AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Gian Maria Pacifici, Associate Professor of Pharmacology,via Sant’Andrea 32,56127 Pisa,Italy.
Citation: Gian M Pacifici. (2021) Clinical Pharmacology of Propranolol in Infants and Children. Journal of Clinical and Laboratory Research. 3(3); DOI:10.31579/2768-0487/037
Copyright: © 2021 Gian Maria Pacifici. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 July 2021 | Accepted: 07 August 2021 | Published: 18 August 2021
Keywords: propranolol; dosing; efficacy; safety; effects; adverse-effects; metabolism; pharmacokinetics; drug-interactions; prophylaxis; treatment; trials; placenta; breast-milk; infants; children
Propranolol is α nonselective β adrenergic receptor antagonist with equal affinity for β1 and β2 adrenergic receptors, lacks intrinsic sympathomimetic activity, and does not block α receptors. Propranolol is absorbed following oral administration and consists in two enantiomers, the (-) enantiomer is the active form and is cleared from the body more slowly than the inactive (+) enantiomer. Much of propranolol is metabolized in the liver and the metabolites of propranolol are 4-hydroxypropranolol, 5-hydroxypropanolol, N-desisopropranol, and propranolol β-D-glucuronide. The oral dose of propranolol hydrochloride is 250 to 750 µg/kg thrice-daily in infants and in children it is 200 to 500 µg/kg thrice-daily or 4 times-daily. Propranolol has been found efficacy and safe in infants and children but may induce adverse-effects. The elimination half-life of propranolol is about 15 hours in term and preterm infants and the distribution volume of propranolol is larger than the water volume. Propranolol interacts with drugs. Halofenate, phenytoin, phenobarbitone, rifampicin, and ethanol which affect the clearance of propranolol, and chlorpromazine and cimetidine inhibit the metabolism of propranolol. The prophylaxis, treatment, and trials with propranolol have been extensively studied in infants and children. Propranolol crosses the human placenta but it does not equilibrate between the maternal and foetal compartment and migrates into the beast-milk. The aim of this study is to review the published of propranolol dosing, efficacy and safety, effects, adverse-effects, metabolism, pharmacokinetics, interaction with drugs, prophylaxis, treatment and trials in infants and children and propranolol transfer across the human placenta and migration into the beast-milk.
The β adrenergic receptor antagonists are classified as non-subtype-selective (“first generation”) β1 selective (“second generation”), and non-subtype- or subtype-selective with additional cardiovascular action (“third generation”). These last drugs have additional cardiovascular properties (especially vasodilation) that seem unrelated to β blockage. Propranolol is α nonselective β adrenergic receptor antagonist with equal affinity for β1 and β2 adrenergic receptors, lacks intrinsic sympathomimetic activity, and does not block α receptors. Propranolol has membrane stabilizing activity, low lipid solubility, the extent of oral absorption is < 90>
Absorption distribution metabolism and excretion of propranolol
Propranolol is highly lipophilic and almost completely absorbed after oral administration. Much of the drug is metabolized by the liver during its first passage through the portal circulation and only about 25% reaches the systemic circulation. In addition, there is great interindividual variation in the presystemic clearance of propranolol by the liver; this contributes to enormous variability in plasma concentrations (about 20-fold) after oral administration of the drug and to the wide dosage range for clinical efficacy. The degree of hepatic extraction of propranolol declines as the dose increases. The bioavailability of propranolol may be increased by the concomitant ingestion of food during long-term administration of the drug. Propranolol readily enters the central nervous system. Approximately 90% of the drug in the circulation is bound to plasma proteins. It is extensively metabolized, with most metabolites appearing in the urine. One product of hepatic metabolism is 4-hydroxypropanolol which has some β adrenergic antagonist activity. Analysis of the distribution of propranolol, its clearance by the liver, and its activity is complicated by the stereospecificity of these processes. The (-) enantiomer of propranolol is the active form and it is cleared more slowly from the body than the inactive enantiomer. The clearance of propranolol may vary with the hepatic blood flow and liver disease and also may change during the administration of other drugs that affect the hepatic metabolism. For the treatment of hypertension and angina, the initial oral dose of propranolol generally is 40 to 80 mg daily in adults. For the treatment of angina, the dose may be increased at intervals of less than 1 week as indicated clinically. In hypertension, the full blood pressure response may not develop for several weeks. Propranolol may be administered intravenously for the management of life-threatening arrhythmias or to patients under anaesthesia. Under these circumstances, the usual dose is 1 to 3 mg, administered slowly with careful and frequent monitoring of blood pressure, electrocardiogram, and cardiac function. If bradycardia is excessive, atropine should be administered to increase heart rate. A change to oral therapy should be initiated as soon as possible [1].
Literature search
The literature search was performed electronically using PubMed database as search engine and the following key words were used: “propranolol dosing infants, children“, propranolol efficacy, safety infants, children”, “propranolol effects infants, children”, Propranolol adverse effects infants, children”, “propranolol metabolism”, “propranolol pharmacokinetics infants, children”, “propranolol drug interactions”, “propranolol prophylaxis infants, children”, “propranolol treatment infants, children”, “propranolol trials infants, children”, “propranolol placental transfer”, and “propranolol migration into the breast-milk”. In addition, the books: The Pharmacological Basis of Therapeutics [1], Neonatal Formulary [2], NEOFAX® by Young and Mangum [3], and The British National Formulary for Children [4] were consulted.
Administration schedules of propranolol hydrochloride to infants and children
Administration of propranolol hydrochloride to infants [2].
Oral treatment of neonatal thyrotoxicosis
Infants. Give: 250 to 750 µg/kg of propranolol hydrochloride thrice-daily to control symptoms with 1 drop of Lugol iodine® trice-daily to control the transient neonatal thyrotoxicosis.
Lugol iodine® is a British formulation.
Intravenous treatment of arrhythmia
Infants. Try 20 µg/kg by slow intravenous injection over 10 min with electrocardiogram monitoring and increase this dose in step to cumulative total of 100 µg/kg if necessary. Give the effective dose intravenous thrice-daily for maintenance. The same strategy may also work for the “spells” sometimes seen in severe Fallot tetralogy (with oxygen, morphine, and, if necessary, sodium bicarbonate, to correct serious acidosis). For sustained oral maintenance try 250 to 500 µg/kg thrice-daily, adjust the dose according to response to a maximum of 4 mg/kg daily.
Oral treatment of neonatal hypertension
Infants. Start with 250 µg/kg thrice-daily together with hydralazine and increase the dose if necessary to a maximum of 2 mg/kg per dose.
Oral treatment of infantile haemangioma
Infants. The target dose for treatment is 1 to 3 mg/kg daily in 3 divided doses. Begin with the lowest possible dose and titrate upwards according to the response; many haemangioma will respond to even small doses. This is the best done under supervision especially in younger infants.
Propranolol is used for the treatment of tachycardia and hypertension. The preferred therapy for supraventricular tachycardia when is associated with Wolff-Parkinson-White syndrome. Other uses are the palliation of tetralogy of Fallot and hypertrophic obstructive cardiomyopathy, and adjunctive treatment of neonatal thyrotoxicosis. Propranolol is incompatible with most cephalosporins and penicillins [3].
Administration of propranolol hydrochloride to children
Oral administration for hyperthyroidism with autonomic symptoms
Children. Give initially 200 to 500 µg/kg thrice-daily, adjust the dose according to the response; increase the dose if necessary up to 1 mg/kg thrice-daily (maximum dose = 40 mg thrice-daily).
Intravenous administration for hyperthyroidism with autonomic symptoms
Children. Give initially 20 to 50 µg/kg thrice-daily or 4 times-daily (maximum per dose = 5 mg), adjust the dose according to the response, to be given over 10 min.
Oral treatment of thyrotoxicosis
Children. Give initially 250 to 500 µg/kg thrice-daily, adjust the dose according to the response; increase the dose if necessary up to 1 mg/kg thrice-daily (maximum dose = 40 mg thrice-daily).
Intravenous treatment of thyrotoxicosis
Children. Give initially 25 to 50 µg/kg thrice-daily or 4 times-daily (maximum per dose = 5 mg), adjust the dose according to the response, to be given over 10 min.
Oral treatment of thyrotoxic crisis
Children. Give initially 250 to 500 µg/kg thrice-daily or 4 times-daily, adjust the dose according to the response.
Intravenous treatment of thyrotoxic crisis
Children. Give initially 20 to 50 µg/kg thrice-daily or 4 times-daily (maximum per dose = 5 mg), adjust the dose according to the response, to be given over 10 min.
Oral treatment of hypertension
Children aged 1 month to 11 years. Give initially 0.25 to 1 mg/kg thrice-daily, and then increase the dose to 5 mg/kg in divided doses, the dose should be increased at weekly intervals.
Children aged 12 to 17 years. Give initially 80 mg twice-daily, and then increase the dose if necessary up to 160 to 320 mg daily, the dose should be increased at weekly intervals, slow-release preparations may be used for once-daily administration.
Oral prophylaxis of migraine
Children aged 2 to 11 years. Give initially 200 to 500 µg/kg twice-daily; usual dose is 10 to 20 mg twice-daily (maximum per dose = 2 mg/kg twice-daily).
Children aged 12 to 17 years. Give initially 20 to 40 mg twice-daily; usual dose is 40 to 80 mg twice-daily (maximum per dose = 120 mg, maximum dose = 4 mg/kg daily).
Oral treatment of arrhythmias
Children. Give: 250 to 500 µg/kg trice-daily or 4 times-daily (maximum dose = 1 mg/kg 4 times-daily), adjust the dose according to the response (maximum dose = 160 mg daily).
Intravenous treatment of arrhythmias
Children. Give: 25 to 50 µg/kg, and then 25 to 50 µg/kg thrice-daily or 4 times-daily if required, and the electrocardiogram monitoring is required.
Oral treatment of tetralogy of Fallot
Children aged 1 month to 11 years. Give 0.25 to 1 mg/kg thrice-daily or 4 times-daily (maximum dose = 5 mg/kg daily).
Intravenous treatment of tetralogy of Fallot
Children aged 1 month to 11 years. Give initially 15 to 20 µg/kg (maximum per dose = 100 µg/kg), higher doses are rarely necessary; and then 15 to 20 µg/kg thrice-daily or 4 times-daily if required, the electrocardiogram monitoring is required with the administration.
Efficacy and safety of propranolol in infants and children
Propranolol administered at a dose of 3.6 mg/kg daily is safe and successfully treats infants with supraventricular arrhythmias [5]. Propranolol is well tolerated with minimal adverse-effects in children with portal hypertension [6]. Propranolol is efficacy and safe in infants younger than 5 weeks and older than 5 months with infantile haemangioma [7]. Oral propranolol given at a dose of 2 mg/kg daily is a safe and effective treatment for infantile haemangiomas [8]. Oral propranolol administered at a dose of 2 mg/kg daily is well-tolerated and is an effective treatment for infantile haemangiomas [9]. Oral propranolol given at a dose of 3 mg/kg daily shows a consistent, rapid, and therapeutic effect of superficial infantile haemangiomas without significant adverse-effects [10]. Propranolol administered topically in 1% ointment has a beneficial effect on superficial haemangiomas of the skin and the treatment is well tolerated without adverse-effects [11]. Topical propranolol is safer than oral propranolol though may be less effective. Topical propranolol may be more suitable for infants with small superficial haemangiomas [12].
Effects of propranolol in infants and children
Oral propranolol inhibits angiogenesis via down-regulating the expression of vascular endothelial growth factor in infantile haemangioma derived stem cell [13]. Early effects of propranolol are attributable to vasoconstriction due to decreased release of nitric oxide and long-term effects are characterized by induction of apoptosis in proliferating endothelial cells which results in tumour regression [14]. Oral propranolol is highly effective and safe in the treatment of periocular capillary haemangiomas in infants [15]. Propranolol treatment improves heart failure scores, shorts lengths of hospital stay, lowers plasma renin activities, and corrects the diastolic ventricular function [16]. Propranolol eliminates symptoms attributed to idiopathic hypertrophic subaortic stenosis in all children and abolished hypoxemic spells in 12 of 17 (70.6%) children. Oral propranolol is an excellent drug for use in paediatric patients with different types of cardiac disease [17]. Propranolol is able to cross the blood-brain-barrier and induces the formation-rate of nitric oxide and/or H2O2 in the hypothalamus [18].
Adverse-effects caused by propranolol in infants and children
When used on very preterm infants, propranolol hydrochloride may have some temporary effects on the vital functions of these infants; however no serious adverse-effects are detected that may affect the physical and mental development in the long run [19]. Intolerable adverse-effects are rare in infants with haemangioma who are treated with propranolol. Predictive factors for intolerable adverse-effects include younger age and lower body-weight [20]. Six of 35 infants (17.1%) who were treated with oral propranolol underwent retinopathy of prematurity intervention, as opposed to 14 of 36 (38.9%) control infants [21]. An 18 month old boy presented caries in the upper central incisors following the use of propranolol solution for the treatment of an infantile haemangioma [22].
Metabolism of propranolol in human liver microsomes
Propranolol is converted into 4-hydroxy-, 5-hydroxy-propranolol, and N-desisopropranol whereas 7-hydroxypropranolol appears in trace amounts [23]. The formation of propranolol 5-hydroxylation as well as 4-hydroxylation is mainly catalysed by CYP2D6 and the formation of N-desisopropranol is catalysed by CYP1A2 in human liver microsomes [23].


P-value for correlation *P-value < 0>
This table shows that the side-chain N-desisopropylation of both propranolol enantiomers is mediated mainly by the CYP1A subfamily and to some extent by CYP2D6, whereas the ring 4-hydroxilation of the enantiomers is mediated almost exclusively by CYP2D6. The contribution of S-mephenytoin 4’-hydroxylase (CYP2C19) to the N-desisopropylation of propranolol enantiomers appears to be of negligible importance in human liver microsomes.
The glucuronidation of R- and S-propranolol is catalysed by at least 3 UGT isoforms: UGT1A9, UGT2B4 and UGT2B7. UGT1A9 shows remarkable stereoselectivity in Vmax and CLint values of R-propranolol < S>

Metabolism of propranolol in human subjects
The oral clearance of propranolol is significantly higher in men (65.7+7.7 ml/min/kg) than in women (40.2+6.2 ml/min/kg), P-value < 0>
Pharmacokinetics of propranolol in term and preterm infants
Filippi et al. [28] studied the pharmacokinetics of propranolol in 36 term and preterm infants who were suffering from congenital heart disease (N = 1), hypertrophic obstructive cardiomyopathy (N = 2), supraventricular tachycardia (N = 3), neonatal thyrotoxicosis (N = 4), Fallot tetralogy (N = 5), infantile haemangioma (N = 15), and to control hypotension (N = 6). The infants had postmenstrual and postnatal ages of 27.8+4.0 weeks and 66.5+20.1 days, respectively, and weighed 1,014+710 grams. Propranolol was administered orally at a dose of 0.5 mg/kg 4 times-daily to 28 infants and at a dose of 0.25 mg/kg 4 times-daily to 8 infants with extremely low postmenstrual age.
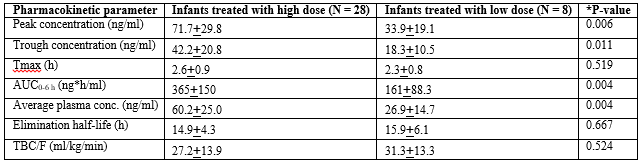
Tmax = time to reach the peak concentration. TBC/F = apparent total body oral clearance. F = oral bioavailability. *Student t test for umpired data.
This table shows that all pharmacokinetics parameters of propranolol, except for the Tmax, the elimination half-life, and the apparent total body clearance are different according to the two doses.

Tmax = time to reach the peak concentration. TBC/F = apparent total body oral clearance. F = oral bioavailability.
This table shows that the pharmacokinetic parameters of propranolol are not different in the three groups of infants. The difference among groups was tested by Analysis of variance (ANOVA).
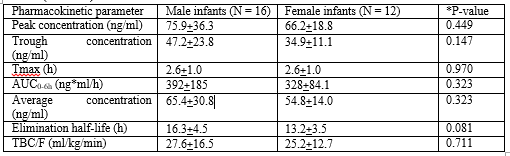
Tmax = time to reach the peak concentration. TBC/F = apparent total body oral clearance. F = oral bioavailability. *Student t test for umpired data.
This table shows that the pharmacokinetic parameters of propranolol are not different according to the sex.
Takechi et al. [29] investigated the pharmacokinetics of propranolol in 32 infants and young children (9 males and 23 females) suffering from infantile haemangioma. Subjects had mean postmenstrual, postnatal ages, and body-weight of 374 days (range, 317 to 437), 113 days (range, 53 to 150), and 6,115 grams (range, 3,150 to 8,710), respectively. Propranolol was administered orally at an initial dose of 0.5 mg/kg twice-daily and then the dose was increased to 3 mg/kg daily and the treatment lasted for 24 weeks.
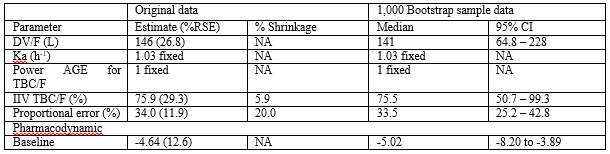
DV = apparent distribution volume. Ka = absorption rate constant. TBC = apparent total body clearance. F = oral bioavailability. Power AGE for TBC/F = power exponent of age for TBC/F. %RSE = %relative standard error. Baseline indicates the intercept coefficient of logistic regression. NA = not applicable.
This table shows that the distribution volume is larger than the water volume, propranolol is rapidly absorbed following oral administration, and there is a remarkable interindividual variability of the total body clearance. This variability is accounted by a wide variability in the demographic characteristics of subjects enrolled in the study.
Interaction of propranolol with drugs
Blood concentration of lithium is increased when it is co-administered with propranolol [30]. There is a correlation between in-vitro drug dissolution and in-vivo plasma concentration of propranolol when it is co-administered with paracetamol [31]. The absorption, protein binding, and metabolism of propranolol is affected by the co-administration of other drugs. Halofenate, phenytoin, phenobarbitone, rifampicin and ethanol affect the clearance of propranolol and chlorpromazine and cimetidine inhibit the metabolism of propranolol [32]. Although the propranolol and nifedipine alone are significantly more effective than placebo, their combination provides an even greater improvement (P-value < 0>
Prophylaxis with propranolol in infants and children
Prophylactic oral propranolol is effective in preventing severe retinopathy of prematurity in premature infants [36]. Prophylaxis with propranolol is efficacy in controlling the progression of retinopathy of prematurity in preterm infants [37]. Prophylactic propranolol, in the prescribed dose of 1 mg/kg daily, shows a decreasing trend in all outcomes of retinopathy of prematurity [38]. The use of propranolol prevents the occurrence of cyanotic spells in preoperative infants with the tetralogy of Fallot [39]. Propranolol is useful for preventing the first and recurrent variceal bleeding in cirrhotic children [40]. Topiramate and propranolol have the same efficiency in preventing migraine headaches [41]. Prophylaxis with propranolol reduces monthly headache frequency up to 3.73+6.11 and 3.34+5.95 after 4 and 8 weeks, respectively [42].
Treatment with propranolol in infants and children
Propranolol reduces the recurrence of supraventricular tachycardia in 70% of infants [43]. There is no difference in supraventricular tachycardia recurrence in infants treated with digoxin or propranolol [44]. Propranolol treatment, but not digoxin and diuretics alone, effectively reduce clinical symptoms of heart failure in infants with congenital heart disease [45]. Propranolol is effective in treating hypoxemic spells in 80% of infants with teratology of Fallot and the effectiveness is greater with large doses of propranolol [46]. Propranolol treatment is safety and efficacy in infantile haemangioma and a higher response-rate can be gained with early treatment and a prolonged course of therapy [47]. Propranolol is a useful and safe treatment option for severe or complicated infantile haemangioma achieves a rapid and significant reduction in haemangioma size, and no adverse-effects are observed [48]. Propranolol administered at doses of 1.5 or 2 mg/kg daily, given in divided doses, with stepwise escalation is safe and effective for treating proliferating infantile haemangioma [49]. Propranolol administered orally at doses of 2 to 3 mg/kg daily has a consistent, rapid, and therapeutic effect, leading to considerable shortening of the natural course of infantile haemangiomas with good clinical tolerance [50].
Trials with propranolol in infants and children
Preterm newborns with retinopathy of prematurity, especially in stage 2 retinopathy of prematurity, were given oral propranolol and have a reduced risk of disease progression [51]. Oral propranolol in early stages of retinopathy of prematurity prevents the disease progression and reduces the need for invasive rescue therapy with laser or bevacizumab [52]. A trial showed that propranolol is effective at a dose of 3 mg/kg daily for 6 months in the treatment of infantile haemangioma [53]. Propranolol administered orally at a dose of 2 mg/kg daily reduces the volume, colour, and elevation of focal and segmental infantile haemangioma in infants and children [54]. Propranolol is efficacious in patients with infantile haemangioma. The most pronounced response is seen in the first 8 weeks and in infants aged 6 months or younger. A decline in heart-rate > 20% is an early marker of response to propranolol [55].
Transfer of propranolol across the human placenta
With recirculation of the fetal and maternal compartments propranolol rapidly equilibrated in the two perfusion circuits at 35% of the initial level in the maternal circuit [56]. The ratios of cord plasma to simultaneous maternal plasma levels of propranolol and its major metabolites are: propranolol 0.32+0.17, propranolol glucuronide 0.86+0.36, 4-hydroxypropranolol 1.4+1.0, 4-hydroxypropranolol β-D-glucuronide 0.71+0.45, and naphthoxylactic acid 3.0+1.6 [57]. The maternal concentration of propranolol is approximately four times that of the umbilical circulation [58].
Migration of propranolol into the breast-milk
In a woman taking 10 mg thrice-daily of propranolol, the peak of propranolol in the breast-milk is 30 µg/L at 2 hours after the dose [59]. Five postpartum women taking 40 mg twice-daily have average breast-milk concentration of propranolol 30 µg/L at 2 hours after the dose [60]. The concentration of propranolol in the breast-milk is 110 to 120 µg/L in two women 3 hours after an oral dose of 160 mg [61]. A hypertensive woman was treated throughout pregnancy with propranolol 40 mg daily, the breast-milk to plasma ratio is < 1>
Propranolol is α nonselective β adrenergic receptor antagonist with equal affinity for β1 and β2 adrenergic receptors, lacks sympathomimetic activity, and does not block α receptors. Propranolol may be administered orally or intravenously, the oral absorption-rate is < 90>
In conclusion, propranolol is α nonselective β adrenergic receptor antagonist with equal affinity for β1 and β2 adrenergic receptors, lacks intrinsic sympathomimetic activity, and does not block α receptors. Propranolol may be administered orally or intravenously, the extent of oral absorption is < 90>
The authors declare no conflicts of financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employments, gifts, and honoraria.
This article is a review and drugs have not been administered to men or animals.
The author thanks Dr. Patrizia Ciucci and Dr. Francesco Varricchio, of the Medical Library of the University of Pisa, for retrieving the scientific literature.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
