AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Abbas AR Mohamed, Consultant General and Laparoscopic Surgeon, Head of General Surgery Department, NGH –Madinah –KSA.
Citation: Abbas AR Mohamed, Safaa A Mobarki, Ashwag H Al Qabasani, Alaa A El Sayed and Nusiba A Al Shingiti (2020) Accuracy of Alvarado Scoring System and Selective Computed Tomography in Diagnosis of Suspected Cases of Acute Appendicitis: J Clinical Research Notes, 1(2); DOI:10.31579/2690-8816/015
Copyright: © 2020 Abbas AR Mohamed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 March 2020 | Accepted: 12 March 2020 | Published: 17 March 2020
Keywords: alvarado scoring; appendicitis; CT scan
Objective: To evaluate the diagnostic accuracy of combined Alvarado scoring system and selective computed tomography (CT) in the diagnosis of suspected cases of acute appendicitis.
Material and methods: This study was conducted during the period March 2018 to January 2020 at Prince Mohammed bin Abdul-Aziz hospital (NGHA) in Al Madinah, KSA. It is a prospective study involving 100 consecutive patients attending the emergency department with right iliac fossa pain, excluding children below the age of 14 years and pregnant women. All patients were initially assessed by the Alvarado scoring system, and the result of each patient was recorded in a separate predesigned data sheath. Based on the patient's calculated Alvarado scores, patients were stratified into three groups: Group A (score ≤ 4), Group B (score 5-6), and group C (score ≥ 7). All patients in group A were discharged from the emergency department with instruction to return if their symptoms persist or get worse while all patients in group B had an abdominal multidetector CT scan (MDCT) with IV contrast and no oral contrast to help the diagnosis. Group C patients had surgery without further investigation. Alvarado scores were compared to intraoperative findings and histopathological examination of the removed appendix in those who were operated. The sensitivity, specificity, positive and negative predictive values of the scoring system in each group were calculated with special reference to the role of CT scan in improving the diagnostic accuracy of the scoring system in the middle group (group B).
Result: 58 patients were male and 42 were female. Age range between 14 and 43 years with median age 24 years. Out of the 100 patients, 14 (8 males, 6 females) belonged to Group A, 23 (11 males, 12 females) to Group B and 63 (39 males, 24 females) to group C.
Two patients from group A (one male and one female) were returned with worsening symptoms and subsequently operated for acute appendicitis. CT scan established the diagnosis of acute appendicitis in 16 out of the patients of group B with subsequent histological confirmation of acute appendicitis in 15 of them. Histopathology confirmed the diagnosis of acute appendicitis in 32 out of 63 patients of group C.
Conclusion: Alvarado score has a high accuracy of ruling in and out acute appendicitis at the extremes of the score (≤7 and ≥4), however, the accuracy of the score to confirm or rule out acute appendicitis in the middle group (5 -6) is significantly low. Selective utilization of CT scan in patients in the middle of the score improves the diagnostic accuracy of the score and limits overutilization of CT scan in the other patients at the extremes of the score saving patients unnecessary exposure to radiation and health authorities’ time and cost without increasing the rate of negative appendectomy.
Acute appendicitis remained the most common of acute abdomen since Reginald H Filz, first described the disease and introduced the term appendicitis in 1886 (1)
Typical cases of acute appendicitis usually present with migrating pain start in the para-umbilical region and then localized to the right iliac fossa, associated with nausea, vomiting, low-grade fever, and leukocytosis. Typical cases of acute appendicitis are easy to diagnose and treat, however, atypical presentation is common, occurring in about 20 – 33% of cases (2).
Atypical presentations result from many factors including variation in the anatomical position of the appendix, extremes of age, and female sex during childbearing age. The diagnosis of atypical appendicitis is difficult and remains a clinical challenge for even experienced surgeons (3). Studies showed that the accuracy of the clinical diagnosis of acute appendicitis is correlating with the 57 surgeon’s experience and ranging between 76% and 92%, with values (4).
Despite recent advances in radiological imaging techniques, the diagnosis of appendicitis is still a clinical diagnosis based primarily on taking a proper medical history and conduct proper physical examination (5).
Accuracy of diagnosis of acute appendicitis entitles reaching an early and accurate diagnosis, without increasing the rate of negative appendectomies or perforation.
Misdiagnosis or delay in diagnosis of cases of acute appendicitis associated with serious complications and morbidities, on the other hand, Precaution appendectomy or negative appendectomy is an adverse outcome.
There general tendency of overdiagnosis of the condition to avoid complications related to delayed diagnosis or treatment resulted in a high rate of negative appendectomy.
The old dictums, “When in doubt, take it out” and ‘it is better to remove a hundred normal appendices than to leave an inflamed one” is no more valid. Negative appendectomies have an adverse effect as it leads to unnecessary surgery (3, 6), serious interruption of patient’s daily activities and a considerable waste of hospital resources (3, 7) in addition to the postoperative complications.
It was estimated that misdiagnosis occurs 20% of cases of appendicitis; however, negative appendectomy is found in (15-35%) of patients who were emergency operated for acute appendicitis (8-10).
Over the years various clinical scoring systems have been used to improve the diagnostic accuracy of acute appendicitis. Although many clinical scoring systems have been developed (11-15), the Alvarado scoring system is the most famous. The scoring system was devised in 1986 by the American surgeon Alfredo Alvarado who identified eight predictive factors to stratify risk of acute appendicitis in his single-center study involving 305 patients in Philadelphia (11).
Alvarado score is a 10-point scoring system, based on three signs, three symptoms, and one investigation. The scoring system classifies patients into three groups based on their scores. Low risk (unlikely to have acute appendicitis with score ≤ 4), Intermediate risk (have a possible diagnosis of acute appendicitis with score 4-5) and high risk (probably having acute appendicitis with score ≥ 7).
The high sensitivity and specificity of computed tomography (CT) in the diagnosis of acute appendicitis were well documented by many researchers. At present, CT plays an important role in the clinical decision-making process in acute appendicitis and is considered as the gold standard in the diagnostic work-up for suspected acute appendicitis (16–19).
In spite of the documented high sensitivity and specificity of CT scan in diagnosis of acute appendicitis and its considerable ability to reduce the level of negative appendectomy, some studies have shown that the use of CT does not necessarily change the clinical management of a patient, especially in those at high risk (20, 21). CT imaging may also delay the time of operation and, therefore, may increase the subsequent risk of perforation (22), expose patients to potentially harmful radiation (23), and possibly adds to the overall cost of the emergency department visit (24) in addition to the risk of ionizing radiation.
Increasing reliance and overutilization of (CT) imaging for the diagnosis of acute appendicitis should be discouraged especially in the developing world as it constitutes wasting of resources that should be reserved only for patients whose diagnoses remain uncertain.
Our study aims to evaluate the role of selective CT scan in improving the diagnostic accuracy of the Alvarado scoring system and hence suggest a clinical pathway for patients presenting with clinical features suggestive of acute appendicitis aiming to ensure high diagnostic accuracy without overutilization of CT scan as a diagnostic tool.
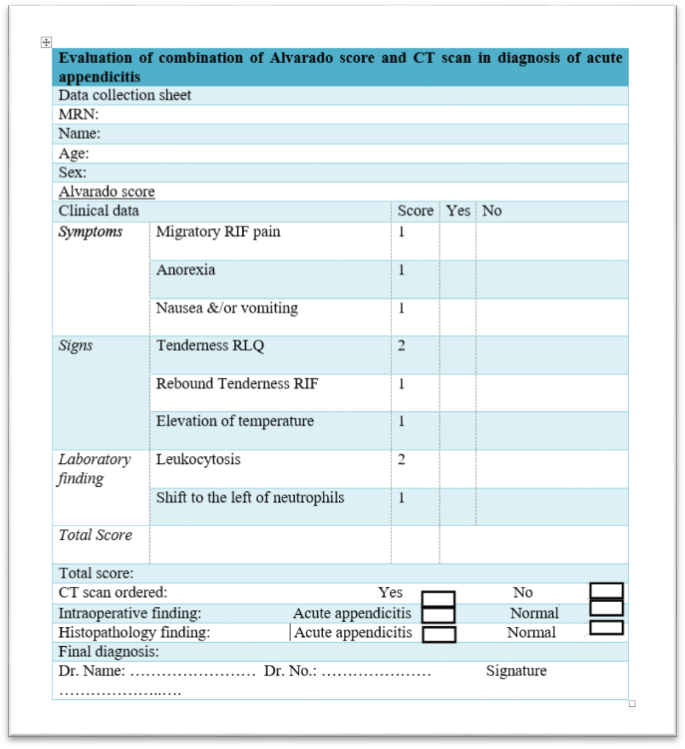
A prospective study of 100 consecutive patients who presented to the emergency department at Prince Mohammed bin Abdul-Aziz hospital NGHA in Al Madinah, KSA with the complaint of right iliac fossa pain, in the period from first of March 2018 to 30th of January 2020 excluding patients below the age of 14 years and pregnant females. Patients were assessed initially by detailed history, clinical examination, and basic laboratory tests including urine analysis, full blood count, urea and electrolytes, and coagulation profile. Alvarado score was calculated for each patient and recorded in a predesigned data sheath (Figure 1). Based on the calculated Alvarado scores, patients were stratified into three groups: Group A (Alvarado score ≤ 4) Group B (Alvarado score 5-6) and group C (Alvarado score ≥ 7).
Patients scored ≤ 4 were considered very unlikely to have acute appendicitis and were discharged from the emergency department with instruction to come back if their symptoms persist or become worse. Patients scored 5-6 were considered to have a diagnosis compatible with acute appendicitis, but not convincing enough to warrant appendectomy, they all had an abdominal MDCT scan and decisions were taken on the CT scan findings. Patients scored ≥ 7 were considered to have acute appendicitis and were submitted to operation without further investigations.
The abdomen CT scans were done by the multidetector scanner with IV contrast and no oral contrast. The criteria for positive CT scan were, appendix diameter >6 mm, appendix thickening >3 mm with wall enhancement, caecal and periappendiceal inflammatory changes.
The Alvarado scores were correlated with the CT scan, operative findings and the histopathology of the removed appendices of all patients who were operated for acute appendicitis. The sensitivity, specificity, positive and negative predictive values of the scoring system in each group were calculated with special reference to the role of CT scan in improving the diagnostic accuracy of the scoring system in the middle group. The collected data were analyzed using the 2x2 table with the calculation of the different variables using the following equations (table 1).
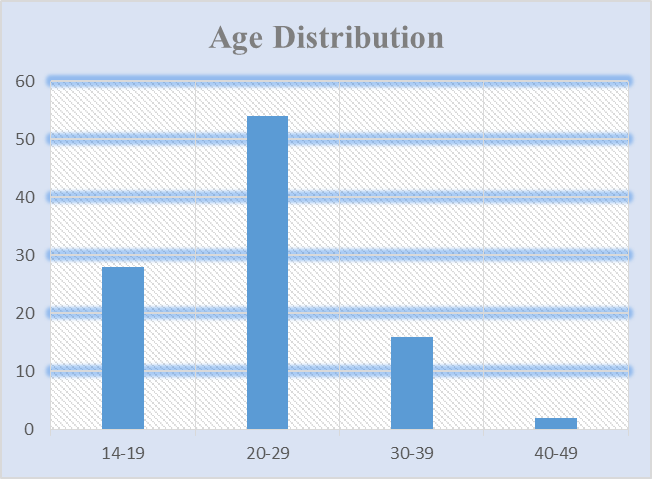
Among the 100 patients 58 were male (58%) and 42 were female (42%). The female to male ratio was 1:1.38 (Table 1, Diagram1). Age range between 14-43 years with Mean age was 24 years (Table 2, Diagram 2).
Sex | Number |
Male | 58 |
Female | 42 |
Total | 100
|
Table 2: Sex distribution.

Age / Years | No of patients |
14-19 | 28 |
20-29 | 54 |
30-39 | 16 |
40-49 | 2 |
Table 2: Age distribution.
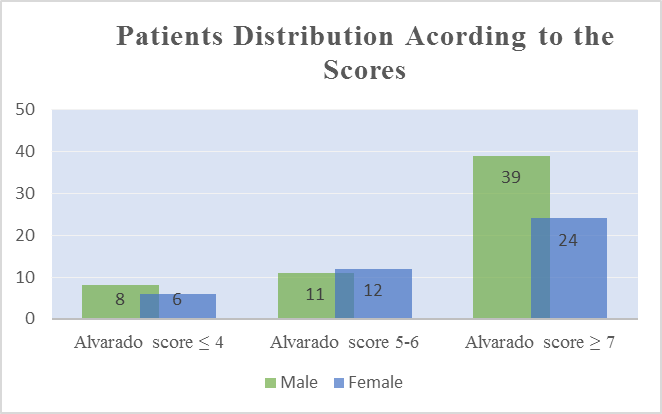
Patient’s distribution according to scoring system is shown in (Table 3, Diagram 3). In group A we had 14 patients (8 males and 6 females), group B 23 patients (11 males and 12 females) and group C 63 patients (39 males and 24 females).
Score | Male | Female | Total |
Alvarado score ≤ 4 | 8 | 6 | 14 |
Alvarado score 5-6 | 11 | 12 | 23 |
Alvarado score ≥ 7 | 39 | 24 | 63 |
Total | 58 | 42 | 100 |
Table 3: Patients distribution according to their scores
All patients in group A were discharged from the emergency department with instruction to return if their symptoms persist or get worse with only two patients (one male and one female) returned and subsequently operated for acute appendicitis. Each patient in group B had an abdominal MDCT scan which established the diagnosis of acute appendicitis in 16 patients (9 males and 7 females). On laparoscopic exploration one (male patient) was found to have torsion of epiploic appendicitis of the caecum bringing the number of the true positive to 15 with one false-positive result. The intraoperative findings and histopathological examination of the removed appendices confirmed the diagnosis of acute appendicitis in the 15 patients. The CT scan excluded acute appendicitis in the remaining 7 patients of this group who on followed up were found to have other pathologies rather than acute appendicitis. All patients of group C had appendectomy without further investigations. The histopathology of the removed appendices confirmed the diagnosis of acute appendicitis in 59 patients with 4 negative appendectomies (3 females and one male).
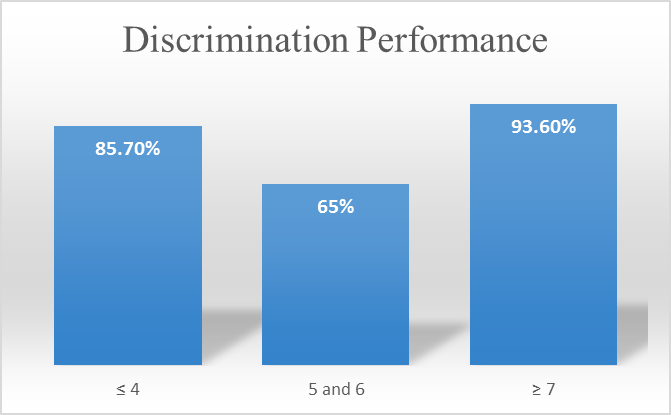
The overall diagnostic accuracy or discrimination performance of Alvarado score to rule out acute appendicitis in Group A and to rule in acute appendicitis in Group B and C was calculated and found to be 85.7% in Group A, 65% in Group B and 93.6% in Group C (Table 4, Diagram 4).
Score | Discrimination performance |
≤ 4 | 85.7% |
5-6 | 65% |
≥ 7 | 93.6% |
Table 4: Accuracy of Alvarado score in each group
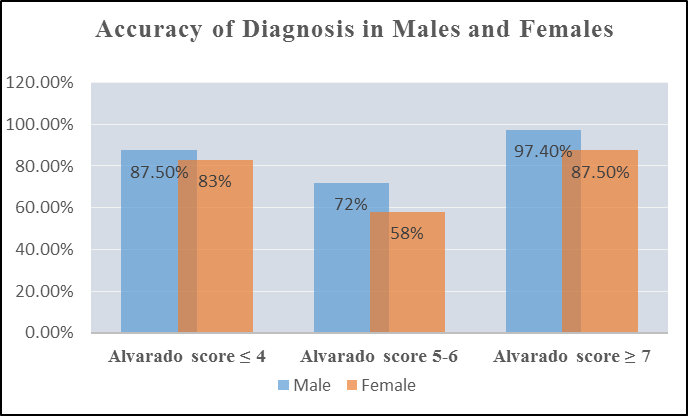
The diagnostic accuracy of Alvarado score stratified by sex was found to be (males 87.5% / females 83%) in Group A, (males 72% / females 58%) in Group B and (males 97.4% / females 87.5) in Group C. (Table 5,Diagram 5).
Score | Male | Female |
Alvarado score ≤ 4 | 87.5% | 83% |
Alvarado score 5-6 | 72% | 58% |
Alvarado score ≥ 7 | 97.3% | 87.5 |
Table 5: Accuracy of Alvarado score stratified by sex
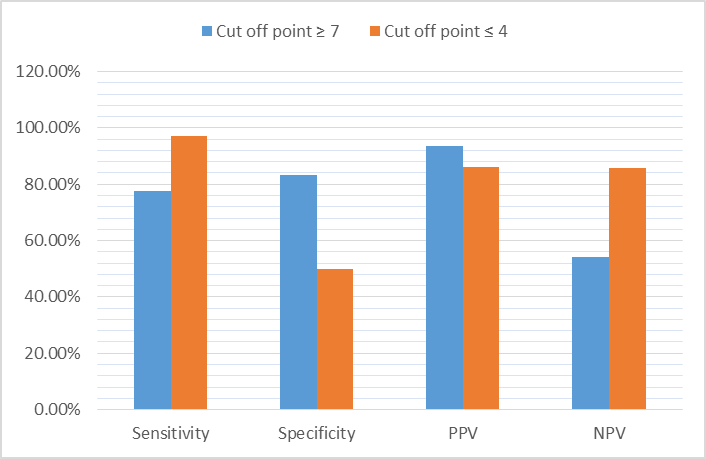
The calculated sensitivity, specificity, PPV, and NPV of 77.6%, 83.3%, 93.7% and 54% respectively at cut off point ≥ 7 and 97.3%, 50%, 86% and 85.7% respectively at cut off point ≤ 4(Table 6, Diagram 6).
Cut off point / variables | Sensitivity | Specificity | PPV | NPV |
Cut off point ≥ 7 | 77.6% | 83.3% | 93.6% | 54% |
Cut off point ≤ 4 | 97.3% | 50% | 86% | 85.7% |
Table 6: Alvarado score performance at cut off point ≥ 7and ≤ 4.
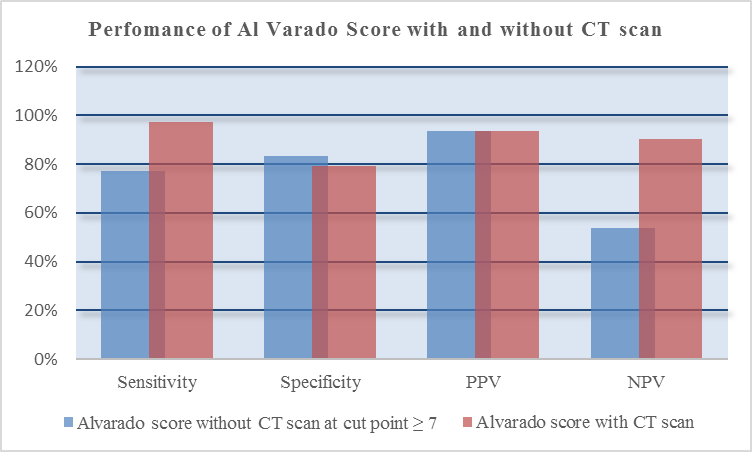
The calculated discrimination performance of the score with CT revealed sensitivity, specificity, PPV and NPV at cut off point ≥ 7 were 97.3%, 79.2%, 93.6%, and 90.4% respectively in comparison to the calculated discrimination performance of the score without CT of 77.6%, 83.3%, 93.7% and 54% respectively (Table 7, Diagram7).
The score/ the variable | Sensitivity | Specificity | PPV | NPV |
without CT scan | 77% | 83.3% | 93.6% | 54% |
with CT scan | 97.3% | 79.2% | 93.6% | 90.4% |
Table 7: Comparison of the performance of Alvarado score with and without CT scan.
Acute appendicitis is the most common surgical emergency seen in most hospitals throughout the world and the most common cause of acute abdomen requiring surgical intervention. Appendectomy remained the most commonly performed emergency surgical procedure since the first appendectomy was performed by Treves in England (25).
The incidence of acute appendicitis and male and female distribution varies from one population to another. The estimated lifetime risk is 8.6% for males and 6.7% for females in the United States (26). Addis's DG et al, (26) in their analysis of the epidemiology of appendicitis and appendectomy in the United States reported slight female to male predominance (1:1.3). A similar female to male ratio of 1:1.4 was reported by Omran, M et al, (27) in their study of the epidemiologic features of acute appendicitis in Ontario, Canada.
Körner H, et al,(28) in their Age-specific and Sex-specific Analysis of the incidence of Acute no perforated and perforated appendicitis, in 1486 Scandinavian patients reported male to female predominance. Similarly, Ceresoli M, et al, (29) in their retrospective cohort study derived from the administrative dataset of the Bergamo district healthcare system in Italy which involved 16544 consecutive cases of acute appendicitis, reported incidence of 54.7% in males versus 45.3% in females with female to male ratio of 1.2:1. Our study showed a comparable sex distribution with an incidence of (58%) in males and (42%) in females with female to male ratio of 1:1.38 (table1), however, this may not presents the true incidence of the disease in the population because of the exclusion criteria.
Acute appendicitis is most common in the western population at the age (10-20) years but no age is exempt (26, 30). Our study showed a higher incidence of acute appendicitis in the age group 20-29 (54%) which represents the incidence in the adult population. A similar age incidence was reported in many studies that excluded children from the developing world (31-33), however, some studies, reported high incidence in the third decade (34).
Since the Alvarado scoring system was introduced, the accuracy and predictive values of the score in the diagnosis of acute appendicitis were intensively investigated by many researchers with very conflicting results. The accuracy (discrimination performance) of the Alvarado scoring system differs from one study to another and also differs at the different cut off points. Many studies suggested that patients with score ≤4 can be safely discharged home, those with scores 5–7, are in need of radiological investigations, and those with score >7 should be operated without further investigations (35-37).
Our study showed an accuracy of Alvarado score (discrimination performance) in ruling in acute appendicitis of 93.6% at a cut-off point of ≥ 7 which is comparable to the accuracy of 93% reported by Alvarado (11) in the same group of patients and an accuracy in ruling out acute appendicitis at cut off point of ≤ 4 of 85.7% comparable to the 85% reported by McKay Ret, et al (38) at the same cut of point. In the middle group of patients with (Alvarado score 5-6) the accuracy of the score to rule in acute appendicitis was 65%%.
Our study also showed better performance of Alvarado score in males than in females throughout the scores (table5, diagram5) which was reported in most of the published studies (39-42).
The sensitivity, specificity, PPV, and NPV of Alvarado score varies from one study to another. The wide discrepancy between the different studies is most probably due to variation in the selected cut off points for the negative and positive values. Although there is no agreeable ideal optimum cut-off point for the Alvarado score, most studies consider score ≥ 7 as an optimum cut off point (43).
Ohle Robert, et al, (42) in their systematic review and meta-analysis of validation studies that assess the Alvarado score in order to determine its performance (diagnostic accuracy at two cut- points commonly used for decision making, and calibration of the score) found that the cut-point of 5 is good at 'ruling out' admission for appendicitis (sensitivity 94% to 99%).
The discriminant analysis of Shrivastava UK et al, (44) to determine the cut-off value in an Indian set-up revealed that a cut-off value of ≥ 6 rather than the original value of ≥ 7 increases the sensitivity of the Alvarado score from 69.2% to 92%.
Our study revealed a sensitivity 77.6%, specificity of 83.3%, PPV of 93.7%, and NPV of 54% respectively at cut off point ≥ 7 and sensitivity of 97.3%, specificity of 50%, %, PPV of 86%, and NPV of 85.7% respectively at cut point ≤ 4 (Table 6, Diagram 6) which explains and confirms the differences of those variables at different cuff off points and in the different published studies.
The calculated sensitivity and specificity at the cut-off point ≥ 7 in our study (77.6%, and 83.3% 278 respectively) were comparable to the result of Ohmann et al, (12) who reported a sensitivity of 64%, and specificity of 84%. It is also comparable to the results of McKay R et al (38) who reported sensitivity for 0f 77%, and the specificity 100% at the same cut off point.
Our reported PPV of 93.7% is comparable to the PPV reported by Özsoy Z, et al (43) and Pogorelić et al (45) who reported PPV of 93.7% and 93.1% respectively at the same cut off point.
Computed tomography (CT) is considered the gold standard in the diagnosis of acute appendicitis. The impact of CT scan in improving the diagnostic accuracy in patients presenting with clinical symptoms suspicious of appendicitis was widely researched in the literature. Many studies (46, 47) documented the high sensitivity and specificity of the (CT) for the diagnosis of acute appendicitis. Some authors reported that the use of CT scan in the diagnosis of acute appendicitis has decreased the rate of negative appendectomy to less than 10 %( 48, 49).
Krajewski S, et al, (50) in their systematic review of the literature which included 28 full-text articles that examined the clinical outcomes related to the use of abdominal CT in the diagnosis of acute appendicitis reported a significant reduction of the rate of negative appendectomy( from 16.7% to 8.7%) when using CT compared with when using clinical evaluation alone.
Balthazar EJ, et al (51) evaluated the impact of CT on negative appendectomy and perforation rates in patients with the equivocal clinical presentation of acute appendicitis in their retrospective analysis of 146 consecutive patients with suspected acute appendicitis. They reported a negative appendectomy rate of 4% out of 122 patients who had an appendectomy. Unnecessary surgery was avoided in 24 patients. They concluded that the judicious use of CT imaging in patients suspected with acute appendicitis with equivocal clinical presentation led to a significant improvement in diagnosis and resulted in a decrease in the negative appendectomy rate, without increasing the perforation rate.
In our study, the combination of the Alvarado scoring system and selective CT scan in patients with equivocal clinical presentation (Alvarado score 5-6) resulted in a total of 5 negative appendectomies in 79 patients who were diagnosed to have acute appendicitis with 6.3% rate of negative appendectomy. Our result is comparable to many studies. The selective use of CT scan also saved 7 patients with an equivocal presentation from having unnecessary surgery.
McKay R, et al (38) in their retrospective review of 150 charts of patients who presented with abdominal pain documented that CT scan improves the sensitivity Alvarado scoring system in patients with an equivocal clinical presentation of appendicitis (defined by Alvarado scores of 4 to 6) from 35.6% to 90.4%. They concluded that CT scan is beneficial in patients with equivocal scores. Our study showed similar improvement of Alvarado scores by CT scan in patients with an equivocal clinical presentation of appendicitis (score 5-6) with an improvement of the PPV of the scoring system from 65% to 93.7%.
The calculated sensitivity, specificity, PPV and NPV of CT scan in our study were 100%, 87.5%, 93.7%and 100% respectively which is comparable to the reported values in many studies that reported sensitivity of 90–100%, specificity of 91–99%, accuracies of 94–98%, positive predictive values (PPVs) of 92–98%, and negative predictive values (NPVs) of 95–100% for diagnosing acute appendicitis (18, 52-54).
The overall discrimination performance of the Alvarado score and the selective CT scan in the consecutive 100 patients who presented with right iliac fossa pain of our study resulted in a total of 74 patient correctly diagnosed to have acute appendicitis who were proved to be positive both by intraoperative findings and histopathology (true positives). Negative appendectomy was performed in 5 patients (5 false positives) and 2 patient was diagnosed not to have acute appendicitis who were subsequently operated for acute appendicitis (false negative). Acute appendicitis was correctly excluded in 19 patients (true negatives), 7 patients were saved from unnecessary surgery and 77 patients were save from having unnecessary CT scan. The calculated sensitivity, specificity, PPV and NPV of Alvarado scoring system and selective CT scan at cut off point ≥ 7 were 97.3%, 79.2%, 93.6%, and 90.4% respectively in comparison to 77.6%, 83.3%, 93.6%, and 54% respectively of Alvarado scoring system without CT scan at the same cut off point, with significant improvement in the sensitivity, and the NPV without significant change of the specificity and the PPV of the score (Table 7, Diagram7).
Our clinical pathway resulted in 5 negative appendectomies, 7 patients were saved from having a negative appendectomy, and 77 patients were save from having unnecessary CT scan with its potential risk, and health authority was saved considerable time and cost. As most cases of suspected acute appendicitis are dealt with by junior surgical staff in most hospitals throughout the world, lacks an efficient clinical pathway to guide junior staff in decision making in diagnosis and management of those cases resulted in over diagnosis, miss diagnosis, and overutilization of the available resources namely ultrasound CT scan. We highly recommend adopting similarly efficient clinical pathways in emergency departments set up for the diagnosis of suspected cases of acute appendicitis especially in developing countries with limited facilities and resources.
Since the Alvarado scoring system was introduced, the accuracy and predictive values of the score in the diagnosis of acute appendicitis was intensively investigated by many researchers with conflicting results. Alvarado score has a high accuracy of ruling in and out acute appendicitis at the extremes of the score (≤7 and ≥4) however the accuracy of the score at the middle group (5 - 6) is significantly low. Although CT scan is proved to have high sensitivity and specificity in the diagnosis of acute appendicitis, CT imaging may delay the time of operation increases the risk of perforation in addition to its cost and potentially harmful radiation.
Increasing reliance and overutilization of CT scan imaging for the diagnosis of acute appendicitis should be discouraged especially in the developing world as it constitutes wasting of resources that should be reserved only for patients whose diagnoses remain uncertain.
A combination of Alvarado scoring system and selective CT limited to the patients with equivocal clinical presentation (score 5-6) improves the diagnostic accuracy of the Alvarado scoring system and limits overutilization of CT scan saving patients unnecessary exposure to radiation and health authorities’ time and cost.
We highly recommend adopting similarly efficient clinical pathways in emergency departments set up for the diagnosis of suspected cases of acute appendicitis especially in developing countries with limited facilities and resources.
Conflict of Interest: None declared
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
