AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Gian Maria Pacifici, Associate Professor of Pharmacology via Sant’ Andrea 32, 56127 Pisa.
Citation: Gian Maria Pacifici, (2022) Clinical pharmacology of fentanyl in infants and children. J, Clinical Case Reports and Studies 3(2); DOI: 10.31579/2690-8808/099
Copyright: © 2022 Gian Maria Pacifici, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 October 2021 | Accepted: 05 November 2021 | Published: 04 January 2022
Keywords: fentanyl; dosing; efficacy and safety; effects; adverse-effects; metabolism; pharmacokinetics; drug interaction; treatment, trials; placenta; breast-milk; infants; children
Fentanyl is a systemic opioid related to the phenylpiperidines, it is used in anaesthetic practice and in analgesia and the analgesic effect is about 100 times higher than that of morphine. Fentanyl is highly lipid soluble, rapidly crosses the blood-brain-barrier, and fentanyl concentrations rapidly decline in plasma and cerebrospinal fluid. Fentanyl causes respiratory depression and decreases the heart rate through vagal activation. Fentanyl may be administered intravenously, orally, by transdermal, intranasal or by buccal application and the oral bioavailability is poor. In infants, fentanyl is given for short term use, sustained use, and during therapeutic hypothermia. In children, fentanyl is given intravenously, by transdermal application, or by buccal administration and the fentanyl dose varies with the child age and body-weight. Fentanyl has been found efficacy and safe in infants and children but it may induce adverse-effects and fentanyl causes different effects in infants and children. Following intravenous administration of fentanyl to infants and children, the fentanyl elimination half-life ranges from 208 to 1,266 min and the distribution volume ranges from 1.92 to 15.2 L/kg. Such variability is due to the wide variation of subject’s demographic characteristics. Fentanyl interacts with drugs, the treatment and trials with fentanyl have been studied in infants and children. Fentanyl freely crosses the human placenta and poorly migrates into the breast-milk. The aim of this study is to review fentanyl dosing, efficacy, safety, effects, adverse-effects, metabolism, pharmacokinetics, drug interaction, treatment, and trials in infants and children, and fentanyl placental transfer and migration into the breast-milk.
Mechanism of fentanyl action Fentanyl is a systemic opioid related to the phenylpiperidines. The actions of fentanyl and its congeners sulfentanil, remifentanil, and sulfentanil are similar to those of other MOR agonists. Fentanyl and sulfentanil are important drugs in anaesthetic practice because of their relatively short time to peak analgesic effect, rapid termination of effect after small bolus doses, cardiovascular safety, and capacity to significantly reduce the dosing requirement for the volatile agents. In addition, to a role in anaesthesia, fentanyl is used in the management of severe pain states delivered by several routes of administration [1].
Absorption, distribution, metabolism, and elimination of fentanyl
These agents are highly lipid soluble and rapidly cross the blood-brain-barrier. This is reflected in the half-life for equilibration between the plasma and the cerebrospinal fluid of about 5 min for fentanyl and sulfentanil. The levels in plasma and cerebrospinal fluid decline rapidly to redistribution of fentanyl from highly perfused tissue groups to other tissues such as muscle and fat. As saturation of less well-perfused tissue occurs, the duration of effect of fentanyl and sulfentanil approaches the length of their elimination half-life is 3 to 4 hours. Fentanyl and sulfentanil undergo hepatic metabolism and renal excretion. With the use of higher doses or prolonged infusions, the drugs accumulate, these clearance mechanisms become progressively saturated, and fentanyl and sulfentanil become longer acting [1].
Pharmacologic effects of fentanyl, Effects on the cerebral nervous system
Fentanyl and its congeners are all extremely potent analgesics and typically exhibit a very short duration of action when given parenterally. As with other opioids, nausea, vomiting, and itching can be observed. Muscle rigidity, while possible after all narcotics, appears to be more common after the high doses used in anaesthetic induction. Rigidity can be treated with depolarizing or non-depolarizing neuromuscular-blocking agents, while controlling the patient’s ventilation, but care must be taken sure that the patients are not simply immobilized and aware. Respiratory depression is similar to that observed with other MOR agonists but onset is more rapidly. As with analgesia, respiratory depression after small doses is of shorter duration than with morphine but of similar duration after large doses or lung infusions. Delayed respiratory depression also can be seen after the use of fentanyl or sulfentanil, possibly owing to enterohepatic circulation [1].
Effects on the cardiovascular system
Fentanyl and its derivatives decrease heart rate through vagal activation and may modestly decrease blood pressure. However, these drugs do not release histamine, and direct depressant effects on the myocardium are minimal. For this reason, high doses of fentanyl or sulfentanil are commonly used as the primary anaesthetic for patients undergoing cardiovascular surgery or for patients with poor cardiac function [1].
Therapeutic use of fentanyl
Fentanyl citrate and sulfentanil citrate have widespread popularity as anaesthetic adjuvants administered intravenously and epidurally. After systemic delivery, fentanyl is about 100 times more potent than morphine and sulfentanil is about 1,000 times more potent than morphine. The time to peak analgesic effect after intravenous administration of fentanyl and sulfentanil (about 5 min) is notable less than that of morphine and meperidine (about 15 min). Recovery from analgesic effects also occurs more quickly. However, with large doses or prolonged infusions, the effects of these drugs become more lasting, with durations of action becoming similar to those of longer-acting opioids. The use of fentanyl in chronic pain treatment has become more widespread. Transdermal patches that provide sustained release if fentanyl for 48 to 72 hours are available. However, factors promoting increased absorption (e.g., fever) can lead to relative overdosage and increased adverse-effects. Trans-buccal absorption by the use of buccal tablets and lollipop-like lozenges permit rapid absorption and has found use in the management of acute incident pain and for the relief of breakthrough cancer pain. As fentanyl is poorly absorbed in the gastrointestinal tract, the optimal absorption is through buccal administration. Fentanyl should only be used in opioid-tolerant patents, defined as consuming more than 60 mg of oral morphine equivalent. Epidural use of fentanyl and sulfentanil for postoperative or labour analgesia is popular. A combination of epidural opioids with local anaesthetics permits reduction in the dosage of both compounds. Illicit use (self-administration by chewing) of fentanyl patches can be deadly, and practitioners must be aware of this potential and keep careful control of fentanyl stocks [1]. Fentanyl is used to provide perioperative pain relief. Remifentanil is a related very short acting alternative. A continuous infusion will cause tolerance to develop and exposes infants to symptoms of opiate withdrawal. Routine use of a continuous fentanyl infusion seems to offer little advantage over bolus prior to painful procedures in ventilated preterm newborns [2]. Fentanyl is used in analgesia, sedation, or anaesthesia. Fentanyl is a synthetic opioid narcotic analgesic that is 50 to 100 times more potent than morphine on a weight basis and fentanyl is extremely lipid soluble. Fentanyl penetrates the cerebral nervous system rapidly. Transient rebound in fentanyl serum concentration may reflect sequestration and subsequent release of fentanyl from body fat. Fentanyl is metabolized extensively in the liver by CYP3A4 enzyme system and then excreted by the kidney. Serum elimination of fentanyl is prolonged in infants with liver failure and it is highly bound to plasma protein. The distribution volume widely varies (10 to 30 L/kg) and the serum elimination half-life is 1 to 15 hours. It is recommended to monitor respiratory and cardiovascular status closely, and to observe the abdominal distention, loss of bowel sounds, and muscle rigidity [3].
Literature search
The literature search was performed electronically using PubMed database as search engine and the following key words were used: “fentanyl dosing infants, children”, “fentanyl efficacy safety infants, children”, “fentanyl effects infants, children”, “fentanyl adverse-effects infants, children”, “fentanyl metabolism”, “fentanyl pharmacokinetics infants, children”, “fentanyl drug interactions”, “fentanyl treatment infants, children”, “fentanyl trials infants, children”, “fentanyl placental transfer”, and “fentanyl breast-milk”. In addition, the books: The Pharmacological Basis of Therapeutics [1], Neonatal Formulary [2], NEOFAX® by Young and Mangum [3], and The British National Formulary for Children [4] are consulted.
Administration schedules of fentanyl to infants and children
Intravenous administration to infants [2]
Short term use: Smaller doses (1 to 3 µg/kg), given over 30 seconds, may be used to provide analgesia in the spontaneously breathing infant but 5 µg/kg intravenous dose will abolish respiration whilst providing good brief analgesia; twice this dose is effective for an hour. A low dose of 0.67 to 1 µg/kg is sometimes used during less invasive surfactant administration in the occasional infant who is seen to “struggle” during this procedure. The short duration of action of fentanyl means that the infant can be maintained on continuous positive airway pressure.
Sustained use: Give an initial intravenous injection of 5 µg/kg, and then infuse intravenously at a rate of 1 to 1.5 µg/kg/hour. Adjust the dose according to response.
Use during therapeutic hypothermia: There are currently insufficient data from hypothermic newborns to recommend any specific dosing schedule, however it would seem sensible to begin by halving the “normthermic” dose (i.e., by giving 5 µg/kg, and then infusing at 0.75 µg/kg/hour) and titrating according to the response of the infant.Administration to children [4] Transdermal application for chronic intractable pain not currently treated with a strong opioid analgesic
Children aged 16 to 17 years. Give initially 12 µg/kg/hour every 72 hours, alternatively give initially 25 µg/kg/hour every 72 hours, when starting, evaluation of the analgesic effect should not be made before the system has been worn for 24 hours (to allow for the gradual increase in plasma fentanyl concentration) - previous analgesic therapy should be phased out gradually from time of first patch application, the dose should be adjusted at 24 to 72 hours intervals in step of 12 to 25 µg/kg/hour if necessary, more than one patch may be used at a time (but applied at the same time to avoid confusion) – consider additional or alternative analgesic therapy if the dose required exceeds 300 µg/kg/hour (important: it takes 17 hours or more for the plasma fentanyl concentration to decrease the dose by 50% - replacement opioid therapy should be intimately at a low dose and increased gradually). Transdermal application for chronic intractable pain currently treated with a strong opioid analgesic
Children aged 2 to 17 years. Give an initial dose based on previous 24 hour opioid requirement (consult product literature), for evaluating analgesic efficacy and dose increments. Intravenous injection for spontaneous respiration: analgesia and enhancement of anaesthesia during operation
Children aged 1 month to 11 years. Give initially 1 to 3 µg/kg, and then 1 µg/kg as required, the dose to be administered over at least 30 seconds.
Children aged 12 to 17 years. Give initially 50 to 100 µg (maximum per dose = 200 µg), the dose maximum on specialist advice, and then 25 to 50 µg as required, the dose to be administered over at least 30 seconds. Intravenous injection of assisted ventilation: analgesia and enhancement of anaesthesia during operation
Children aged 1 month to 11 years. Give initially 1 to 5 µg/kg, and then 1 to 3 µg/kg as required, the dose to be administered over at least 30 seconds.
Children aged 12 to 17 years. Give initially 1 to 5 µg/kg, and then 50 to 200 µg as required, the dose to be administered over at least 30 seconds.
Intravenous injection of assisted ventilation: analgesia and respiratory depression in intensive care
Children. Give initially 1 to 5 µg/kg, and then (by intravenous infusion) give 1 to 6 µg/kg/hour, adjust the dose according to the response.
Buccal administration using lozenges for breakthrough pain in children receiving opioid therapy for chronic cancer pain
Children aged 16 to 17 years. Give initially 200 µg, the dose to be given over 15 min, and then 200 µg after 15 min if required, no more than 2 dose units for each pain episode; if adequate pain relief not achieved with 1 dose unit for consecutive breakthrough pain episode, increase the strength of the dose unit until adequate pain relief achieved with 4 lozenges or less daily, if more than 4 episodes of breakthrough pain each day, adjust background analgesia.
Efficacy and safety of fentanyl in infants and children
In very preterm infants on mechanical ventilation, continuous fentanyl infusion is efficacy and safe in reducing acute pain [5]. Oral administration of fentanyl 30 min before entrance to the holding room for an operation is found efficacy and safe in children in reducing pain [6]. Intranasal fentanyl is found effective and safe in infants and reduces pain and does not induce adverse-effects [7]. Intranasal fentanyl is a safe and effective medication for the treatment of acute attacks of respiratory distress in children with life-limiting conditions [8]. Intranasal fentanyl, at a dose of 1.5 µg/kg, is a safe and effective analgesic in the prehospital management of acute severe pain in children and may be an attractive alternative to both oral and intravenous opiates [9]. Intranasal fentanyl has proven to be useful in both in-hospital and out-of-hospital pain management settings of pain [10]. Intranasal fentanyl, at doses of 50, 100, and 200 µg, is associated with an onset of activity at 10 minutes and effective treatment of breakthrough pain compared with placebo [11]. Intranasal fentanyl is an effective, safe and well tolerated mode of analgesia for children aged 1 to 3 years with moderate to severe pain [12]. Intranasal fentanyl has been found safe and efficacy in reducing acute pain in children [13].
Effects of fentanyl in infants and children
Administration of fentanyl bolus for procedural pain and sedation is not shown to significantly affect cerebral oxygenation, cerebral tissue oxygen extraction, or cardiac output in stable preterm infants [14]. Fentanyl added to epidural bupivacaine infusions during labour does not depress neonatal respiration or adversely affect neurobehavioral scores and other indices of neonatal welfare [15]. The use of intranasal fentanyl during halothane or sevoflurane anaesthesia for tympanosotomy tube placement is associated with diminished postoperative agitation without an increase in vomiting, hypoxemia, or discharge times [16]. There are significant correlations between fentanyl dosage and Neonatal Abstinence Score Tool score (r = 0.76, P-value < 0 xss=removed xss=removed>
Common or very common adverse-effects caused by fentanyl in infants and children [4] With parenteral use: apnoea, hypertension, movement disorders, muscle rigidity, post procedural complications, respiratory disorders, and vascular pain. With transdermal use: anxiety, appetite decreased, asthenia, depression, diarrhoea, dyspnoea, gastrointestinal discomfort, hypertension, insomnia, malaise, muscle complains, peripheral oedema, sensation abnormal, temperature sensation altered, and tremor.
Uncommon adverse-effects caused by fentanyl in infants and children [4]
With parenteral use: airway complication of anaesthesia, chills, hiccups, and hypothermia. With transdermal use: consciousness impaired, cyanosis, fever, gastrointestinal disorders, influenza like illness, memory loss, respiratory disorders, seizures, sexual dysfunction, and vision blurred.
Rare or very rare adverse-effects caused by fentanyl in infants and children [4]
With transdermal use: apnoea.
Adverse-effects caused by fentanyl in infants and children whose frequency is not known [4]
With buccal use: adrenal insufficiency, androgen deficiency, anxiety, appetite decreased, asthenia, coma, depersonalization, depression, diarrhoea, dyspnoea, emotional lability, fever, gait abnormal, gastrointestinal discomfort, gastrointestinal disorders, gingival haemorrhage, gingivitis, injury, loss of consciousness, malaise, myoclonus, oral disorders, peripheral oedema, seizures, sensation abnormal, sleep disorders, speech slurred, taste altered, thinking abnormal, throat oedema, vasodilation, vision disorders, weight decreased, and withdrawal syndrome neonatal. With parenteral use: biliary spasm, cardia arrest, cough, hyperalgesia, loss of consciousness, and seizure. With transdermal use: myoclonus, and withdrawal syndrome neonatal.
Fentanyl metabolism
CYP3A4*1G genetic polymorphism affects the metabolic-rate of fentanyl. There is a positive correlation between CYP3A4 mRNA level and metabolic-rate of fentanyl [18]. CYP3A4 is the major catalyst involved in fentanyl oxidation to norfentanyl in human liver [19]. Human intestinal and liver microsomes catalyse fentanyl metabolism and the enzyme which metabolizes fentanyl is CYP3A4 [20].
Pharmacokinetics of fentanyl in infants and children
Ziesenitz et al. [21] reviewed the pharmacokinetics of fentanyl in 51 infants and children aged 0 to 1 month to 9.5+2.8 years, and fentanyl dose is reported in table 1.
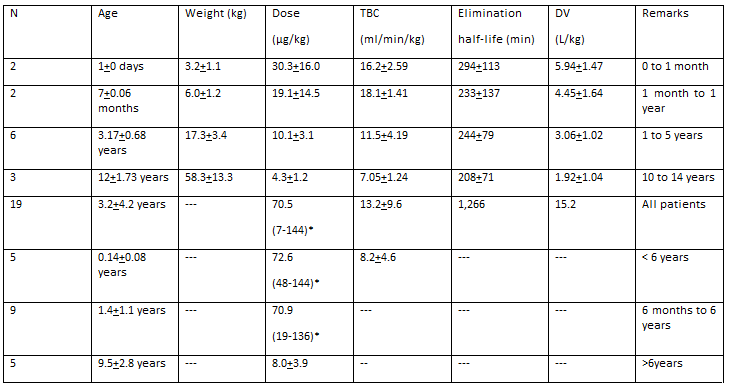
Fentanyl plasma concentrations after an intravenous bolus (about 30 µg/kg) are found to be lower in infants than in children and these findings may result from a larger distribution volume or age-related differences in protein binding. An increase in the total body clearance probably reflects maturation of CYP enzymes suggesting that the Michaelis-Menten constant is age dependent. In newborn infants and in older infants during non-cardiac surgery, the total body clearance increases with age, with the most rapid increase at a postnatal age of 2 weeks, whereas the distribution volume and the elimination half-life do not change after a bolus of 54.1+2.3 µg/kg. After a fentanyl continuous infusion, the elimination half-life is prolonged and the distribution volume at steady-state is increased due to a slow redistribution from peripheral compartments. The total body clearance is higher in children aged 6 months to 6 years compared to younger or older children (8.2 versus 18.9 versus 8.0 ml/min/kg) which is attributed to increase liver metabolism.
Interaction of fentanyl with drug
A patient using a fentanyl patch was started on a course of clarithromycin and experienced a respiratory arrest 2 days later [22]. Fentanyl and clarithromycin are metabolized by CYP3A4 and following the co-administration of these drugs clarithromycin inhibits fentanyl metabolism and induces respiratory depression and death [23]. Two infants developed chest wall rigidity following the co-administration of neuromuscular blocking with fentanyl [24]. A patient who received amitriptyline and fentanyl reported an adverse-reaction [25]. Fentanyl is metabolized by CYP3A4 and the co-administration of fentanyl with drugs which are metabolized by this enzyme inhibits fentanyl metabolism and results in excess of fentanyl serum concentration enhancing fentanyl effects [26]. Diltiazem and fentanyl are metabolized by CYP3A4; fentanyl inhibits the metabolism of diltiazem and induces delirium [27]. The co-administration of ranitidine and fentanyl increases the risk of seizures [28]. Fentanyl inhibits the P-glycoprotein-mediated digoxin transport in Caco-2 cells with IC50 value of 6.5 µM [29]. The dose of tacrolimus was reduced from 1.28 to 0.68 ml/min/kg when it was combined with fentanyl as tacrolimus and fentanyl are metabolized by CYP3A4 [30].
Treatment of infants and children with fentanyl
Fentanyl treatment of newborn infants during therapeutic hypothermia contributes to ameliorate neuroprotection in asphyxiated cooled newborns [31]. Fentanyl combined with midazolam is safe and more effective than midazolam alone for sedation therapy in mechanically ventilated children [32]. Enteral administration of methadone may expedite fentanyl discontinuation and reduce the risk of withdrawal in critically ill children at high risk for opioid abstinence syndrome [33]. Transdermal fentanyl is a useful opioid-agonist for the treatment of moderate to severe chronic cancer pain [34]. Treatment of children with therapeutic transdermal fentanyl is feasible and well tolerated [35]. Prophylactic fentanyl-droperidol prolongs the length-to-stay and recovery time and provides no discrete identifiable benefit over acetaminophen alone in paediatric strabismus repair [36].
Trials with fentanyl in infants and children
In very preterm infants on mechanical ventilation, continuous fentanyl infusion protects the developing brain by relieving pain during the first 72 hours of mechanical ventilation [37]. Higher cumulative fentanyl dose in preterm infants correlated with a higher incidence of cerebellar injury and lower cerebellar diameter [38]. Integrated pharmacokinetic/pharmacodynamic modelling showed that the usually prescribed dosage regimens of fentanyl in neonates may not always provide the optimum degree of sedation [39]. A short course of low dose fentanyl infusion reduces behavioural sedation scores, O2 desaturations, and neuroendocrine stress response in preterm ventilated infants [40]. Fentanyl is a more effective analgesic agent than morphine and causes fewer adverse-effects than morphine. Fentanyl is superior to morphine for short-term postnatal analgesia in newborn infants [41]. The current analyses indicate that fentanyl around the end of surgery reduces the incidence of emergence agitation in children undergoing general anaesthesia [42]. A meta-analysis suggests that fentanyl decreases the incidence of emergence agitation under sevoflurane anaesthesia in children and postoperative pain but has a higher incidence of postoperative nausea and vomiting [43].
Transfer of fentanyl across the human placenta
The mean umbilical vein to maternal fentanyl ratios is 1.12 for total drug and 1.20 for the free drug and values are unrelated to the last epidural bolus to delivery interval [44]. There is rapid transfer of fentanyl to the fetus in early pregnancy and the drug remains in foetal tissue for some time after the initial dose is given to the mother [45]. Fentanyl rapidly transfers across the early placenta into the amniotic cavity and foetal blood circulation [46]. Fentanyl is detected in the foetal blood 1 min after dosing and peaks at 5 min [47]. Thirty paired samples were obtained from healthy pregnant women and foetuses and the foetal to maternal fentanyl plasma concentration ratio ranges between 0.23 and 0.73 indicating fentanyl crosses the human placenta [48].
Migration of fentanyl into the breast-milk
Nitsun et al. [49] studied the pharmacokinetics of fentanyl in the breast-milk of 5 lactating women on the 11+4 weeks of post-partum. Fentanyl was intravenously infused at a dose of 100 µg and the concentration of fentanyl in the breast-milk was measured 4, 7, 9, 11, and 24 hours after fentanyl dosing.

This table shows that the maximum exposure of fentanyl to the nursing infants is < 0>
Leuschen et al. [50] studied the migration of fentanyl into the breast-milk of 10 lactating women and observed a lack of substantial fentanyl excretion into the breast-milk after short-term maternal fentanyl exposure.
Fentanyl is a systemic opioid related to phenylpiperidines and it is used in anaesthetics and in analgesia and the analgesic effects is about 100 times higher than that of morphine. Fentanyl is highly lipid soluble and rapidly crosses the blood-brain-barrier and it is rapidly eliminated in plasma and cerebrospinal fluid. Fentanyl may cause nausea, vomiting, itching, muscle rigidity, respiratory depression, and decreases heart rate through vagal activation. Fentanyl may be administered intravenously, orally, and by buccal, transdermal and intranasal applications, and the oral bioavailability is poor whereas the bioavailability following buccal administration is good [1]. In infants, fentanyl is given intravenously for short and sustained uses and during therapeutic hypothermia. For the short and sustained uses the fentanyl dose is 1 to 3 µg/kg and 5 µg/kg, respectively. For the treatment of hypothermia fentanyl is given at a dose of 5 µg/kg followed by an infusion of 0.75 µg/kg/hour [2]. In children, fentanyl may be given intravenously, by transdermal application, and by buccal administration and the dose varies according to child age and body-weight [4]. Fentanyl has been found efficacy and safe in infants and children [5-13]. Continuous infusion of fentanyl is found efficacy and safe in reducing acute pain in preterm infants maintained on mechanical ventilation [5]. Oral fentanyl administered 30 min before starting surgery is efficacy and safe in reducing pain [6]. Intranasal fentanyl has been found efficacy and safe in reducing pain in infants without inducing adverse-effects [7], and in treatment of acute attacks of respiratory distress in children with life-limiting conditions [8]. Intranasal fentanyl, administered at a dose of 1.5 µg/kg, is an effective and safe analgesic agent in reducing acute severe pain in children [9] and in the management of pain in both in-hospital and out-hospital children [10]. Intranasal fentanyl, at doses of 50, 100, or 200 µg, is an effective treatment of breakthrough pain [11], and intranasal fentanyl treats moderate to severe pain in children [12, 13]. Fentanyl causes different adverse-effects in infants and children [4]. Fentanyl produces different effects in infants and children [14-17]. Intravenous fentanyl reduces pain and induces sedation in infants and does not affect cerebral oxygenation or cardiac output in preterm infants [14], and fentanyl co-administered with bupivacaine during labour does not depress neonatal respiratory or adversely affect neurobehavioral scores in infants [15]. Intranasal fentanyl use during halothane or sevoflurane anaesthesia for tympanosotomy tube placement is associated reduced postoperative agitation without increase adverse-effects or discharge times [16]. There are significant correlations between fentanyl dosage and Neonatal Abstinence Score Tool [17]. Fentanyl is metabolized into norfentanyl by liver and intestinal CYP3A4 [18-20] and CYP3A4*1G genetic polymorphism affects the metabolic-rate of fentanyl [18]. The pharmacokinetics of fentanyl have been studied in infants and children [21]. The elimination half-life ranges from 208 to 1,266 min suggesting that fentanyl is rapidly cleared from the body and the distribution volume ranges from 1.92 to 15.2 L/kg. The remarkable variation in the elimination half-life and distribution volume is accounted by the wide variation in infants and children demographic characteristics. Fentanyl interacts with drugs [22-30]. Fentanyl and clarithromycin are metabolized by CYP3A4, and clarithromycin inhibits the metabolism of fentanyl and induce respiratory depression and death [22, 23]. The combination of fentanyl with neuromuscular blocking agents causes chest wall rigidity in two infants [24], and the co-administration of amitriptyline with fentanyl causes adverse-reactions [25]. Fentanyl is metabolized by CYP3A4 and the combination of drugs which are metabolized by this enzyme inhibits fentanyl metabolism causing excessive serum concentrations of fentanyl enhancing fentanyl effects [26]. Diltiazem and fentanyl are metabolized by CYP3A4 and fentanyl inhibits the metabolism of diltiazem causing high serum concentration of diltiazem which induces delirium [27]. The co-administration of fentanyl with ranitidine induces the risk of seizures [28]. Fentanyl inhibits the P-glycoprotein-mediated digoxin in Caco-2 cells [29]. Tacrolimus is metabolized by CYP3A4 and the combination of tacrolimus with fentanyl increase tacrolimus serum concentration and the dose of tacrolimus must be reduced when tacrolimus is co-administered with fentanyl [30]. The treatment of infants and children with fentanyl has been studied [31-36]. Fentanyl treatment of newborn infants during therapeutic hypothermia ameliorates neuroprotection in asphyxiated cooled newborn infants [31]. Fentanyl combined with midazolam is safe and more effective than midazolam alone for sedation therapy in mechanical ventilated children [32]. Enteral administration of methadone expedites fentanyl discontinuous and reduces the risk of withdrawal in critically ill children at high risk for opioid abstinence syndrome [33]. Transdermal fentanyl is useful for the treatment of moderate to severe chronic cancer pain [35], and the prophylactic fentanyl-droperidol prolongs the length-to-stay and recovery time and provides no discrete benefit over acetaminophen alone in paediatric strabismus repair [36]. The trials with fentanyl have been extensively reported in infants and children [37-43]. In preterm infants on mechanical ventilation, fentanyl protects the developing brain shortly after mechanics ventilation [37]. High cumulative fentanyl dose correlates with a higher incidence of cerebellar injury and lower cerebellar diameter in preterm infants [38]. Integrated pharmacokinetic/pharmacodynamic modelling showed that the dosing regimen of fentanyl in neonates may not provide the optimum sedation [39]. A short course of low dose fentanyl infusion reduces behavioural sedation, O2 desaturation, and neuroendocrine stress in preterm ventilated infants [40]. Fentanyl used for analgesia is superior to morphine produces fewer adverse-effects than morphine and it is superior to morphine for short-term postnatal analgesia in newborn infants [41]. Fentanyl reduces the incidence of emergence agitation in children undergoing general anaesthesia [42], and fentanyl decreases the incidence of agitation under sevoflurane anaesthesia in children and reduces postoperative pain but has a higher incidence of postoperative nausea and vomiting [43]. Fentanyl freely crosses the human placenta [44-48] and poorly migrates into the breast-milk [49-50].
In conclusion, fentanyl is a systemic opioid related to the phenylpiperidines and it is used in anaesthetic practice and in analgesia. The analgesic effect of fentanyl is about 100 times more potent than that of morphine. Fentanyl is highly lipid soluble, rapidly crosses the blood-brain-barrier, and the time to peak analgesic effect after intravenous administration is about 5 min. Following intravenous administration fentanyl is rapidly eliminated in plasma and in cerebrospinal fluid. Fentanyl may be administered intravenously, orally, or by intranasal, transdermal, or buccal application, the oral bioavailability is poor whereas the bioavailability following buccal administration is good. Fentanyl may cause nausea, vomiting, itching, and rigidity and the last is treated with neuromuscular-blocking agents. Fentanyl may decrease heart rate through vagal activation and may modestly decrease blood pressure. In infants, intravenous fentanyl is administered for short use, for sustained use, and during therapeutic hypothermia. In children, fentanyl is administered by intravenously or by transdermal or buccal application and fentanyl dose varies according to the child age and body-weight. Fentanyl has been found efficacy and safe in infants and children but it may cause adverse-effects. The effects caused by fentanyl, the treatment of infants and children with fentanyl, and the trials conducted with fentanyl in infants and children have been extensively studied. The pharmacokinetics of infants have been studied in infants and children and the elimination half-life of fentanyl ranges from 208 to 1,266 min suggesting that fentanyl is rapidly eliminated. Fentanyl is metabolized by CYP3A4 in both human liver and intestine and fentanyl interacts with drugs. Some interactions occur with drugs which are metabolized by CYP3A4; the co-administration of these drugs with fentanyl affect the fentanyl metabolism or pharmacokinetics. Fentanyl freely crosses the human placenta and poorly migrates into the beast-milk. The aim of this study is to review the clinical pharmacology of fentanyl in infants and children.
The authors declare no conflicts of financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employments, gifts, and honoraria.
This article is a review and drugs have not been administered to men or animals.
The author thanks Dr. Patrizia Ciucci and Dr. Francesco Varricchio, of the Medical Library of the University of Pisa, for retrieving the scientific literature.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
