AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Gian Maria Pacifici,, Associate Professor of Pharmacology, via Sant’Andrea 32, 56127 Pisa, Italy.
Citation: Gian M. Pacifici, (2022) Clinical Pharmacology of Phenobarbital in Infants and Children, Clinical Medical Reviews and Reports. 4(3); DOI: 10.31579/2690-8794/116
Copyright: © 2022, Gian Maria Pacifici, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 November 2021 | Accepted: 16 December 2021 | Published: 07 January 2022
Keywords: phenobarbital; metabolism; pharmacokinetics treatment; trials; human brain; human placenta; breast-milk; infants, children
Phenobarbital inhibits seizures by potentiation of synaptic inhibition through an action on the GABAA receptor. Phenobarbital is an effective agent for generalized tonic-clonic focal-to-bilateral tonic-clonic and focal seizures. Phenobarbital may be administered orally or intravenously and following oral dosing phenobarbital is completely absorbed. In infants, seizures are controlled by an intravenous loading dose of 20 mg/kg followed by a maintenance dose of 4 mg/kg once-daily. In children, the treatment of all forms of epilepsy, except for typical absence seizures, consists in an oral phenobarbital and the status epilepticus is treated with intravenous phenobarbital and treatments consist in a loading dose followed by a maintenance dose. Phenobarbital induces several CYPs, UGT1A1, and CYP2B and CYP3A genes. In newborns and children, the elimination half-life is 46.9 hours and the distribution volume is 0.49 L/kg. In children with severe falciparum malaria and convulsions, the distribution volume is 0.79 L/kg. The treatment and trials with phenobarbital have been studied and phenobarbital interacts with drugs. Phenobarbital is transported into the human brain where reaches therapeutic concentrations and phenobarbital freely crosses the human placenta. Following therapeutic treatment with phenobarbital to lactating women, the concentrations of phenobarbital in the breast-milk are few µg/ml suggesting that phenobarbital poorly migrates into the breast-milk. The aim of this study is to review the published data of phenobarbital dosing, pharmacokinetics, treatment, and trials in infants and children, and the phenobarbital metabolism, phenobarbital transport in the human brain, placental transfer of phenobarbital, and phenobarbital migration into the breast-milk.
Phenobarbital was the first effective organic antiseizure agent. It has relatively low toxicity, is inexpensive, and is still one of the more effective and widely used antiseizure drugs [1].
The mechanism by which phenobarbital inhibits seizures likely involve potentiation of synaptic inhibition through an action on the GABAA receptor. Phenobarbital enhances responses to iontophoretically applied GABA in mouse cortical and spinal neurons, effects that are observed at therapeutically relevant concentrations of phenobarbital; in patch-clamp studies, phenobarbital increases the GABAA receptor-mediated current by increasing the duration of bursts of GABAA receptor-mediated currents without changing the frequency of bursts. At levels exceeding therapeutic concentrations, phenobarbital also limits its sustained repetitive firing; this may underline some of the antiseizure effects of higher concentrations of phenobarbital achieved during therapy of status epilepticus [1].
Phenobarbital is an effective agent for generalized tonic-clonic focal-to-bilateral tonic-clonic, tonic-clonic of unknown onset (generalized tonic-clonic), and focal seizures. Its efficacy, low toxicity, and low cost make it an important agent for these types of epilepsy. However, its sedative effect and its tendency to disturb behaviour in children have reduced its use as a primary agent. It is not effective for absence seizures [1]. Phenobarbital remains, over 100 years since it was the first introduced into clinical practice, perhaps the most widely used anticonvulsant in neonatology and it is still, for many, the first-line treatment for seizures in cooled and non-cooled infants [2]. Phenobarbital may improve outcomes in severely asphyxiated infants. Phenobarbital is administered by an intravenous infusion at a dose of 40 mg/kg over 1 hour, prior to onset of seizures. Phenobarbital may enhance the bile excretion in infants with cholestasis before technetium 99m-image display and analysis scanning. Phenobarbital is incompatible with: fat emulsion, hydralazine, hydrocortisone succinate, insulin, methadone, pancuronium, ranitidine, and vancomycin [3].
Oral absorption of phenobarbital is complete but somewhat slow; peak concentrations in plasm occur several hours after a single dose. It is 40 to 60% bound to plasma proteins and bound to a similar extent in the tissues, including brain. Up to 25% of a dose is eliminated by pH-dependent renal excretion of the unchanged drug; the remainder is inactivated by hepatic microsomal enzymes, principally CYP2C9, with minor metabolism by CYP2C19 and CYP2E1. Phenobarbital induces UGT enzymes as well as the CYP2C19 and CYP2E1 subfamilies. Drug metabolized by these enzymes can be more rapidly degraded when co-administered with phenobarbital; importantly. Oral contraceptives are metabolized by CYP3A4. The elimination half-life of phenobarbital varies widely, 50 to 140hours in adults and 40 to 70 hours in children younger than 5 years of age, often longer in infants. Phenobarbital’s duration of effect usually exceeds 6 to 12 hours in nontolerant patients [1].
During long-term therapy in adults, the plasma concentrations of phenobarbital averages 10 µg/ml per daily dose of 1 mg/kg; in children, the value is 5 to 7 µg/ml per 1 mg/kg. Although a precise relationship between therapeutic results and concentration of drug in plasma does not exist, plasma concentrations of 15 to 35 µg/ml are usually recommended for control of seizures. The relationship between plasma concentration of phenobarbital and adverse-effects varies in the development of tolerance. Sedation, nystagmus, and ataxia usually are absent at concentrations below 30 µg/ml during long-term therapy, but adverse-effects may be apparent for several days at lower concentrations when therapy is initiated or whenever the dosage is increased. Concentrations more than 60 µg/ml may be associated with marked intoxication in the nontolerant individual. Because significant behavioural toxicity may be present despite the absence of overt signs of toxicity, the tendency to maintain patients, particularly children, on excessively high doses of phenobarbital should be resisted. The plasma phenobarbital concentrations should be increased above 30 to 40 µg/ml only if the increment is adequately tolerated and only if contributes significantly to control of seizures [1].
The literature search was performed electronically using PubMed database as search engine and the following key words were used: “phenobarbital dosing infants, children“, “phenobarbital metabolism”, “phenobarbital pharmacokinetics infants, children”, “phenobarbital treatment infants, children”, “phenobarbital trials infants, children”, “phenobarbital drug interactions”, “phenobarbital human brain”, “phenobarbital placental transfer”, and “phenobarbital breast-milk”. In addition, the books: The Pharmacological Basis of Therapeutics [1], Neonatal Formulary [2], NEOFAX® by Young and Mangum [3], and The British National Formulary for Children [4] have been consulted.
Administration schedules of phenobarbital to infants and children
Administration to infants [2]
Give 20 mg/kg as a slow intravenous loading dose over 20 min to control seizures (once any biochemical disturbance, such has hypoglycaemia, has been excluded or treated) followed by 4 mg/kg once-daily by intravenous or intramuscular injection or by mouth (when a higher dose may be needed). Increase this to 5 mg/kg once-daily if treatment is needed for more than 2 weeks. While higher loading dose have been used, these can cause respiratory depression in the preterm infant and can cause prolonged sedation in infants undergoing therapeutic hypothermia.
Administration to children [4]
Oral treatment of all forms of epilepsy except typical absence seizures
Children aged 1 month to 11 years. Give initially 1 to 1.5 mg/kg twice-daily, and ten increase the dose in steps of 2 mg/kg daily as required; the maintenance dose is 2.5 to 4 mg/kg once-daily or twice-daily.
Children aged 12 to 17 years. Give: 60 to 180 mg once-daily.
Slow intravenous injection for the treatment of the status epilepticus
Children aged 1 month to 11 years. Give initially 20 mg/kg, the dose should be administered at a rate no faster than 1 mg/min, and then give 2.5 to 5 mg/kg once-daily or twice-daily.
Children aged 12 to 17 years. Give initially 20 mg/kg (maximum dose = 1 gram), the dose should be administered at a rate no faster than 1 mg/min, and then 300 mg twice-daily.
Induction of CYPs and UGTs by phenobarbital
A distal gene fragment, of about 2000 kb in CYP2B1, CYP2B2, and CYP2B10, has been shown to be a phenobarbital-responsive enhancer independent of proximal promoter elements. This fragment contains several binding sites for proteins and several functional elements, including an NF-1 site, and, therefore, has been designated as a phenobarbital-responsive unit [5]. Patients co-medicated with phenobarbital had significantly lower plasma clozapine levels than those of the controls (232+104 versus 356+138 ng/ml, P-value < 0>
Pharmacokinetics of phenobarbital in newborns and infants maintained on extracorporeal membrane oxygenation with phenobarbital
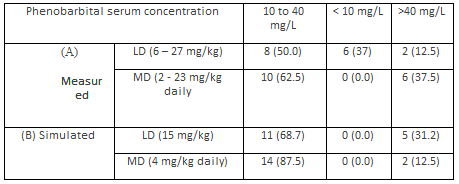
Pokorná et al. [13] studied the pharmacokinetics of phenobarbital in 7 newborns and 9 infants. Table 1 summarizes the demographic characteristics of subjects included in the study, table 2 shows the administration schedules of phenobarbital, and table 3 provides the pharmacokinetic parameters of phenobarbital.
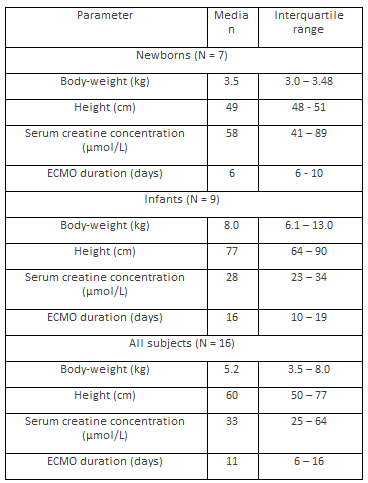
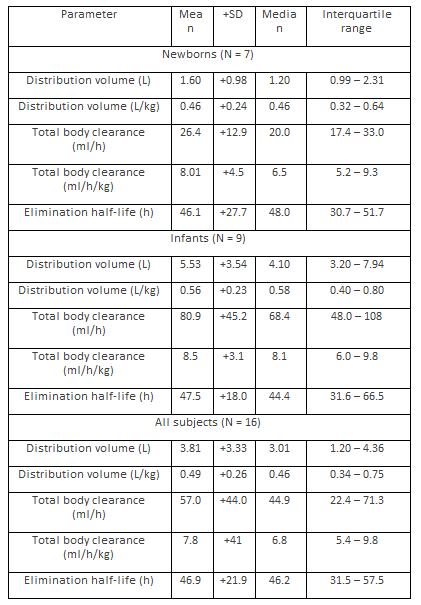
This table shows that the pharmacokinetic parameters obtained in newborns are not significantly different from those obtained in infants probably because the wide variability of the pharmacokinetic parameters.
Shellhaas et al. [14] investigated the pharmacokinetics of phenobarbital in 39 infants with neonatal encephalopathy. Twenty infants had hypothermia and 19 infants were normthermic. Table 4 summarizes the demographic characteristics of infants included in the study and table 5 shows the pharmacokinetics of phenobarbital obtained in these infants. Phenobarbital was administered as a loading dose followed by a maintenance dose. After loading phenobarbital doses of up 35 mg/kg, seven infants were treated with 2.5 mg/kg maintenance dosing twice-daily, while the remaining infants received 1.5 mg/kg maintenance dosing twice-daily.
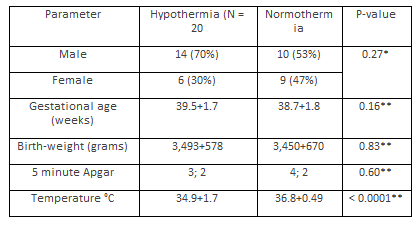
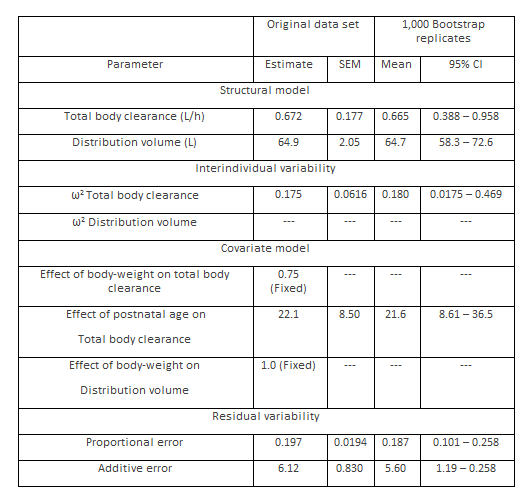
This table shows that the distribution volume is larger than the water volume and there is a remarkable interindividual variability of the total body clearance and the distribution volume. The comparison of the total body clearance and the distribution volume, obtained in these infants, with those obtained in infants maintained on extracorporeal membrane oxygenation (see table 3) is difficult because of the different diseases in these infants and the different expression units of pharmacokinetic parameters.
Pharmacokinetics of phenobarbital in children with severe falciparum malaria and convulsions
Kokwaro et al. [15] studied the pharmacokinetics of phenobarbital in 12 children, aged 7 to 62 months, with severe falciparum malaria and convulsions. Phenobarbital was administered as a loading dose followed by a maintenance dose. The intravenous loading dose was 15 mg/kg followed by a maintenance dose of 5 mg/kg 24 and 48 hours later.
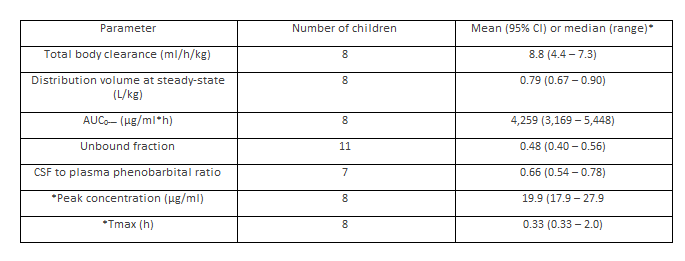
This tale shows that the distribution volume is similar to the water volume, phenobarbital is transported into the cerebrospinal fluid in significant amounts, and there is a remarkable interindividual variability in the pharmacokinetic parameter. The comparison of total body clearance and distribution volume with those obtained in infants (for infants see tables 3 and 5) is difficult because of the different diseases in infants and children and the different units of expression the pharmacokinetic parameters.
Treatment of infants and children with phenobarbital
Among infants with neonatal opioid withdrawal syndrome receiving morphine and secondary therapy, those treated with phenobarbital, had shorter length of hospital stay and shorter morphine treatment duration [16]. Intravenous administered phenobarbital controls seizures in 77% of both term and preterm newborns [17]. The mortality-rate caused by intracerebral haemorrhage in infants is significantly lower in the phenobarbital-treated group (8.0%) than in the control group (84.8%, P-value < 0>
Trials with phenobarbital conducted in infants and children
Phenobarbital is more effective than levetiracetam for the treatment of neonatal seizures [25]. Levetiracetam achieves better control than phenobarbitone for neonatal seizures when used as first-line antiepileptic drug and is not associated with adverse drug reactions [26]. Phenobarbital is associated with more adverse-effects than levetiracetam and the two drugs were equally but incompletely effective in treating electrographically confirmed seizures in neonates following cardiac surgery [27]. The significant difference (P-value < 0>
Interaction of phenobarbital with drugs
Phenobarbital has a great impact on the pharmacokinetics of tacrolimus over time in paediatric and adult patients. Phenobarbital can reduce the pharmacokinetic parameters of tacrolimus more effectively than intravenous phenobarbital [29]. After discontinuation of phenobarbital effective tacrolimus trough levels are increased [30]. Phenobarbital leads to a remarkable reduction in the plasma concentration of dolutegravir in a dose-dependent manner [31]. Phenobarbital co-administration with midazolam significantly increased midazolam clearance [32]. Tipranavir-ritonavir is a substrate of CYP3A4 and phenobarbital is an inductor of this CYP and phenobarbital decreases the plasma concentration of tipranavir-ritonavir [33]. Phenobarbital reduces the plasma concentration of chloramphenicol [34]. Phenobarbital lowers the plasma concentration of warfarin and reduces the half-life of warfarin [35]. Phenobarbital decreases the plasma concentration of warfarin antagonising the anticoagulant effect of warfarin [36].
Transport of phenobarbital into the human brain
In 10 patients, a significant correlation is found between brain and plasma of phenobarbital concentrations and the mean brain to plasma phenobarbital ratio is 0.91+0.08 [37]. In 12 epileptic patients undergoing temporal lobectomy, a significant correlation (P-value < 0>
Transfer of phenobarbital across the human placenta
The placental transfer of phenobarbital was investigated in 35 mother-infant pairs at birth. The drug was administered prenatally to the mothers for maternal epilepsy (group A, N = 5), gestational hypertension and preeclampsia (group B, N = 20) and prophylaxis of intraventricular haemorrhage in premature deliveries (group C, N = 10). The phenobarbital levels in arterial cord blood were 100+2.8% in group A, 89+21% in group B and 77+16% in group C with respect to the levels observed in the mothers. The most important factor influencing the transplacental passage was the duration of maternal treatment in the infant of group A (r = 0.80, P-value < 0 xss=removed xss=removed>
Migration of phenobarbital into the breast-milk
In lactating women taking phenobarbital for 3 days, the average breast-milk concentrations at 23 hours after the last dose are as follows: 90 mg daily in 4 women, 0.85 µg/ml (range, 0.8 to 1.0); 150 mg daily in 2 women, 1.25 µg/ml (range, 1.0 to 1.5); 225 mg daily in 2 women, 5.2 µg/ml (range, 2.7 to 5.0). The breast-milk phenobarbital concentrations are fairly constant during the day, averaging from 5.6 to 6.0 µg/ml at 9 am, 10 am and 8 pm in one lactating woman between days 3 and 7 postpartum. In the others, the phenobarbital concentrations averages to 7.3, 7.8, and 8.8 µg/ml at 6 am, 10 am and 8 pm, respectively, between days 5 and 11 postpartum [45]. A breast-milk phenobarbital concentration of 2.7 µg/ml is found 16 hours after the last dose in a lactating mother taking 30 mg of phenobarbital 4 times-daily from 3.5 to 6 days postpartum [46]. Eight phenobarbital breast-milk concentrations were measured between the days 3 and 32 postpartum at unstated times after the dose in an unstated number of nursing women who were taking phenobarbital and other anticonvulsants in unstated dosages. Phenobarbital breast-milk concentration averages to 10.4 µg/ml (range, 0.5 to 33), while the maternal serum concentration averages to 19.3 µg/ml [47]. Breast-milk samples were obtained during the first week postpartum from 4 lactating women who were taking phenobarbital. Their phenobarbital dosages ranged from 30 to 150 mg daily in 3 divided doses and the breast-milk samples were obtained 2 to 3 hours after the dose. Breast-milk concentration of phenobarbital ranged from 4.5 µg/ml in a woman taking 30 mg daily of phenobarbital to 7.6 µg/ml in a woman taking 150 mg daily. Phenobarbital concentration in breast-milk is less than that in simultaneous maternal serum samples in all cases [48].
Phenobarbital inhibits seizures by potentiation of synaptic inhibition through an action on GABAA. In patch-clamp studies, phenobarbital increase the GABAA receptor-mediated current by increasing the duration of burst of GABAA. Phenobarbital treats generalized tonic-clonic focal-to-bilateral tonic-clonic and focal seizures. Phenobarbital may be administered orally or intravenously, the oral absorption is complete, and peak plasma concentration occurs several hours after an oral dose [1]. In infants, the seizures are controlled with phenobarbital intravenous loading dose of 20 mg/kg followed by a maintenance dose of 4 mg/kg once-daily [2]. In children, all forms of epilepsy, except for typical absence seizures, are treated with oral phenobarbital and the status epilepticus is treated with intravenous phenobarbital, treatments consist in a loading dose followed by a maintenance dose, and phenobarbital dose increases with child age [4]. Phenobarbital induces several forms of CYPs and UGT1A and CYP2B and CYP3A genes [5-12]. Phenobarbital induces CYP2B1, CYP2B2, and CYP2B2 [5], phenobarbital induces the metabolism of clozapine increasing the formation-rate of N-oxide clozapine and demethylation pathway [6], and phenobarbital induces CYP2B and CYP3A genes [7]. In human liver slices, phenobarbital induces CYP2B6 and CYP3A4 mRNA and apoprotein [8]. In co-cultured HepG2, phenobarbital induces the expression of CYP2C and CYP3A family genes [9], and phenobarbital induces UGT1A1 [10-12]. The pharmacokinetics of phenobarbital have been studied in newborns and infant; the elimination half-life, the total body clearance, and the distribution volume of phenobarbital are about 47 hours, 57 ml/h, and about 0.5 L/kg, respectively [13]. In children with neonatal encephalopathy, the total body clearance and the distribution volume are 0.672 L/h and 64.9 L, respectively [14]. In children with severe falciparum malaria and convulsions, the total body clearance and the distribution volume are 8.8 ml/h/kg and 0.79 L/kg, respectively [15]. The comparison of the total body clearance and the distribution volume between infants and children is difficult because of the different diseases in infants and children and the different units of expression the pharmacokinetic parameters. The treatment of infants and children with phenobarbital has been extensively studied [16-24]. Phenobarbital treats the opioid withdrawal syndrome in newborns and this treatment provides a shorter hospitalization duration and shorter morphine treatment duration [16], intravenous phenobarbital controls seizures in the majority of newborns [17], and phenobarbital decreases the mortality-rate in preterm infants with intracerebral haemorrhage [18]. A phenobarbital loading dose of 15 mg/kg followed by a maintenance dose of 6 mg/kg once-daily controls convulsions in infants [19], an intravenous loading dose of phenobarbital of 15 to 20 mg/kg followed by a maintenance dose of 5 mg/kg once-daily controls seizures in infants [20], and phenobarbital decreases the incidence of neonatal hyperbilirubinemia [21]. Phenobarbital manages seizures in infants and children but phenobarbital my causes poisoning and phenobarbital should be administered with caution to avoid toxicity [22], phenobarbital controls the seizures in infants and children [23, 24]. The trials with phenobarbital have been conducted in infants and children [25-28]. Phenobarbital is more effective than levetiracetam for the control of neonatal seizures [25], in contrast with this finding, levetiracetam may control neonatal seizures more effectively than phenobarbital [26, 27], and phenobarbital is more effective than placebo in the control of febrile seizures in children [29]. The interaction of phenobarbital with drugs has been extensively reported [29-36]. Phenobarbital reduces the pharmacokinetic parameters of tacrolimus [29, 30], increases the midazolam clearance [30], reduces the plasma concentration of dolutegravir in a dose-dependent manner [31], phenobarbital increases the midazolam clearance [32], induces the CYP3A4 and this enzyme metabolizes tipranavir-ritonavir thus phenobarbital decreases the plasma concentration of tipranavir-ritonavir [33], phenobarbital reduces the plasma concentration of chloramphenicol [34], and lowers the plasma concentration of warfarin antagonising the anticoagulant effect of warfarin [35, 36]. The transport of phenobarbital into the human brain has been extensively studied [37-41]. The brain to plasma phenobarbital ratio is 0.91+0.08 [37], and it is 0.46+0.12 [38], a good correlation has been found between the plasma and brain [39, 40], phenobarbital is rapidly and uniformly transported into the brain [40], and the transport of phenobarbital into the newborn brain occurs rapidly and depends on brain lesion [41]. These results indicate that phenobarbital is transported into the human brain rapidly and the brain concentration of phenobarbital in brain equilibrates with that in plasma. Phenobarbital freely crosses the human placenta; the major factors influencing the transfer-rate of phenobarbital are the duration of maternal treatment, the gestational age, and the pH in the arterial umbilical cord [42], the umbilical cord to maternal concentration ratio of phenobarbital is 0.97+0.04 [43], and phenobarbital equilibrates between umbilical cord and maternal plasma [44]. These findings suggest that phenobarbital freely crosses the human placenta. The migration of phenobarbital into the breast-milk has been extensively studied [45-48]. Following therapeutic treatment with phenobarbital to lactating mothers, phenobarbital achieves concentrations of few µg/ml in the breast-milk indicating that phenobarbital poorly migrates into the breast-milk, and the concentrations of phenobarbital in the breast-milk are lower than the maternal ones [48].
In conclusion, phenobarbital is an effective gent for treatment of the generalized tonic-clonic focal-to-bilateral tonic-clonic and focal seizures. Phenobarbital may be administered orally of intravenously, and following oral dosing, phenobarbital is complete absorbed. The treatment of infants with seizures consists in an intravenous loading dose of 20 mg/kg followed by a maintenance dose of 4 mg/kg once-daily. The treatment of children with all forms of epilepsy, except for the typical absence seizures, consists in oral phenobarbital and the status epilepticus is treated with intravenous phenobarbital, and treatments consist in a loading dose followed by a maintenance dose, and phenobarbital dosage varies according to the child age. Phenobarbital induces different CYPs and UGT1A1 and CYP2B and CYP3A genes. The phenobarbital elimination half-life is about 47 hours in infants and no results are available for children. The treatment and trials with phenobarbital have been studied in infants and children. Phenobarbital interacts with drugs. The transport of phenobarbital into the human brain, the transfer of phenobarbital across the human placenta, and the migration of phenobarbital into the breast-milk have been extensively studied. The aim of this investigation is to review the clinical pharmacology of phenobarbital in infants and children.
The authors declare no conflicts of financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employments, gifts, and honoraria. This article is a review and drugs have not been administered to men or animals.
The author thanks Dr. Patrizia Ciucci and Dr. Francesco Varricchio, of the Medical Library of the University of Pisa, for retrieving the scientific literature.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
