AUCTORES
Globalize your Research

Review Article
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology Manchester, M8 5RB. United Kingdom.
Citation: Anthony K-G Venyo. (2020) Anaplastic Lymphoma Kinase (ALK) Translocation Re-arrangement Renal Cell Carcinomas: A Review and Update of the Literature. International Journal of Clinical Case Reports and Reviews. 3(5); DOI: 10.31579/2690-4861/055
Copyright: © 2020 Anthony Kodzo-Grey Venyo, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 September 2020 | Accepted: 25 September 2020 | Published: 29 September 2020
Keywords: anaplastic lymphoma kinase-associated renal cell carcinoma; histopathology; electron microscopy; cytogenetics, nephrectomy; alk-inhibitor. ALK; PAX8; INI1; AE1/AE3; CAM5.2; CK7; EMA; LMWCK; P53; Vimentin; CD10; AMACR; TFE3.
Less than 50 cases of anaplastic lymphoma kinase (ALK) re-arrangement-associated renal cell carcinoma (ALK-RCC) been reported in the literature. ALK-RCC does affect children who have sickle cell trait and also adults with no evidence of sickle cell trait or sickle cell disease. ALK-RCC may be diagnosed incidentally or in individuals who have typical symptoms that simulate those or more common renal tumours.. Diagnosis of ALK-RCC does depend upon histopathology examination, immunohistochemistry studies as well as electron microscopy studies of nephrectomy / biopsy specimens of the kidney lesion that that show: typical pathology examination features of ALK-RCC as described within the text. Immunohistochemistry studies in ALK-RCC tend to show positive staining for: ALK, PAX8, INI1 (Intact), AE1/AE3, CAM5.2, CK7, EMA, LMWCK, P53, +Vimentin, CD10 (this tends to be variable), AMACR (this tends to be variable), and TFE3 (within the majority of the tumour cells). Majority of ALK-RCCs have been localized tumours at the time of initial diagnosis, but some cases of locally advanced tumours or tumours associated with metastases have been reported. There is no consensus opinion on the treatment of ALK-RCC but nephrectomy has been undertaken in most cases with good short term and medium term; nevertheless metastases and death have been reported. Response to utilization of to ALK inhibitor alectinib, as well as ALK Translocation Renal Cell Carcinoma does respond to Crizotinib. Improvements in the outcome of ALK-RCC could possibly be achieved through routine screening of sickle cell trait individuals, routine pre-operative per-cutaneous radiology imaging guided biopsies of all renal lesions, small localized tumours could be treated by (a) partial nephrectomy, or (b) radical nephrectomy, (c) cryotherapy, (d) radiofrequency ablation, (e ) irreversible electroporation plus / minus adjuvant therapy (radiotherapy, chemotherapy or ALK inhibitor plus or minus immunotherapy.
Anaplastic lymphoma kinase (ALK) is stated to be a membrane-associated receptor kinase which belongs to insulin superfamily [1]. It has been iterated that ALK re-arrangement is oncogenic which does activate cellular signalling pathways by dimerization through the specific structures of fusion partners [2]. It has been stated that genetic alterations within ALK has been found in various tumours [3]. The World Health Organization (WHO) 2016 edition assigned anaplastic lymphoma kinase (ALK) re-arrangement-associated renal cell carcinoma (ALK-RCC) as an emerging kidney tumour entity [3]. It has been iterated that the identification of ALK-RCC is important or pertinent in that ALK inhibitors have been demonstrated to be effective with regard to treatment of ALK re-arrangement renal cell carcinoma. [3]. It had been iterated that up to March 2020, 28 cases of ALK-RCC had been reported and six partner genes had been confirmed within the tumour [3], [4] [5] [6] [7]. It has been iterated that the recognition of ALK alterations within neoplasms is important in view of the potential benefit of ALK inhibitors. Despite this knowledge, it had been noted that screening for ALK re-arrangement within RCC has not been routinely undertaken in view of cost-effectiveness problems. [3] [8]. It has been indicated that previous studies had reported that ALK-RCC is encountered in less than 1% of renal cell carcinomas (RCCs) and in 3.8% of paediatric and young adults who have renal cell carcinomas (RCCs) [3] [9] [10]. It has been stated that attempts had been undertaken to ascertain the the characteristics of ALK-RCC; nevertheless, in view of its rarity, as well as the various histological features of the tumour depending upon the fusion partners does make it difficult. [3]. Many partner genes including VCL, TPM3, EML4, HOOK1, STRN, and RAD51AP2 have been reported in association with ALK-RCC in association with their linkages with a variety of clinicopathological findings. [3] It has been documented that out of the aforementioned genes, VCL-ALK Renal cell carcinoma had been described in children who have sickle cell trait as well as that TPM3 had been primarily reported as a partner in ALK-RCC [3]. It has also been stated that the coiled-coil structure of TPM3 does induce dimerization of the fusion protein protein and does promote ALK activation. Considering that less than 30 cases of ALK Translocation-associated renal cell carcinomas have been reported so far, it would not be surprising if majority of clinicians globally are not aware of the diagnostic features, clinical behaviour, management as well as outcome of the malignancy because most people globally would certainly have not encountered the tumour before. The ensuing review and update of the literature on ALK Translocation-associated Renal Cell Carcinoma is divided into two parts: (A) Overview, and (B) Miscellaneous narrations and discussions from some case reports, case series, and studies related to ALK Translocation-Associated Renal Cell Carcinoma.
Aim
To review and update the literature on ALK Translocation-Associated Renal Cell Carcinoma.
Method
Internet data bases were searched including: Google, Google Scholar, Yahoo, and PUBMED. The search words that were used included: ALK Translocation-Associated Renal Cell Carcinoma, ALK Renal Cell Carcinoma, and ALK RCC. Thirty four references were identified which were used to write the review and update of the literature on ALK Translocation-Associated Renal Cell carcinoma that is divided into two parts: (A) Overview and (B) Miscellaneous narrations and discussions from some case reports, case series, and studies related to ALK Translocation-Associated Renal Cell Carcinoma.
Result / Review and Update of the Literature on ALK Translocation-Associated Renal Cell Carcinoma.
(A) Overview
Definition / General Comments
It has been iterated that ALK Translocation Renal Cell Carcinoma is a terminology that is utilized for renal cell carcinoma (RCC) that is associated with anaplastic lymphoma kinase (ALK) gene re-arrangement (chromosome 2p23). [11]
It has been documented that ALK Translocation Renal Cell Carcinoma does tend to affect children who have sickle cell trait as well as adults who do not have sickle cell trait. [11]
It has been stated that ALK Translocation Renal Cell Carcinoma that affects children does simulate renal medullary carcinoma in that it tends to be medulla centric and it tends to be associated with diffuse infiltrating growth that contains lymphoplasmacytic infiltrate as well as large polygonal dis-cohesive or spindle cells and cytoplasmic vacuoles as well as vesicular nuclei [11].
It has been iterated that ALK Translocation Renal Cell Carcinoma that affects adults does tend to exhibit heterogeneous solid architecture as well as microscopic examination of the specimen does demonstrate mucinous cribriform, signet-ring, as well as solid rhabdoid patterns, and high-grade eosinophilic cells and intra-cytoplasmic lumens [11] [12] [13].
Essential Features
It has been documented that microscopy pathology examination features of ALK Translocation Renal Cell Carcinoma does demonstrate an architecturally heterogeneous eosinophilic tumour that contains polygonal, rhabdoid, signet ring and spindled cells, which produce mucin and does also contain cytoplasmic vacuoles [11].
It has also been iterated that immunohistochemistry staining studies of ALK Translocation Renal Cell Carcinoma does demonstrate Diffusely positive ALK protein expression (positive staining for ALK protein) [11].
It has also been stated that in cases of ALK Translocation Renal Cell Carcinoma, ALK gene re-arrangements tend to be demonstrated by utilization of FISH, RT-PCR, or RNA sequencing [11].
Terminology
It has been iterated that the first documented case of VCL-ALK fusion renal cell carcinoma was described in 2010 [11] [14].
It has been stated that the three terminologies that are utilized for ALK Translocation Renal Cell Carcinoma include: [11]
ALK re-arrangement associated RCC.
ALK translocation RCC
ALK-RCC
It has been documented that ALK Translocation Renal Cell Carcinoma is a provisional tumour entity that has been incorporated into the 2016 World Health Organization (WHO) Classification of Tumours [11].
Epidemiology
It has been iterated that ALK Translocation Renal Cell Carcinoma is an uncommon tumour and less than 25 cases of the tumour have been reported [11].
It has been documented that cases of ALK Translocation Renal Cell Carcinoma have tended to have a bimodal distribution with regards to age as follows:
ALK Translocation Renal Cell Carcinomas do affect children who have Sickle Cell Trait, and the disease tends to affect children of African descent whose ages have tended to range between 6 years and 19 years.
ALK Translocation Renal Cell Carcinomas do also affect adults who do not have Sickle Cell Trait and their ages have tended to range between 33 years and 61 years.
It has been iterated that with regard to the incidence of ALK Translocation Renal Cell Carcinoma, the incidence in children has ranged between 3.5% and 3.8% of all renal carcinomas and the incidence in adults, has ranged between 0.4% to 0.5% of all renal cell cancers in adults [9] [10] [11] [13] [15].
Sites
It has been documented that with regard to the sites of the kidney that tend to be affected by ALK Transformation Renal Cell Carcinoma, the ensuing summations can be made: [11]
ALK Translocation Renal Cell Carcinomas tend be encountered as solitary kidney tumours.
ALK Translocation Renal Cell Carcinomas tend to often affect the medulla of the kidney, the renal pelvis, as well as the middle of the kidney.
Pathophysiology of ALK Translocation Renal Cell Carcinoma
The ensuing remarks have been made regarding the pathophysiology of ALK Translocation Renal Cell Carcinoma: [11]
ALK does belong to the insulin receptor tyrosine kinase superfamily and it tends to be normally expressed at a low-level within the central nervous system. [11]
ALK translocation does represent an oncogenic driver mutation which perhaps does occur during the early stage of carcinogenesis [13].
Aetiology
With regard to the aetiology of ALK Translocation Renal Cell Carcinoma in children, the Sickle trait has been noted to be a factor in a sub-set of the patients [8] [11].
Clinical features
It has been documented that pertinent clinical features of ALK Translocation Renal Cell Carcinoma include haematuria, flank pain, abdominal pain, or peri-umbilical pain [10] [11] [12].
It has been documented that 33 percent of cases of ALK Translocation Renal Cell Carcinoma have been diagnosed incidentally [11].
It has been stated that ALK Translocation Renal Cell Carcinomas have tended to be pT1a or pT1b tumours. [11].
Laboratory Investigations
Urine
Urinalysis, urine microscopy and culture are routine tests that tend to be undertaken in the initial assessment and follow-up of all individuals who have ALK Translocation-Associated RCC and most often the results tend to be normal but there could be red blood cells in the urine specimens of those individuals who have been having haematuria. In the event of evidence of urinary tract infection, it would be treated with an appropriate antibiotics based upon the antibiotic sensitivity pattern of the cultured organism and the allergic status of the individual.
Haematology blood tests
Full blood count, erythrocyte sedimentation rate, and coagulation screen are routine tests that tend to be undertaken in the initial and follow-up assessments of individuals who have ALK Translocation-Associated Renal Cell Carcinoma and most often the results would be normal but in cases of recurrent haematuria there may be evidence of anaemia. If there is any abnormality, it would be investigated and treated to improve upon the general condition of the individual.
Usually individuals who have sickle cell trait tend to have haemoglobin electrophoresis prior to their presentation and the results would be available.
Biochemistry blood tests
Serum urea, glomerular filtration rate, electrolytes, blood glucose and liver function tests are routine tests that tend to be undertaken in the initial and follow-up assessments of individuals who have ALK Translocation-Associated Renal Cell Carcinoma and most often the results tend to be normal but if there is any abnormality it would be investigated and treated accordingly to improve the general condition of the individual.
Radiology imaging features
Ultrasound scan
It has been stated that ultrasound scan of abdomen, pelvis, and renal tract does show a hypo-echoic medulla centric mass. [11]
Ultrasound scan is a common radiology imaging that tends to be undertaken in the initial assessments of individuals who have ALK Translocation-Associated Renal Cell Carcinoma and ultrasound scan of renal tract, abdomen, and pelvis can be undertaken in the follow-up assessments of individuals who have undergone nephrectomy or partial nephrectomy for the malignancy in addition to chest x-ray to establish presence or absence of metastasis but this has been superseded by utilization of CT Scan/MRI scan of thorax abdomen and pelvis.
Ultrasound scan-guided biopsy of the kidney lesion can be done pre-operatively for pathology examination to establish the diagnosis following which various treatment options could be discussed including: Partial nephrectomy, radical nephrectomy, cryotherapy, radiofrequency ablation, and irreversible electroporation plus adjuvant therapy including chemotherapy, radiotherapy, ALK inhibitor, and immunotherapy.
Computed tomography scan
It has been documented that simple computed tomography scan of abdomen and pelvis does show an iso-dense kidney mass [11].
Computed Tomography Scan of abdomen and pelvis does show a slightly enhanced or heterogeneously enhancing mass [12].
CT scan is a common radiology imaging that tends to be undertaken in the initial assessments of individuals who have ALK Translocation-Associated Renal Cell Carcinoma and CT scan of thorax, renal tract, abdomen, and pelvis can be undertaken in the follow-up assessments of individuals who have undergone nephrectomy or partial nephrectomy for the malignancy in addition to chest x-ray to establish presence or absence of metastasis.
CT scan-guided biopsy of the kidney lesion can be done pre-operatively for pathology examination to establish the diagnosis following which various treatment options could be discussed including: Partial nephrectomy, radical nephrectomy, cryotherapy, radiofrequency ablation, and irreversible electroporation plus adjuvant therapy including chemotherapy, radiotherapy, ALK inhibitor, and immunotherapy.
Magnetic Resonance Imaging Scan
MRI scan is a common radiology imaging that tends to be undertaken in the initial assessments of individuals who have ALK Translocation-Associated Renal Cell Carcinoma and MRI scan of thorax, renal tract, abdomen, and pelvis can be undertaken in the follow-up assessments of individuals who have undergone nephrectomy or partial nephrectomy for the malignancy in addition to chest x-ray to establish presence or absence of metastasis.
MRI scan-guided biopsy of the kidney lesion can be done pre-operatively for pathology examination to establish the diagnosis following which various treatment options could be discussed including: Partial nephrectomy, radical nephrectomy, cryotherapy, radiofrequency ablation, and irreversible electroporation plus adjuvant therapy including chemotherapy, radiotherapy, ALK inhibitor, and immunotherapy.
Positron Emission Tomography – Computed Tomography Scan
PET-CT scan tends to be undertaken in the follow-up assessments of individuals who have undergone treatment for ALK Translocation-Associated Renal Cell Carcinoma to establish if they have developed metastasis as well as the site of the metastasis.
Isotope Bone Scan
Isotope bone scan tends to be undertaken in the follow-up of individuals who have had treatment for ALK Translocation-Associated Renal Cell Carcinoma to establish if they have developed bone metastasis.
Prognostic factors
It has been iterated that with regard to the prognosis of Children who had VCL-ALK, so far following treatment, no case of local recurrence or distant metastasis has been reported [11].
It has been stated that with regard to adult non-VCL-ALK Renal Cell Carcinomas, 33 percent of the tumours tend to be associated with adverse prognosis. [10] [11] [13]
It has been iterated that in view of the few reported cases and the short period of follow-up reported in association with the reported cases, the accurate assessment of the prognosis and the associated risk factors cannot be ascertained at the moment [11].
Treatment
Some of the treatment strategies that have been utilized for ALK Translocation Renal Cell Carcinoma have been summated as follows: [11]
Primary Localized Tumour – Cases of early stage localized ALK Translocation Renal cell carcinoma have been treated by means of nephrectomy or nephroureterectomy.
Metastatic ALK Translocation Renal Cell Carcinomas – It has been documented that ALK-RCC does respond to ALK inhibitor alectinib [11] [16].
It has also been stated that ALK Translocation Renal Cell Carcinoma does respond to Crizotinib like the response of re-arrangement lung cancer for this treatment [17].
Macroscopic examination features
The macroscopy pathology examination features of ALK-Translocation Renal Cell Carcinoma have been summated as follows: [11]
Paediatric patients who have ALK Translocation Renal Cell Carcinoma – It has been iterated that macroscopic examination of the kidney tumour of a paediatric individuals who has ALK Translocation Renal Cell Carcinoma does tend to demonstrate a solid tumour mass that is irregular with regard to shape as well as associated with infiltrative borders [12] [18].
Adult Individuals who have ALK Translocation Renal Cell Carcinoma – It has been iterated that macroscopic pathology examination of the kidney tumours of an adult individual who has ALK Translocation Renal Cell Carcinoma does tend to show a well-demarcated tumour that is localized within the middle of the kidney and which tends to be tan to brown, or white to grey with regard to colour in which cystic change or haemorrhage could found; however, there tends to be absence of a pseudo-capsule encompassing the tumour. [11]
With regard to the size of the tumour, it has been stated that gross examination of ALK Translocation Renal Cell Carcinoma does tend to reveal a kidney tumour that measures between 3 cm and 7 cm. [11]
Microscopy histopathology examination features.
The microscopy histopathology examination features of ALK Translocation Renal Cell Carcinomas in Children and Adults have been summated as follows: [11]
Paediatric Individuals who have ALK Transformation Renal Cell Carcinoma – of Microscopy pathology examination of a paediatric individuals who has ALK Translocation Renal cell carcinoma would tend to show: [9] [18].
Diffuse infiltrating growth pattern that is sheet like.
Evidence of lymphoplasmacytic infiltrate as well as intra-vascular sickling.
Round, oval and polygonal tumour cells that contain abundant vaguely granular eosinophilic cytoplasm, as well as frequent intra-cytoplasmic lumens.
Presence of abundant mucin within the background as well as intra-cytoplasmic mucin.
Presence of moderately polymorphic, and predominantly vesicular nuclei, that contain small nucleoli, and occasional grooves, as well as rare vacuoles.
Adult Individuals who have ALK Transformation Renal Cell Carcinoma – of Microscopy pathology examination of an adult individuals who has ALK Translocation Renal cell carcinoma would tend to show: [13] [17].
Evidence of more heterogeneous architecture with demonstration of solid, mucinous cribriform, reticular, tubular, papillary growth, dis-cohesive sheets or infiltrating single cells.
Presence of eosinophilic polygonal cells, rhabdoid or signet ring as a result of intracytoplasmic vacuolization.
The tumour could contain Psammoma bodies as well as foamy macrophages.
Immunohistochemistry staining studies
Positive staining
It has been iterated that immunohistochemistry staining studies of ALK Translocation Renal Cell Carcinoma specimens tend to show tumour cells that exhibit positive staining for the following tumour markers: [11]
ALK
PAX8
INI1 (Intact)
AE1/AE3
CAM5.2
CK7
EMA
LMWCK
P53
Vimentin
CD10 (this tends to be variable)
AMACR (this tends to be variable)
It has also been iterated that immunohistochemistry staining studies of ALK Translocation Renal Cell Carcinoma specimens tend to show tumour cells that exhibit positive staining for the following tumour marker: [11]
TFE3 (within the majority of the tumour cells) [12] [14] [17].
Negative staining
It has been iterated that immunohistochemistry staining studies of ALK Translocation Renal Cell Carcinoma specimens tend to show tumour cells that exhibit negative staining for the following tumour markers: [11]
RCC
CD117/KIT
S100
HMB45
Melan A
Cathepsin K
WT1
It has also been iterated that immunohistochemistry staining studies of ALK Translocation Renal Cell Carcinoma specimens tend to show tumour cells that exhibit negative staining for the following tumour marker: [11]
Ki67 – In this case it has been stated that the Ki67 has tended to be very low and this has tended to be less than 5%.
Electron Microscopy Examination Features
It has been iterated that electron microscopy examination of ALK Translocation Renal Cell Carcinoma does show tumour cells that contain bundles of tonofilaments, intercellular junctions, desmosomes, intra-cytoplasmic lumens that are lined by microvilli as well as lipofuscin-like lysosomal structures [11] [18].
Molecular and cytogenetics examination features
It has been iterated that electron microscopy and cytogenetics studies of ALK Translocation Renal Cell Carcinoma specimens tend to show the following features: [11].
VCL-ALK fusion which has tended to be strongly associated with sickle cell trait [19].
TPM3-ALK fusion which has tended not to be associated with sickle cell trait [18].
Other less common fusions that include: STRN-ALK, EML4-ALK, and HOOK1-ALK [12] [20].
Clonal inversion that involve 2p23 [14]
No fusion but increased copy number of ALK1- there may be no evidence of fusion but an increased number of ALK1 may be found [[21].
It has also been pointed out that it is worth noting that ALK copy number gain could be found in up to 10% of clear cell renal cell carcinoma and this also tends to be associated with worse cancer specific survival [11] [22].
Differential diagnosis
It has been pointed out that with regard to differentiating ALK Translocation Renal Cell Carcinoma, broadly speaking, immunohistochemistry staining studies with utilization of ALK antibody as well as molecular studies that confirm ALK Translocation are critical for the diagnosis of ALK Translocation Renal Cell Carcinoma [11]. Some of the differential diagnoses of ALK Translocation Renal Cell Carcinoma include:
Renal medullary carcinoma – [11]
It has been stated that renal medullary carcinoma also does tend to affect young patients who have sickle cell trait and that the tumour tends to be a very large aggressive tumour and which also tends to be associated with metastasis at the time of the initial presentation of the lesion.
It has been stated that in cases of Renal medullary carcinoma, there tends to be loss of INI1 and the KI67 proliferation rate tends to be high [11].
Collecting duct carcinoma -
It has been pointed out that collecting duct carcinoma of the kidney also does affect the medullary area of the of the kidney but the tumour tends to be larger with regard to its size, and the tumour tends to be a predominantly tubular growth, with evidence of stromal desmoplasia as well as the Ki67 proliferation rate of the tumour tends to be high [11].
MiT Family Translocation Renal Cell Carcinoma -
It has been iterated that MiT Translocation Renal Cell Carcinoma could have morphology that is similar to the morphology of ALK Translocation Renal Cell Carcinoma but MiT Translocation Renal Cell Carcinoma does tend to be TFE3 positive [11].
It has been stated that MiT Translocation Renal Cell Carcinoma can exhibit positive immunohistochemistry staining for melanocyte markers and for cathepsin K.
Papillary Renal Cell Carcinoma and mucinous tubular and spindle cell carcinoma –: [11]
It has been iterated that the aforementioned tumour (s), also tend to contain tubule-papillary architecture, and also tend to produce mucin, tend to contain Psammoma bodies, tend to contain macrophages as well as overlapping immune-profile.
The aforementioned tend to exhibit absence of ALK expression with negative staining for ALK.
Unclassified Renal Cell Carcinoma [11]
It has been pointed out that unclassified renal cell carcinoma tends to exhibit negative immunohistochemistry staining for ALK [11].
Metastases
It has been stated that metastases to the kidney from a primary malignant tumour elsewhere especially ALK re-arranged adenocarcinoma of the lung is one of the differential diagnoses of ALK Translocation Renal Cell Carcinoma [11].
It has been stated that with regard to metastases within the kidney from a primary tumour elsewhere, immunohistochemistry staining studies tend to exhibit positive staining for TTF1/Napsin A as well as negative staining for PAX8.
It has also been advised that in order to diagnose metastasis to the kidney, it is important to check the clinical history of the patient. [11] [12] [17]
(B) Miscellaneous narrations and discussions from some case reports, case series, and studies related to ALK Translocation Renal Cell Carcinoma.
Woo et al. [3] reported a 14-year-old male who had manifested with visible haematuria. He had computed tomography (CT) scan of abdomen and pelvis and renal tract which showed a 5.3 cm x 4.5 cm that was well-demarcated, solid/cystic mass within the upper pole of his left kidney (see figure 1A). He was asymptomatic otherwise. The results of his routine haematology and biochemistry blood tests were within normal range. He had haemoglobin electrophoresis which showed normal red blood cells. He underwent left radical nephrectomy for a stage III (pT1bN1) tumour and he did not receive any adjuvant therapy pursuant to that. During his 4 months post-operative follow-up, there was no evidence of local recurrence or metastasis.
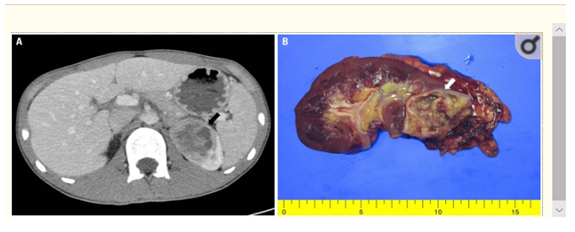
Gross findings of ALK rearrangement-associated renal cell carcinoma. (A) A well-demarcated, solid cystic mass (arrow), at the upper pole of the left kidney is observed on abdominal computed tomography. (B) The mass is yellow-to-grey, involving the renal medulla and cortex. [3] which permits unrestricted non-commercial use, distribution and reproduction in any medium, provided the original work is properly cited.
Macroscopic pathology examination of the specimen showed that the tumour mass had involved the medulla and cortex of the left kidney (see figure I B). Microscopy pathology examination of the tumour demonstrated a diffuse growth, focal tubolo-cystic changes, and multi-focal inflammatory cell infiltration that simulated medullary renal carcinoma (RMC) (see figure 2A and figure 2 B). The infiltrated inflammatory cells comprised mainly of lymphocytes. The tumour cells were noted to be dis-cohesive as well as epithelioid and contained abundant eosinophilic cytoplasm as well as cytoplasmic vacuoles. Even though majority of the nuclei were round to oval, some of the nuclei were noted to be multi-nucleated as well as pleomorphic consistent with ISUP grading of 4. Mitosis was visualized in two to three of the cells per 10 high-power fields with a Ki-67 proliferation index of 10%. There was abundance of mucin within the background as well as intracytoplasmic mucin was visualized. There was evidence of coagulative necrosis within the tumour. Immunohistochemistry staining studies of the tumour showed that the tumour cells had exhibited diffuse positive staining for pan-cytokeratin as well as preservation of INI1 expression. The tumour cells additionally exhibited positive staining for PAX8, CD10, as well as for Vimentin. Immunoreactivity for TFE3, but without TFE3 re-arrangement was found. Next generation sequencing studies of the tumour demonstrated a TPM3-ALK fusion gene between exon 7 of TPM3 and exon 20 of ALK. The tumour demonstrated membraneous as well as cytoplasmic ALK-expression within the tumour cells (see figure 2 C). Woo et al. [3] stated the following:
With the incusion of their reported case, 8 cases of TPM3-ALK Renal cell carcinomas had been reported in the literature.
TPM3-ALK RCCs had been reported in five (5) teenagers and three (3) young to middle age adults.
Men and women had been affected by TPM3-ALK RCC equally; nevertheless, the number of patients who had so far been reported as having TPM3-ALK had been too small to seek any meaning into the sex distribution of the tumour.
None of the patients that had been reported as having TPM3-ALK RCC had sickle cell trait.
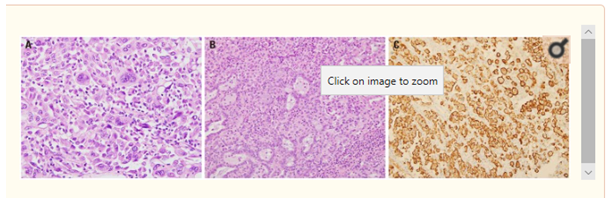
Microscopic findings of ALK rearrangement-associated renal cell carcinoma. (A) The tumour cells are dis-cohesive and epithelioid with abundant eosinophilic cytoplasm, cytoplasmic vacuoles, and intracytoplasmic mucin. Some tumour cells have extreme nuclear pleomorphism and multinucleated giant cells (H&E, x400). (B) The tumour shows diffuse growth and focal tubulo-cystic changes (H&E, x200). (C) Membranous and cytoplasmic ALK expression was confirmed by immunohistochemistry (x200). [3] which permits unrestricted non-commercial use, distribution and reproduction in any medium, provided the original work is properly cited. [23] screened consecutively resected renal cell carcinomas (RCCs) from one institution for the expression of ALK with utilization of immunohistochemistry staining studies which was ensued by the undertaking of fluorescence in situ hybridization to in order to confirm the ALK gene alteration in ALK immunohistochemistry staining positive cases of renal cell carcinoma. Lee et al. [23] screened 829 RCCs by undertaking immunohistochemistry staining studies on the specimens of the tumours and they undertook fluorescence in situ hybridization analysis with utilization of ALK dual-colour break-apart re-arrangement probe. Histopathology review analysis and additional immunohistochemistry analyses were undertaken with regard to the positive cases. With regard to the results, Lee et al. [23] reported that they did find 1 ALK positive case and the initial histopathology examination diagnosis of the tumour was papillary renal cell carcinoma type 2. The finding of 1 ALK positive RCC out of 829 cases constituted 0.12% the RCC cases and there were 53 cases of papillary renal cell carcinoma which meant that one case of the 53 cases constituted 1.9% of papillary renal cell carcinomas being positive for ALK. The patient was a 44-year-old man whose renal cell carcinoma was diagnosed incidentally based upon routine medical check-up assessment. He was alive and well 12 years pursuant to his operation without any evidence of local recurrence or metastasis. Pathology examination of the tumour demonstrated a papillary and tubular pattern and immunohistochemistry staining of the tumour showed tumour cells that exhibited focal positive staining for CD10, and positive staining for: epithelial membrane antigen (EMA), cytokeratin 7, pan-cytokeratin, PAX-2, as well as for vimentin. Lee et al. [23] made the ensuing conclusions:
They had found the first case of RCC that was associated with ALK gene re-arrangement in Korean patients by utilization of ALK immunohistochemistry staining studies among 829 patients who had renal cell carcinomas.
The tumour demonstrated similar histopathology examination features and immunohistochemistry staining features that were similar to the features that were found in previously reported adult cases of renal cell carcinoma that were associated with ALK re-arrangement, and the tumour portended a relatively good prognosis.
It would be stated that the findings of this study has demonstrated additional pathology features of renal cell carcinomas. Nevertheless, some people would argue that the finding of 1 case out of 829 RCCs that amounted to 0.12% of cases being ALK re-arrangement RCCs which was associated with a good prognosis following routine radical nephrectomy and no adjuvant treatment would not be cost-effective and if similar findings are made then clinicians in the less resourced developing countries would consider the option of not undertaking routine ALK-assessments of their RCCs in that it would appear to be more beneficial to utilize the resources for the study on the investigation of other malignancies of the results of the studies would provide information related to an alternative / additional treatment that would be aimed at improving the prognosis of patients.
Chen et al. [24] screened for ALK expression in 87 cases of pathology examination based diagnosed clear cell renal cell carcinomas (ccRCCs) by undertaking immunohistochemistry staining studies. Chen et al. [24] stated that four patients had tested positive for ALK expression based upon the immunohistochemistry studies and out of them they had confirmed the ALK expression by utilization of fluorescence in situ hybridization (FISH) test. Additionally, Chen et al. [24] did detect the existence of the echinoderm micro-tubule-associated protein-like 4/anaplastic lymphoma kinase (EML4-ALK) (E13:A20, variant 1) fusion gene in tumours from the two patients also with utilization of rapid amplification of cDNA ends (RACE)-coupled PCR sequencing and RT-PCR. Chen et al. [24] also pointed out that they had first shown that enforced EML4-ALK expression could significantly promote in vitro proliferation, clonogenic colony formation and apoptosis resistance in HK2 immortalized normal tubular epithelial cells as well as their in vivo outgrowth when injected into immunocompromised nude mice. Chen et al. [24] reported their additional important finding that demonstrated that this pro-tumorigenic effect had been completely abolished by utilization of ALK-specific inhibitor crizotinib, which had indicated the potential effectiveness of ALK-specific inhibitors with regard to the treatment of ALK-re-arranged clear cell renal carcinoma (ccRCC) patients. They concluded that their data had revealed that ALK fusions do exist in adult clear cell renal cell carcinoma (ccRCC) and this finding would provide a rationale for the utilization of ALK inhibitor therapy in the management of selected patients who have clear cell renal cell carcinoma (ccRCC). It would be argued that this finding is significant in that if the results are reproduced in human beings, then this would provide concrete evidence that routine screening for ALK expression in all RCCs would prove useful with regard to the identification of patients who undergo treatment for ccRCC who would benefit from utilization of ALK inhibitors as adjuvant treatment for curative intent purposes.
Kuroda et al. [25] described 12 ALK-RCCs from 8 establishments together with their detailed clinical, pathological, immunohistochemical (IHC), fluorescence in situ hybridization (FISH), as well as next-generation sequencing (NGS) analyses. Kuroda et al. [25] reported that the ages of the patients had ranged between 25 years and 68 years and their mean was 46.3 years. Seven of the patients were females and five of the patients were males which demonstrated a female to male ratio of 1.4:1. The sizes of the tumours had ranged between 1.7 cm to 7.0 cm and the mean and median sizes of the tumours were 3.15 cm and 2.5 cm respectively. The pathology TNM staging of the tumours were documented as pT1a in 7 cases, pT1b in 1 patient, and pTN3a in 4 patients respectively. Follow-up information was available for 9 patients out of the 12 patients for which the follow-up had ranged between 2 months and 153 months and the mean follow-up was 37.6 months. Eight (8) of the patients were alive with no evidence of local recurrence or metastasis but one (1) patient was alive with distant metastases. Based upon the pathology examination features of the tumours, the tumours were stated to have demonstrated heterogeneous and difficulty to classify in 10 out of the 12 cases which typically had shown diverse architectural as well as cellular morphologies which had included: papillary, tubular, tubulocystic, solid, sarcomatoid (spindle cell), rhabdoid, signet-ring cell, and intracytoplasmic vacuoles, which were often set within a mucinous background. With regard to the remaining two tumours, one of them had morphology that simulated mucinous tubular and spindle cell renal cell carcinoma (MTSC-RCC-like), and the remaining tumour had features indistinguishable from metanephric adenoma. One additional case was also reported to have demonstrated a focal metanephric adenoma-like area, within an otherwise heterogeneous tumour. Immunohistochemistry staining studies of the tumours revealed that all the tumours had exhibited diffusely positive staining for ALK and PAX8. With regard to both cases that had metanephric adenoma-like features, WT1 and ALK were co-expressed in their immunohistochemistry studies. FISH tests were utilized that demonstrated ALK re-arrangement in 9 out of 11 tumours. ALK fusion partners were also identified in 12 cases with utilization of NGS, that included the previously reported cases of: STRN in 3 cases, TPM3 in 3 cases, EML4 in 4 cases, and PLEKHA7 in 1 case, as well as three novel fusion partners that included: CLIP1 in 1 case, KIF5B in 1 case, and KIAA127 in 1 case. Kuroda et al. [25] made the ensuing iterations:
ALK-RCC does represent a genetically distinct entity that demonstrates a heterogeneous histopathological morphology features which had been expanded in their studies to include unreported metanephric adenoma-like and MTSC RCC-like variants.
They would advocate a routine ALK immunohistochemistry staining studies screening for “unclassifiable RCC” that depict heterogeneous features.
Yang et al. [26] reported a 58-year-old Chinese man who had been diagnosed as having ALK Translocation-associated Renal Cell carcinoma in the upper pole of his right kidney. Radiology imaging of his abdomen, pelvis and renal tract including ultrasound scan and computed tomography scan revealed a 2.4 cm x 2.2 cm hypoechoic mass that had clear cut margin within the upper pole of his right kidney by the ultrasound scan, and a 1.9 cm x 1.8 cm x 2.2 cm low-density mass within the upper pole of his right kidney. Ne metastasis was demonstrated. He did not have sickle cell trait, and he did not have any distinct clinical symptoms. He underwent laparoscopic right radical nephrectomy. Pathology examination of the tumour showed that the tumour comprised of sheets of large cells that contained abundant eosinophilic cytoplasm as well as indistinct cell borders that contained conspicuous intra-cytoplasmic vacuoles. Microscopy examination of the tumour showed that the nuclei of the tumour cells were enlarged and had features that were graded as nucleolar grade 4. Immunohistochemistry staining of the tumour showed that the tumour cells had exhibited diffusely positive staining for: PAX8, Keratin (AE1/AE3), epithelial membrane antigen (EMA), as well as CK7. Fluorescent in situ hybridization (FISH) test of the tumour demonstrated re-arrangement of ALK within the tumour cells. Yang et al. [26] stated the following:
The dramatic treatment benefit of therapies that target ALK for patients who have non-small cell carcinoma of the lung (NSCLC) that is driven by ALK fusion has now been widely accepted. [27] [28].
Recently, the results of a few studies have demonstrated that ALK inhibitors, like ebtrectinib, and alectinib, could be dramatically effective with regard to the treatment of ALK Translocation-Associated Renal Cell Carcinomas [4] [29] [30]
Despite the fact that the incidence rate of ALK Translocation-Associated Renal Cell Carcinomas is low, the identification and in-depth investigation of ALK Translocation Renal Cell Carcinomas does seem to be very important in view of the potentially similar therapeutic response as well as prospects.
Yang et al. [26] made the ensuing concluding iterations:
ALK-Translocation-Associated Renal Cell carcinoma is an uncommon sub-type of adult renal cell carcinoma.
The diagnosis of ALK Translocation RCC is very difficult to diagnose in view of its very wide spectrum of histopathological features.
They would suggest that renal cell carcinomas (RCCs) should be routinely screened for the expression of ALK by utilization of immunohistochemistry (IHC) staining studies due to the fact that the individual patient might benefit from ALK inhibitors therapy.
Jenneau et al. [31] reported an exceptional case of renal cell carcinoma (RCC) that was associated with ALK translocation in an adult. The tumour had been localized within the left kidney and had measured 4 cm. Pathology examination of the tumour demonstrated that the tumour had comprised of sheets of large eosinophilic cells that contained frequently intra=cytoplasmic vacuoles. The nuclei were noted to be very large and were graded as nucleolar grade 3. Immunohistochemistry staining of the tumour showed that the tumour cells had exhibited diffusely positive staining for PAX8, and vimentin, as well as focally positive staining for CK7. Immunohistochemistry staining for ALK demonstrated diffusely positive staining and fluorescent in situ hybridization (FISH) test demonstrated re-arrangement of ALK in many tumour cells. Jeanneau et al. [31] stated the following:
By the time of the report of their case, less than 17 cases of RCCs with ALK re-arrangements had been reported in children and adults.
The prognosis of ALK Translocation-Associated RCC had remained uncertain; nevertheless, ALK re-arrangement could be of potential value for targeted treatment with crizotinib.
Hang et al. [32] reported a peculiar renal cell carcinoma which morphologically mimicked metanephric adenoma that harbored a novel PLEKHAF7-ALK fusion. Microscopy pathology examination of the tumour showed that the tumour had comprised of bland epithelial cells that contained scant to moderate amount of amphophilic cytoplasm, round and uniform nuclei, delicate chromatin, as well as inconspicuous nucleoli that were arranged in tightly packed small acini and angulated tubules. Microscopy examination of the tumour also demonstrated papillary formation, intraluminal glomeruloid tufts, microcysts, as well as solid nests. Psammomatous calcifications were visualized within the tumour. Immunohistochemistry studies of the tumour demonstrated that the tumour cells had exhibited diffusely positive staining for CK7, AMACR, PAX8, as well as ALK. But the tumour cells did exhibit negative staining for WT1< BRAF V600E, CD57, Carbonic anhydrase IX, TFE3, and cathepsin K. Fluorescence in situ hybridization (FISH) test of the tumour showed breaking apart of ALK. A novel PLEKHAF7 exon 18-ALKexon20 fusion was identified with utilization of ArcherDX FusionPlex next-generation sequencing panel and this was additionally confirmed by means of reverse-transcriptase PCR. Hang et al. [32] made the ensuing conclusions:
Their case had demonstrated that in contrast to previous reported cases that showed high-grade tumour cells, ALK-Rearranged renal cell carcinoma could manifest as low-grade renal tumour that simulate metanephric adenoma.
Immunohistochemistry staining studies and molecular testing are helpful with regard to the identification of this tumour, which could be eligible for inhibitor-targeted treatment.
Tao et al. [5] reported a 22-year-old man who had manifested with visible haematuria and anaemia. He had computed tomography (CT) scan which showed a 14 cm x 13 cm x 12 cm heterogeneous mass which had almost completely replaced his right kidney parenchyma. He did undergo a right radical nephrectomy and pathology examination of the tumour showed a stage III (pT3aN1) high-grade (nuclear grade IV) renal cell carcinoma with pleomorphic features as well as 23 tumour positive lymph nodes. The tumour was felt to be completely resected. He had CT scan 2 months pursuant to his surgery which did not reveal any local recurrence or metastasis. Next-generation sequencing of the primary tumour demonstrated a VCL-ALK translocation generating a fusion between exon 16 of VCL and exon 20 of ALK. Histopathology examination of the tumour revealed markedly pleomorphic cells that contained abundant eosinophilic (rhabdoid) cytoplasm as well as cytoplasmic vacuoles. INI-1 (BAF47) was retained by the tumour. Immunohistochemistry staining studies of the tumour showed overexpression of ALK. Fluorescence in situ hybridization (FISH) test confirmed VCL-ALK gene fusion. He had haemoglobin electrophoresis which confirmed presence of sickle cell trait. His 12-months post-operative surveillance radiology imaging showed presence of confluent lymph node enlargement within his right retro-crural space as well as an enlarged left superior mediastinal metastatic node which was biopsied and pathology examination of the specimen confirmed metastatic disease. The patient was enrolled in a clinical trial of entrectnib (RXDX-101); Clinical Trials.gov identifier: NCT02097810). Four weeks pursuant to commencement of entrectinib 600 mg per day, he had a CT scan which showed 31.4% decrease in the size of the disease or partial response. The patient continued his treatment and at his 15 months follow-up radiology imaging had shown 61.9% decrease in the size of the metastatic disease. His treatment with entrectinib was continued for 19 months which he tolerated well with the exception of grade 1 peripheral lower extremity oedema and grade 2 weight gain. After 19 months of treatment radiology follow-up imaging demonstrated progression of the metastatic disease with increased mediastinal lymph node enlargement and entrectinib treatment was stopped. Lessons that were learnt from this case report include (a) Patients who have ALK Translocation-associated Renal Cell Carcinomas might respond to entrectinib therapy. (b) Large sized ALK Translocation-Associated Renal Cell Carcinomas that are also associated with lymph nodes positive for tumour would be aggressive tumours with a great chance of the subsequent development of metastases that would continue to progress and these metastatic lesions might initially respond to entrectinib therapy but would subsequently progress further. (c) Perhaps the best time to commence entrectinib therapy is immediately after complete excision of the tumour as adjuvant therapy so that if there are microscopic metastases that are too small for radiology imaging to identify the tumour cells would be completely destroy but if one waits till the metastatic tumour burden is large there could be problems in that perhaps the medicaments might not be able to completely destroy all the metastases. (b) Perhaps other additional adjuvant treatments including adjuvant radiotherapy and immunotherapy should also be tried in such situations of large sized tumours with nodal disease after the operation.
Yu et al. [10] embedded into tissue microarrays for immunohistochemistry staining a total of 477 Renal Cell Carcinoma (RCC) patients in China. They undertook fluorescence in situ hybridization (FISH) as well as fluorescence quantitative transcription polymerase chain reaction (RT-PCR) to identify as well as confirm re-arrangement of ALK, as well as to identify the genes that are fused with ALK. They identified ALK expression in two out of 477 renal cell carcinomas (0.42% of cases). They undertook FISH analysis and two tumours showed either a 1R1G1F or a 2R2G signal pattern, which indicated re-arrangement that had involved ALK. They also undertook fluorescence quantitative RT-PCR which identified TPM3-ALK fusion and EML4-ALK fusion transcripts in two tumours respectively. They did analyse follow-up data on the two cases together with eight other ALK-re-arranged Renal Cell Carcinomas (RCCs) that had been reported in the literature. They found that with regard to the outcome, two patients had died from renal cell carcinomas, during the 16th month and 48th month respectively pursuant to their surgery. The 5-year cancer-specific survival of the patients who had ALK-rearranged renal cell carcinomas (RCCs) were found to be lower in comparison with that of patients who had the International Society of Urological Pathology (ISUP) G1, G2, and G3 clear cell renal cell carcinoma (CCRCC) as well as papillary renal cell carcinoma (PRCC), but the 5-year cancer-specific survival was higher than that of patients who had G4 CCRCC and PRCC. Yu et al. [10] made the following conclusions:
ALK-rearranged renal cell carcinoma (RCC) is an uncommon sub-type of renal cell carcinoma (RCC) which is associated with distinct histopathological features as well as poor prognosis.
The identification of ALK-rearranged renal cell carcinoma (RCC) does have an important clinical significance in view of the fact that patients who have that type of carcinoma might derive benefit from ALK inhibitor treatment as is utilized in adenocarcinoma of the lung.
Smith et al. [8] reported the third case of a renal cell carcinoma that bore a fusion of the vinculin (VCL) as well as anaplastic kinase (ALK) genes. Smith et al. [8] stated that like the other two previously reported cases, their reported tumour did occur in a young six years old patient who had sickle cell trait which had demonstrated distinct morphology features that included medullary epicentre, dis-cohesive polygonal or spindled-shaped cells that contained prominent cytoplasmic vacuoles, as well as prominent lymphocytic infiltrate. The tumour cells did demonstrate focal membranous labelling for ALK protein with utilization of immunohistochemistry, ALK gene re-arrangement with utilization of fluorescence in situ hybridization, and a specific VCL-ALK gene fusion by utilization of reverse transcriptase polymerase reaction test. Smith et al. [8] stated that VCL-ALK renal cell carcinoma could represent the eighth (8th) sickle cell nephropathy.
Kusano et al. [20] stated that anaplastic lymphoma kinase (ALK) translocation renal cell carcinomas (ALK Translocation-associated RCCs) had been reported by many independent groups recently and that the clinical behaviour as well as the histopathological features of these carcinomas are not fully understood in view of the paucity of these cases. They described 2 cases of renal cell carcinomas that were associated with a novel striatin (STRN)-ALK fusion. The first case was that of a 33-year-old woman who had sickle cell trait who had undergone right nephrectomy for a right renal mass and who developed late recurrence within the para-aortic lymph nodes twice 10 years and 12 years pursuant to her initial surgery. Following her second recurrence, she was carefully observed without any treatment. Twenty six years pursuant to her initial nephrectomy, she underwent her second para-aortic lymphadenectomy as well as she underwent gastrectomy for a newly developed primary gastric cancer. The resected para-aortic lymph nodes were found upon pathology examination to have been largely replaced by metastatic carcinoma. The second case was that of a 38-year-old man who did not have sickle cell trait who had undergone cytoreductive nephrectomy that was followed by his treatment with sunitinib for metastatic renal cell carcinoma. Kusano et al. [20] stated that in both cases, the tumour upon pathology examination showed solid, papillary, tubular, as well as mucinous cribriform structures. Psammoma bodies were also occasionally visualized within the stroma. The tumour cells contained large nuclei and prominent nucleoli and the cells contained eosinophilic cytoplasm. Rhabdoid cells and signet-ring cells were also seen in the tumours. Intra-cytoplasmic deposition of mucin as well as background mucinous stroma were also visualized. With regard to the second case, tumour necrosis was visualized within some areas of the tumour. The tumour cells did exhibit diffusely positive staining for ALK with regard to both cases. By the utilization of fluorescence in situ hybridization test, ALK translocation was confirmed and further gene analysis was undertaken of the tumours which did reveal STRN-ALK fusion. Kusano et al. [20] iterated that these reported cases had provided great insight into ALK translocation-associated renal cell carcinomas.
Ahluwalia et al. [33] stated the following:
Renal cell carcinoma with Xp11.2 translocations and TFE3 fusions (Xp11.2TRCC) had been recognized as a distinct tumour entity in 2004 World Health Organization (WHO) of kidney tumours [1]
Renal cell carcinoma translocations which had been primarily described in the paediatric population and which had accounted for 30% of children had recently been reported in the adult population as associated with poorer prognosis [2].
The tumours had been typified by a variety of chromosome translocations, and all of the chromosome translocations have involved a breakpoint at Xp11.2 as well as fusion that involves the TFE gene (see figure 3). Ahluwalia et al. [33] reported two young female adult patients who had been referred to them. One of the patients was a 20-year-old, who was incidentally found to have a mass within the right kidney (who would be referred to as patient 1 in this summation), and the second patient was a 17-years, who had manifested with visible haematuria that was associated with blood clots as well as right flank pain (who would be referred to as patient 2). Contrast-enhanced computed tomography scan with regard to both patients demonstrated findings that were consistent with kidney tumour (see figure 4). Pursuant to the undertaking of appropriate assessment, both patients did undergo right radical nephrectomy. With regard to patient 1, during the operation, the retroperitoneum was found to contain enlarged hilar lymph nodes. With regard to patient 1, macroscopic pathology examination of the nephrectomy specimen demonstrated a well-encapsulated predominantly unilocular cystic lesion that contained grey brown solid areas and focal areas of haemorrhage and the tumour measured 7.5 cm x 9 cm x 7 cm (see figure 5 a). With regard to patient 2, Macroscopic pathology examination of the specimen demonstrated a well-defined encapsulated grey white to yellow white solid/cystic lesion within the mid-pole of the right kidney that measured 3 cm x 3 cm x 5 cm. Sinus fat infiltration by tumour was not visualized in any of the patients’ tumours. Microscopic pathology examination of the tumour showed that the tumour had comprised of cells that had been arranged in papillary pattern and they had contained eosinophilic cytoplasm and prominent nucleoli. (see figure 5b). Psammoma bodies were frequently visualized in the tumour. Mitosis was occasionally visualized. The hilar lymph node upon microscopy examination was seen to contain neoplastic infiltration with regard to one of the patients (see figure 6). The differential diagnosis was between Renal Cell Carcinoma with Xp11 translocation and papillary Renal Cell Carcinoma type 2. Immunohistochemistry staining studies of the tumours showed that the tumour cells had exhibited positive staining for Cd10, Vimentin, and EMA but the tumour cells exhibited negative staining for CK7. The features of the tumours were adjudged to be suggestive of renal cell carcinoma with Xp11 translocation. TFE3 gene mutation study was further undertaken which demonstrated that the immunostaining had shown that the tumour cells were positively stained for TFE3 but negative for cathepsin K. FISH analysis of the tumours demonstrated that 55% and 36% of the cells had split TFE3 signal in patient 1 and patient 2 respectively, which did support the diagnosis of translocation renal cell carcinoma. At their follow-up assessments which was approximated 12 months following their operations, they were well with normal clinical examination findings, normal chest x-ray, normal results of their laboratory blood tests and their MRI scans were normal with no evidence of any local recurrence or metastasis. Ahluwalia et al. [33] stated the following:
Xp11.2 translocation renal cell carcinomas in adult patients could be associated with advanced stages, large tumour sizes, and extra-capsular disease and could manifest with metastatic disease with possible poor prognosis.
Female preponderance tends to be seen in adults as was seen in their patients also.
With regard to young patients, Xp11.2 renal cell carcinoma should be suspected if prominent lymph node metastases are present as was found in their patients.
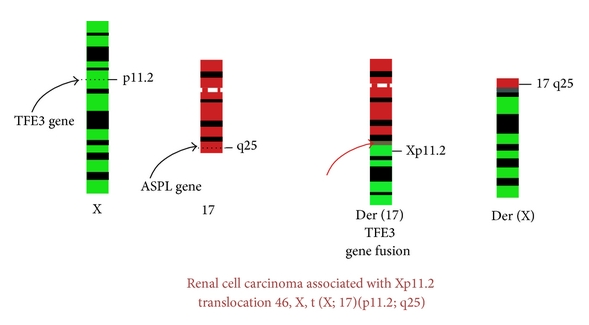
Renal cell carcinoma associated with Xp11.2 translocation 46, X, t(X; 17) (p11.2; q23). [33].

Contrast CT scan of the abdomen and pelvis in patient 1 with (a) axial section and (b) coronal section showing a large predominantly cystic (white arrow) right renal mass measuring 9 x 8 x 8 cm with solid mass (black arrow).[33].
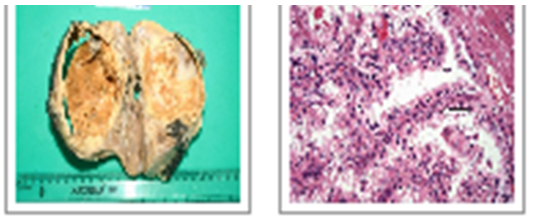
Cut surface showing well encapsulated predominantly unilocular cystic lesion with grey brown solid areas with focal areas of haemorrhage measuring 7.5 x 9 x 7 cm in size. (b) Microscopically, cells are arranged in papillary pattern (arrow) with some areas showing alveolar and nesting pattern. Cells showed abundant clear to eosinophilic cytoplasm with prominent nucleoli [33].

[33] undertook a study which was aimed at determining the incidence of Xp11 translocation renal cell carcinoma (RCC) in adults patients by utilization of cytogenetics and immunohistochemistry studies. Komai et al. [34] undertook cytogenetic studies prospectively with the use of tumour samples obtained from 443 consecutive adult Japanese patients whose ages had ranged between 15 years and 89 years who had undergone nephrectomy for renal cell carcinoma. They undertook TFE3 immunohistochemistry studies for cases in which cytogenetic results had not been obtained. They examined the clinicopathological characteristics of Xp11 translocation renal cell carcinoma. Komai et al. [34] stated that mitotic cells that were suitable for cytogenetic analysis had been obtained in 244 tumour samples that amounted to 55% of all the tumours, and among these, they did identify 4 cases of Xp11 translocation renal cell carcinoma that amounted to 1.6% of the tumours. Through the undertaking of TFE3 immunohistochemistry studies, 3 postive cases that amounted to 1.5% the tumours among 199 cases were obtained. The ages of the 7 patients had ranged between 15 years and 59 years and their median age was 41 years, and 15% of the renal carcinoma patients that accounted for 4 patients out of the 26 individuals who were younger than 45 years of age had this type of renal cell carcinoma. Out of the four (4) Xp11 translocation renal cell carcinoma patients whose karyotypes had been determined, two had an ASPL-TFE3 gene fusion. Out of these two (2) patients, one (1) patient had lung metastasis at initial presentation and the other patient developed hepatic metastasis 12 months pursuant to undergoing nephrectomy and died of the disease. The remaining two patients did have PRCC-TFE3 and PSF-TFE3 gene fusions respectively. Both of the patients did have nodal involvement but they remained free of disease for 3 and 5 years, respectively, following urgical resection of their lymph node metastases. Out of the 3 individuals who had been diagnosed with utilization of immunohistochemistry staining studies, 1 had nodal metastases and died 9 months pursuant to undergoing surgery. Komai et al. [34] made the ensuing conclusions:
Their reported study, was the first study to determine the incidence of Xp11 translocation renal cell carcinoma in adult patients.
They had found that the disease is relatively common in young adults.
Conflict of interest – None
Acknowledgements
Acknowledgements to:
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
