AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Gian Maria Pacifici, Associate Professor of Pharmacology, via Sant’Andrea 32, 56127 Pisa, Italy.
Citation: Gian M. Pacifici (2021) Clinical pharmacology of sildenafil in infants and children. J Pharmaceutics and Pharmacology Research 4(4), DOI: 10.31579/2693-7247/045
Copyright: © Gian Maria Pacifici, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 August 2021 | Accepted: 23 September 2021 | Published: 09 October 2021
Keywords: sildenafil, dosing, efficacy and safety, effects, adverse-effects, pharmacokinetics, drug-interaction, metabolism, treatment, placenta, breast-milk, infants, children
Sildenafil is a competitive and selective inhibitor of phosphodiesterase 5. Sildenafil is cleared by hepatic CYP3A (major route) and CYP2C9 (minor route) and concomitant administration of potent CYP3A inducers (e.g., bosentan) causes decreases in plasma levels of sildenafil. CYP3A4 inhibitors (erythromycin and cimetidine) inhibit sildenafil metabolism prolonging the half-life and elevating blood levels of sildenafil. Sildenafil is a pulmonary arterial vasodilator and it has been used in the treatment of persistent pulmonary hypertension. The initial oral dose is 250 to 500 µg/kg 4 times-daily in infants and the oral dose is 10 to 20 mg thrice-daily in children with a body-weight up to 20 kg or > 20 kg, respectively. Sildenafil has been found efficacy and safe in infants and children but it may induce adverse-effects. Following an oral dosing, the absorption rate constant is 0.343 h-1, and the elimination half-life is 2.41 hours in children suggesting that sildenafil is rapidly absorbed and eliminated. The interaction of sildenafil with drugs and the metabolism of sildenafil have been extensively studied. The principal routes of sildenafil metabolism are: N-demethylation, oxidation, and aliphatic dihydroxylation, and the major metabolite is N-desmethyl sildenafil. The treatment of infants and children with sildenafil has been extensively studied. Sildenafil citrate and sildenafil cross the human placenta and sildenafil migrates into the breast-milk in significant amounts. The aim of this study is to review the sildenafil dosing, efficacy and safety, effects, adverse-effects, pharmacokinetics, interaction with drugs, metabolism, treatments, and sildenafil placental transfer and migration into the breast-milk.
Mechanism of action of sildenafil
Sildenafil, which structurally mimics the purine ring of cGMP, is a competitive and selective inhibitor of phosphodiesterase 5. Sildenafil has a relatively high selectivity (>1,000-fold) for human phosphodiesterase 5 over other phosphodiesterases. By inhibiting cGMP hydrolysis, sildenafil elevates cellular levels of cGMP and augments signalling through the cGMP-protein kinase G pathway, provided guanylyl cyclase is active [1].
Administration distribution metabolism and excretion of sildenafil
Sildenafil is rapidly absorbed and reaches a peak plasma concentration 1 hour after oral administration. Sildenafil is cleared by hepatic CYP3A (major route) and CYP2C9 (minor route). Sildenafil and its major active metabolite, N-desmethyl sildenafil, have terminal half-lives of about 4 hours in adults. Both the parent compound and the major metabolite are highly bound to plasma protein (96%). Metabolites are predominantly excreted into the faeces (73 to 88%) and to a lesser extent into the urine; non-metabolised sildenafil is not detected in urines or faeces. The clearance is reduced in elderly (> 65 years), leading to an increase in the AUC values for the parent drug and the N-desmethyl metabolite [1].
Clinical use and adverse-effects of sildenafil
Sildenafil, 5 to 20 mg thrice-daily improves exercise capacity, functional class, and hemodynamics. In addition, improved exercise capacity and hemodynamic parameters, sildenafil (initiated at 20 mg thrice-daily, titrated to 40 to 80 mg thrice-daily) plus long-term epoprostenol therapy also resulted in delayed time to clinical worsening of PAH in clinical studies. Dose adjustment for reduced renal and hepatic function is usually not necessary except for severe hepatic and renal impairment. Concomitant administration of potent CYP3A inducers (e.g., bosentan) will generally cause substantial decreases in plasma levels of sildenafil. The mean reduction in the bioavailability of sildenafil (80 mg thrice-daily) when co-administered with epoprostenol was 28%. CYP3A4 inhibitors (e.g., protease inhibitors used in HIV therapy, erythromycin and cimetidine) inhibit sildenafil metabolism, thereby prolonging the half-life and elevating blood levels of sildenafil. Consistent with its mechanism of action, potentiation of cGMP signalling, sildenafil and other phosphodiesterase 5 inhibitors potentiate the hypotensive effects of nitrate vasodilators, producing dangerously low blood pressure. Thus, the administration of phosphodiesterase 5 inhibitors to patients receiving organic nitrates is contraindicated. In any event, the patient’s undergoing cardiovascular status and concurrent use of hypotensive agents (e.g., nitrate vasodilators, α adrenergic antagonists) must be considered prior to use of this class of drugs. Headache (16%) and flushing (10%) are the most frequently reported adverse-effects. Patients taking sildenafil or vardenafil may notice a transient blue-green tinting of vision due to inhibition of retinal phosphodiesterase 6, which is involved in phototransduction [1]. Sildenafil is used as a pulmonary artery vasodilator in infants and children with primary post-surgical pulmonary hypertension. It is also being used to treat persistent pulmonary hypertension of the newborn infant, and to wean them from inhaled nitric oxide treatment [2]. Sildenafil is used for the treatment of persistent pulmonary hypertension, and the retinal vascularity must be established before sildenafil is used in extremely preterm infants. Sildenafil is contraindicated in infants taking organic nitrates in any form and in infants with a known hypersensibility to sildenafil. The monitoring of blood pressure and oxygenation should be continuously performed [3].

Literature search
The literature search was performed electronically using PubMed database as search engine and the following key words were used: “sildenafil dosing infants, children“, sildenafil efficacy, safety infants, children”, “sildenafil effects infants, children, “sildenafil adverse-effects infants, children”, “sildenafil pharmacokinetics infants, children”, “sildenafil drug interactions”, “sildenafil metabolism”, “sildenafil treatment infants, children”, “sildenafil placental transfer”, and “sildenafil migration into the breast-milk”. In addition, the books: The Pharmacological Basis of Therapeutics [1], Neonatal Formulary [2], NEOFAX® by Young and Mangum [3], and The British National Formulary for Children [4] are consulted.
Administration schedules of sildenafil to infants and children
Oral treatment to infants [2]. Start by giving 250 to 500 µg/kg 4 times-daily and increase the dose as required, to no more than 2 mg/kg thrice-daily. Start with a low dose if there is hepatic or renal impairment. There are a few reports of infants who respond benefiting from substantial oral treatment for some weeks or months. Intravenous treatment to infants [2]. The usual dose is 100 µg/kg as a continuous infusion. Occasionally an infusion rate of 200 µg/kg/hour is required. Loading dose of up to 200 µg/kg given over 30 min has been used but can cause profound hypotension. Oral treatment of pulmonary arterial hypertension (initiated under specialist supervision) [4]
Children aged 1 to 11 months. Give initially 250 to 500 µg/kg 6 times-daily to thrice-daily. Adjust the dose according to the response, and start with the lower dose and frequency, especially if used with other vasodilators; the maximum dose = 30 mg daily.
Children aged 1 to 17 years with a body-weight of 20 kg. Give: 10 mg thrice-daily.
Children aged 1 to 17 years with body-weight of 20 kg and above. Give: 20 mg thrice-daily.
Dose adjustments due to interactions [4]
The manufactures advise to reduce the dose with concurrent use of moderate and potent inhibitors of CYP3A4 (avoid treatment with ketoconazole, itraconazole, and ritonavir) no specific recommendation made for children. Contra-indications to sildenafil treatment [4]. Hereditary degenerative retinal disorders, history of non-arthritic anterior ischaemic optic neuropathy, recent history of stroke, and sickle-cell anaemia.
Cautions for sildenafil treatment [4]
Active peptic ulcerations, anatomical deformation of the penis, autonomic dysfunction, blending disorders, cardiovascular disease, hypotension (avoid if severe), intravascular volume depletion, left ventricular outflow obstruction, ocular disorders, predisposition to priapism, and pulmonary veno-occlusive disease.
Efficacy and safety of sildenafil in infants and children
There is currently no evidence of serious adverse-effects in infants exposed to sildenafil. Sildenafil remains a valuable option for the treatment of pulmonary hypertension in young infants [5]. Sildenafil used for treatment of pulmonary hypertension has potential for reducing mortality-rate and improving oxygenation in infants, especially in resource-limited settings where inhaled nitric oxide is not available [6]. Oral sildenafil is a safe, simple, and effective treatment for persistent pulmonary hypertension in newborn infants [7]. Sildenafil treatment for 16 weeks has no effect on pulmonary vascular resistance index or mean pulmonary arterial pressure in children with Down syndrome and pulmonary arterial hypertension. Children with Down syndrome may be less responsive to sildenafil for pulmonary arterial hypertension [8]. Oral sildenafil is a safe and effective alternate for persistent pulmonary hypertension following congenital heart surgery in children [9]. Medium term Sildenafil therapy improves oxyhaemoglobin saturations and exercise tolerance in children with pulmonary hypertension without any adverse-effects [10]. Safety data suggest that sildenafil is well tolerated among children with idiopathic pulmonary arterial hypertension and pulmonary arterial hypertension associated with congenital heart disease [11].
Effects of sildenafil in infants and children
Sildenafil is associated with increasing foetal weight at birth [12]. Treatment of newborn infants with intravenous sildenafil, during the first day of life, is associated with acute improvement in oxygenation in more than 40% of infants [13]. Treatment with sildenafil provides a dose-dependent recovery of neonatal retinal function and structure [14]. Oral sildenafil is administered easily and tolerated as well as placebo and improves oxygenation index in infants with severe persistent pulmonary hypertension [15]. Sildenafil reduces N-terminal pro b-type natriuretic peptide levels in all infants with bronchopulmonary dysplasia-associated pulmonary hypertension [16]. The use of perioperative sildenafil in children has a statistically significant reduction in the mean pulmonary artery pressure without any adverse-effects [17]. Intravenous sildenafil is as effective as inhaled nitric oxide and causes pulmonary vasodilator in children with congenital heart disease [18].
Common or very common adverse-effects in infants and children [4]
Alopecia, anaemia, anxiety, cough, diarrhoea, dizziness, fluid retention, gastrointestinal discomfort, headaches, increased risk of infections, insomnia, nasal complains, nausea, night sweats, pain, skin reactions, tremor, vasodilatation, and vision disorders.
Uncommon adverse-effect in infants and children [4]
Arrhythmias, chest pain, drowsiness, dry eye, dry mouth, eye discomfort, eye disorders, eye inflammation, fatigue, feeling hot, gynecomastia, haemorrhage, hypertension, hypotension, myalgia, numbness, palpitations, sinus congestion, tinnitus, vertigo, and vomiting.
Rare or very rare adverse-effects in infants and children [4]
Acute coronary syndrome, arteriosclerotic retinopathy, cerebrospinal insufficiency, glaucoma, haematospermia, hearing impairment, irritability, optic neuropathy (discontinue treatment if sudden visual impairment occurs), oral hypaesthesia, priapism, retinal occlusion, scleral discolouration, seizure, severe cutaneous adverse reactions, sudden cardiac death, syncope, and throat tightness.
Pharmacokinetics of sildenafil in infants
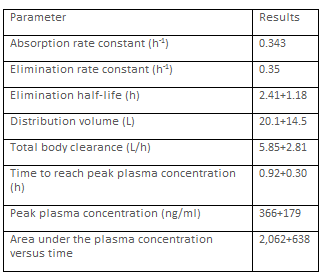
den Otter et al. [19] studied the pharmacokinetics of sildenafil in 23 newborn infants, aged 0.3 to 0.9 days, with congenital diaphragmatic hernia and pulmonary hypertension who were treated with sildenafil loading dose of 0.35 mg/kg (IQR 0.16 mg/kg) for 3 hours, followed by a continuous infusion of 1.5 mg/kg daily (IQR 0.1 mg/kg daily). All infants received inotropic drug support and were treated with inhaled nitric oxide.
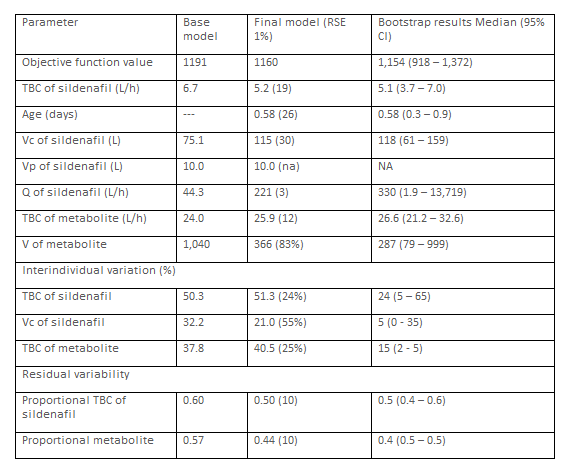
This table shows that Vc of sildenafil is greater than Vp of sildenafil, the total body clearance of the metabolite is greater than that of sildenafil, and there is a remarkable interindividual of the pharmacokinetic parameters.
Gonzalez et al. [20] investigated the pharmacokinetics of sildenafil in 34
premature infants with mean postmenstrual, postnatal ages of 125 days (range, 7 to 279), 41.6 weeks (range, 26.0 to 62.7), respectively, and weighing 3.41 kg (range, 0.59 to 8.1). Sildenafil was administered enterally at a dose of 2.79 mg/kg daily (range, 0.13 to 8.38).
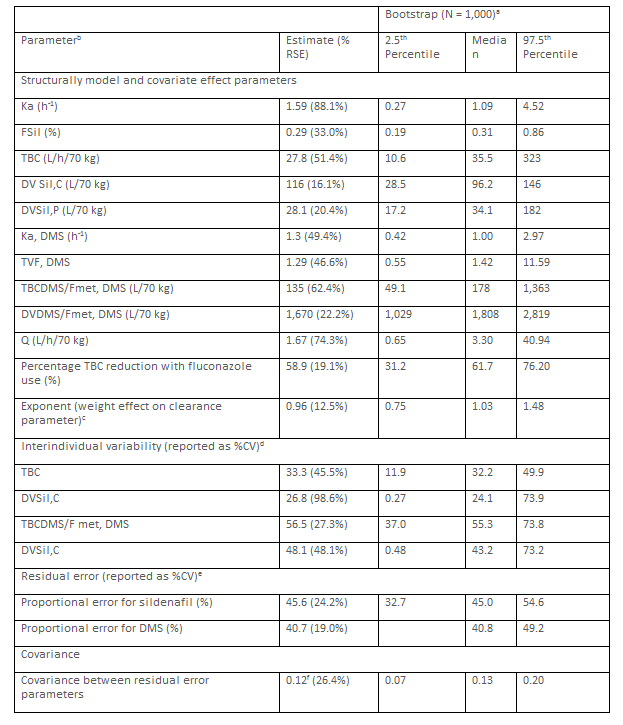
a83.4% of bootstrap runs resulted in a successful minimization. bKa (h-1) = 1.59. FSil = 0.29. TBC (L/h) = 27.8*(WTi/70kg)0.96*(0.411 [if infant received fluconazole])*exp(ɲi,DVSSil,C). DVSil,P (L) = 28.1*(WTi/70 kg). Ka,DMS (h-1) = 1.3. FDMS*(1-FSil). TBCDMS/Fmet,DMS (L/h) = 135*(WTi/70 kg)0.96*Exp (ɲTBCDMS/Fmet,DMS). DVDMS/Fmet,DMS (L) = 1,670*(WTi/70 kg/*Exp (ɲ DVDMS/Fmet,DMS). And Q (L*/h) = 1.67*(WTi is the individual participant body-weight.
cThe same exponent is assumed for all Sil and DMS total body clearance parameters. The exponent for the weight effect on the distribution volume parameter is fixed to 1. dETA shrinhage (%). TBC = 10.5%. DVSil,C = 48.0%. TBCDMS/Fmet,DMS = 6.43%. DVDMS/Fmet,DMS = 38.2%. eEPS shrinkage (%): Sil: 117%. DMS = 12.0%. fCorrelation coefficient = 0.65.
This table shows that sildenafil is rapidly absorbed following enterally
dosing, the central distribution volume is larger than the peripheral distribution volume, the absorption rate of the N-desmethyl sildenafil is similar to that of sildenafil, the total body clearance and the distribution volume of N-desmethyl sildenafil are greater than those of sildenafil, and there is a remarkable interindividual variability of the pharmacokinetic parameters. Such variability is accounted by the wide range of the postmenstrual, postnatal ages, and body-weight values.
Pharmacokinetics of sildenafil in children
Oya et al. [21] studied the pharmacokinetics of sildenafil in 13 children with a postnatal age, body-weight, and body-surface of 382+345 days, 6.67+2.52 kg, and 0.340+0.094 m2, respectively, who underwent cardiac surgery for congenital heart disease. Sildenafil was administered orally at a dose of 0.5 mg/kg 4 times-daily.
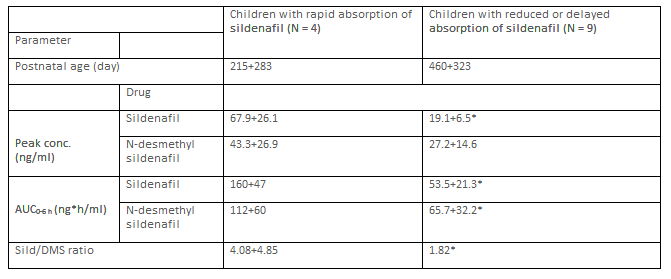
Sil = sildenafil. DMS = N-desmethyl sildenafil. *P-value < 0>
This table shows that children with rapidly absorption of sildenafil have higher peak concentration and AUC than children reduced are delayed adsorption of sildenafil.
Olguín et al. [22] investigated the pharmacokinetics of sildenafil in 12 children with pulmonary arterial hypertension aged 11.1+4.8 years (range, 1.4 to15.0) and weighing 14.0+1.5 kg (range, 7.5 to 26.0). Sildenafil was administered orally at a dose of 1 mg/kg once-daily.
This table shows that sildenafil is rapidly absorbed following oral dosing, is rapidly eliminated, and the distribution volume is larger than the water volume.
Interaction of sildenafil with drugs
When sildenafil is given in combination with fluconazole resulted in a geometric mean ratio of 1.01 for simulated AUCss,0‐24 relative to virtual infants receiving sildenafil alone and the. Thus the sildenafil dose should be reduced by 60% [23]. Lesinurad (200 mg once-daily) is an inducer of CYP3A and affects sildenafil exposure. Sildenafil exposure decreases by approximately by 34% the peak concentration and AUC when administered with multiple-dose of lesinurad 200 mg [24]. Exposure of sildenafil increases in presence of boceprevir. A dose adjustment of sildenafil is therefore necessary and an initial dose of 25 mg of sildenafil is suggested [25]. In men with angina, the blood pressure is reduced when sildenafil is co-administered with glyceryl trinitrate for ≥ 8 hours [26]. Sildenafil exposure is increased in the presence of darunavir/ritonavir and a dose adjustment of sildenafil is warranted when is co-administered with darunavir/ritonavir [28]. Both saquinavir and ritonavir modify the pharmacokinetics of sildenafil presumably through inhibition of CYP3A4 and the more pronounced effect of ritonavir may be attributed to its potent inhibition of CYP2C9 [29]. The co-administration of ciprofloxacin and clarithromycin significantly increases sildenafil bioavailability due to the inhibitory effect of ciprofloxacin and clarithromycin on CYP3A4 [30]. Co-administration of sildenafil with isosorbide mononitrate or glyceryl trinitrate significantly reduces blood pressure than isosorbide mononitrate or glyceryl trinitrate alone and sildenafil should not be administered to patients taking nitrates [31]. Plasma sildenafil AUC is markedly increased in the presence of indinavir compared with controls [32].
Metabolism of sildenafil
The CYP3A4, and to a lesser extent CYP2C9, mediate metabolism of sildenafil into N-desmethyl sildenafil [33]. The relative contributions to net intrinsic clearance of sildenafil are 79% for CYP3A4, 20% for CYP2C9; and < 2>
Treatment of infants and children with sildenafil
Bronchopulmonary dysplasia is the most common complication in preterm infants and often is complicated by pulmonary hypertension and sildenafil is used to treat these diseases [39]. Sildenafil is used in treating pulmonary hypertension associated with lung and renal hypoplasia in infants with congenital diaphragmatic [40]. The low cost, the oral availability, and the good tolerability of sildenafil make it a suitable and simple alternative therapy for secondary pulmonary hypertension including persistent postoperative pulmonary hypertension associated with ventricular septal defect [41]. Sildenafil continues to be the major treatment option for paediatric pulmonary arterial hypertension in infants and children [42]. Pulmonary arterial hypertension is a life-threatening disease and sildenafil is one of the therapeutic agents used extensively in the treatment of pulmonary arterial hypertension in infants and children [43]. Pulmonary arterial hypertension contributes to disability and death in children and the treatment with sildenafil has been approval by the European Medicines Agency for its paediatric use in Europe and in the U.S. by the Food and Drug Administration [44]. Oral sildenafil given in low doses controls pulmonary hypertension safely and effectively in children undergoing operations to correct congenital heart defects [45]. A single dose of sildenafil prevents rebound after withdrawal of nitric oxide and reduces the duration of mechanical ventilation in children [46]. Sildenafil therapy reduces the mortality-rate of pulmonary arterial hypertension in children [47].
Transfer of sildenafil across the human placenta
Of the 150 participants administered sildenafil citrate, 33 post-treatment maternal samples and 26 cord blood samples were obtained. The interval between sildenafil citrate administration and maternal blood sampling was 2.5 hours (range, 1.9 to 3.2) and the interval between last dose of sildenafil citrate and cord blood sampling was 5.6 hors (range, 3.5 to 6.7). Sildenafil citrate crosses the human placenta in significant amounts [48]. At steady state, the foetal-to-maternal transfer ratio of sildenafil is 0.37+0.03 in healthy placentas versus 0.66 and 0.47 in the 2 preeclampic placentas [49]. Transfer clearance of sildenafil in the high dose, during the first hour of perfusion, is 3.15 ml/min (range, 2.14 to 3.19 ml/min) for the maximum tolerated concentration and 3.07 ml/min (range, 2.75 to 3.42 ml/min) for the therapeutic concentration (not significant). The foetus-to-maternal concentration ratio significantly increases over time, up to 0.91+0.16 for the maximal concentration and 0.95+0.22 for the therapeutic concentration at the end of the perfusion (not significant). Sildenafil crosses the term placenta at a relatively high rate ex-vivo, which suggests that there is sufficient placental transfer to reach clinically active foetal drug levels at the currently used maternal doses [50].
Migration of sildenafil into the breast-milk
The concentrations of sildenafil and its major metabolite N-desmethyl sildenafil are measured in three breast-milk samples. The concentration of sildenafil ranges from 1.64 to 4.49 ng/ml and that of N-desmethyl sildenafil ranges from 1.18 to 1.82 ng/ml in the breast-milk [51].
Sildenafil, which structurally mimics the purine ring of cGMP, is a competitive and selective inhibitor of phosphodiesterase 5. By inhibiting cGMP hydrolysis, sildenafil elevates cellular levels of cGMP and augments signalling through the cGMP-protein kinase G pathway, provided guanylyl cyclase is active. Sildenafil is rapidly absorbed following oral dosing and it is cleared by hepatic CYP3A4 (major route) and by CYP2C9 (minor route) and the major metabolite is N-desmethyl sildenafil which is predominately excreted into the faeces. Concomitant administration of potent CYP3A inducers (e.g., bosentan) causes decrease in plasma levels of sildenafil and the co-administration of sildenafil with CYP3A4 inhibitors (e.g., erythromycin and cimetidine) inhibits sildenafil metabolism prolonging the half-life and elevating blood levels of sildenafil [1]. Sildenafil is a pulmonary artery vasodilator [2] and it is used to treat persistent pulmonary hypotension [3]. Sildenafil is contraindicated in infants taking organic nitrates and in infants with a known hypersensitivity to sildenafil [3]. Sildenafil may be administered orally; the oral treatment consists in 250 to 500 µg/kg 4 times-daily in infants [2]. In children, the oral dosage of sildenafil varies with the child age and body-weight and it is 10 or 20 mg thrice-daily in children with a body-weight up to 20 kg or > 20 kg, respectively [4]. Sildenafil has been found efficacy and safe in infants and children [5-11]. Sildenafil is used in the treatment of pulmonary hypertension and does not induce serious adverse-effect in infants [5], and sildenafil reduces the mortality-rate in infants with pulmonary hypertension [6]. Oral sildenafil is safe and effective in the treatment of persistent pulmonary hypertension in newborn infants [7]. Children with Down syndrome may be less responsive to sildenafil for pulmonary arterial hypertension [8]. Oral sildenafil is safe and effective for persistent pulmonary hypertension in children [9], and sildenafil improves oxyhaemoglobin saturation and exercise tolerance in children with pulmonary hypertension [10]. Sildenafil is well tolerated in children with idiopathic pulmonary arterial hypertension [11]. The effects of sildenafil have reported in infants and children [12-18]. Sildenafil increases foetal body-weight at birth [12] and intravenous sildenafil improves oxygenation in infants [13]. Treatment with sildenafil recovers neonatal retinal function and structure and these effects are dose dependent [14]. Oral sildenafil improves oxygenation index in infants with severe persistent pulmonary hypertension [15]. Sildenafil reduces N-terminal pro b-type natriuretic peptide levels in infants with bronchopulmonary dysplasia-associated to pulmonary hypertension [16], and sildenafil reduces the pulmonary artery pressure in children [17]. Intravenous sildenafil is as effective as inhaled nitric oxide in children with pulmonary vasodilator and with congenital heart diseases [18]. Sildenafil induces various adverse-effects which are classified as: common or very common, uncommon, or rare or very rare [4]. The pharmacokinetics of sildenafil and its metabolite N-desmethyl sildenafil have been studied by Otter et al. [19], Gonzalez et al. [20], Oya et al. [21], and by Olguin et al. [22]. The absorption rate constant, the total body clearance, and the central and peripheral distribution volumes rage in a wide interval. Following oral administration, the absorption rate constant is 0.343 h-1, the elimination half-life is 2.41 hours, and the time to reach peak plasma concentration is 0.92 hours suggesting that sildenafil is rapidly absorbed and eliminated [22]. The central distribution volume is larger than the peripheral distribution volume [19, 20]. The total body clearance and the distribution volume of N-desmethyl sildenafil are higher than those of sildenafil. The higher total body clearance of N-desmethyl sildenafil suggests that this metabolite is cleared more rapidly than sildenafil [20]. Following oral administration of sildenafil, the peak plasma concentration and the AUC of sildenafil are greater in children with rapid absorption than in children with reduced or delayed absorption of sildenafil [21]. Sildenafil interacts with drugs [23-32]. When sildenafil is co-administered with fluconazole, the sildenafil dose should be reduced [23]. Lesinurad is an inducer of CYP3A and decreases sildenafil exposure [24], and boceprevir increases the exposure of sildenafil [24]. Sildenafil combined with glyceryl trinitrate reduces the blood pressure [25]. Darunavir/ritonavir [28] and saquinavir/ritonavir [29] modify the sildenafil pharmacokinetics being inhibitors of CYP3A4 and CYP2C9, respectively. The co-administration of ciprofloxacin and clarithromycin with sildenafil increases the bioavailability of sildenafil due to the inhibitory effect of CYP3A4 [30], the combination of sildenafil with isosorbide mononitrate or glyceryl trinitrate decreases the blood pressure [31], and indinavir increases the plasma AUC of sildenafil [32]. The CYP3A4, and to a lesser extent CYP2C9, mediate the metabolism of sildenafil into N-desmethyl sildenafil [33, 35]. The relative contributions to the intrinsic clearance of sildenafil are 79% for CYP3A4, 20% for CYP2C9, and < 2>
In conclusion, sildenafil, which structurally mimics the purine ring of cGMP, is a competitive and selecting inhibitor of phosphodiesterase 5. By inhibiting cGMP hydrolysis, sildenafil elevates cellular levels of cGMP and augments signalling through the cGMP-protein kinase G pathway, provided guanylyl cyclase is active. Sildenafil may be administered orally and following oral dosing it is rapidly absorbed. Sildenafil is cleared by hepatic CYP3A (major route) and CYP2C) (minor route) and the major metabolite of sildenafil is N-desmethyl sildenafil. Concomitant administration of CYP3A inducers (e.g., bosentan) causes decrease in plasma concentration of sildenafil. CYP3A4 inhibitors (e.g., protease inhibitors used in HIV therapy, erythromycin and cimetidine) inhibit sildenafil metabolism, prolonging the half-life and elevating blood concentration of sildenafil. Sildenafil is used as a pulmonary artery vasodilator and in the treatment of persistent pulmonary hypertension. The initial oral dosage of sildenafil consists in 250 to 500 µg/kg 4 times-daily in infants. In children, the oral dosage of sildenafil varies with the child age and with the body-weight and is 10 or 20 mg thrice-daily in children with a body-weight up to 20 or > 20 kg, respectively. Sildenafil has been found efficacy and safe in infants and children but it may cause averse-effects. The effects of sildenafil have been extensively studied. Following oral dosing of sildenafil, sildenafil is rapidly absorbed and eliminated; the absorption rate constant is 0.343 h-1 and the elimination half-life is 2.41 hours. The total body clearance and the central and peripheral distribution volumes range in a wide interval in infants and children. Sildenafil interacts with drugs and the treatment of infants and children with sildenafil has been extensively studied. Sildenafil citrate and sildenafil cross the human placenta and sildenafil migrates into the breast-milk in significant amounts. The aim of this study is to review the clinical pharmacology of sildenafil in infants and children.
The authors declare no conflicts of financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employments, gifts, and honoraria.
This article is a review and drugs have not been administered to men or animals.
The author thanks Dr. Patrizia Ciucci and Dr. Francesco Varricchio, of the Medical Library of the University of Pisa, for retrieving the scientific literature.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
