AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Ayman M Abu Mustafa, Palestine College of Nursing, Ministry of Health, Khan Younis, Gaza Strip, Palestine.
Citation: Mohamad S. Alhamss, Ahmad M. Tabash, Abdrabbou M. Elregeb, Ayman M. A Mustafa2, Asmaa A. Hejazi, et al. (2021) Assessment of biochemical parameters and hematological profile in the chronic renal failure of pre and post dialysis at Martyr Mohammed El-Najjar Hospital in Rafah, Gaza Strip, Palestine. International Journal of Clinical Case Reports and Reviews. 6(1); DOI: 10.31579/2690-4861/097
Copyright: © 2021 Ayman M. Abu Mustafa, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 November 2020 | Accepted: 30 December 2020 | Published: 07 January 2021
Keywords: biochemical parameters; hematological profile; chronic renal failure; martyr mohammed el-najjar hospital; rafah, gaza strip; palestine
Background: There are limited data on the assessment biochemical and hematological profile in the chronic renal failure of pre and post dialysis in the Gaza Strip.
Objective: To evaluating some biochemical parameters and hematological profile in the chronic renal failure of pre and post dialysis at Martyr Mohammed El-Najjar Hospital in Rafah, Gaza Strip, Palestine.
Methods: Forty-three (end-stage renal disease) ESRD patients, aged 20-70 years old who were referred to Martyr Mohammed Youssef Al-Najjar Hospital in Rafah for the dialysis department. 43 apparently healthy individuals matched for ages were used as a control group for comparisons.
Results: The results showed that post-dialysis higher statistically significant in Hb, RBC, HCT, PLT, AST, ALT, ALP and Ca level than pre-dialysis. While Ph, WBC, RDW, creatinine, Urea was lower statistically significant in post-dialysis than pre-dialysis (P < 0.05).
Conclusion: chronic kidney disease shows abnormal hematological parameters, precisely reduced levels of RBC count, hemoglobin, hematocrit, and platelet count, in addition, pre-dialysis patients are more anemic and thrombocytopenic than post-dialysis patients and this is may indicate of lack of blood pressure and diabetic control in these patients. AST& ALT activities vary in concentration before and after dialysis and make the post-dialysis patients are higher than pre-dialysis.
The kidney is a vital organ that eliminates waste and extra water from the blood and preserves electrolytes balance such as sodium, potassium, and calcium normally in the body (Yang et al., 2014). the kidneys also control blood pressure and stimulate erythropoiesis (Santoro et al., 2015).
Kidney failure, also known as End-stage renal disease means kidneys are only functioning at 10 to 15% of their normal capacity and with GFR of 15ml/min or less (Alexander et al., 2012). It is can occur suddenly or slowly (Bindroo & Challa, 2018).
There are several options for treating kidney failure including kidney transplant, hemodialysis and peritoneal dialysis (de Francisco, 2010). Hemodialysis is a process of purifying the blood and eliminating waste products such as creatinine and urea and free water from the blood and correct electrolyte imbalance (Vadakedath & Kandi, 2017).
The hematological disturbance is common in chronic kidney disease (CKD) due to relative deficiency/reduction in erythropoietin (EPO) production and other factors such as increased hemolysis, suppression of bone marrow erythropoiesis, and hematuria and gastrointestinal blood loss (Islam et al., 2015).
Creatinine is created in the muscles by the non-enzymatic changes of creatine and phosphocreatine. Plasma levels of creatinine reflect endogenous production and GFR. Therefore it is an excellent indicator of assessment of renal function. Urea is an organic compound, playing a vital role in the metabolism of nitrogen-containing compounds (NPN). Urea is a major excretory product of protein metabolism.90% of it is excreted through the kidneys and kidney disease is associated with accumulation of urea in the blood. The concentration of urea in plasma is determined by renal function and perfusion, the protein content of the diet and the amount of protein catabolism (Amin et al., 2014).
The serum liver enzymes most commonly used to evaluate the diagnosis of hepatobiliary disorders include the alkaline phosphatase (ALP), aspartate aminotransferase (AST) and alanine aminotransferase (ALT). ALT and AST are routinely measured to evaluate liver functions in patients with and without renal failure (Kakey & Abdoulrahman, 2017). Serum ALP increases in patients with chronic kidney disease (CKD). ALP may be related to cardiovascular calcification in CKD (Lomashvili et al., 2008). The alanine aminotransferase ALT is normally present in the circulation in low concentrations, usually less than 40 IU/L. The concentrations of serum ALT in both chronic dialysis and CRF patients most commonly fall within the lower end of the range of normal values (Lopes et al., 2009).
Calcium is one of the key elements to be considered in patients on dialysis due to its relationship with cardiovascular risk (Maduell et al., 2012). Accurate assessment of calcium balance in patients on hemodialysis (HD) is crucial. A negative calcium balance can cause hemodynamic instability, muscle cramps, secondary hyperparathyroidism and loss of BMD. A positive calcium balance may lead to hypercalcemia, vascular calcification and increased cardiovascular morbidity and mortality (Bech et al., 2013).
An increase in the risk of cardiovascular morbidity and mortality due to chronic hyperphosphatemia in patients undergoing hemodialysis has been demonstrated (Kendrick & Chonchol, 2011).
Chronic renal failure (CRF) is associated with increased levels of some biochemical parameters and decreased others. Hence; we evaluated the pre-dialysis and post-dialysis mean values of serum renal biochemical markers in CRF patients undergoing dialysis to elucidate the effect of dialysis on CRF patients.
Objectives of the study
The main objective of this study
The general goal of the study is to determine to evaluate some biochemical parameters and hematological profile in the chronic renal failure of pre and post dialysis at Martyr Mohammed El-Najjar Hospital in Rafah, Gaza Strip, Palestine.
Material and methods
Study Design:
The present study is a case-control study.
Target Population:
The study included patients with renal failure (males and females) under hemodialysis. aged (20-70) years old among Rafah patients.
Study Setting
The researcher was visiting the department of dialysis for easy collection.
Sample Size:
The population of the study includes 43 (end-stage renal disease) ESRD patients, aged 20-70 years old who were referred to Martyr Mohammed Youssef Al-Najjar Hospital in Rafah for the dialysis department. 43 apparently healthy individuals matched for ages were used as a control group for comparisons.
Distribution of samples
The study will conduct in the dialysis department in Martyr Mohammed Youssef Al-Najjar Hospital in Rafah.
Period of the study
The study will carry out during the period from September 2019 to September 2020.
Inclusion and Exclusion criteria
Inclusion criteria include the case:
- All the patients suffering from chronic kidney disease
- Aged (20-70) years old.
Inclusion criteria include of control:
- Apparently healthy individuals.
- Aged between (20-70) years old.
Exclusion criteria
- Patients under 20 years of age.
- Patients more than 70 years of age.
- Patients with schizophrenia, obesity, cancer, Alzheimer’s disease,
Vascular dementia, and hepatitis.
- Pregnant and lactating women.
Ethical Consideration
A Consent form to participate in the study will obtain from the participants. Every participant was provided with a full explanation of the intended study.
Data collection
Pilot study
A pilot study will conduct for five participants to identify any problem in research design before starting for data collection
Questionnaire interview
An interview will use for filling in questionnaires that designed for matching the study need of the study population. All interviews will conduct face to face by the researcher. During the survey, the interview will explain any of the questions that were not clear. The questionnaire will base on the questions of previous studies with some modifications. The questionnaire will include questions on the socio-demographic data e.g. age, university level.
Sampling and study parameters
Blood was collected in a plain top tube (serum). Whole blood will collect and test for 2 hours. The serum is stable 4 days at (2-8°C) or 24 hours at room temperature (15–30°C). The hemolysis of the sample is not applicable. Allow sample tubes to reach room temperature (15–30°C) before performing the assay. Also, the complete blood count will collect in the EDTA tube.
All tests will conduct twice; the first time pre-dialysis in case. The second time, post-dialysis treatment in the case. Statistical Analysis
Statistical analyses will form with SPSS version 22.
Socio-demographic characteristics of the study population
Table (1) shows that 14% of cases and controls aged between 20 –30years, 9% vs. 12% aged between 31 – 41years, 21% vs. 23% aged between 42 – 52years, 33% vs. 35% aged between 53-63years and 23% vs. 16% aged between 64-74 years (P= 0.9). In addition, 30% of cases and 28% of controls had primary school education, 47% vs. 44% had secondary school education and 23% vs. 28% had a university education (P= 0.9). Furthermore, 53% of cases were males, 47% were females, and 60% of controls were males and 40% were females (P= 0.5).
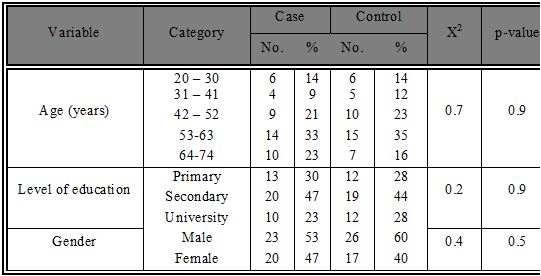
The significance of difference was checked by the chi-square test (compare study group and control), significant at P ≤ 0.05.
Table 2 shows that there were statistically significant differences at 0.05 in Hb level between (cases) pre-dialysis (mean = 8.7) and control (mean = 13.3), P-value 0.001, which means that Hb level was significantly lower among pre-dialysis compared to control. Also, there were statistically significant differences at 0.05 in RBC between cases (mean = 3.1) and controls (mean = 5.0), P-value 0.001, which means that RBC was significantly lower among cases compared to controls. In addition, there were statistically significant differences at 0.05 in WBCs between cases (mean = 4.7) and controls (mean = 5.8), P-value 0.001, which means that WBCs were significantly lower among cases compared to controls. The results also show that there were statistically significant differences at 0.05 in HCT level between cases (mean = 27.4) and controls (mean = 39.9), P-value 0.000, which means that the HCT level was significantly lower among cases compared to controls. Furthermore, there were statistically significant differences at 0.05 in MCH level between cases (mean = 27.9) and controls (mean = 29.1), P-value 0.005, which means that MCH level was significantly lower among cases compared to controls. Also, there were statistically significant differences at 0.05 in the MCHC level between cases (mean = 31.7) and controls (mean = 32.7), P-value 0.005, which means that the MCHC level was significantly lower among cases compared to controls. In addition, there were statistically significant differences at 0.05 in PLT between cases (mean = 126.3) and controls (mean = 264.7), P-value 0.001, which means that PLT was significantly lower among cases compared to controls. On the other hand, there were statistically insignificant differences between the two groups in levels of MCV (P= 0.873) and RDW (P= 1.000).
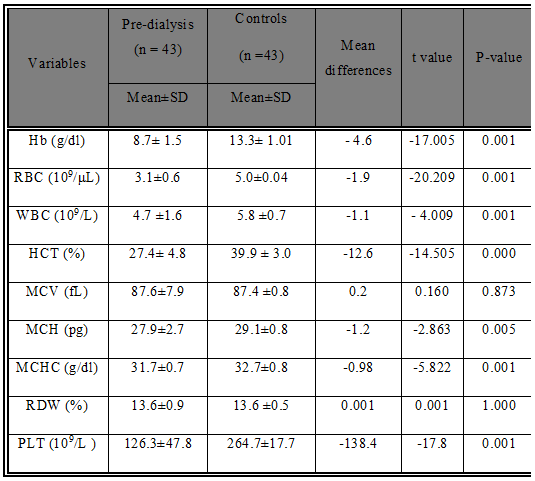
Hb: hemoglobin; RBC: red blood cell; WBC: white blood cell; HCT: hematocrit; MCV: mean corpuscular volume; MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration; RDW: red cell distribution width; PLT: platelets. Significant: p< 0.05.
Table 3 shows that there were statistically significant differences at 0.05 in Hb level between (cases) post-dialysis (mean = 9.4) and control (mean = 13.3), P-value 0.001, which means that Hb level was significantly lower among pre-dialysis compared to control. Also, there were statistically significant differences at 0.05 in RBC between cases (mean = 3.4) and controls (mean = 5.0), P-value 0.001, which means that RBC was significantly lower among cases compared to controls. In addition, there were statistically significant differences at 0.05 in WBCs between cases (mean = 4.5) and controls (mean = 5.9), P-value 0.001, which means that WBCs were significantly lower among cases compared to controls. The results also show that there were statistically significant differences at 0.05 in HCT level between cases (mean = 29.7) and controls (mean = 39.9), P-value 0.000, which means that the HCT level was significantly lower among cases compared to controls. Furthermore, there were statistically significant differences at 0.05 in MCH level between cases (mean = 27.9) and controls (mean = 29.1), P-value 0.005, which means that MCH level was significantly lower among cases compared to controls. Also, there were statistically significant differences at 0.05 in MCHC level between cases (mean = 31.8) and controls (mean = 32.7), P-value 0.005, which means that the MCHC level was significantly lower among cases compared to controls. In addition, there were statistically significant differences at 0.05 in PLT between cases (mean = 119.6) and controls (mean = 264.7), P-value 0.001, which means that PLT was significantly lower among cases compared to controls. On the other hand, there were statistically insignificant differences between the two groups in levels of MCV (P= 0.937) and RDW (P= 0.417).
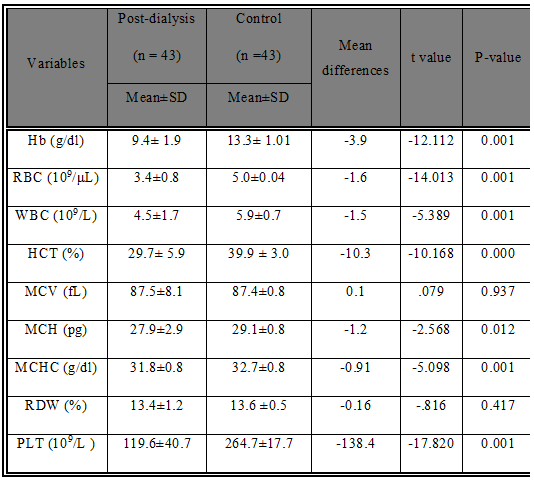
The significance of difference was checked by t-test (compare all case and control), significant at P ≤ 0.05.
Table 4 shows that there were statistically significant differences at 0.05 in Hb level between pre-dialysis (mean = 8.7) and post-dialysis (mean = 9.4), P-value 0.001, which means that Hb level was significantly lower among pre-dialysis compared to post-dialysis. Also, there were statistically significant differences at 0.05 in RBC between pre-dialysis (mean = 3.1) and post-dialysis (mean = 3.4), P-value 0.001, which means that RBC was significantly lower among pre-dialysis compared to post-dialysis. In addition, there were statistically significant differences at 0.05 in WBCs between pre-dialysis (mean = 4.7) and post-dialysis (mean = 4.5), P-value 0.001, which means that WBCs were significantly higher among pre-dialysis compared to post-dialysis. The results also show that there were statistically significant differences at 0.05 in the HCT level between pre-dialysis (mean = 27.4) and post-dialysis (mean = 29.7), P-value 0.000, which means that HCT level was significantly lower among pre-dialysis compared to post-dialysis. Furthermore, there were statistically significant differences at 0.05 in the RDW level between pre-dialysis (mean = 13.6) and post-dialysis (mean = 13.5), P-value 0.031, which means that RDW level was significantly higher among pre-dialysis compared to post-dialysis. In addition, there were statistically significant differences at 0.05 in PLT between pre-dialysis (mean = 126.3) and post-dialysis (mean = 119.6), P-value 0.001, which means that PLT was significantly higher among pre-dialysis compared to post-dialysis. On the other hand, there were statistically insignificant differences between the two groups in levels of MCV (P= 0. .319), MCH (P= 0.486), MCHC (P= 0.412) and RDW (P= 0.417).
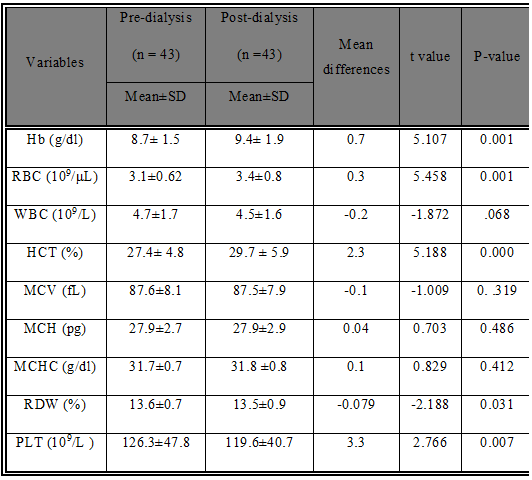
The significance of difference was checked by t-test (compare all case and control), significant at P ≤ 0.05.
Table 5 shows that there were statistically significant differences at 0.05 in creatinine level between (cases) pre-dialysis (mean = 8.5) and control (mean = 0.8), P-value 0.001, which means that creatinine level was significantly higher among pre-dialysis compared to control. Also, there were statistically significant differences at 0.05 in urea between cases (mean = 150.8) and controls (mean = 35.6), P-value 0.001, which means that urea were significantly higher among cases compared to controls. In addition, there were statistically significant differences at 0.05 in AST between cases (mean = 20.1) and controls (mean = 28.6), P-value 0.001, which means that AST was significantly lower among cases compared to controls. The results also show that there were statistically significant differences at 0.05 in ALT level between cases (mean = 20.7) and controls (mean = 29.1), P-value 0.000, which means that ALT level was significantly lower among cases compared to controls. Furthermore, there were statistically significant differences at 0.05 in the ALP level between cases (mean = 450.3) and controls (mean = 99.2), P-value 0.005, which means that the ALP level was significantly higher among cases compared to controls. Also, there were statistically significant differences at 0.05 in Ca level between cases (mean = 8.9) and controls (mean = 9.7), P-value 0.005, which means that Ca level was significantly lower among cases compared to controls. In addition, there were statistically significant differences at 0.05 in phosphorus level between cases (mean = 4.9) and controls (mean = 3.9), P-value 0.001, which means that phosphorus was significantly higher among cases compared to controls.
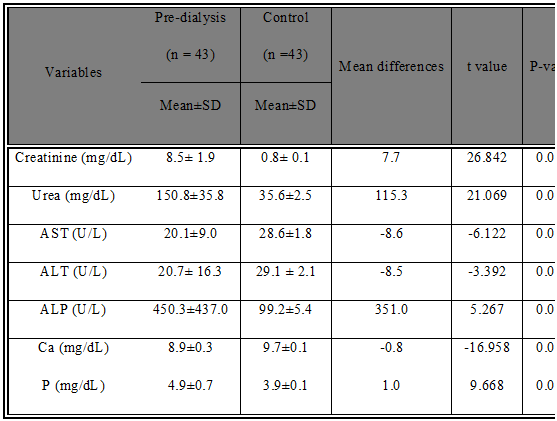
AST: Aspartate transaminase; ALT: Alanine transaminase; ALP: Alkaline phosphatase; Ca: Calcium; P: Phosphorus. The significance of difference was checked by t-test (compare all case and control), significant at P ≤ 0.05.
Table 6 shows that there were statistically significant differences at 0.05 in creatinine level between (cases) post-dialysis (mean = 3.9) and control (mean = 0.8), P-value 0.001, which means that creatinine level was significantly higher among post-dialysis compared to control. Also, there were statistically significant differences at 0.05 in urea between cases (mean = 67.1) and controls (mean = 35.6), P-value 0.001, which means that urea was significantly higher among cases compared to controls. In addition, there were statistically significant differences at 0.05 in AST between cases (mean = 24.8) and controls (mean = 28.6), P-value 0.019, which means that AST was significantly lower among cases compared to controls. Furthermore, there were statistically significant differences at 0.05 in the ALP level between cases (mean = 484.4) and controls (mean = 99.2), P-value 0.001, which means that the ALP level was significantly higher among cases compared to controls. Also, there were statistically significant differences at 0.05 in Ca level between cases (mean = 9.2) and controls (mean = 9.7), P-value 0.001, which means that Ca level was significantly lower among cases compared to controls. In addition, there were statistically significant differences at 0.05 in phosphorus level between cases (mean = 4.0) and controls (mean = 3.9), P-value 0.004, which means that phosphorus was significantly higher among cases compared to controls. On the other hand, there were statistically insignificant differences between the two groups in levels of ALT (P= 0.161)
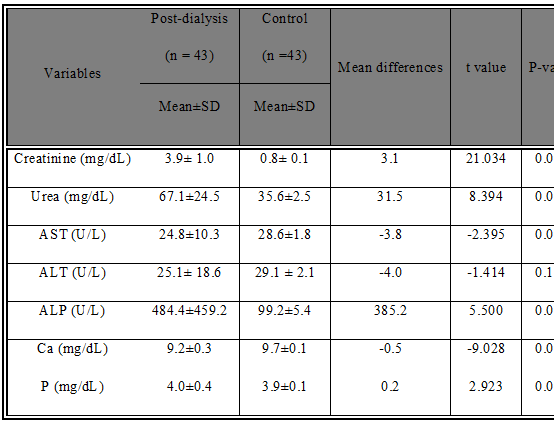
AST: Aspartate transaminase; ALT: Alanine transaminase; ALP: Alkaline phosphatase; Ca: Calcium; P: Phosphorus. The significance of difference was checked by t-test (compare all case and control), significant at P ≤ 0.05.
Table 7 shows that there were statistically significant differences at 0.05 in creatinine level between pre-dialysis (mean = 8.5) and post-dialysis (mean = 3.9), P-value 0.001, which means that creatinine level was significantly higher among pre-dialysis compared to post-dialysis. Also, there were statistically significant differences at 0.05 in urea between pre-dialysis (mean = 150.8) and post-dialysis (mean = 67.1), P-value 0.001, which means that urea was significantly higher among pre-dialysis compared to post-dialysis. In addition, there were statistically significant differences at 0.05 in AST between pre-dialysis (mean = 20.1) and post-dialysis (mean = 24.8), P-value 0.001, which means that AST was significantly lower among pre-dialysis compared to post-dialysis. The results also show that there were statistically significant differences at 0.05 in the ALT level between pre-dialysis (mean = 20.7) and post-dialysis (mean = 25.1), P-value 0.001, which means that ALT level was significantly lower among pre-dialysis compared to post-dialysis. Furthermore, there were statistically significant differences at 0.05 in the ALP level between pre-dialysis (mean = 450.3) and post-dialysis (mean = 484.4), P-value 0.003, which means that ALP level was significantly lower among pre-dialysis compared to post-dialysis. Also, there were statistically significant differences at 0.05 in Ca level between pre-dialysis (mean = 8.9) and post-dialysis (mean = 9.2), P-value 0.005, which means that Ca level was significantly lower among pre-dialysis compared to post-dialysis. In addition, there were statistically significant differences at 0.05 in phosphorus level between pre-dialysis (mean = 4.9) and post-dialysis (mean = 4.0), P-value 0.001, which means that phosphorus was significantly higher among pre-dialysis compared to post-dialysis.

Evaluate the changes in renal function tests
One of the progressive diseases causing irreversible fall in the glomerular filtration rate further resulting in the elevation in values of serum creatinine and blood urea nitrogen values is the chronic renal failure (Tomas et al., 2008). Hypertension, diabetes mellitus, autoimmune causes form the most common cause of chronic renal failure. Since it is irreversible in nature and progresses to further severe form with time, with a decline of glomerular filtration rate to 5 to 10 percent with high levels of uremia (Meenakshi et al., 2016).
Most patients undergoing dialysis were between the ages of 53-63years and 64-74 years, which could be due to advancing age and progressive physiological glomerulosclerosis that leads to a decrease in renal weight. Serum creatinine and urea were estimated in CKD patients pre and post dialysis as these are important renal markers in the diagnosis, follow-up and recovery of CKD patients undergoing Hemodialysis.
Creatinine is a breakdown product of creatine phosphate in muscle and is usually produced at a fairly constant rate by the body depending on muscle mass (Zuo et al., 2008). Creatinine is commonly used as a measure of kidney function. A rise in serum creatinine levels in CRF patients is attributed to the decrease in the number of functioning nephrons, which would reduce the GFR, which causes a major decrease in renal excretion of water and solutes and gathering of toxic products. It is neither secreted nor reabsorbed so its values are relatively more accurate. Thus, the rise in serum creatinine is used in clinical practice as a marker of reduced GFR. Hemodialysis decreases the creatinine levels by its removal from the blood by dialyzing the patient’s blood against fluid containing minerals similar to the natural concentration of blood (Ahmad et al., 2008).
Our study showed that the pre-dialysis group showed that increase and there were statistically significant differences in urea and creatinine level (P= 0.001) when compared to healthy individuals. Also, the post-dialysis group showed increased serum levels of urea and creatinine in post-dialysis groups when compared with control and were statistically significant. Serum urea and creatinine levels in the post-dialysis group are lower than the post-dialysis group and are statistically significant (p-value < 0.05). Our results agree with the previous study which found that the pre-dialysis group showed an increase in the levels of the urea and creatinine which were statistically significant (p-value < 0.05). Our results of Creatinine in the study group were consistent with the clinical studies done by (Shankalia, & Tanna, 2013; Amin et al., 2014; Khaled et al., 2015 and Chielle et al., 2015). These results confirm that hemodialysis is an efficient method to remove undesired substances from CKD patients, even when values are above the desired reference levels. This is due to the fall in the GFR in CRF patients. As the GFR falls, plasma levels of creatinine and urea rise as they are eliminated by glomerular filtration and tubular secretion. Blood urea and serum creatinine levels in the post-dialysis group showed a significant fall in comparison with the pre-dialysis group ((Meenakshi et al., 2016). Similarly, the previous study noticed that the urea and creatinine high significant (P<0.01) increased in patients when compared with the control group, this is due to a decline in the number of nephrons (Hassen et al., 2018).
Similarly, serum creatinine values in the pre-dialysis group were significantly higher in comparison with the post-dialysis group (p-value < 0.05). Also, the blood urea values in the pre-dialysis group were significantly higher (p-value < 0.05). The blood urea level in the post-dialysis group was significantly lower (Meenakshi, 2016).
Pre-HD had mean urea values 150.8±35.8, which is higher than control and post-HD mean values were 67.1±24.5. The results showed that dialysis leads to a significant fall in mean serum urea levels (p < 0.001). Urea is the major nitrogenous end product of protein and amino acid catabolism, produced by the liver and distributed throughout the intracellular and extracellular fluid. In kidneys, urea is filtered out of the blood by glomeruli and is partially being reabsorbed with water (Corbett, 2008). In chronic renal failure, there is a steady and continued decrease in renal clearance or glomerular filtration rate (GFR), which leads to the gathering of urea and other toxic chemicals in the blood. The increase of serum urea is proportional to the progression of the disease, but it is highly influenced by the catabolic state or excessive protein ingestion (Montini et al., 2003).
Our findings of urea were supported by (MohammedJumaah, 2013; Amin et al., 2014; Mahomoodally & Nugessur, 2014). Amin et al. studied 70 patients and found a clear reduction in urea levels. Mahomoodally & Nugessur showed that there was a significant decrease in serum urea. He explained that during hemodialysis, urea, being small molecule flow through membranes into the sterile solution and is removed due to the counter-current flow of the blood and dialysate (Blake, Daugirdas, 2008). Chielle et al with findings supporting our study explained that during hemodialysis, excess urea is just partially removed in order to prevent accumulation, it is very important to balance the number of consumed proteins, avoiding excessive
Production of urea (Chielle et al 2015). The decrease in the level of urea, creatinine in post-dialysis patients compared with pre-dialysis patients with CRF is due to the hemodialysis process which removes toxins from the blood by a closed-loop process where the blood of the patient and is continuously being withdrawn, dialyzed, and returned to the patient. These findings also supported by other studies (Mustafa et al., 2010).
Evaluate the changes in some minerals levels tests
The mean and standard deviation (SD) of serum calcium levels pre-HD is 8.9±0.3 and post-HD is 9.2±0.3. The values are highly significant with p-value = 0.001. Calcium levels in the blood of both males and females of CKD of post HD patients are increased slightly than the pre-HD patients. Calcium is one of the key elements to consider in patients on dialysis due to its relationship with cardiovascular risk. Also decreased Ca level found when the kidneys fail, decreasing its ability to reabsorb calcium and leading to loss of calcium in the urine (Traynor et al., 2010). Our findings are similar to previous study serum which showed that serum calcium levels in the post-dialysis group were higher in the pre-dialysis group (p-value < 0.05). Serum calcium levels in the pre-dialysis group were lower (Meenakshi, 2016). Also, the serum Ca++ was significantly decreased in pre HD compared with the controls but its concentration was increased in post HD compared with the pre HD (Sarhat & Murtadha, 2016). Our study was in accordance with Khaled et al [2015] (Khaled et al., 2015) and Safraneka et al [2015] (Safraneka et al., 2015) who found a significant increase in serum calcium levels post-dialysis.
Bech et al., found a decrease in serum calcium levels post-dialysis (Bech et al., 2013). This study not in accordance with our study. Also, we observed a statistically significant increase in serum phosphorus levels in cases as compared to controls. The previous study reported a significant increase in phosphorus levels (Hassen et al., 2018). Also, the previous study showed that serum phosphorus levels in the pre-dialysis group were statistically significantly higher in comparison with the post-dialysis group (p-value < 0.05) (Meenakshi, 2016). Also, these results in the present study are in accordance with the previous study which observed that the levels of P were significantly increased in CRF in pre HD compared with controls, and they were decreased after HD (Sarhat & Murtadha, 2016). Kidney failure is the medical conditions that cause low blood calcium levels or increased phosphate levels can lead to secondary hyperparathyroidism (Bringhurst & Demay, 2011).
Evaluate the changes in some biochemical parameters tests
Our study showed that the pre-dialysis group showed that decrease and there were statistically significant differences in ALT and AST levels (P= 0.001) when compared to healthy individuals. Also, the post-dialysis group showed decreased serum levels of ALT and AST when compared with control and were statistically significant. Serum ALT and AST levels in the post-dialysis group are lower than the pre-dialysis group and are statistically significant (p-value < 0.05).
This result agreed with the previous study which found that levels of liver enzyme, alanine transaminase (ALT) activity between cases and control participated in this study showed that decreasing levels of Alanine transaminase in patients with renal failure under hemodialysis when compared with control. (10 ± 4versus 24±7, p-value = 0.00). As well as aspartate transaminase (AST) which showed a decrease in levels of Aspartate transaminase in patients with renal failure under hemodialysis when compared with control. (15 ± 5 versus 34±7, p-value =0.00). Also, the levels of (AST&ALT) concentration were significantly decreased in pre-dialysis when compared to post dialysis, ALT (8±4 versus 17±3; p-value ꞊0.00) AST (13±4 versus 22±4; p-value ꞊0.00) (Babekr, 2015). Our study is also consistent with the previous study which showed that serum levels of the enzymes aspartate transaminase and alanine transaminase in patients with renal failure on hemodialysis; were decreased. It was hypothesized that this reduction could be caused by factors such as the withdrawal of aminotransferases during the hemodialysis session; the high lactate serum levels, which, during biochemical dosages, would rapidly consume Nicotinamide Adenine Dinucleotide Phosphate (NADPH) and result in low levels of aminotransferases; the presence of uremic factors that would inhibit the activity of these enzymes; and, finally, the deficiency of pyridoxine, a cofactor for the synthesis of the aminotransferases (Sette & de Almeida Lopes 2014). This result also agreed with previous study which found that both AST&ALT were significantly low (p-value <0.05) in both sexes when compared with their counterparts in the control group the decrease in levels of aminotransferases in patients with renal failure who have not undergone dialysis therapy has observed in this study suggests that renal impairment has an impact on the liver enzymes (Shittu et al., 2014). Also, this result agreed with other study carried by (Sombolos et al., 2012) evaluated 53 patients on hemodialysis and divided them into three groups: hemodialysis, isolated ultrafiltration, and euvolemic hemodialysis (without the removal of fluids) and verified the effects of hemodilution in the serum levels of the aminotransferases. In the patients who underwent euvolemichemodialysis, there were no differences between the ALT and AST levels prior to and after the procedure. However, when isolated ultrafiltration or hemodialysis was performed, there was an increase in the aminotransferase levels when compared with the values prior to and after the procedure, the authors concluded that the rise in the aminotransferase serum levels after hemodialysis should primarily occur due to the hemoconcentration induced by the ultrafiltration. Also, the result (Liberato et al., 2012) showed the aminotransferase levels were lower in the samples collected before hemodialysis compared with the samples collected after the hemodialysis.
In our results showed that a significant increase in the mean of the level of serum alkaline phosphatase (ALP) in patients with renal failure groups compared to the control group. As well as a significant increase in the mean of the level of serum alkaline phosphatase (ALP) in patients after hemodialysis compared to the control group. Also, the level of (ALP) concentration was significantly decreased in pre-dialysis when compared to post-dialysis. Our study agreed with the previous study which found that ALP was significantly higher in both groups of CKD patients when compared to healthy controls (Latiwesh et al., 2018).
Evaluate the changes in hematological parameters tests
In the previous study, subjects were considered as anemic on the basis of WHO criteria of Hb less than 13 g/100 ml for males and less than 12 g/100 ml for females (Abate et al., 2013). The present study was conducted on 43 CKD patients and 43 healthy controls and found that significantly mean RBCs count, hemoglobin concentration and hematocrit levels were significantly lower in both groups of CKD patients than normal healthy controls (p< 0.05). This study agrees with the previous study which showed that significantly lower RBC count, hemoglobin concentration, and hematocrit levels in CKD patients when compared to healthy subjects (Latiweshob et al., 2017). Also, these results were consistent with Almahdi and colleagues (2016) who found a significant decrease in hemoglobin levels in Libyan CKD patients compared to the control group (Almahdi et al., 2016). Another recent work was consistent with our results and found that hemoglobin concentration and RBCs count were significantly different from that of the control at the severe CKD patients in Nigeria (Shittu and colleagues, 2013). Similarly, our results were in agreement with many other studies (Afshar et al., 2010; Suega et al., 2005).
The primary cause of decreased RBCs count in chronic renal failure is impaired erythropoietin production and other factors that suppress marrow erythropoiesis and shortened red cell survival. Erythropoietin is the hormone which is the major humoral regulator of red cell production and helps to maintain the viability of RBC by retarding the cleavage of DNA that occurs normally in CFU-Es. In the absence of EPO, DNA cleavage is rapid and leads to cell death. RBC survival is decreased in uremic patients in proportion to the blood urea nitrogen concentration and, it improves significantly after intensive hemodialysis. Uremic plasma increases the expression of phosphatidylserine on the outer cell surface in red blood cells. This enhances the recognition of damaged red blood cells by macrophage, leading to their subsequent destruction and decreased survival (Means and Glader, 2009). The hemoglobin concentration and hematocrit generally provide an accurate reflection of the extent to which the circulating red cell mass is reduced. In chronic renal disease because of impaired erythropoietin secretion, increased destruction of red blood cells leads to a fall in red blood cell count, which reduces the hemoglobin concentration and hematocrit ( Dessypris & Sawyer, 2004).
Our work indicated that the mean of each RBCs count, Hb, Hct, and RDW levels show a statistically significant increase in renal failure patients’ post-HD when compared to pre-HD levels. Our reports are consistent with the previous study which revealed that shows differences between the mean of RBCs count, Hb, Hct, RDW, RBCs indices in renal failure patients before and after HD (Alghythan & Alsaeed, 2012). The previous study indicated that the mean of each RBCs count, Hb, Hct, MCH, MCHC and RDW levels show a statistically significant increase in renal failure patients’ post-HD when compared to pre-HD levels. The increase of each RBCs count, Hb, Hct levels post-HD were explained by the fact that before HD, patients are usually hypervolemic and the values of each RBCs count, Hb, Hct levels are also lower (Alghythan & Alsaeed, 2012).
The results of our study noticed that there was a significant change of WBC count in pre-dialyzed and post-dialyzed patients compared to control but post-hemodialysis was different when compared to pre-dialysis but not reach to significant. This finding is the disagreement that of other studies (George et al., 2015). A study of Alghythan & Alsaeed, 2012 (Alghythan & Alsaeed, 2012), revealed an insignificant difference in WBC count between hemodialyzed CKD patients and the control group. Also our study inconsistent with the previous study which showed that a non-significant change of WBC count in dialyzed and hemodialyzed patients compared to control (Latiweshob et al., 2017). An inversely previous study also indicated that there were statistically insignificant differences between the mean number of leucocytes and differential counts in renal failure patient’s pre-HD when compared to the counts of the control group (Alghythan & Alsaeed, 2012). Also, this finding is in contrast with Shittu and colleagues (2013) who found that WBC count was significantly increased with the progression of the disease (Shittu et al., 2013).
The possible mechanism by which chronic renal disease leads to a slight decrease in total leukocytic count may be explained by complement activation in vivo due to exposure of blood to artificial membranes in dialyzer in patients undergoing dialysis. The complement is typically C3a or C5a, produced by the classical complement activation pathway. Complement activation stimulates neutrophil aggregation and adherence to the endothelial surface which results in decreased leukocytic count. In patients undergoing hemodialysis, the incidence of this effect may be as high as 20% (Walts et al., 2004).
An inversely previous study observed that the mean of leucocytes counts showed a statistically significant increase in renal failure patients’ after HD when compared to before HD procedures. The increase of leukocyte count after-HD was explained by the fact that at the beginning of HD, patients are usually hypervolemic and the values of the leucocytes counts are lower (Alghythan & Alsaeed, 2012).
In the present work showed that platelets counts were significantly higher in pre-dialyzed CKD patients compared to hemodialyzed CKD patients (p< 0.05) and significant difference in platelet count was seen between pre-dialyzed or hemodialyzed CKD patients and normal healthy controls (p=0.001; p= 0.001, respectively).
Inversely previous study showed that there was a non-significant difference in PLT count of pre-dialyzed CKD patients or hemodialyzed-CKD patients when compared with control group (p=0.052; p= 0.09, respectively) but our work consistent with this study that platelets counts were significantly higher in pre-dialyzed CKD patients compared to hemodialyzed CKD patients (p<0.05) (Latiweshob et al., 2017). Also Inversely the previous study revealed that platelets count in pre-dialysis and post- dialysis no change (p= 0.319) (Bat et al., 2016).
A previous study compatible with our study showed that there was a significant difference in PLT count of pre-dialyzed CKD patients when compared with فاث control group (p= 0.0001) (Dorgalaleh et al., 2013). Similar results with our study also reported that there was a statistically significant decrease in the mean platelet counts, though still within the normal range, failure patients pre- and post-HD when compared to the results of the control group. The mean platelet counts showed a significant decrease in patients’ after-HD when compared to pre-HD procedures (Alghythan & Alsaeed, 2012).
Erythropoietin potentiates the effect of megakaryocyte colony-stimulating factors, acetylhydrolase (PAF-AH) and paraoxonase (PON1). In chronic renal disease, impaired erythropoietin secretion leads to a decrease in platelet count (Papavasiliou et al., 2006). The detection of receptors for erythropoietin in megakaryocytes is understandable because erythropoietin levels can affect platelet level and because of extensive homology between erythropoietin and thrombopoietin, erythropoietin act as the major humoral regulator of platelet mass (Latiweshob et al., 2017). Also, the previous study suggested that thrombocytopenic episodes occurring with hemodialysis were associated with complement activation, specifically C3a, in addition to activation of platelets themselves (Kiaii et al., 2011).
The MCH level showed a statistically significant decrease in pre-HD patients when compared to that of the control group (P<0.05). However, the MCV and RDW levels did not show any statistically significant change in pre-HD patients compared to the control group (p> 0.05). our findings close for the previous study which showed that The MCH and MCHC levels showed a statistically significant decrease in pre-HD patients when compared to that of the control group (P<0.05). However, the MCV and RDW levels did not show any statistically significant change in pre-HD patients compared to the control group (p> 0.05) (Alghythan & Alsaeed, 2012).
It was recommended that in patients with chronic renal failure, to prevent the risk of bleeding, the platelet count should be checked periodically.
From the present study, it can be concluded that patients with chronic kidney disease show abnormal hematological parameters, precisely reduced levels of RBC count, hemoglobin, hematocrit, and platelet count, in addition, pre-dialysis patients are more anemic and thrombocytopenic than post-dialysis patients. These findings expose CKD patients to a higher risk of anemia-related complications and bleeding disorders, which may have a role in increasing the rate of patient mortality and morbidity. Moreover, hypertension and diabetes mellitus is the most common cause of CKD, and this is may indicate of lack of blood pressure and diabetic control in these patients. (AST&ALT) activities vary in concentration before and after dialysis and make the post-dialysis patients are higher than pre-dialysis.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
