be normalization of BBB. (Figure 2) An alternate theory is based on the concept of “virtual electrode polarization”, initially demonstrated in the mechanism of defibrillation [15]. The delivery of stimulus results in ion changes locally. If the stimulus is of sufficient strength it can create an electric dipole (with an anode and cathode), which can redistribute charges and increase the reach of the implanted pacing lead. Thereby recruiting fibers distal to the block and result in successful HBP. Because of anatomical and electrophysiological factors, it is not surprising that the average HBP threshold is higher than conventional pacing sites [16]. A His bundle capture threshold of < 2>
In HBP, short AV delay needs to be set equivalent to native AH interval. Depending upon the lead position and His bundle anatomy ( intramyocardial, naked, or covered with fibrous tissue) [18]. HBP may be selective ( S-HBP) or nonselective (NS-HBP). In S- HBP the ventricular activation happens solely through the His Purkinje system (HPS), so the stimulus to ventricular activation (SV) interval is either equal to the native HV interval or even shorter than HV as in the case of BBB or proximal HV block. The QRS morphology is the same as the native QRS morphology but in the case of BBB, it may result in correction of the block with a narrower QRS duration. NS-HBP results in additional activation of the septal myocardium. On electrogram, it is manifested as a pseudo-delta wave just after stimulus so the QRS duration will usually be longer than the native QRS. It may still result in correction of BBB and narrower QRS in HPCD.17 S-HBP intuitively looks preferable over NS-HBP, but the published data indicate that the clinical and hemodynamic outcomes are comparable [19].

The other target for physiological pacing is the LBB area pacing (LBBAP) and the recent left septal pacing. Huang et al [20] first reported successful direct LBBAP after a failed HBP in a patient with heart failure and LBBB. It resulted in the correction of LBBB and also improvement in heart failure. LBB is accessed by deep penetration of pacing lead trans-septally from the RV side towards the subendocardium of the septal surface of the left ventricle. Since the LBB is compact in proximal 1-2 cm and then fans out, it gives a larger target area to achieve successful pacing. The optimal site is around 1–1.5 cm below the His bundle along an imaginary line drawn from distal His signals to RV apex in RAO 30°[21]. LBBAP usually results in incomplete RBBB pacing, RBBB pattern with relatively longer QRS suggest of left ventricular septal pacing. In LBBP the AV delay has to be programmed 20–30ms less than the nominal values as it takes 20–30ms for the impulse to reach the ventricular myocardium after LB potential [22].Concerns regarding the theoretical risk of LV–RV dyssynchrony due to RBBB induced by LBBAP can be sorted by programming the output above the anodal threshold ( the ring of lead lies over the RV septum, result in anodal captures of the right side of the septum) or optimizing the AV delay to allow native fusion (allowing partial conduction through RBB). If his bundle is relatively disease-free RBB can also be captured retrogradely. (Figure 3)
Recently in a proof of concept study temporary left ventricular septal pacing (LVSP) pacing was shown to provide short-term hemodynamic improvement and electrical resynchronization, which was shown to be as good as during BiV and possibly comparable to HB pacing [23]. The concept of LVSP pacing originates from the fact that in a normal heart the LV septal area is the earliest to depolarise by septal fascicles, so LVSP would provide a near-physiological activation. In an earlier study, Mafi-Rad et al. demonstrated the feasibility of transvenous LVSP using a modified version of the Medtronic 3830 lead (Medtronic, Dublin, Ireland), with a long 4-mm screw in patients with sinus node dysfunction [24].Permanent placement of an LVSP lead by transvenous approach through the interventricular septum is feasible in patients. LVSP preserves acute left ventricular pump function. This new pacing method could serve as an alternative and hemodynamically preferable approach for antibradycardia pacing.
An initial feasibility study by Deshmukh et al [25]. paved the way for achieving transvenous permanent HBP in patients. He could achieve successful HBP in 12 of 18 patients with atrial fibrillation undergoing AV node ablation. Similar results were demonstrated in a larger series of patients with acute improvement in hemodynamics, improvement in LVEF, and exercise performance during a mean follow-up of 42 months [26]. Initial studies were done using conventional hardware with a manually shaped stylet to access His bundle area, but with later development of specialized hardware( like 3830 Select Sure Lead & C315 preshaped catheter, Medtronic Inc., Minneapolis, MN, USA) the technique gained popularity and the learning curve improved resulting in better acute results [27]. Further it was shown by Catanzariti et al [28].that HBP mode compared to RV pacing, resulted in marked improvements in echocardiographic indices of ventricular synchrony, LVEF, and reduction in mitral regurgitation. It was the first demonstrated evidence of physiological superiority of HBP as it does not induce ventricular dyssynchrony like conventional right ventricular apical pacing.
Initial studies did establish HBP as an alternative strategy for antibradycardia pacing but still, limited data was available regarding its medium to long-term clinical outcomes. Sharma et al [29]. first reported encouraging evidence in favor of HBP over RVP in patients requiring pacemaker implantation. At 2 year follow-up, HBP resulted in significant reduction in HFH in patients with % VP > 40% ( 2% vs 15%, P=0.02). The extending follow-up of 5 years in the above cohort, demonstrated a reduction in both HFH and death (32% vs 53%; hazard ratio 1.9; P = .04). As was expected because of the higher pacing threshold needed in HBP at baseline as well as an increase in threshold over time, the need of pulse generator replacement (PGR) was more with HBP compared to RVP ( 9% vs 1%). Also, lead revision was done in 6.7
The traditional method to achieve cardiac resynchronization is placing an LV lead in the posterior or postero-lateral vein of the coronary sinus and additional lead in RV (BVP). Randomized studies have already established BVP as an effective therapy in addition to guideline-directed medical therapy for improving morbidity and mortality in heart failure with reduced ejection fraction (HFrEF) [37,38]. The ideal patients for BVP are patients having wide QRS with LBBB. BVP is not without limitations, about 30% of patients having BVP are either poor responders or nonresponses [37,39]. The procedure itself is technically challenging and is further limited by anatomical factors like lack of suitable venous branches, phrenic nerve stimulation, and high pacing thresholds. And there is a certain subgroup of patients of HFrEF, such as patients with normal QRSd and RBBB, who do not derive benefit [40]. CSP offers an option as a single lead solution instead of two leads for CRT and may offer an alternative in anatomically difficult subsets for BVP-CRT.
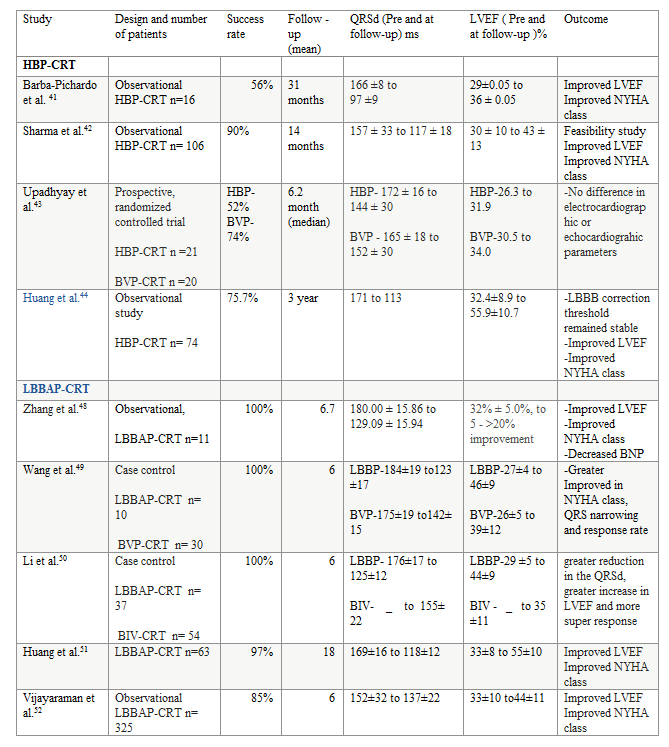
HBP can correct bundle branch block ( both LBBB and RBBB) by recruiting LBB or RBB fibers distal to the block, effectively narrowing QRSd and will result in correction of electro-mechanical dyssynchrony. The data supporting HBP for CRT are primarily from single or multi-centric observational studies. The studies were done in patients with indication for CRT and had reported success rates varying from 56% (9 in 16 patients ) [41]. in the earliest reported study to 90% (95 of 106 patients) in a recently reported study 42. Indicating a role of evolving technique and hardware. These studies have consistently shown a significant narrowing of QRSd and correction of LBBB, improvement in functional class and LV function, and better quality of life. In one of the first multicenter prospective, randomized controlled trials, Upadhyay et al [43]. enrolled a total of 41 patients with severe LV dysfunction with indication for CRT into the His-CRT group(n=21) versus BVP-CRT group(n=20 ). 65% of the patients were having coronary artery disease and mean QRSd 168 ± 18 ms [left bundle branch block pattern = 35, right bundle branch block = 2, paced = 3]. At a median follow-up of 6.2 months, significant improvements in median LVEF relative to baseline were seen in both His-CRT and BVP-CRT patients. His-CRT was not superior to BiV-CRT with regard to LVEF improvement (median +9.1% [IQR: 5.0% to 14.4%] vs. +5.2 [IQR: 1.5% to 11.3%]; p = 0.33) or rate of echocardiographic response ≥5% (76% vs. 53%; p = 0.13). The study was underpowered and was limited by a high crossover rate. Crossover occurred in 48% of patients in the His-CRT group and 26% of patients in the BiV-CRT group. The most common reasons for crossover from His-CRT were the inability to correct QRSd(n = 5), among them, one-half of patients exhibited nonspecific intraventricular conduction delay (IVCD), which is unlikely to be corrected by His-CRT alone. Most of the data for His-CRT is from short-term to mid-term follow up, recently long-term outcome data was published for patients with HFrEF and LBBB (n=74). In this single-center prospective observational study, HBP was successful in 75.7% of the patients. There was a significant improvement in LVEF( super-responder) and NYHA class. The HBP threshold for LBBB correction remained stable at 3-year follow-up (with an acute threshold of 2.13 ± 1.19 V/0.5 ms and 2.29 ± 0.92 V/0.5 ms at follow-up) [44].
IVCD poses a limitation for HBP particularly if there is no His-Purkinje conduction disease (HPCD) and more of myocardial cell-to-cell conduction delay. In such situations, a strategy of HBP in conjunction with sequential LV pacing termed as His -Optimised CRT ( HOT-CRT) may be effective. HOT-CRT was evaluated in a small series of patients with LBBB/IVCD by Vijayaraman et al [45]. in whom HBP alone was not effective ( n= 27). These patients underwent additional LV epicardial lead implantation, resulting in improved electrical resynchronization when compared with conventional BVP or HBP alone. 84% were clinical responders while 92% showed an echocardiographic response. BVP-CRT is not effective in a subgroup of patients of HFrEF with Right Bundle Branch Block (RBBB) if there is no pacing requirement. HBP can correct RBBB and restore RV-LV synchrony. Does HBP will help in patient of HFrEF and RBBB was evaluated by Sharma et al [46].In this retrospective observational study it was shown that HBP resulted in a significant narrowing of QRS from 158 ± 24 ms to 127 ± 17 ms (p=0.0001), with an improvement in LVEF (31 ± 10% to 39 ± 13%) (p=0.004). The overall success rate of HBP was 95% (37 of 39 patients) and complete correction of RBBB could be achieved in 78% of cases. This was the first study indicating that HBP-CRT may be a promising strategy in patients with RBBB and HFrEF.
HBP has its limitations as discussed above and not surprisingly left bundle branch area pacing (LBBAP) is being touted as a promising alternative to BVP-CRT. No doubt LBBAP will be more effective in overcoming LBBB than HBP alone and it has been shown to achieve comparable LV activation times and synchrony parameters [47]. The theoretical LV-RV dyssynchrony resulting from LBBAP can be mitigated to large extent by optimal programming. In the first feasibility study reported by Zhang et al [48]. In 11 patients with CRT indication. LBBAP resulted in significant narrowing in the QRSd as well as improvement in LVEF with a decrease in BNP level in a mean follow-up of 6.7 months. Subsequent case-control studies have consistently shown significant QRS narrowing, and greater LVEF improvement and percentage of echocardiographic response in patients with LBBAP compared with BVP in short and medium-term follow-up [49,50] Huang et al [51]. reported 97% success with low and stable pacing threshold with LBBAP in medium-term follow-up in non-ischemic cardiomyopathy CRT candidates. In addition to improvement in LVEF and functional class, they reported no deaths or heart failure hospitalizations during follow-up. In a recently published multi-centric retrospective, observational study including 325 patients with CRT indication where LBBAP was attempted. LBBAP was successful in 85% of the patients and the pacing parameters were stable during a mean follow-up of 6 ± 5 months. The results were consistent with previously reported smaller studies. The super response was more frequent among nonischemic cardiomyopathy patients than ischemic patients (41% vs. 18%; p < 0>
Very recently LVSP has also been proposed as an alternative to BIV-CRT, as mentioned above, in a proof of concept study it has shown to preserve mechanical synchrony and improved hemodynamics. Anecdotal case reports have shown favorable results.53 Similar to the HOT-CRT strategy, LBBP optimized CRT (LOT-CRT) can be used for patients not deriving optimal QRSd narrowing with LBBAP. Non-responders to BIV-CRT are an important group of patients in need of therapeutic remedies. CSP has shown improvements in LVEF and NYHA functional class in small studies of BIV-CRT non-responders [42-54].
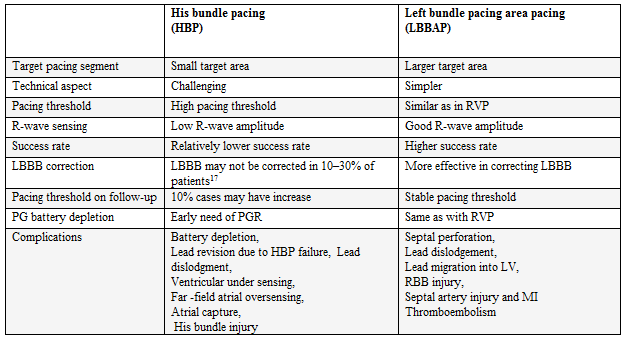
As per the recent 2018 ACC/AHA/HRS guideline, HBP has been given a class IIa indication in patients with pacemaker requirements with LVEF < 50> 40%.6 For patients with normal LVEF irrespective of pacing requirement, still there are no guideline-directed indications for CSP. Regarding LBBAP still it does not find an indication in the guidelines. The accumulating experience and the available data though mostly from non-randomized studies make a case for both HBP and LBBAP. It is expected that future guidelines updates may incorporate more indications for CSP. CSP for CRT looks most promising as per the evidence, it gives a single lead solution for achieving cardiac synchronization in most of the eligible CRT patients. Comparison of HBP and LBBAP puts LBBAP at an advantageous status as per the short and medium-term follow-up data. (Table 3) The most significant limitation with HBP is the inability to achieve a low pacing threshold and sub-acute increase in threshold resulting in more PGR in long-term follow-up. In a multicentric study on HBP for CRT significant increase in HBP threshold (>2 V increase in capture threshold from implant or capture threshold >5 V at 1 ms) was observed in 7.4
For patients with LV dysfunction requiring pacemaker implantation and those who are candidates for CRT, CSP has the potential to become alternative therapy of choice.
Antibradycardia therapy with HBP seems limited by its high threshold of pacing particularly in relatively younger patients, as they may require repeated PGR. LBBAP including LVSP looks promising in patients requiring pacing because of bradycardia. Work is needed to develop dedicated sensing algorithms to reduce far-field atrial sensing and to bring modified His specific pacing systems to improve pacing thresholds and stability. Similarly, specific modifications are needed for LBBAP particularly in terms of hardware. The systems presently used for HBP or LBBP were initially designed for RV pacing ( the lead and catheter ). So dedicated system is the need of the hour and thankfully some new dedicated systems are already available in some parts. Additionally, despite the current evidence, we need further long-term data in form of prospective randomized clinical trials to establish the definite role of each of the CSP modalities. HBP or LBBAP or LVSP, when and where?
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
