AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Gian Maria Pacifici, Associate Professorof Pharmacology,via Sant’Andrea 32, 56127 Pisa, Italy.
Citation: Gian M Pacifici. (2022). Clinical Pharmacology of Levetiracetam in Infants and Children. Journal of Clinical and Laboratory Research. 5(1); DOI:10.31579/2768-0487/054
Copyright: © 2022 Gian Maria Pacifici. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 October 2021 | Accepted: 18 November 2021 | Published: 03 January 2022
Keywords: levetiracetam; dosing; efficacy and safety; adverse-effects; pharmacokinetics; prophylaxis; treatment; trials; placental transfer; breast-milk migration; infants; children
Levetiracetam inhibits focal and secondary generalized tonic-clonic seizures. The mechanism of levetiracetam action is not fully understood, however the correlation between binding affinity of levetiracetam and its analogues and their potency toward audiogenic seizures suggest that the synaptic vesicle glycoprotein 2A mediates the anticonvulsant effects of levetiracetam. The neural function of the synaptic vesicle 2A protein is not fully understood, but binding of levetiracetam to synaptic vesicle glycoprotein 2A might affect neuronal excitability by modifying the release of glutamate GABA through an action on vesicular function. Synaptic vesicle glycoprotein 2A may plain a role in vesicle recycling following exocytosis of neurotransmitter. In addition, levetiracetam inhibits N-type Ca2+ channels and Ca2+ release from intracellular stores. Levetiracetam may be administered intravenously or orally to infants and children and in children the levetiracetam dose varies according to the child age and body-weight. Levetiracetam is almost completed absorbed after oral administration and levetiracetam is found efficacy and safe in infants and children but it may induce adverse-effects. The levetiracetam elimination half-life is about 6 hours in infants and children, and in children the renal clearance is similar to the non-renal clearance. The prophylaxis, treatment, and trials with levetiracetam have been extensively studied in infants and children. Levetiracetam freely crosses the human placenta and freely migrates into the breast-milk. The aim of this study is to review the levetiracetam dosing, efficacy, safety, adverse-effects, pharmacokinetics, prophylaxis, treatment, and trials and transfer of levetiracetam across the human placenta and levetiracetam migration into the breast-milk.
Mechanism of levetiracetam action
Levetiracetam exhibits a novel pharmacological profile: it inhibits focal and secondary generalized tonic-clonic seizures in the kindling model, yet is ineffective against maximum electroshock – and pentylenetetrazol-induced seizure, findings consistent with clinical effectiveness against focal and secondary generalized tonic-clonic seizures. The mechanism by which levetiracetam exerts these antiseizure effects is not fully understood. However, the correlation between binding affinity of levetiracetam and its analogues and their potency toward audiogenic seizures suggests that the synaptic vesicle glycoprotein 2A mediates the anticonvulsant effects of levetiracetam. The synaptic vesicle glycoprotein 2A is an integral transmembrane glycoprotein; expression of human synaptic vesicle glycoprotein 2A in hexose transport-deficient yeast shows that the synaptic vesicle glycoprotein 2A can function as a galactose transporter. The neural function of the synaptic vesicle glycoprotein 2A protein is not fully understood, but binding of levetiracetam to synaptic vesicle glycoprotein 2A might affect neuronal excitability by modifying the release of glutamate GABA through an action on vesicular function. In mice, a missense mutation in the synaptic vesicle glycoprotein 2A is reportedly associated with disruption of action-potential invoked GABA in limbic regions. Synaptic vesicle glycoprotein 2A may play a role in vesicle recycling following exocytosis of neurotransmitter. In addition, levetiracetam inhibits N-type Ca2+ channels and Ca2+ release from intracellular stores [1].
Absorption distribution metabolism and elimination of levetiracetam
Levetiracetam is rapidly and almost completely absorbed after oral administration and is not bound to plasma proteins. In adults, the plasma elimination half-life is 6 to 8 hours, but may be longer in elderly patients. Ninety-five percent of the drug and its inactive metabolite are excreted in the urine, 65% of which is unchanged drug, 24% of the drug is metabolized by hydrolysis of the acetamide group. Because levetiracetam neither induces nor is a high-affinity substrate for CYPs or glucuronidation enzymes, it is devoid of known interactions with other antiseizure drugs, oral contraceptives, or anticoagulants [1].
Therapeutic use of levetiracetam
Levetiracetam is marked for the adjunctive treatment of focal seizures in adults and children, for primary onset tonic-clonic seizures, and for myoclonic seizures of juvenile myoclonic epilepsy. It is available in tablets (10, 25, 50, 75, or 100 mg), oral solution (10 mg/ml), or injectable form (50 mg/5 ml). Adult dosing is initiated at 500 to 1,000 mg daily and increased every 2 to 4 weeks by 1,000 mg to a maximum dose of 3,000 mg daily. The drug is administered twice-daily. In adults with either refractory focal seizures or uncontrolled generalized tonic-clonic seizures associated with idiopathic generalized epilepsy, addition of levetiracetam to other antiseizure medications is superior to placebo. Levetiracetam also has efficacy as adjunctive therapy for refractory generalized myoclonic seizures. Insufficient evidence is available about its use as monotherapy for focal or generalized epilepsy [1]. Levetiracetam is an anticonvulsant which has been used off-label in infants with difficult to treat seizures. It is a pyrrolidone derivative and is chemically unrelated to other currently available anticonvulsants. Although the exact mechanism of action is unclear, it has been shown to regulate glutamate release and NMDA receptor-mediated excitatory synaptic transmission. Unlike other anticonvulsants, it does not induce cell death and apoptosis in the developing brain which might offer a theoretical benefit over older established anticonvulsants. Levetiracetam has a broad antiepileptic activity across different seizure types and syndromes and is licensed in many countries as add-on treatment for partial-onset seizures in children > 4 years. In children and adults, the most common adverse-effects are somnolence and behavioural adverse-effects. Case studies and pharmacokinetic studies in newborn infants have suggested that levetiracetam is also safe in this group but evidence of benefit of randomized trials has yet to be published [2]. Levetiracetam (Keppra®) is an anticonvulsant and in the neonatal period it has been used as a second line of therapy for seizures refractory to phenobarbital and other anticonvulsants. Serum trough concentrations are not routinely monitored although they may be useful when determining the magnitude of dosing adjustment. Therapeutic concentrations are approximately 10 to 40 µg/ml [3].
Literature search
The literature search was performed electronically using PubMed database as search engine and the following key words were used: “levetiracetam dosing infants, children”, “levetiracetam efficacy safety infants, children”, “levetiracetam adverse-effects infants, children”, “levetiracetam pharmacokinetics infants, children”, “levetiracetam prophylaxis infants, children”, “levetiracetam treatment infants, children”, “levetiracetam trials infants, children”, “levetiracetam placental transfer”, and “levetiracetam breast-milk”. In addition, the books: The Pharmacological Basis of Therapeutics [1], Neonatal Formulary [2], NEOFAX® by Young and Mangum [3], and The British National Formulary for Children [4] are consulted.
Administration schedules of levetiracetam to infants and children
Administration to infants [2]
Intravenous administration
May be given with or without a loading dose depending on the urgency with which seizure control is needed. Without a loading dose: start with 10 mg/kg twice-daily increasing by followed by 10 mg/kg over 3 days to 30 mg/kg twice-daily. With loading dose: 40 mg/kg loading dose followed by 10 mg/kg once-daily (Note: the authors of this study suggested from pharmacokinetic studies that a maintenance dose of 19 mg/kg eight hourly results in better maintenance of serum levels towards the end of the first week of life).
Oral or enteral administration
Give 10 mg/kg daily in one to two divided doses, increase the dose daily by 10 mg/kg over 3 days to 30 mg/kg daily (further increases in doses have been reported up to 60 mg/kg daily).
Administration to children [4]
Oral of intravenous infusion treatment of monotherapy of focal seizures with or without secondary generalisation
Children aged 16 to 17 years. Give initially 250 mg daily for 1 week, and then increase the dose to 250 mg/kg twice-daily, and then increase the dose in steps of 250 mg twice-daily (maximum per dose = 1.5 mg twice-daily), adjust the dose according to the response, the dose to be increased every 2 weeks.
Oral treatment for adjunctive therapy of focal seizures with or without secondary generalisation
Children aged 1 to 5 months. Give initially 7 mg/kg once-daily, and then increase the dose in steps of up to 7 mg/kg twice-daily (maximum per dose = 21 mg/kg twice-daily), the dose to be increased every 2 weeks.
Children aged 6 months to 17 years (body-weight up to 50 kg). Give initially 10 mg/kg once-daily, and then increase the dose is steps of 10 mg/kg twice-daily (maximum per dose = 30 mg/kg twice-daily) the dose to be increased every 2 weeks.
Children aged 12 to 17 years (body-weight 50 kg and above). Give initially 250 mg twice-daily, and then increase the dose in steps of 500 mg twice-daily (maximum per dose = 1.5 grams twice-daily), the dose to be increased every 2 to 4 weeks.
Intravenous treatment for adjunctive therapy of focal seizures with or without secondary generalisation
Children aged 4 to 17 years (body-weight up to 50 kg). Give initially 10 mg/kg once-daily, and then increase the dose in steps of up to 1 mg/kg twice-daily (maximum per dose = 30 mg/kg twice-daily), the dose to be increased every 2 weeks.
Children aged 12 to 17 years (body-weight 50 kg or above). Give initially 250 mg twice-daily, and then increase the dose in steps of 500 mg twice-daily (maximum per dose = 1.5 grams twice-daily, the dose to be increased every 2 weeks).
Oral or intravenous treatment for adjunctive therapy of myoclonic seizures and tonic-clonic seizures
Children aged 12 to 17 years (body-weight up to 50 kg). Give initially 10 mg/kg once-daily, and then increase the dose in steps of up to 10 mg/kg twice-daily (maximum per dose = 30 mg/kg twice-daily), the dose to be increased every 2 weeks.
Children aged 12 to 17 years (body-weight 50 kg or above). Give initially 250 mg twice-daily, and then increase the dose in steps of 500 mg twice-daily (maximum per dose = 1.5 grams twice-daily, the dose to be increased every 2 weeks).
Efficacy and safety of levetiracetam in infants and children
Levetiracetam is a good and safe choice for treatment of neonatal seizures in preterm infants [5]. Levetiracetam is found to be well tolerated and efficacious for the treatment of infants with epilepsy [6]. Levetiracetam is efficacy and safe for infants and children with partial onset seizures [7]. Levetiracetam shows good efficacy, safety and tolerability for the long-term neonatal seizure treatment [8]. Levetiracetam is a safe and effective treatment for neonatal seizures which are unresponsive to phenobarbital [9]. Levetiracetam is an effective, well tolerated, and safe agent for the treatment of a variety of seizure types in infants [10]. Levetiracetam is an efficacious medication in treatment of seizures in the setting of neonatal hypoxic ischemic encephalopathy [11]. Intravenous levetiracetam is an efficacious agent for seizure management in preterm neonates [12]. Levetiracetam treatment is efficacy and safe in treating neonatal seizures suggesting that levetiracetam has anticonvulsant activity in term and preterm infants [13]. Levetiracetam is safe and effective for a wide range of epileptic seizures and epilepsy syndromes and therefore represents a valid therapeutic option in infants and young children affected by epilepsy [14]. The adjunctive use of intravenous levetiracetam is effective and well tolerated in paediatric patients with refractory status epilepticus even in patients younger than 2 years [15]. All responding children were on levetiracetam doses ≥ 30 mg/kg daily (median 40 mg/kg daily). No significant adverse-effects of levetiracetam were reported. Levetiracetam is effective and safe adjuvant therapy in children with refractory status epilepticus [16]. In children, intravenous levetiracetam may be effective in various clinical situations requiring intravenous administration of an antiepileptic drug [17]. Intravenous levetiracetam is effective in terminating status epilepticus or acute repetitive seizures and well tolerated in critically ill children [18]. Intravenous administration of levetiracetam is safe and effective for the treatment of acute repetitive seizures and convulsive status epilepticus in children and adolescents [19]. Levetiracetam given twice-daily in children with refractory epilepsy reduces seizure frequency in all types of epilepsy [20]. Intravenous levetiracetam is effective and safe in the treatment of children with acute repetitive seizures [21].
Common or very common adverse-effects caused by levetiracetam in infants and children [4]
Anxiety, appetitive decreased, asthenia, behavioural abnormal, cough, depression, diarrhoea, dizziness, drowsiness, gastrointestinal discomfort, headache, increased risk of infection, insomnia, mood altered, movement disorders, nausea, skin reaction, vertigo, and vomiting.
Uncommon adverse-effects caused by levetiracetam in infants and children [4]
Alopecia, concentration impaired confusion, hallucination, leukopenia, muscle weakness, myalgia, paraesthesia, psychotic disorder, suicidal tendencies, thrombocytopenia, vision disorders, and weight changes.
Rare or very rare adverse-effects caused by levetiracetam in infants and children [4]
Acute kidney injury, agranulocytosis, hepatic disorders, hyponatraemia, neutropenia, pancreatitis, pancytopenia, personality disorders, rhabdomyolysis, severe cutaneous adverse reactions, and thinking abnormal.
Pharmacokinetics of levetiracetam in infants
Merhar et al. [22] studied the pharmacokinetics of levetiracetam in 18 infants with gestational and postnatal ages of 38+6 weeks (range, 2 to 41) and 2 days (range, 0 to 32), respectively, and weighed 3.5 kg (range, 2.0 to 4.4) and levetiracetam was intravenously infused and the initial loading dose ranging from 14.4 to 39.9 mg/kg and all infants received at least 20 mg/kg of phenobarbital before receiving levetiracetam.
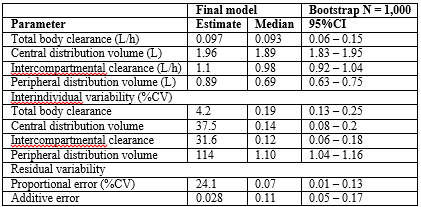
This table shows that the central distribution volume is larger than the peripheral and there is a remarkable interindividual variability of the pharmacokinetic parameters.
Pharmacokinetics of levetiracetam in infants and children
Glauser et al. [23] investigated the pharmacokinetics of levetiracetam in 12 infants and children aged 19.9 +14.16 months (range, 2.3 to 46.2) who received a single oral dose of levetiracetam of 20 mg/kg.
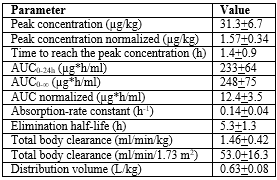
AUC = area under the plasma concentration-time curve. Peak concentration normalized and AUC normalized are normalized to a dose of 1 mg/kg.
This table shows that levetiracetam is rapidly absorbed as the absorption rate constant is 0.14+0.04 h-1 and the time to reach the peak plasma concentration is 1.4+0.9 h. The levetiracetam distribution volume is lower than the water volume, levetiracetam is rapidly eliminated and there is a remarkable interindividual variability in the pharmacokinetic parameters. Such variability is accounted by the wide variability of the subject demographic characteristics and also by the concomitant administration of different drugs.
Pharmacokinetics of levetiracetam in children
Pellock et al. [24] explored the pharmacokinetics of levetiracetam in 15 boys and 9 girls and subjects were aged 9.4+2.2 years (range, 5.6 to 12.6) who received a single oral dose of 20 mg/kg levetiracetam.
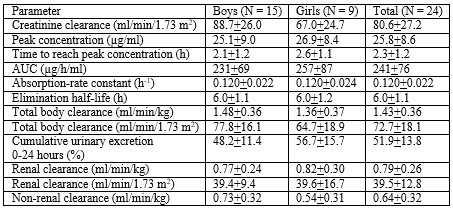
AUC = area under the plasma concentration-time curve.
This table shows that levetiracetam is rapidly absorbed as the absorption-rate constant is 0.120+0.022 h-1, the time to reach the peak concentration is 2.3+1.2 h, levetiracetam is rapidly eliminated. The renal clearance of levetiracetam is similar to the non-renal clearance suggesting that levetiracetam is eliminated by kidney and non-renal route. In addition, there is no gender-related difference in the pharmacokinetic parameters.
Wang et al. [25] studied the pharmacokinetics of levetiracetam in children aged 0.5 to 14 years and levetiracetam was orally administered at a dose of 20 to 60 mg/kg.
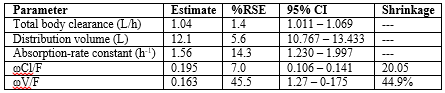
ωCl/F = variance of the Cl/F. ωV/F = variance of the ωV/F. %RSE = %relative standard error.
This table shows that there is a remarkable interindividual variability of the pharmacokinetic parameters which is accounted by the wide variability of the demographic characteristic of the subjects enclosed in the study. The total body clearance and the distribution volume significantly correlate with the age and body-weight of subjects. In particular, the total body clearance increases with the subject age and body-weight and the distribution volume decreases with the subject age and body-weight.
Prophylaxis with levetiracetam in infants and children
Levetiracetam is as effective as flunarizine in paediatric migraine Prophylaxis [26]. Levetiracetam and phenytoin have similar safety and effectiveness for the prevention of busulfan-induced seizures in a paediatric hematopoietic cell transplantation population [27]. Levetiracetam is a reasonable alternative to (fos) phenytoin for prophylaxis of early post-haemorrhagic seizures in infants and children [28]. Children receiving prophylaxis with levetiracetam after severe traumatic brain injury have a lower incidence of seizures of 9% [29].
Treatment of infants and children with levetiracetam
Very low certainty of evidence suggests that levetiracetam might not be more effective than phenobarbital. Moderate certainty of evidence indicates levetiracetam is associated with a lower risk of adverse-events [30]. Levetiracetam is an efficacious medication in treatment of seizures in the setting of neonatal hypoxic ischemic encephalopathy [31]. Levetiracetam is an alternative therapeutic option in neonatal seizures [32]. Levetiracetam monotherapy is effective in treating neonatal seizures [33]. Adjunctive levetiracetam is an efficacious and well-tolerated treatment for partial-onset seizures in infants and young children [34].Levetiracetam treatment is safe and effective in very paediatric patients with various types of epilepsy [35]. Levetiracetam combined with sodium valproate is effective in the treatment of children with epilepsy, and does not increase the clinical adverse-drug reactions [36]. There are significant differences in controlling seizures between levetiracetam and carbamazepine and the suppression of focal seizure occurs in 87% of children treated with levetiracetam [37]. Levetiracetam is an anticonvulsant agent with a favourable tolerability profile and a low potential for drug interactions and it is a useful option as adjunctive therapy in paediatric patients with epilepsy [38].
Trials with levetiracetam in infants and children
Levetiracetam is efficacy in the treatment of neonatal seizures and may be considered as the first-line anticonvulsant in infants with epilepsy [39]. The efficacy of levetiracetam is similar to that of phenytoin as second-line antiseizure medication for paediatric convulsive status epilepticus [40]. A trial showed that levetiracetam is efficacy and safety for preventing and treating paediatric epilepsy [41]. Levetiracetam is an effective anti-epileptic drug for both adults and children with generalized or partial-onset refractory seizures with a favourable adverse-event profile [42]. Levetiracetam has comparable effects concerning efficacy, tolerability, and adverse-events and levetiracetam is effective as mono- and adjunctive-therapy for all types of epilepsy syndromes and seizures in children [43]. A trial showed that levetiracetam is similar to phenytoin in children with convulsive status epilepticus resistant to benzodiazepines [44]. Although levetiracetam is not superior to phenytoin, the results suggest that levetiracetam is an appropriate alternative to phenytoin as the first-choice anticonvulsant agent in the treatment of paediatric convulsive status epilepticus [45]. Two clinical trials confirm that levetiracetam is a broad spectrum anti-epileptic drug with a favourable safety profile in children [46].
Transfer of levetiracetam across the human placenta
Tomson et al. [47] administered levetiracetam at a dose ranging from 1 to 3 grams daily to 14 pregnant women on the third trimester of pregnancy and measured the concentration of levetiracetam in the maternal and umbilical cord on delivery and 6, 12, 24, and 36 hours after delivery.
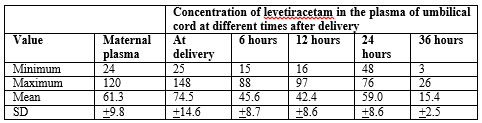
This table shows that levetiracetam freely crosses the placenta and slowly decays in the umbilical cord.
López-Fraile et al. [49] described the transfer of levetiracetam across the human placenta in 5 women at delivery at term of pregnancy. The mean umbilical cord to maternal plasma ratio is 1.21 suggesting the levetiracetam freely crosses the human placenta.
Johannessen et al. [50] administered levetiracetam at doses of 1.5 to 3 grams daily to 3 pregnant women at delivery at the third trimester of pregnancy. The levetiracetam concentration in the maternal and umbilical cord serum levetiracetam concentrations are 155+65.9 and 177+72.8 µg/kg, respectively, and the umbilical cord to maternal serum ratio of levetiracetam is 1.2+0.1.
Migration of levetiracetam into the breast-milk
Tomson et al. [47] administered levetiracetam at doses of 1 and 3 grams daily to 5 lactating women and measured the concentration of levetiracetam in the maternal plasma in the breast-milk.
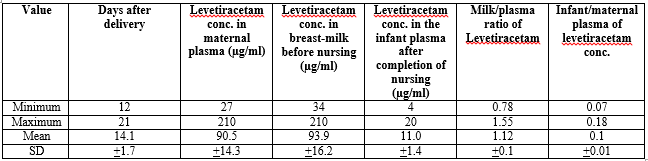
This table shows that levetiracetam freely migrates into the breast-milk and the infant exposition to levetiracetam is limited.
Johannessen et al. [50] administered levetiracetam at doses of 1.5 to 3 grams daily to 7 lactating mothers and measured the concentration of levetiracetam in the maternal plasma and in the breast-milk on the third to fifth days after delivery.

This table shows that levetiracetam freely migrates into the breast-milk and the infant exposition to levetiracetam is limited.
Levetiracetam was administration to 5 lactating women and the mean umbilical cord serum to maternal serum ratio is 1.14 (range, 0.97 to 1.45). The mean milk to maternal serum concentration ratio of levetiracetam is 1.00 (range, 0.76 to 1.33) at 3 to 5 days after delivery. At sampling 2 weeks to 10 months after delivery, this ratio is similar and ranges from 0.85 to 1.38. At 3 to 5 days after delivery, the infants had very lowlevetiracetam serum concentrations (< 10>
Levetiracetam inhibits focal and secondary generalized tonic-clonic seizures in the kindling model but it is ineffective against maximum electroshock and pentylenetetrazol-induced seizures. In addition, levetiracetam inhibits N-type Ca2+ channels and Ca2+ release from intracellular stores. Levetiracetam is rapidly and almost completely absorbed after oral administration and 95% of the drug and its inactive metabolite are excreted in the urine, 65% of which is unchanged drug, 24% of the drug is metabolized by hydrolysis of the acetamide group [1]. Levetiracetam may be administered orally or intravenously in infants [2] and in children [4] and in children the dose varies according to the child age and body-weight. Levetiracetam has been found efficacy and safe in infants and children [5-21] but levetiracetam may induce adverse-effects [4]. Levetiracetam is effective, safe, and well tolerated in treating neonatal seizures and epilepsy in infants [5-14] and in children [15-21]. The pharmacokinetics of levetiracetam have been studied in infants [22], in infants and children [23] and in children [24-25]. In infants, the central distribution volume is larger than the peripheral distribution volume [22]. Following oral administration to infants and children, levetiracetam is rapidly absorbed and the elimination half-life is 5.3+1.3 hours suggesting that levetiracetam is rapidly eliminated [23]. In children, the levetiracetam elimination half-life is 6.0+1.1 hours and the renal clearance is similar to the non-renal children suggesting that levetiracetam is eliminated by kidney and by other routes [24]. In children, aged 0.5 to 14 years, levetiracetam is rapidly absorbed following oral dosing and the mean total body clearance and distribution volume are 1.04 L/h and 12.1 L, respectively [25]. The prophylaxis with levetiracetam has been studied in infants and children [26-29]. Levetiracetam is effective as flunarizine in the prophylaxis of migraine in paediatric patients [26], levetiracetam and phenytoin have similar effectiveness for prevention of seizure induced by busulfan [27], levetiracetam and (fos) phenytoin are similarly effective in preventing early post-haemorrhagic seizures in infants and children [28], and prophylactic levetiracetam reduces the incidence of seizures in children after severe traumatic brain injury [29]. The treatment of infants and children with levetiracetam has been extensively studied [30-38]. Levetiracetam is similarly effective to phenobarbital in treating seizures but levetiracetam induces lower risk of adverse-effects [30]. Levetiracetam treats neonatal seizures in infants with hypoxic ischemic encephalopathy [31] and levetiracetam is an alternative therapeutic option in neonatal seizures [32, 33]. Levetiracetam is efficacious and well-tolerated in the treatment of partial-onset seizures in infants and children [34], and levetiracetam successfully treats various types of epilepsy in very young children [35]. Levetiracetam, combined with sodium valproate, treats childhood epilepsy and does not increase clinical adverse-drug reactions [36], levetiracetam is more effective than carbamazepine in treating seizures in children [37], and levetiracetam treats epilepsy and is well tolerated in paediatric patients [38]. The trials with levetiracetam have been extensively studied in infants and children [39-46]. Levetiracetam successfully treats neonatal seizures and is a first-line anticonvulsant in infants with epilepsy [39], levetiracetam and phenytoin are similarly effective as a second-line antiseizure medication in paediatric epilepsy [40], levetiracetam prevents and treats paediatric epilepsy [41], levetiracetam is an effective anti-epileptic drug in children and adults with generalized or partial-onset refractory seizures [42], and levetiracetam is safe and efficacy in treating all types of epilepsy in children [43]. Levetiracetam has similar effects to phenytoin in treating children with status epilepticus resistant to benzodiazepine [44], levetiracetam is an appropriate alternative to phenytoin in treating paediatric convulsive status epilepticus [45], and levetiracetam is safe and effective agent for treating epilepsy in children [46]. Levetiracetam freely crosses the human placenta [47-50] and levetiracetam slowly decays in infant plasma [47], and levetiracetam freely migrates into the breast-milk [47-51].
In conclusion, levetiracetam treats focal and secondary generalized tonic-clonic seizures. Levetiracetam is rapidly and almost completely absorbed after oral administration and 95% of the drug and its inactive metabolite are excreted in the urine 65% of which is unchanged drug and 24% of the drug is metabolized by hydrolysis of the acetamide group. Levetiracetam may be administered intravenously or orally to infants and children and in children the dose varies according to the child age and body-weight. Levetiracetam has been found efficacy and safe in infants and children but it may induce adverse-effects. The pharmacokinetics of levetiracetam have been studied in infants and in children and the levetiracetam elimination half-life is about 6 hours in infants and children and the renal clearance is similar to the non-renal clearance in children suggesting that levetiracetam is eliminated by kidney and by other routes. The prophylaxis, treatment, and trials with levetiracetam have been extensively studied in infants and children and levetiracetam freely crosses the human placenta and freely migrates into the breast-milk. The aim of this study is to review the clinical pharmacology of levetiracetam in infants and children.
The authors declare no conflicts of financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employments, gifts, and honoraria.
This article is a review and drugs have not been administered to men or animals.
The author thanks Dr. Patrizia Ciucci and Dr. Francesco Varricchio, of the Medical Library of the University of Pisa, for retrieving the scientific literature.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
