AUCTORES
Globalize your Research

original article
*Corresponding Author: Jayesh Anant Mhatre, Department of Orthopaedics, Grant Government Medical College, Mumbai, Maharashtra, India.
Citation: Amit Supe, Jayesh Anant Mhatre, Kartik Pande, Niraj Tiwari (2022). A Study To Analyse Correlation Of Plate Position With Flexor Pollicis Longus Tendon Attrition In Patients Managed With Volar Plating. J. Clinical Orthopedics and Trauma Care, 4(1); DOI:10.31579/2694-0248/025
Copyright: © 2022 Jayesh Anant Mhatre, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 December 2021 | Accepted: 31 December 2021 | Published: 11 January 2022
Keywords: distal radius fracture; flexor pollicis longus tendon attrition; attritional changes; plate position
Background: Purpose of this study was to study association of flexor pollicis longus tendon (FPL) attrition using Ultrasonography with plate position on radiographs in patients managed with volar locked compression plate fixation (LCP) in distal radius fractures.
Methods: Status of flexor pollicis longus tendon was analysed by ultrasonography in patients who underwent volar locked compression plating a minimum of one year follow up. Soong’s criteria were used to assess the plate position and then correlated with the ultrasonography findings of flexor pollicis longus.
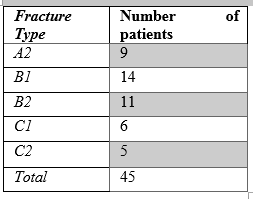
Results: There were 45 patients included in our study, of which 28 belonged to Soong’s grade zero, 10 were grades one and 7 were grade two. Flexor pollicis longus attrition was noted in 5 cases with grade two plating.
Conclusion: Amongst the cases with grade 2 of Soong’s criteria, attritional changes were seen in 72 percent of patients , which warrants a proper follow up to identify any impending signs of tendon rupture and to make early intervention to prevent rupture.
Distal end radius fractures are one of the commonest fractures treated by surgeons and accounts for 2.5% of all cases presenting at the emergency room [1]. Treatment options for these fractures range from conservative management with cast, percutaneous k wire fixation, external fixator and open reduction and internal fixation with various of plates available [2]. The appropriate treatment depends on fracture patterns with associated soft tissue condition, age other variables like fracture comminution, pattern, and displacement type [3]. The volar locked compression plate (LCP) has gained popularity in the recently and is used in commonly among of the fracture pattern. This method enables good functional results with better fragment stability and lesser complication rates and early mobilisation when compared to other procedures. Sometimes the volar locked compression plating maybe associated with complications like infection, stiffness and rarely tendon ruptures or attrition due to very distal plate position which may irritate these tendons [4, 5].
Among these complications, rupture of the flexor is a rare but serious complication. The flexor pollicis longus (FPL) is the most frequently ruptured tendon, followed by the index flexor digitorum profundus. Symptoms and signs of FPL attrition or rupture include pain and a rubbing sensation with movement, sometimes preceded by volar radial-sided wrist pain, volar wrist swelling, a popping or clicking sensation, and even an inability to flex the interphalangeal joint of the affected phalanx [6, 7]. In view of the above problems, we should strive to identify the risk factors for tendon attrition or rupture and to intervene accordingly. The pathogenesis of FPL attrition or rupture after volar plating of distal radius fractures is multifactorial [8]. Reported risk factors include excessive distal placement of the plate, increased prominence of the distal edge of the plate, prominent screw heads, inbuilt malreduction, and incorrect plate usage. However, no studies have included the use of multiple regression analysis to explore the aforementioned possible factors [9, 10]. In the present study, binomial analysis combined with multivariate logistic regression analysis was performed to investigate the risk factors associated with FPL attrition or rupture. Based on previous studies by other research groups, we hypothesized that the type of plate used, the fracture reduction status, the plate position, whether the pronator quadratus is repaired, and the time of plate removal are significant risk factors associated with FPL attrition or rupture. The flexor tendon attrition and ruptures appear to be related to inappropriate plate position, where crossing the water shed line may increase the possibility of tendon irritation [11]. This study was undertaken to look for flexor pollicis longus (FPL) tendon attrition or rupture by ultrasonography (USG) and correlate the same with radiographs for plate position following volar locked compression plating in patients who had undergone PQ repair for distal radius fractures. We also noted the status of PQ repair. The objective was to know whether the information provided by the USG would be useful to a surgeon for deciding early plate removal.
We retrospectively reviewed the records of 45 consecutive patients who had underwent surgical repair involving volar plating from January 2020 to June 2021 at our hospital. Informed consent was explained and then obtained from all patients before the operation. The inclusion criteria were
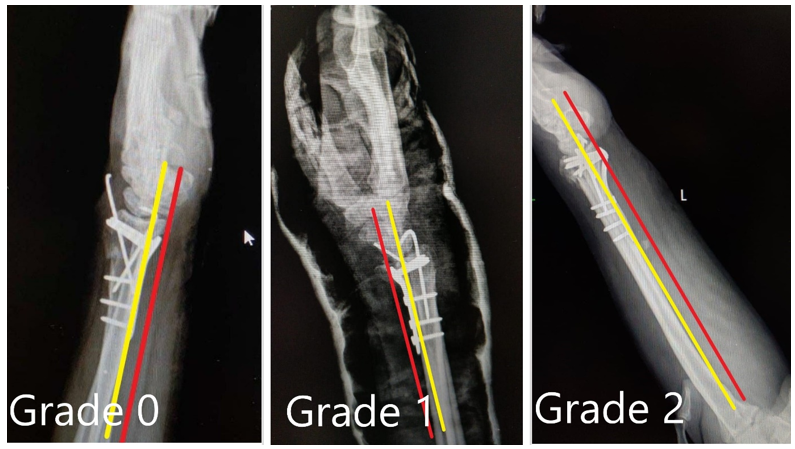
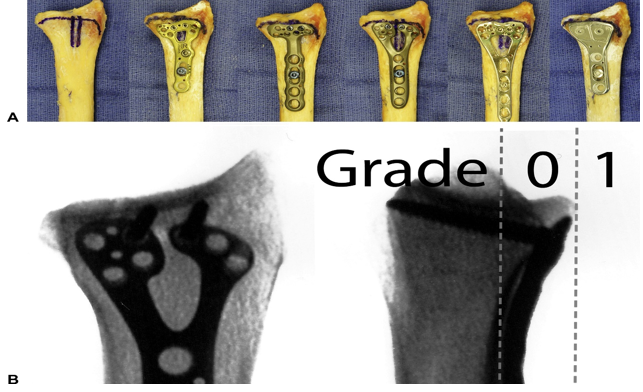
All patients were regularly followed up at 6 weeks, 3 months, 6 months and up to a period of minimum of one year after the distal radius fracture fixation and observed for fracture healing and clinical improvement (12–36 months with mean follow up of 18 months). At the end of one year follow up, standard posterior-anterior and lateral radiographs were taken to assess the plate position according to the Soong’s criteria [12, 13]. The true lateral radiograph was taken with forearm in midprone position and wrist in neutral position such that on drawing a straight line, axes of radius, lunate, capitate and third metacarpal all are in same line or within 10 degrees coaxial. On a true lateral radiograph of wrist, a "critical line" was drawn tangential to the most volar extent of the volar rim, parallel to the volar cortical bone of the radial shaft. Plates that did not extend volar to the critical line were recorded as Grade 0. Plates volar to the line but proximal to the rim (such that the recess of the pronator fossa could be clearly visualized) were recorded as Grade 1. Plates directly on or beyond the rim were recorded as Grade 2 (Fig.1 and 2). The patients then underwent an ultrasound examination. Each patient was seated with the elbow flexed, the forearm supinated, and the shoulder in neutral position for ultrasound examination. Ultrasonography (USG) was done by a dedicated musculoskeletal radiologist to look for any attritional changes like thinning of tendon, fibrillation changes, intra-tendinous changes and complete or incomplete tears in the FPL tendon. The status of PQ repair (1) age of 18 years upto 70 years, (2) closed distal radius fracture (at the time of presentation), (3) no nerve/vascular/tendon injuries, (4) treatment with open reduction and internal fixation with volar plating, and (5) available initial and post-reduction standard posteroanterior and lateral wrist radiographs. The exclusion criteria were (1) open fractures, (2) old malunited fractures, (3) pathological fractures, (4) ipsilateral upper limb fractures and/or dislocation.
Demographic information was recorded at the time of the original injury included age, sex, fracture side, mechanism of injury, fracture classification, time from injury to surgery, operative approach, type of plate, fracture reduction status, plate position, repair of pronator quadratus, and timing of plate removal. The fractures were classified using the OTA fracture classification system (type A, B, and C). Operative approaches included the modified Henry approach. Volar tilt, radial tilt, radial height, and ulnar variance were measured to determine the status of fracture reduction. We measured the Soong grade for each patient according to the methods described by Soong et al.
was also noted. The atrophic changes in FPL tendons on the operated side was detected by measuring their thickness at the level of volar lip of distal end of radius and comparing them with the contralateral side. Attritional changes were defined by the presence of thinning of the tendon, fibrillation changes, focal changes within the tendon substance or rupture of the FPL tendon. Usage of high frequency transducer ensured us in identifying the millimetric difference in the thicknesses of the tendons.
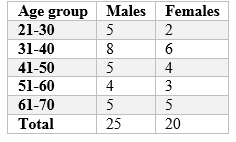
There were 45 patients with a minimum of one year follow up following volar plating for distal radius fracture with PQ repair included in the study. There were 25 male and 20 female patients, with a mean age of 46.50 years (range 20–71 years). 30 patients had right wrist involvement while 15 had injury on the left wrist. 35 patients were right hand dominant and 1o were left hand dominant. Soong’s criteria for plate position is shown in Fig.1 and 2. As per this criteria, 28 patients belonged to grade 0 (22 extraarticular fractures, 6 partial -articular fractures), 10 patients belonged to grade 1 (3 extra-articular fractures, 6 partial articular fractures, one complete articular fracture) and seven patients belonged to grade 2 (2 partial-articular fractures, 5 complete articular fractures).


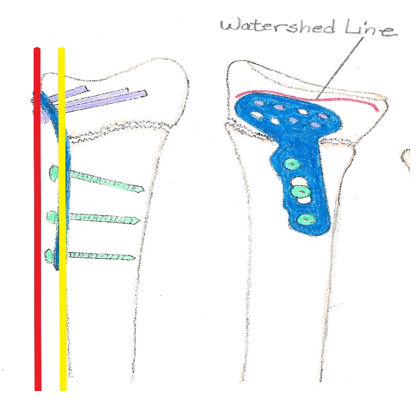
Since its inception in 2000, volar fixed-angle fixation method has provided an effective alternative for the management of dorsal and volar fractures, it is used because fixed-angle plates eliminate the need to place the implant on the unstable side of the fracture; therefore, the more physiologic and less damaging to the soft tissue, volar approach can be used to treat the majority of fractures [14, 15]. This approach is less damaging to the tendons as there is more space available on the volar aspect of the radius. Flexor tendons are located away from the volar surface of the radius, and the extensor tendons run directly on the dorsal surface of the bone. The volar approach allows the use of a thicker, stronger profile of the implant to better resist the loads applied during functional rehabilitation. Furthermore, modifications of volar fixed-angle fixation were based on insights into the anatomy of the radius, biomechanics, and blood supply [16, 17]. Until recently, volar reduction and internal fixation of dorsally displaced distal radius fractures was avoided as it was not believed possible. Initial attempts to achieve volar fixation of dorsal fractures were successful, leading to the extended flexor carpi radialis (FCR) volar approach that allows volar management of complex dorsally displaced distal radius fractures or their malunions [18]. The most fascinating anatomic feature of the volar aspect of the distal radius is the lack of flexor tendon-bone intimacy. Implant fixation on the volar aspect of the distal radius is also beneficial because its surface, except at the very distal margin, is flat in the transverse plane. This feature allows the accurate restoration of rotational alignment. The volar radius also presents a concave profile in the sagittal plane (the pronator fossa). This feature is limited distally by a ridge called the watershed line and allows the application of implants of substantial profile. The gliding surface of the flexor tendons should not come in contact with the plate as long as the implant is nested in the pronator fossa, does not cross its distal boundary, or project above it (Fig 1 and 2). The watershed line used as a surgical landmark because it is easily palpable as a bony prominence through the fibrous tissue that covers it, especially over the most ulnar aspect (volar rim of lunate fossa) where it is very close (2 mm) to the joint line. The radial aspect of the watershed line is proximal (10–15 mm) to the joint line as it courses along the base of the styloid process [18, 19]. The volar wrist capsule and ligaments insert distal to the watershed line, and the most distal edge of the pronator quadratus muscle is located several millimetres proximal [19]. Volar exposure of dorsal fractures is enhanced by releasing the radial septum (distal FCR tendon sheath, intermuscular septum, first extensor compartment, and brachioradialis). Distal release of the dorsal and volar aspects of the FCR sheath, usually distal to the superficial radial artery and scaphoid tuberosity, locates the fracture site in a more central position on the surgical approach and greatly facilitates reduction. The sheath of the first dorsal compartment must be opened on its proximal aspect to retract the abductor pollicis longus (APL) and identify the insertion of the brachioradialis into the radial styloid. Releasing this tendon eliminates the major deforming force on the radial column. A step cut tenotomy facilitates the tendon’s subsequent repair and create an anchoring point for suturing the pronator quadratus muscle over the plate. Mobilizing the proximal radial fragment into pronation provides the exposure necessary to access the dorsal and articular aspects of the fracture. Exposure through the fracture plane (intrafocal exposure) allows easy debridement of fracture hematoma or interposed callus and allows reduction of complex dorsally displaced distal radius fractures. Direct observation of the reduced surface is not possible through a volar approach [19]. Assessment of fracture reduction must be achieved with fluoroscopy. Perfusion of the distal fragment occurs mainly through a dorsal vascular retinaculum that remains undisturbed during a volar approach. Perfusion to the proximal fragment occurs through branches of the anterior interosseous artery that lay on the interosseous membrane and must be protected. All main articular fracture fragments are stabilized by volar fixed-angle fixation. Posteromedial (dorsoulnar) fragments are fixed by the most ulnar pegs on the plate’s proximal row, anteromedial fragments by the volar buttressing surface and the ulnar pegs on the distal row, and radial styloid fragments by the most radial pegs on both rows. Another indication for volar fixed-angle plating is the correction of established deformity. Changes in the osseous architecture of dorsal malunited fractures affect the mechanics of the radiocarpal joint, the distal radioulnar joint (DRUJ), and the forearm axis. Several investigators have advocated early surgical management of this problem to prevent degenerative changes and reduce rehabilitation time.
The clinical importance of an adequate reduction has been stressed, and laboratory studies have shown that optimal restoration of normal volar tilt of the distal radius is crucial to prevent increased contact forces in the radiocarpal and radioulnar joints. Biomechanical studies comparing volar fixed-angle fixation plates with conventional dorsal implants report volar fixed-angle fixation plates are stronger.
Rupture or attrition of flexor tendon has been noted after volar plate fixation for distal radius fractures. Soong et al. graded the plate position on lateral radiographs and found that Soong grade 2, which is prominence of the plate above the critical line was associated with a higher risk of tendon rupture due to repeated friction of the tendon over the prominent plate. Nanno et al., using the dynamic ultrasound did the evaluation of the FPL tendon in 25 patients following volar plating of distal radius fracture evaluated the dynamic FPL movement 1 month before the plate removal and 1 month after the plate removal [20]. In their study, they showed that dynamic USG can be very useful detecting early tendon attrition of FPL by identifying the friction between the FPL tendon and plate margin. Similarly, Tanaka et al. evaluated 40 patients following distal radius volar plate fixation with mean follow up of 12 months with ultrasonic Doppler study and established different wave forms and their association with tendon attrition. They concluded that the presence of a spiked waveform would be more likely to have FPL tendon attrition[21]. However Lutsk et al. found that most of the patients who needed to undergo plate removal had Soong grade 1 prominence which theoretically had lesser possibility of tendon attrition due to proper placement of plate. They concluded that Soong grading was not correlated with the need for plate removal, even though it is recommended by many hand surgeons to prevent FPL tendon rupture in patients suspected to be at risk [22]. In our study we have noticed that all patients with grade 2 Soong had associated FPL attrition with or without PQ atrophy and two patients had partial FPL rupture, they were managed with implant removal and further physiotherapy was started to restore the function and strength. Even though it is desirable to use the volar locked compression plate in grade 0 or grade 1 position, the placement at times is determined by the fracture pattern as juxta-articular fractures may require a very distal plate placement. Dedicated rim plates or hook plates may not be available always and are more expensive. It can also occur due to placement of the plate very distal making the plate proud leading to tendon attrition. Hence, the fracture patterns may not always correlate with the position of plate. Repairing the pronator quadratus theoretically protects the flexor tendons against the volar plate and sharp edges of the screw heads and serves as a dynamic stabilizer of the distal radioulnar joint. However, PQ repair may not be optimal at all times. The repair itself might not always reach up to the distal most edge of the plate [23, 24]. In high energy fractures, the PQ is often seen damaged badly and the repair becomes difficult in these cases owing to friability of the torn muscle fibres [25, 26]. In our study, all patients had undergone distal radius volar plate fixation. At one year follow up, 28 patients out of 45 patients had no FPL atrophy and 10 patients had positive findings on usg in spectrum of thinning of tendon, fibrillation changes, intra-tendinous changes and complete or incomplete tears in the FPL tendon and clinically 7 patients had symptomatic tenosynovitis (swelling and pain), no patient had complete tear and the two patients with partial tear on one year follow up had radiological sings of union and thus were managed with implant removal and then later physiotherapy was started , strength improved and symptoms subsided in 1 month post second surgery.
In our study, all patients had undergone open reduction and internal fixation with volar plating for distal radius fracture. At one year follow up, all patients even though showed intact FPL, 10 patients out of 45 patients had some of the FPL changes on USG. We did have significant relation between the plate position and FPL atrophy, leading to implant removal in 20 percent of the total symptomatic patients(n=10) at one year duration and hence meticulous placement of the plate becomes important for reducing attrition of the tendon post-surgery . Based on our results we recommend that if the plate has to be positioned very distally then the patients are to be followed up regularly with a dynamic USG examination and any early signs of FPL attrition should be noted. Early implant removal can be advocated in these patients once the fracture shows union to prevent tendon rupture. From our study we conclude that the plate position has greater influence on FPL tendon following distal radius fracture fixation.
Funding:nil
Conflict of interest: nil
Informed consent Written informed consent was obtained from the patient (s) for their anonymized information to be published in this article along with their surgical consent.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
