AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Orlando Villarreal-Barrera, MD. Neurologic Endovascular Therapy Fellow, National Autonomous University of Mexico, Mexico Juarez Hospital. Instituto Politecnico Nacional Avenue 5160, Magdalena de las Salinas, Gustavo A. Madero Municipality, Mexico City, Me
Citation: Melo-Guzman G, Ramirez-Rodriguez JI, Ortiz Rafael J, Macias-Cortes EC, Sanchez-Garcia LM, Villarreal-Barrera OE (2022). Balloon expandable Stent utility for early Secondary Prevention of new Cerebral Ischemic events Caused by Intracranial Atherosclerotic Stenosis. Technical Nuances. J. Neuroscience and Neurological Surgery. 11(1); DOI:10.31579/2578-8868/220
Copyright: © 2022 Orlando Villarreal-Barrera, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 November 2021 | Accepted: 13 December 2021 | Published: 03 January 2022
Keywords: intracranial atherosclerotic disease; balloon coronary stent; stroke; symptomatic intracranial vascular stenosis
Objective: Recurrent cerebral ischemic events are estimated to appear in between 12-15% of symptomatic intracranial atherosclerotic disease (ICAD), regardless of the use of leading pharmacological therapies. Balloon expandable stent (balloon mounted coronary stent) could represent a feasible alternative in this disease’s treatment. This study pretends to report the balloon-expandable placement experience in our center.
Materials and Methods: A unicentric retrospective study dated between September 2009 and March 2018 was conducted. Patients previously diagnosed with ICAD and symptomatic stenosis treated with balloon-expandable stent were included. Clinical features, morbidity, mortality, short and long-term evolution, and pre-and post-treatment angiographic features were analyzed, as well as a mean 8 years-period follow-up. Data are presented as means, frequencies, and percentages for categorical variables, and ranks for continuous variables. Statistical analysis was carried by IBM SPSS Statistics Base V22.0 (IBM Corporation, Mexico). A Wilcoxon Signed-rank test statistical analysis was performed. Statistical significance was considered when a p-value lesser than 0.05 was measured for every result.
Results: A total of 6 patients with 7 affected vessels were treated, with an average age of 62.7 years. Affected and treated vessels were located in the Internal Carotid Artery (ICA) segment in 42.9%, Vertebral Artery (VA) V4 segment in 14.3%, Middle Cerebral Artery (MCA) M1 segment in 28.5%, and Posterior Cerebral Artery (PCA) P1 segment in 14.3%. The incidence of peri-operatory thrombotic events was 0%. Intracranial hemorrhage presented in 0% of cases. Recurrent ischemic or thrombotic events were not reported in a 97-months mean follow-up. 71.4% of patients scored ≤2 in the modified Rankin Score (mRS) pre-treatment, in a 90 day and 12-month follow-up. 100% presented a favorable evolution with mRS ≤2. Restenosis cases were not reported in radiologic control and retreatment was not needed in a 97-month mean follow-up.
Conclusions: This study suggests that balloon-expandable stent therapy with some technical endovascular variants for its navigation and placement could be a safe and effective alternative in the treatment of ICAD as a means of cerebral ischemic event early secondary prevention. We propose to consider not to limit endovascular treatment exclusively to those symptomatic ICAD patients refractory to medical-exclusive treatment, as a means to reduce the risk of presenting a new neurological deficit. Further expanded clinical trials are needed to confirm these findings and the advantage of this kind of stents against other kinds reported in the literature.
Intracranial atherosclerotic disease (ICAD) is a frequent cause of cerebral ischemic events in adults, it represents 10% of ischemic cerebral disease in the United States of America, 14.7% in Mexico, and 26% in the Asiatic and Afro-American population. [1-4] In addition to genetic and ethnic components, diabetes mellitus, systemic arterial hypertension, dyslipidemia, and smoking have been associated with a higher incidence of ICAD. [5]
ICAD representative clinical feature is transient ischemic attack, characterized by specific neurologic deficit such as hemiparesis, hemi-hypoesthesia, dysarthria, or amaurosis fugax. Neurologic deficits are related to anatomical vascular stenosis location, in the following order of appearance: Medial Cerebral Artery (MCA) 44.4%, Basilar Artery (BA) 18.5%, Internal Carotid Artery (ICA) 17.2%, Vertebral Artery (VA) 16.1%, Posterior Cerebral Artery (PCA) 2.15%, and vertebrobasilar junction 1.65%. [6]
ICAD neurologic deficit may be the consequence of thrombosis in a stenotic site, single or multiple perforating vessel occlusion by the atheromatous plaque, embolic event, or hypoperfusion. [7] Clinical treatment is based on lifestyle changes and risk-factor control such as diabetes mellitus, systemic arterial hypertension, hypercholesterolemia, and smoking, as well as pharmacological therapy with platelet antiaggregant, and statins. [7] Variability in clinical evolution in ICAD has been described for medical-exclusive treatment against endovascular therapy. [8,9] WASID (Warfarin versus Aspirin for Symptomatic Intracranial Disease) study states that the risk of recurrence of ischemic cerebrovascular disease depends on the stenosis grade, with 19% recurrence risk in 70-99% stenosis, and 10% risk in stenosis lesser than 70%. (10) SAMPRIS (Stenting versus Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis) describes a higher risk of recurrence posterior to endovascular stenosis treatment with non-coronary stent vs. medical-exclusive treatment in one-year follow-up (23.4% vs 12.0%). [11] VISSIT (Vitesse Intracranial Stent Study for Ischemic Stroke Therapy) study reports similar findings to those of SAMPRIS, with 36.2% recurrence for endovascular treatment with a non-coronary stent versus 15.15% for medical- exclusive treatment. [11,12]
Durst et al. described lesser morbidity than that previously reported (7.1%), when using balloon expandable stent in the secondary prevention of ischemic cerebrovascular disease in symptomatic patients with ICAD, despite medical treatment based on double platelet antiaggregant and statins. [13] Similarly, Mayer et al. reported a decreased frequency in ischemic disease with auto-expandable closed-cell stents (Acclino Stent). [14] Some authors consider that the discrepancy between SAMPRIS/VISSIT and other studies might be explained by the lack of experience of neuro interventional specialists in the use of the non-coronary stent (Wingspan Stent), combined with a complex technique that requires exchange of the micro guides in the stent positioning, demanding multiple steps for precise deployment. [13] Despite the best medical-exclusive treatment, a high frequency of ischemic cerebrovascular disease recurrence is reported (12-15.1%). Posterior to SAMPRIS, other studies have described a lessening in morbidity (2-4.4%) in symptomatic ICAD with treatment based on stents in selected patients. [15,16] Thus, our study aims to test the safety and efficiency of using balloon expandable stent with some technical deployment variants in early secondary prevention of patients with previous ischemic cerebrovascular disease.
Patient selection: a unicentric retrospective study dated between September 2009 and March 2018 was conducted, previously approved by our institution’s local bioethics and research committee (HJM 018/21R institutional protocol). All patients who met the study selection criteria that received treatment in the time period were considered to be included in the study. Confidentiality and anonymity were carried out in conformity to the Declaration of Helsinki.
Data collection was performed in our institute medical registry database and the following variables were considered: sex, comorbidity, localization of stenosis and occlusion grade, risk factors, grade of stenosis reduction posterior to stent placement, pre-and post-treatment modified Rankin Scale (mRS), pharmacological treatment with antiaggregant or statins, peri-operatory adverse events, and imageology control with computed axial tomography and magnetic resonance image. [13-15].
The inclusion criteria were age between 18-85 years old, patients referred from Neurology to Endovascular Neurological Therapy, atherosclerotic disease confirmed by angiography, with stenosis grade of 60-99% in a major intracranial artery, and previous ischemic cerebrovascular disease related to the anatomical site of vessel stenosis. A single patient was excluded, with V4 segment stenosis treated by stent placement as this patient did not present neurological symptoms associated with this vascular territory. Posterior to the first symptomatic stroke, and confirming by imagenology, all patients were started on statins and antiaggregant in a period of one month, to afterward carry out endovascular treatment by balloon expandable stent. The exclusion criteria were an absence of post-treatment institutional clinical follow-up, a partial or total absence of clinical information relevant to the study in the institutional clinical record, and treatment with at least one type of stent other than balloon expandable. [13,15]
Stenosis grading was performed by the WASID method using angiographic images obtained by digital subtraction: [(1 − (Dstenosis/Dnormal))] × 100, where Dstenosis = the luminal diameter of the artery at the most severe stenosis site and Dnormal = the diameter of the proximal normal artery. [10]
A series of 7 affected vessels in 6 patients treated with balloon expandable stent was assessed, with presential follow-up initially, and posteriorly by telephone with a mean follow-up of 97-months, in order to evaluate all complications in long-term clinical follow-up from the endovascular treatment to the collecting data date in clinical records.
Processing: Previous informed consent was obtained of all patients. They received dual antiaggregant treatment with acetylsalicylic acid (ASA) 325mg and clopidogrel 75mg, with a minimal administration period of 7 days previous to endovascular therapy treatment. Platelet reactivity tests were not possible due to technical reasons of the institute. In all cases, endovascular treatment was performed after 14 days from the last symptomatic ischemic vascular event by an experienced neuro interventionalist. [18]
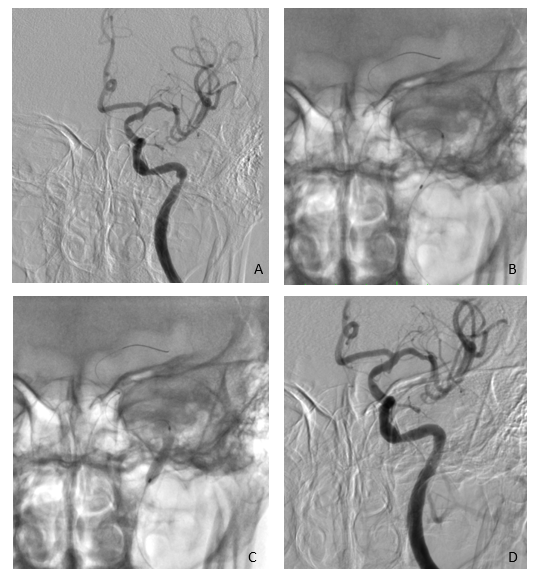
Siemen’s monoplane angiography was used. Prior to the procedure, every dispositive was irrigated, and the guide catheter was plugged to a constant saline 0.9% infusion at an 800ml/h rate and the microcatheter was plugged to a 150ml/h infusion rate. Intravenous heparin bolus was not administered. Every procedure was performed under general anesthesia, perioperative systolic blood pressure was kept between 90mm Hg to 120mm Hg. The right femoral artery was catheterized by a 6Fr sheath as vascular access of preference. 6 vessel angiographies were executed, and stenosis grade was assessed by the WASID method. A Guider 6Fr (Stryker) alone or Multipurpose guide catheter 7 Fr (Boston Scientific®) together with an Intracranial Support Catheter Navien® (ev3) 6 Fr were used in those cases with tortuosity vessels proximal to the stenosis site. The Tsunami Gold® (Terumo) or Taxus Liberté® and Rebel® (Boston Scientific) Coronary Stent were introduced using a Trascend® microwire, with the support of RoadMap fluoroscopy to reach the stenosis site. Angiographic stent positioning confirmation and a micro guide retraction until the soft tip would be inside the stent were performed. Afterward, balloon angioplasty was performed, inflating the balloon at 1 atmosphere below maximal particular nominal of each device, in a lapse of 30 seconds. Angiographic control was performed immediately and after 10 minutes to evaluate residual stenosis and late thrombus formation in the stent placement vascular territory (Figure 1-3). Dual platelet antiaggregant was extended 6-months posterior to the intervention, and afterward, only ASA treatment was kept. [10,13,19]
Clinical evaluation: Clinical parameters assessed in follow-up were new neurological deficit related to the treated vascular territory confirmed by computed axial tomography or magnetic resonance image, ischemic or hemorrhagic cerebrovascular disease, and morbimortality assessed by pre-treatment mRS and at 90-day and 1-year post-treatment. The recurrence of an ischemic or hemorrhagic cerebrovascular event was also evaluated in a mean follow-up of 97 months. [13]
Radiologic evaluation: Computer tomography angiography control was
performed 12-months posterior to the intervention, evaluating possible subsequent vascular pathology, late thrombotic events, inadequate stent positioning or migration, and recurrent stenosis, defined as 50% or higher residual stenosis posterior to stent placement. [13] These findings were reported by two independent neuroradiologists.
Statistical Analysis: Epidemiologic and radiologic data were obtained via institutional medical registry base, in concordance to confidentiality and anonymity standard. Data are presented as means, frequencies, and percentages for categorical variables, and ranks for continuous variables. Statistical analysis was carried by IBM SPSS Statistics Base V22.0 (IBM Corporation, Mexico). A Wilcoxon Signed-rank test statistical analysis was performed. A logistical regression model was used to estimate the association of variables. Statistical significance was considered when a p-value lesser than 0.05 was measured for every result.


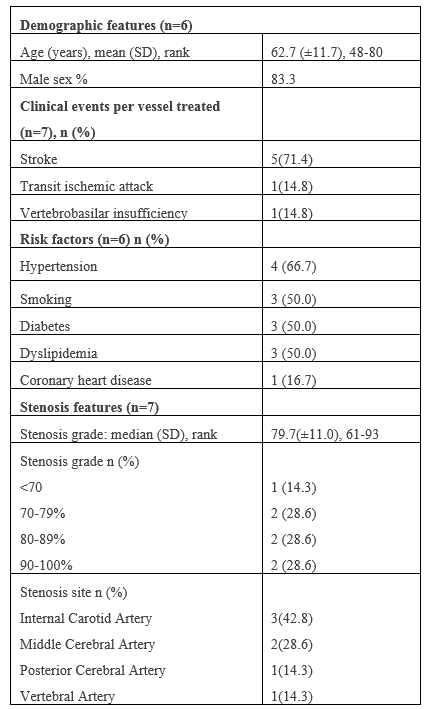
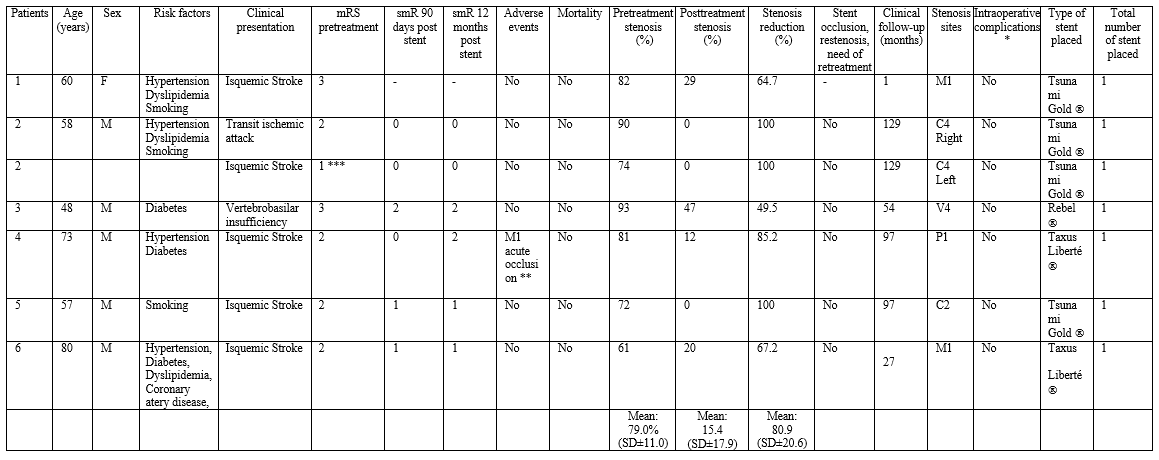
In a period between September 2009 and March 2018, a total of 6 patients with 7 symptomatic affected vessels were treated using balloon expandable stent. Average age of presentation was 62.7-years old ±11.7 (SD 48-80), and 83% of cases were in male patients. Clinical presentation was concordant with an ischemic cerebrovascular disease in 71.4%, transient ischemic attack in 14.3%, and vertebrobasilar insufficiency in 14.3% of all vessels treated. Identified risk factors were systemic arterial hypertension (66.7%), diabetes mellitus (50.0%), dyslipidemia (50%), smoking (50.0%) and coronary artery disease (16.7%). Evidence of previously diagnosed peripheral occlusive vascular disease or atrial fibrillation was not documented. A single patient presented with multiple stenoses requiring treatment in two different vascular territories. Posterior circulation was compromised in 2 cases, whereas 5 vessels corresponded to anterior circulation. Affected vessel location was: ICA C2 and C4 segment in 42.9%, MCA M1 segment in 28.5%, VA V4 segment in 14.3%, and PCA P1 segment in 14.3%. (Table 1)
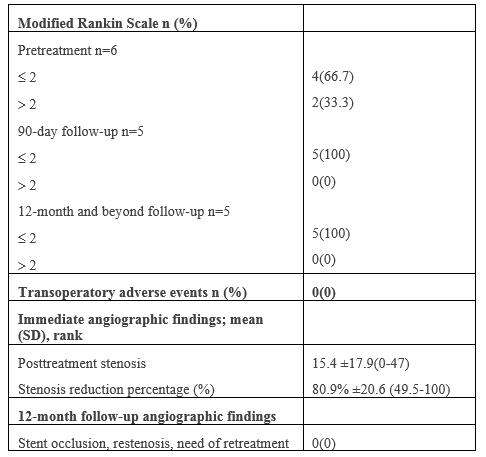
Immediate hemorrhagic or thromboembolic in the trans operatory period was not presented (Table 2). Early peri-operatory morbidity/mortality (<30>30 days) were not reported in any case. One patient presented a thromboembolic event in the MCA M2 segment that required mechanical thrombectomy 9 months posterior of the stent placement to treat PCA P1 segment stenosis, this event was not considered as a late adverse event as it involved a different vascular territory. No new adverse events were reported in a median 97-month follow-up (SD ± 50.0). Risk factors or other features as adverse events predictors were not possible to identify using logistical regression analysis due to small sample size.
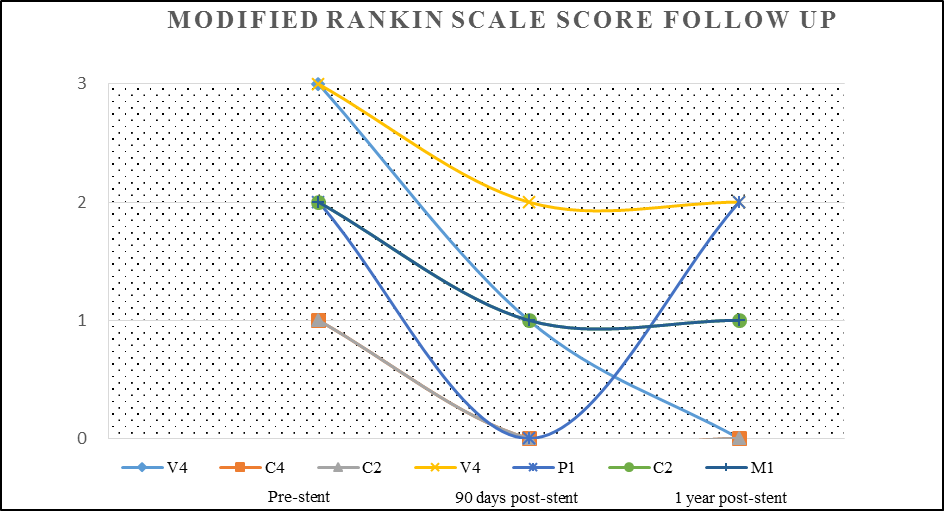
Prior to endovascular neurological therapy treatment, 66.7% of the patients presented with a mRS score of ≤2, in the post-treatment clinical assessments at 90-days and 12-motnhs, a favorable outcome with a mRS score of ≤2 was reported in 100% of cases (Table 2, Figure 4).
A total of 7 stents were used to treat 7 intracranial vascular stenosis. No technical complications were documented during endovascular approaches. Pre- or post-dilation of the affected vessel in stent liberation was not needed in any case. Radiological follow-up was done in 85.7% of patients in a period of 12-months or less, posterior to the endovascular treatment. There was no evidence of recurrent stenosis, new
thromboembolic event related to the treated vascular territory, inadequate stent positioning or migration, and there was no need for new procedures in previously treated vessels in any case. (Table 2)
Pre-treatment stenosis grade was 79.0% (SD±11.0), and 15.4% (SD±17.9) in the post-treatment (p=0.008) and immediate stenosis grade reduction was reported in 80.9% (SD±20.6). (Table 3)
Findings in this study suggest that ICAD’s treatment with balloon expandable stent placement by neurologic endovascular therapy is safe and feasible and presents with a low rate of complications related to the dispositive, ischemic cerebrovascular disease recurrence and mortality. Neurologic endovascular therapy should be reconsidered as a viable treatment alternative in the secondary prevention of ICAD. Even if SAMPRIS and VISSIT studies report a higher incidence of ischemic cerebrovascular disease in 12 months post-treatment in groups treated with medical therapy and stenting versus medical-exclusive treatment, the risk of recurrence in the last group is still high. Inclusion criteria and treatment modality were based upon medical-exclusive treatment presenting a failure rate of 12.0%-15.5% in preventing new strokes in those patients with previous ischemic vascular cerebral disease, compared to 2-4.4% of recurrence in those that receive combined medical and endovascular treatment. [11,12,15,16] Thus, early endovascular therapy performance can reduce the risk of a subsequent ischemic event in patients receiving medical treatment. [12,15]
In this study, posterior to endovascular treatment in 7 vessels, no complications were reported. A single symptomatic VA V4 segment and one in PCA P1 segment were treated and no technical periprocedural adverse events were reported in this subgroup. Compter et al. described in phase II clinical trial of symptomatic stenosis superior to 50% of the VA treated with stent placement, a morbidity rate of 22.3% for medical-exclusive treatment and 24.6% for stent placement. [17] In the morbidity of the stent group, 3.5% were represented by hemorrhagic cerebrovascular disease, and a mortality of 1.7% was reported. Despite these findings, the potential benefit from stent endovascular placement in the treatment of symptomatic stenosis of the vertebrobasilar circulation has shown a lesser accumulative risk of presenting cerebrovascular adverse events, compared to treatment in the anterior circulation, which may indicate a long-term significative benefit. [13,17]
In an 8-year follow-up, recurrent thrombotic disease, restenosis, or other adverse events were not reported. This frequency of complications reported in stent-based treatment is low and could be related to drug-eluting stents implementation (2 of 7 treated vessels), which may perhaps lessen hyperplasia rate, and subsequently, the need for retreatment caused by stenosis or occlusion. [13] Although the use of medicated balloon expandable stents for the treatment of intracranial stenosis has been shown to be a viable alternative, with an apparent decrease in restenosis rates compared to non-medicated stents, there is little data available to justify their use or certain benefit of one type of stent over the other. [20,21]
Some authors attribute an increased morbimortality in groups treated with stent-based therapy to vascular lesions or thromboembolic events triggered by micro guide exchange maneuvers, need of angioplasty prior to stent placement, and in some cases, the necessity of an additional angioplasty. [13] Similarly, previous articles indicate the deployment of the balloon-expandable stent over the rigid segment of the micro guidewire at the site of the stenosis. [19.22]. In our experience, positioning the floppy end of the micro guidewire over the site of the stenosis just before deploying the stent allows it to have a better apposition to the atherosclerotic plaque and vessel walls immediately adjacent to the site of the stenosis, which could theoretically reduce ischemic events due to distal migration of plaque fragments. (Figure 3.C)
The balloon expandable stents utility may be limited for intracranial use in patients with tortuous vascular anatomy. This is due to the feature that its delivery system is relatively rigid; based on this fact we use in selected cases an intracranial support catheter Navien® (Ev3) 6 Fr with 0.072” lumen which we place up to the supraclinoid segment of the internal carotid artery allowing us to navigate the stent without difficulty. The use of this type of catheter and the CAT 5® (Stryker), has been previously described as an adjunct for balloon expandable stent navigation in patients with large vessel occlusion associated with intracranial atherosclerotic stenosis. This is associated with higher technical success rates and recanalization but also with higher rates of bleeding and mortality, probably related to multiple previous failed attempts of thrombectomy using stent retriever. [19]
In addition to the technique used to navigate the stent, we consider that insufflating the balloon one atmosphere below the particular nominal value for each stent in order to achieve submaximal angioplasty, theoretically reduces the risk of plaque fragmentation, embolic and hemorrhagic phenomena, and perforators arteries occlusion due to possible plaque mobilization. [23,24] The usefulness of submaximal balloon angioplasty without the use of a stent has been previously described in a meta-analysis by Seyedsaadat et al, where they reported a technical success rate of 93% with a low incidence of stroke in the first 30 days and at one year of follow-up (3% and 5% respectively). [6]
Our study describes a single-step deployment for stents, opposing the multiple phases previously described; the use of submaximal stent angioplasty, and the use of distal access catheter that facilitates navigability, as well as variations in the positioning of the micro guidewire at the time of stent release, all which could be some of the factors that decrease the rate of adverse events.
From the total of patients that received a follow-up longer than 12 months in our study (83.3%), 100% showed a favorable clinical evolution (mRS score 0-2).
The limitations of this study include a small sample size that did not allow a logistic regression analysis for the association of risk factors, its retrospective and non-randomized nature, selection bias of anatomically favorable lesions to be treated by neurological endovascular therapy, and lack of a control group verifying the efficacy of this treatment modality.
At the moment, there are reports of large cohorts describing success in balloon expandable stent usage in patients with recurrent ischemic vascular cerebral disease, secondary to medical exclusive treatment failure. The value in this study relies on its extended period of time follow-up compared to other studies, reporting the feasibility and safety in the employment of these devices with some technical variants for their navigation and placement in early-stage symptomatic patients that received medical exclusive treatment. We propose not to limit endovascular treatment exclusively to those symptomatic ICAD patients refractory to medical-exclusive treatment, as a means to reduce the risk of presenting new neurological deficit.
A bigger sample size clinical trial is needed, with the employment of expandable balloon stents using similar criteria selection in an early stage prior to a new ischemic event, to verify the superiority of this therapeutic modality against medical exclusive treatment or other stent types used in the treatment of ICAD.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
