AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Jan Van De Rakt, Physical Therapist NDT teacher IBITA, Course Leader and teacher on the Dutch Institute for Allied Health Sciences. Nursing Home “Waelwick” in Ewijk the Netherlands.
Citation: Jan Van De Rakt, Steve M. Grunwald, (2024), Can Disturbed Perception Be Improved Through Task-Specific Resistance Treatment at A Stroke Patient? J. General Medicine and Clinical Practice, 7(11); DOI:10.31579/2639-4162/187
Copyright: © 2024, Jan Van De Rakt. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 May 2024 | Accepted: 10 June 2024 | Published: 18 June 2024
Keywords: stroke; perception; task specific training; muscles- input-perception
Aid:
We know that the perception of people after an stroke is disturbed and that this give this people an extra problem to handle. We know further that when the tone is high and the selectivity is poor than the disturbances of the perception is often extreme. That give by some patients an fear that is almost not to understand.
Materials and Methods:
The purpose from this study is to try an intervention to improve the perception. The hypothesis that we try to prove the perception of his body sec but also in the environment was, that in the total program of the rehabilitation we explicit give more task-specific resistance treatment for the affected leg in stand phase to get through the better working of the muscle spindles and better coordination and through that also an better perception of his body sec but also of his body in his environment.
Results;
His power an coordination was clearly translate in better and faster walking in the exercise department and there were with adaptation some improvements in the ADL (Activities of Daily Living) at his home but the test of the perception of his body stay almost the same
Conclusion;
Improvements were absolute there but they were visible in the walking speed and walking with different aid. But the test that gives us an picture of the perception gave no great improvement. The passive test stay the same but when the muscle spindles were used there was an improvement and what was clear is that this cost an great amount of time over an long period and when the training stop the result were decreasing. Authorship credit: “Criteria authorship scientific article” has been used “Equal Contribution” (EC). Citation:
jan@vanderakt.nl
Impairment of the perception, the translation of input (from tactile, vibration, two-point discrimination, proprioceptive input etc. [1]. is the system that the literature is called the somatosensory afferent system. By person after an stroke is this system intact all away till the brain, but there are signals [2] that this system will adapt in time and his frequency of firing will decrease,
The biggest problem by patients after a stroke is assimilation of all input in the damage brain and the possibilities that this brain has to instructed the efferent system. Kluger [3] has investigated this and he found, that there is an delay in the transport and assimilation of stimuli and that can lead to less perception or as he called it “less perceptual awareness “. And his conclusion is therefore that through this the possibilities are obvious lesser. A small group of patients after an stroke, in the literature is not to find how much, had this problem such an problem that they never will build up an reasonable walking pattern. Walking stays for them a tremendous problem that so much asked that this people will choose for the wheelchair and walking rather try to avoided in the participation though the day. [4]
Case Gentlemen T.A.
A gentleman of now 55 years, who has 10 years ago had an severe stroke. Beside the loss of perception on his affected side, he has also a severe hemianopia, that makes his visual control extra difficult. Still, he lives independent, but much he doing sitting at home in a wheelchair, certainly because he was fallen at home and had broken his hip on the affected side. He was capable to walk with a hand-stick, behind a high chair but on the moment that someone asked him something or when he heart somethings strange than he stop withy walking. (Stop Walking When Talking - S.W.W. T. [5] When he was walking in the therapy with no aid or with an Nordic walking stick, often was than there the moment that stand still and dare not walk further and cry for help (freezing). He stays in that standing position and could only further when some give him an hand-on facilitation and he was often for an hour in panic, In the last year this behavior was increase and he was not able at home to pick something and walk with it, only walking with his stick was at home possible but that hasn’t no value because he couldn’t take something with him, therefore was the function in his affected arm/hand to bad.
Motricity Index (M.I.): Arm = 28: in shoulder14 and elbow 14 and hand 0.M.I.
Leg = 28 Hip 14, knee 14 en foot 0.[6]
His main question was:
Walk without in stick at home because otherwise this exercising has no value for me!”
This question means, that the perception must improve to get that degree of independent walking at his home. This must also be automatic so that he can focus on a task as carrying something through his house. As this automatism cannot achieve than he needs so many attentions for his walking that he is never capable to carry something through his house, certainly not a full glass!
Search in the literature.
From the past two books were know by us, that were books that pointed on the possibilities that perception/ sensorics /preprocess was an item that can improve through treatment The approach Rood [7] with skin stimulation direct above the muscle that must be stimulated was done by dorsal flexors of the foot and knee extensor muscles. This gave more feeling at the beginning but was often after two steps extinguish. The treatment according Yekutiel [8] was pointed on the treatment of the arm but the stimulation of the two discrimination – feeling can be very important for the foot. Now he feels his foot at the ground but not how and that he must control visual and that was an great problem. He was not capable to feel or he stand correctly on his foot and that he doesn’t fall backward when he lifts and place his not-affected foot. All this treatment has no value because his attention on the discrimination- possibilities of the foot was possible in sit but in stand wasn’t it possible that he makes attention free for this because he has it elsewhere needed. Search in PubMed gave as a result of 7 articles [,3,9,10,11,12,14,15] including 3 articles [9,11,12] that pointed on the “pusher-syndrome. That this is this case play an role was clear but there was no clear answer “how to stimulated the perception “. There were articles that focus on the Why and How important perception is [3,10] and only one article [14] try an treatment. This was done by giving electric stimuli on the fingers and that is seem possible that the discrimination- feeling was improved and that hold about 4 weeks after the treatment. Application of this electro therapy (TENS 50 Hrz-120µs) was a success in sit but after a few meters walking this feeling was gone.
Only Sato [15] that capable to show that on nerve level a brain level something change in the senso-motoric cortex as someone moves in water. This effect is only there when that part of the body was fully submerged and as that person moves. Well has Patten [18], but also in the guidelines of the Royal Dutch Society Physiotherapy [16] (K.N.G.F.), and [19/20] pointed out that muscle strengthening by stroke patients has an positive effect certainly in combination with task specific exercising, but to give an muscle- strengthening to get an improvement of the perception, seem to us an bridge to far. In his article give Martin Moons [1,13] clear how important it is that the muscle spindles are for the preprocess and the correct tension can change the perception. This is confirmed by Henri Kiers [17] in thesis about patient with back pain problems. In this thesis he proves that balance by back pain patient can be disturbed through this person let stand on an unstable platform and vibrated the low spine muscles. Vibration on the muscle is a method to influence the muscle spindles negative. Patients stand on a stable platform than the vibration on the back had no effect, but was the vibration on the calf muscles was the greatest disruption. On an unstable platform was the vibration of the back muscles the greatest disturbance by back pain patients. Therefore, less propriocepsis from the muscle’s spindles had an influence on the holding of the balance, certainly when the underground was unstable. Back complaints have a negative influence on the propriocepsis of the back muscle and that give an perception than was decreased. Patients after a stroke will have certainly an interruption of the function of the muscles spindles because the tone is often not normal, but would it be possible that task-specific training has an effect on it as by people with back pain? Task specific strengthening gave by an number of stroke patients an coordination improvement [18] Therefore could it be possible that the influence of the muscles spindles can improve the perception. But it must be task specific and that asked for an analysis of the walking performance and especially there where the biggest problem lies. Top trainers focus on that task-specific by injuries must almost perfect fit in the task- specific and that training of isolated muscles give an very difficult transfers to the task specific movement.[21]
Investigation question.
Is it possibility that task-specific muscle strengthening can improve the perception of the leg and had that as result that he can better walk and can we generate an form of automatic walking?
The participation level when he is walking must be so change so much, that he can use this on participation level the whole day at least at his own home!
To investigated this, we must know what during the walking performance the most difficult moment is and which muscles are at that moment essential. Through a strengthening of the group of this muscles or muscles pattern, must there create a grow of the feedback and that must create an greater feeling of security and more perception.
Analysis of the walking-pattern.
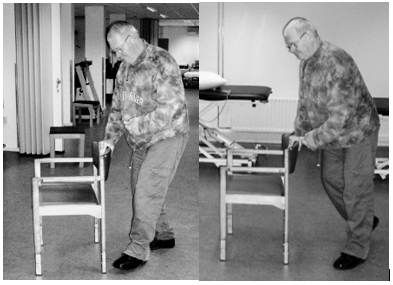
Photo 1 Photo 2
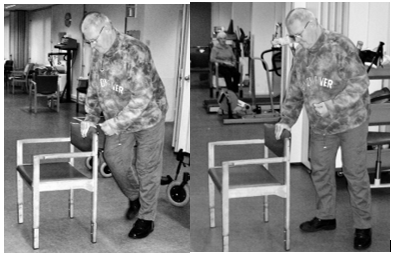
Photo 3 Photo 4
Analysis of the most difficult moment.
Photo 1.
Give a picture on the end of the swing phase en the start of the stand phase (“Heel strike) of the affected leg. There is on this way no real heel strike, because the tone in the plantar flexors in the leg is than so high that the foot is placed flat on the whole foot with almost no load. Further-one is the ankle mobility restricted to maximum of 90 ˢ. The ankle has an double peroneus string (EVO) with an T- aid to hold the ankle in the right position with not too much eversion. The foot is placed with a blow. Attempts to decrease the amount of striker foot are all failed. A test treatment with lidocaine gave a total loss of the perception and after that he couldn’t walk. Casting was for him no option because he couldn’t stay at home.
Photo 2
Loading response. The time between photo 1 -2 to 3 is long. This goes very slow and asked fora n great amount of attention
Photo 3 mid-stance.
Also, this moment to get the weight on his affected foot and make the not-affected foot ready for the swing phase cost also much time. He stays for some seconds complete still and his amount of support on the chair rest is great.
This is the moment that is goes wrong most of the time. When he isn’t certain that all is right, he will stop and in the best case he goes back but otherwise he will than cry for help.
Photo 4.
He stands again on his not-affected led and we see that the movement over his affected hip isn’t complete because through the restriction in the foot and in the hip, he must make and rotation away from his affected hip. A push-off of his affected leg isn’t present.
The moment with the greatest problems and with his greatest attention is the moment that he starts with placing load on his affected leg. Then is it important that he isn’t stand still too long because than the extinction take place and goes all wrong.
With the chair support in front of him he can solved this through take a huge amount of support on the chair. And through the position of the chair in front of him is a great amount of his body fast in front of the affected foot/leg. But when he walks with a stick or even without an aid than must there be an concentric contraction in his gluteal muscle to get an movement to the front, to come over or better along his affected foot. That contraction must he “experience” through the muscles spindles and his brain must register this – perception.
“Normal action “after the heel strike goes the movement as follow;
Prof. J. Buurke [22] in his thesis about walking that the heel strike is the moment for the great gluteal muscle to act. This more than enough power to “push” us over the hip. But by the patient in this casus is no heel strike present and he must build up this tension /contraction when he stands on his affected leg and that will happen when he lift his not-affected leg. But this contraction will not be concentric but a reaction on the elongation of the muscle. And the moment is with his body behind affected foot and will not transfer the body over the foot and hip. When we look to the diagonal principle [23,24,25]is the concentric action of the gluteal muscle an important part of the back diagonal but this muscle has mostly fast fiber structure and that is by people after a stroke a muscle that fast decrease or changes in a slow muscle. To get an action in this muscle or to activated this muscle the patient will use the whole diagonal, especially the part on the not-affected side and that is possible by using a stick to push away. Still, this asked for a concentric action also when this isn’t possible, therefore will the patient be lengthening the muscle. Lieber [26] write that this lengthening can give an action on spinal level, this is still no eccentric contraction, because than there is an action within the cortical area. This is only a stretch reaction on the muscle spindles and through the spine segment back to the muscle.
Looking at photo 2 and 3 and comparing this two with the other two, than is the amount of support on the backside of the chair gigantic. And his upper trunk moves almost over this backside. That means that the amount of pressure on his not-affected arm is great and that the back diagonal starts here and goes to the affected leg. There is a contraction in the gluteal because between photo 2 and 3 there is no more flexion in his hip. Still is there a change that the adductor muscle created the extension because the diagonal is maybe not ended in the “heart” of the hip.
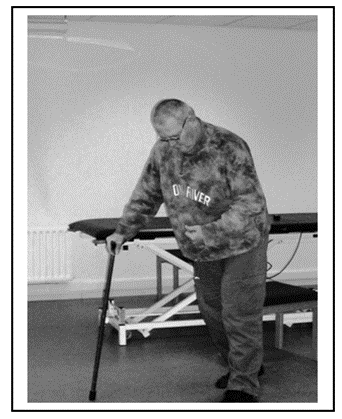
Photo 5: Look when he walks with a normal cane and compare it with walking behind a chair or special rollator frame. The placing of the cane is far in front of him and far lateral also. Still, he places a great amount of support to activated the back diagonal from the not-affected arm/upper trunk to the affected leg. Even the index finger pointing to floor must help to activated the extension power of his affected leg.
This moment was often very important! when he “feel” that his affected leg give an answer, he walks further but when that feeling wasn’t there than he freezes.
At the moment that he freezes no info came from his affected leg and he must have someone else to get him walk again. Therefore, he must “feel” his affected leg!!
Hypothese
Foto 5
Hypothesis
Would it be possible through Task Specific Resistance Therapy increase the concentric power of the gluteal muscles and would that have an effect on the coordination and also on the perception of the affected hip muscle
But first we must know what his perception possibilities are because than we can search for an improvement.
Test for Perception.
Test for perception is present but often debating about their validity.
Therefore, have we chosen for an combination of several test.
1. The propriocepsis and movement- feeling but almost never in the task itself. That means that we have an image of the perception but we need to create an translation to the task. The propriocepsis and movement –feeling was tested through the “Lage –und bewegungssinn” writing by Marks [27]and in the book “Assessment in der Neurorehabilitation” [28]) has the validity be studied:
2. “When the results are the number of degrees that the person has failed than this test is reasonable reliable “! Failures of more than 11° by great joint, and more than 5° by the knee. For the foot is this not sure but we hold more than 5 ° on. This test must be done in lying position and that is disadvantage because it isn’t in the task. The 10-meter walking test [29] makes clear what the possibilities of the patient are. Walking under supervision asked for a speed of 0,27 m/s, independent walking inside asked for a speed of 0.53 M/S and walking around the house asked more 0.70 m/s and normal walking is 1,17m/s, according Koolstra [29]. But it gives a clue what we need for an speed to stay independent with an walking capacity that is “automatic” more or less, but with an base of perception in it.
Stop Walking When Talking (S.W.W.T.) –test. This test we could use to test how far he was able to walk automatic”.
Before the task- specific training, the results of the 3 test on propriocepsis test ( A. mirror technique, B. movement feeling without active tension and C. with active tension were:
Test A.
Mirroring.
Knee 65 degree wrong – 3 times after each other tested (flexion – Extension movement)
Hip 50 degree wrong - 3 times after each other tested (flexion –Extension movement)
Exorotation from neutral position 15-20 degree wrong 3 times after each other tested.
Test B
Movement –feeling without active tension/movement.
Knee 40 degree wrong - 3 times after each other tested (Flexion-Extension)
Hip 50 degree wrong- 3 times after each other tested (Flexion –extension)
Exorotation from neutral position 15 degree wrong – 3 times after each other tested.
Test C
Movement –feeling with active movement.
Knee 20 degree wrong - 3 times after each other tested. (Flexion- Extension)
Hip 20 degree wrong -3 times after each other tested. (Flexion –extension)
Exorotation from neutral position 15 degree wrong – 3 times after each other tested.
Clear that in the case there is a great perception problem and he gave the best performance when he was able to move together with the investigator (test C). But this are test in lying or sitting position and impossible to test in stand but we have no wan indication what her “feel in his brain “.
10meter walking test
With different walking aids to achieve that the training was possible with much variation because we search for the best translation of the walking at his home later on.
Walking- test was done 3 times and the best [performance was recorded.
In this test, we choose to start at the highest level of speed he can perform, walking through the finish-line, this according Koolstra – on page 78 [29].
| 10 meter walking test | Time | M/S | M/m. | Km/h |
| 1. Walking- test behind high chair (photo 1) | 40 sec | 0.25 | 15 | 0.90 |
| 2. Walking -test behind special rollator frame (Photo 6) | 42 sec | 0.23 | 14.28 | 0.85 |
| 3. Walking -test with normal cane (photo 5) | 45 sec | 0.22 | 13.33 | 0.8 |
| 4. Walking-test with Nordic Walking stick. | Not possible | |||
| 5. Walking-test behind chair and with another task. S.W.W.T. | Not possible |
M/S = Meter per second. M/m = Meter per minute. Km/H= kilometers per hour.
Table 1: Impression for the start of the extra task-specific resistance training.
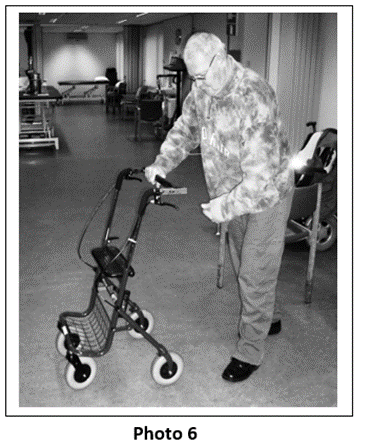
Photo 6: His walking attitude don’t change much. Every time is this moment the most difficult moment when he searches for the optimal situation that he feels that he can manage the load on his affected leg and can lift his not-affected leg to the front. A high amount of visual control, attention and an bended trunk to stretch the extensors of the hip. He cannot with this rollator frame go so far over the support point as with the chair and that is in influence of the rollator -form/wheels. His speed (table 1) is lower than the supervision speed of Koolstra (0.23 M/S - Koolstra 0,27 m/s.)
The base treatment was 3 times a week:
The extra part of the training was:
Ad 1. To get an good power training (strength × speed) for the gluteal muscle group in his task, thus when the movement over the affected hip take place and the affected leg is in the stand phase, wasn’t easy.
There were some problems that had to eliminated:
Translated this to the practice:

Photo 7: Task- Specific resistance training.
Resistance is given against the not-affected leg. This resistance is given through the whole swing movement when this possible. From the start when the not-affected leg stands behind the affected leg till the end at the start of the heel-strike of the not-affected leg. This to get a contraction in the extensor muscle of the affected hip in the stand-phase movement over the affected hip.
Problems that there were to start this program.
At the start the movement that he makes, was especially in the upper trunk. This he did, to get tension on the muscle Gluteus Maximum trough an elongation of the muscle. This would mean that this contraction was a contraction on spinal level and therefore will give no reaction in the brain and no perception improvement. Therefore, we must search how to inhibit the trunk elongation and more important how we can create an contraction in the hip extensors that has concentric elements. Because this element is supra-spinal and would have an effect in the brain. This was possible to do the movement without resistance but with a good stabilization of the affected leg and his trunk. After that we give an little resistance against the swing phase of the not-affected leg and now it was certain that the hip extensors gave an concentric contraction we could increase the resistance an little in the beginning. Often this give a cramp in the beginning and was it not possible to get the amount of rehearsal.
In the measurements can be find back as we look to the walking speed test. These measurements of the walking speed were done 4 times;
The second extra training was:
Statiek –Training. [30,31] The principle of the statiek training is that we give little pressure at the pelvis or at shoulder height to test the reaction of this person on that pressure. This pressure is given to the back, but also a pull to the front. Further can this also done on left and right side to assess or the person is capable immediately to react on that pressure. Second part is the reaction as this pressure is suddenly withdrawn. In this casus was the patient not capable to create a reaction as there is given pressure on the front, but also was not capable to given the right reaction on the not-affected side but there was a little reaction. The reaction when the pressure was gone was negative. Was this test done on shoulder height on the front there was almost no reaction. The pull on the back side gave an trunk inclination and at the end of the flexion was some resistance that means that he wasn’t capable to give resistance against this pull and must the gluteal muscle give an stretch to get an reaction. Never was he capable to get an situation that he brace the fall to the front by toe standing. After the training was this part still very difficult but there was at the end an reaction on the affected side and there was at the end an better reaction of the hip-extensor and some better balance. One leg standing G [RAMPS 32] at the beginning was standing on his affected leg impossible when there was no support on the not-affected side in the beginning an stable table, latter on an chair. And he must be first lifting his not- affected leg against resistance with support of an chair and then he could do an one leg standing at the end of the training period of 20 sec. with eyes always open.
| 10 meter Walking - test | Time | M/S | M/m | Km/h |
| 1.Walking test behind chair. | 38 sec | 0.26 | 15.78 | 0.94 |
| 2.Walking test behind special rollator frame. | 40 sec | 0.25 | 15 | 0.9 |
| 3. walking test with normal cane. | 42 sec | 0.23 | 14.28 | 0.85 |
| 4. Walking test with Nordic Walking Stick. | 60 sec | 0.16 | 10 | 0.6 |
| 5. Walking test with chair and extra task. S.W.W.T. | Not possible |
Table 2 -Task Specific Muscle Resistance Training and statiek after 10 weeks.
| 10 meter Walking test | Time | M/S | M/m | Km/h |
| 1. Walking test behind a chair. | 32 sec | 0.31 | 18.75 | 1.12 |
| 2. Walking test behind special rollator frame. | 34 sec | 0.29 | 17.64 | 1.05 |
| 3. Walking test with normal cane. | 36 sec | 0.27 | 16.66 | 1 |
| 4. Walking test with Nordic walking Stick. | 40 sec | 0.25 | 15 | 0.90 |
| 5. Walking test with chair and extra task. S.W.W.T. | Not Possible |
Table 3-Task Specific Muscle Resistance Training and statiek after 20 weeks.
| 10 meter Walking test | Time | M/S | M/m | Km/h |
| 1. Walking test behind chair. | 17 sec | 0.59 | 35,3 | 2.1 |
| 2. Walking test behind special rollator frame. | 19 | 0.53 | 31.6 | 1.9 |
| 3. Walking test with normal cane. | 20 sec | 0.5 | 30 | 1.8 |
| 4a. Walking test with Nordic walking Stick. | 21 sec | 0.48 | 28.6 | 1.7 |
| 4b. Walking test without a cane. | 3 meter | |||
| 5. Walking test with chair en extra task. S.W.W.T. | Not possible * |
Table 4- Task Specific Muscle Resistance Training and statiek after 30 weeks.
* in the three test-sessions, once he was able to walk through an make math. His time was 40 sec. over the 10-meter walking test.
Smallest Detectable Difference (SDD) for the 10-meter walking test is -- 0.16 m/s.
Improvement in the time.
| Start | 10 weeks | 20 weeks | 30 weeks | Difference Total | Difference 20-30 w | |
| Green chair | 0,25 | 0,26 | 0.31 | 0.59 | 0,34 ** | 0.28** |
| Special rollator frame | 0,23 | 0,25 | 0.29 | 0.53 | 0,3 ** | 0,24 ** |
| Normal cane | 0,22 | 0,23 | 0.27 | 0.5 | 0, 28 ** | 0.23** |
| Nordic Walking | - | 0,16 | 0.25 | 0.48 | 0,32 ** | 0,23 ** |
| Without | - | - | - | - | - | |
| Green chair and SWWT | - | - | - | - | - |
** all these values were above the SDD norm.
Perception developmental?
After the 10-20-30 weeks we have also done the perception tests and look at his attitude changes.
Participation level after 30 weeks;
There was a significant improvement in faster walking with an lot of aids.
In his apartment he was also faster with a normal cane and along the wall and the 3 meters without he uses in the kitchen.
Walking in the corridor was better but especially faster.
But open space, such as the mid of the therapeutic ward was still difficult.
There was therefore no generalization but a small participation improvement but only there were he had exercised and therefore also in his apartment.
After 10 weeks.
Test A Mirroring
Test B Movement feeling without active tension/movement.
Test C Movement feeling with active movement, own contribution.
Test A and B no change.
Test C there seem to be a difference, but that wasn’t expressing in degrees.
This was around the 20° for flexion/extension hip and knee and 15° exorotation in the hip.
After 20 weeks
Test A Mirroring
Test B Movement feeling without movement/tension.
Test C Movement feeling with active movement and own contribution.
Test A en B no change.
Test C again it looks like an progression but not measurable in degrees. Maybe that he knows the measurements now?
After 30 weeks.
Test A Mirroring
Test B Movement feeling without active tension/movement.
Test C Movement feeling with active movement and own contribution.
Test A and B they were different as 10 weeks before but the measurement was almost the same.
Test C Here was the change measurable: In the hip 5ᵒ less, now around the 15 ᵒ. Also, the knee 5 ᵒ lesser. The extension stays around the 20°for hip and knee.
The exorotation was still around the 15 ᵒ.
Attitude.
Increasing of the tone in the buttock muscle can also have an effect on the attitude, because the flexion of the trunk isn’t necessary anymore.

Photo 8 Photo 9
Photo 8: Walking with Nordic Walking Stick after 10 weeks. The horizontal line is equal with the radiator and then the inclination of the trunk. This angle is 25 ᵒ.
Photo 9
Walking after 30 weeks and the horizontal line is now fixed on the wall structure.
The angle is now 14 ᵒ.
That is a significant progression of 13ᵒ.
A significant improvement of the walking speed on the same place in the therapeutic ward of a nursing home but ……elsewhere? But the improvement of the perception through more coordination and power is a question that remain open, there is no answer from this investigation. But one conclusion can be done: there are signs that the last 10 weeks had the most changes and maybe we must do this over a much longer period. Also had his attitude improved and that is also a combination of muscle tone and perception. We also observed that he couldn’t keep this level on his own. In a holiday period he decreases with his speed on the level between 10 and 20 weeks. Are his participation possibilities increased? His stair raising is improved and he walks between the stairs through without a support. In the kitchen he works in standing position without a cane and is out his wheelchair what very difficult was in that small area. The remaining part of the house he walks along the wall and with a cane, but often with the cane off the ground. Again, the same feeling as with the walking speed, we stop too early. Further investigation by person with this degree of perception loss, this approach must do minimal 60 weeks with increasing difficulties and resistance.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
