AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Kehinde Adebola Atoloye, University of Ibadan, Ibadan, Nigeria.
Citation: Kehinde A. Atoloye, Temitayo V. Lawal, Ayo S. Adebowale, Adeniyi F. Fagbamigbe, (2023), A Spatio-temporal mapping and Bayesian modelling of fever, cough and short rapid breaths, as symptoms of pneumonia in under-five children in Nigeria, International Journal of Clinical Case Reports and Reviews, 14(2); DOI:10.31579/2690-4861/321
Copyright: © 2023, Kehinde Adebola Atoloye. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 June 2023 | Accepted: 07 July 2023 | Published: 17 July 2023
Keywords: pneumonia symptoms; under-five children; cough; fever; short rapid breadth; Nigeria
Background
Pneumonia remains a public health challenge in most parts of the world, with Nigeria having the highest number of pneumonia-related deaths. Understanding the geographical distribution, trends and risk factors associated with some symptoms of pneumonia can aid an appropriate preventive intervention towards abating its burden in Nigeria.
Method
This cross-sectional study used data from the 2008, 2013, and 2018 Nigeria Demographic Health Surveys. The outcome variables include fever, cough, and short, rapid breaths as selected symptoms of pneumonia. Optimized hotspot analysis was used to identify areas with a significantly high prevalence of fever, cough, and short rapid breaths, and a MCMC random-intercept logistic regression model was fitted to each symptom.
Results
The prevalence of cough was 12.1%, 10.1% and 16.9% in 2008, 2013 and 2018 respectively, 16.2%, 13.3%, and 25.7% for fever; and 41.7%, 42.5% and 6.5% for short rapid breaths respectively with variations across the states. Children aged 6-11 months had the highest higher odds (adjusted odds ratio (aOR) =1.95, 95% Credible Interval (CrI): 1.77, 2.18) of having cough, compared to children of other age groups. Similar pattern was noticed for fever and short rapid breaths. Other significantly associated factors with symptoms include the mother’s education, mother’s age, residence type, housing quality, wealth index and region.
Conclusion
The northern states were more characterized by short, rapid breaths while the southern states were more characterized by fever but both regions have a fair share of cough among under-five children. For cough and fever symptoms, the increased prevalence between 2013 and 2018 indicates more attention is needed. There are also higher odds of finding the symptoms amongst children aged 6-11 months compared to children of other age groups, especially in the North-eastern part of the country. Hence, government needs to strengthen immunization against diseases such as Hib, pneumococcus, measles and whooping cough (pertussis) which has been shown to be the most effective way to prevent pneumonia. Adequate nutrition is also key to improving children's natural defenses. Educated mothers needs to be adequately sensitized to understand that exclusive breastfeeding for the first 6 months of life of a child is paramount.
Pneumonia is an acute respiratory infection in one or both lungs, characterized by cough, fever, shortness of breath, shallow breathing, low energy, etc. [1]. On an annual basis, the disease has accounted for over ten million hospital admissions and more than a million deaths among under-five children globally [2,3]. In 2017, pneumonia was identified as the 4th leading cause of mortality and may eventually become the 3rd by 2024 [4]. According to the World Health Organization (WHO), pneumonia accounts for about 14% of the disease burden globally [2]. The Sustainable Development Goals (SDGs) aim to reduce the global burden of pneumonia by 2030 through universal access to vaccination, improved healthcare, and early detection and treatment of the disease [17].
In Africa, pneumonia is a potentially life-threatening ailment [2,5,6]. It is not just a major causal factor of mortality and morbidity, but it is as well associated with a non-negligible burden on healthcare infrastructures [7,8] and incomes of households [9]. Oftentimes, pneumonia involves several pathogens that are transmissible among individuals. Analyses have identified various pneumonia results to be temporally seasonal [10,11]. Paynter et al. found that admissions based on pneumonia are clustered spatially on a high level aided by contact with infected individuals [12].
WHO estimated 868,000 deaths as a result of pneumonia in 2010 with 140,000 deaths on an annual basis among under-five children, the highest in Africa [13]. In Nigeria, pneumonia is one of the leading communicable diseases. Nigeria is one of the countries with the highest burden of pneumonia in childhood and accounts for 162,000 pneumonia-related deaths worldwide in 2018, constituting 20.2% of global deaths [14]. The prevalence of pneumonia in a study conducted in Nigeria in 2013 was 13.3% and 23.9% in another study in 2015 [15,16]. This high prevalence may attract poor health outcomes within the population if unchecked. Therefore, it is of utmost importance to abate the prevalence of pneumonia in Nigeria to ensure not just healthy living in children but for the future national sustainability as emphasized in the Sustainable Development Goal (SDG)-3, to “Ensure healthy lives and promote well-being for all and sundry and to bring to an end, avoidable deaths of under-five children with all countries aiming to abate neonatal deaths to as low as 12 per 1 000 live births and under-5 deaths to as low as 25 per 1 000 live births’ by 2030” [17]. In a situation where actual pneumonia diagnostic data of under-five children are sparse, understanding factors associated with some of the symptoms of pneumonia may help to design some form of intervention based on the demographics and other factors that may be found to associate with some of the symptoms of pneumonia. Fever, Short Rapid Breaths and Cough are the symptoms of focus in this study.
Several factors have been identified as risk factors for childhood pneumonia, ranging from indoor air pollution due to biomass, outdoor air pollution as a result of vehicular emission and many other factors [18,19]. Previous studies have also documented that the air intake from polluting fuel is an influential risk factor for acute respiratory infection among under-five children in developing countries [20–27].
Other studies have shown that some socioeconomic characteristics like maternal education, region of residence, and household wealth status are important precursors to the risk factors for pneumonia symptoms among children [28–33]. Moreover, studies have also demonstrated that rural-urban residence [34], maternal age at the child’s birth and the child’s birth order (Mishra, 2003) and water and sanitation facilities [35] are other risk factors for child pneumonia.
Concurrent assessment of the geographical distribution, trends and risk factors associated with symptoms of pneumonia remains a grey area for research in Nigeria. Understanding the spatial-temporal distribution, trends and risk factors associated with fever, short rapid breaths and cough as some of the symptoms of pneumonia, can help to prevent pneumonia and subsequently reduce its prevalence and attendant burden. Therefore, this study attempts to identify significant factors associated with each of cough, fever and short rapid breaths as symptoms of pneumonia and to understand the odds of contracting these symptoms with respect to each significant factor identified. It also examines the pattern of distribution of the prevalence of these symptoms across the 36 states of Nigeria over three DHS survey years, that is, 2008, 2013, and 2018.
Study Area
This study was conducted in Nigeria - a West African country with an estimated population of about 215 million. Nigeria consists of six (6) geo-political zones (North-Central, North-East, North-West, South-East, South-South and South-West), which are further divided into 36 states and the Federal Capital Territory (FCT), where each state consists of a third-tier local government and wards. Temperature and humidity are fairly constant all-round year in the south, while the seasons vary considerably in the north. Nigeria’s climate is relatively hot and is usually classified into two seasons, dry and wet. The dry season runs from November to March, whereas, the wet season begins in April and ends in October. These seasons come with the symptoms of pneumonia depending on individuals’ susceptibility, adaptation, and body reactions to changes in environmental conditions.
The data used in this study were nationally representative and based on the Nigeria Demographic Health Survey (NDHS) conducted in 2008, 2013 and 2018. In the surveys, the unit of inquiry was women of reproductive age (15 to 49 years). They were asked questions regarding their reproductive health, births and children alongside other related topics. The sampling of the respondents during the survey was based on a 2-stage stratified cluster design (National Population Commission [Nigeria] and ICF International, 2014). Data were collected from all eligible women in selected households with the aid of a pretested questionnaire by trained interviewers. Data collected from women about their under-five children were specially processed to constitute the children recode file which was utilized for analysis in this study. A detailed explanation of the field processes has been reported elsewhere [39–41].
Outcome Variables
The outcomes/dependent variables for this study are fever, cough, and short and rapid breaths as symptoms of pneumonia. Each of these symptoms as outcomes of interest are measured as 1=Has symptom in 2 weeks preceding survey and 0=Has no symptom in 2 weeks preceding the survey.
Explanatory Variables
Based on existing literature, the explanatory variables were grouped into children, maternal and household characteristics.
Children's characteristics: These include current age (in months) and sex.
Maternal Characteristics: These include mother’s age and mother’s education.
Household characteristics: These included cooking fuel (clean/unclean), drinking water source (improved or unimproved), housing material (improved or unimproved) and toilet facility (improved or unimproved). Clean fuel includes electricity, and liquefied natural gas/biogas and unclean fuel include wood, charcoal, kerosene, straw shrubs, animal dung and grass. The improved sources of drinking water include a protected well, borehole, bottled water and spring rainwater. The unimproved includes a spring tanker, unprotected well with drum, sachet water, surface water, and other sources. The housing material quality derivation was based on a composite score of the type of wall, floor and roof materials. If cement/carpet/rug/ceramic tiles/vinyl asphalt strips were used for the floor, the floor quality is coded 1 else it is coded 0. In the same vein, wall material quality is coded 1 is made of cement blocks/bricks else 0. If the roof material is made of calamine/cement roofing shingles/cement fibers/ceramic tiles/zinc, it is coded 1 else 0. Categories of the housing material were further aggregated and coded as poor (1), average (2) and good (3). For toilet facilities, it was coded as improved or unimproved depending on the type of toilet facility used. Household wealth quintile, place of residence, and geopolitical zone are as well included.
The outcome and explanatory variables are conceptualized in Figure 1 below:
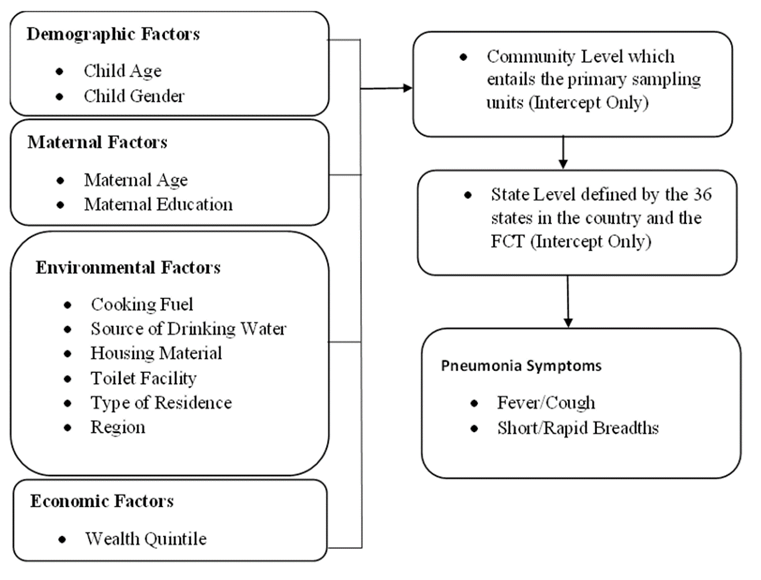
Figure 1: Conceptual Framework
Descriptive statistics, Bayesian MCMC logistic regression and spatial hotspot analyses were used in this study. The spatial variation of the prevalence of the symptoms of pneumonia was analysed using the Optimized Hotspot Analysis. It entails the creation of maps of statistically significant hot and cold spots using the Getis-Ord Gi* statistic employing incident points or weighted features (points or polygons). It evaluates the characteristics of the input feature class to produce optimal results. Optimized Hotspot analysis uses the Getis-Ord Gi* statistic using a fixed distance band in ArcGIS software [42].
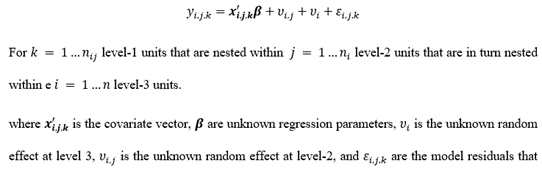
The Bayesian MCMC logistic regression model is as specified below:
that follow a logistic distribution. The model is a random-intercept mixed-effect model. Level 1 is fixed and consists of fixed effect predictors while levels 2 and 3 are the random effect levels defined by the group-level variables. Level 2 group level is defined by the community groups/cluster group variable while the level 3 group is defined by the state group variable. No group-level predictor is involved as interest is more of the amount of variation contributed by the group-level variables. The absence of group-level predictors makes the model a random-intercept mixed model.
In fitting the MCMC model, parameters specified in the brms package in R included 4 chains, 4 cores, 4 threads, 50,000 iterations and a thinning rate of 50. A weakly informative prior, derived from the sample was also used.
Distribution of Pneumonia Symptoms and the Demographic Characteristics of the Children and their mothers.
Distribution of Cough
Table 1 shows the prevalence of cough between 2008 and 2013. The prevalence of cough is highest in 2018 (16.9%) and lowest in 2013 (10.1%). Across the survey years, the prevalence of cough was consistently highest among children aged 6 to 11 months and least among children whose mothers are has no formal education where the prevalence was 9.9%, 7.6%, and 14.7% in 2008, 2013, and 2018 survey year respectively.
| 2008 | 2013 | 2018 | |
|---|---|---|---|
| (N=22139) | (N=26076) | (N=11375) | |
| n (%) | n (%) | n (%) | |
| Total | 2673 (12.1) | 2630 (10.1) | 1921 (16.9) |
| Characteristics | |||
| Sex of Child | 2.71 | 0.887 | 0.052 |
| Male | 1319 (11.7) | 1350 (10.3) | 968 (16.8) |
| Female | 1354 (12.4) | 1280 (9.9) | 953 (17.0) |
| Child Age (In Months) | 147.532* | 268.016* | 92.017* |
| 0-5 | 257 (9.7) | 205 (7.3) | 164 (13.6) |
| 6-11 | 399 (15.5) | 429 (14.1) | 271 (22.0) |
| 12-23 | 684 (15.3) | 763 (14.1) | 496 (20.8) |
| 24-35 | 553 (13.4) | 513 (10.5) | 360 (16.5) |
| 36-47 | 424 (9.7) | 407 (8.0) | 362 (16.6) |
| 48-59 | 356 (9.0) | 313 (6.5) | 268 (12.3) |
| Maternal Age | 11.237 | 19.614* | 17.875* |
| 15-19 | 158 (13.4) | 140 (11.3) | 69 (15.3) |
| 20-24 | 524 (12.3) | 566 (11.3) | 388 (19.2) |
| 25-29 | 793 (12.5) | 718 (9.8) | 580 (17.9) |
| 30-34 | 587 (12.3) | 589 (10.2) | 414 (15.6) |
| 35-39 | 370 (11.2) | 383 (9.3) | 302 (15.6) |
| 40-44 | 174 (11.0) | 166 (8.5) | 118 (15.2) |
| 45-49 | 67 (9.7) | 68 (9.4) | 50 (17.0) |
| Maternal Education | 99.797* | 170.411* | 29.459* |
| No Education | 1063 (9.9) | 935 (7.6) | 646 (14.7) |
| Primary | 702 (13.5) | 622 (11.5) | 375 (19.8) |
| Secondary | 765 (15.0) | 888 (13.0) | 725 (17.9) |
| Higher | 143 (12.6) | 185 (12.2) | 175 (16.8) |
| Source of Drinking Water | 0.008 | 0.019 | 1.283 |
| Improved | 1372 (12.1) | 1561 (10.1) | 1153 (16.6) |
| Unimproved | 1301 (12.1) | 1069 (10.1) | 768 (17.4) |
| Cooking Fuel Type | 23.816* | 1.991 | 2.481 |
| Clean | 466 (14.7) | 451 (10.7) | 361 (15.8) |
| Unclean | 2207 (11.6) | 2179 (10.0) | 1560 (17.2) |
| Toilet Facility | 0.406 | 0.441 | 2.21 |
| Improved | 1295 (12.2) | 1268 (10.0) | 1049 (17.4) |
| Unimproved | 1378 (11.9) | 1362 (10.2) | 872 (16.3) |
| Housing Quality Material | 30.726* | 5.101 | 14.678 |
| Poor | 1084 (10.8) | 1087 (9.9) | 539 (19.2) |
| Average | 374 (12.2) | 392 (9.4) | 326 (16.7) |
| Good | 1215 (13.4) | 1151 (10.5) | 1056 (16.0) |
| Place of Residence | 2.361 | 8.192* | 0.701 |
| Urban | 783 (12.6) | 921 (10.9) | 733 (16.5) |
| Rural | 1890 (11.9) | 1709 (9.7) | 1188 (17.1) |
| Wealth Index | 36.247* | 29.890* | 13.817 |
| Poorest | 596 (10.9) | 498 (8.4) | 434 (19.2) |
| Poorer | 560 (10.7) | 614 (10.1) | 362 (15.9) |
| Middle | 544 (12.6) | 605 (11.3) | 419 (16.7) |
| Richer | 537 (13.8) | 489 (10.1) | 408 (17.2) |
| Richest | 436 (13.6) | 424 (11.0) | 298 (15.3) |
| Region | 567.619* | 745.567* | 337.491 |
| North Central | 353 (8.4) | 324 (8.2) | 307 (15.3) |
| North East | 817 (15.5) | 914 (16.7) | 544 (26.7) |
| North West | 346 (6.3) | 362 (4.4) | 304 (10.9) |
| South East | 408 (20.5) | 364 (15.5) | 298 (18.6) |
| South South | 477 (19.8) | 449 (14.5) | 310 (24.7) |
| South West | 272 (9.7) | 217 (7.4) | 158 (9.5) |
Table 1: Prevalence of Cough by Selected Demographic Characteristics, per Year
*Chi-square values significant at 95% Confidence Interval.
Distribution of Fever
Table 2 also shows that the prevalence of fever dipped between 2008 and 2013, from 16.2% to 13.3% and rose to 25.8% in 2018. Across the survey years, the data show that children in the age group 12-23 months mostly experienced fever more than their counterparts in the other age group while the least prevalence was found among those aged 0 to 5 months. The data further depict that in each survey year, fever’s prevalence was persistently higher in children living in households where their source of drinking water was unimproved and those who used unclean fuel. Urban residents also had a lower prevalence of fever in under-five children compared to the rural residents and this pattern was observed across the survey rounds.
| 2008 | 2013 | 2018 | |
|---|---|---|---|
| (N=22164) | (N=26116) | (N=11374) | |
| n (%) | n (%) | n (%) | |
| Total | 3590 (16.2) | 3483 (13.3) | 2925 (25.8) |
| Characteristics | |||
| Sex of Child | 4.123* | 2.792 | 0.111 |
| Male | 1880 (16.7) | 1803 (13.7) | 1473 (25.6) |
| Female | 1710 (15.7) | 1680 (13.0) | 1452 (25.9) |
| Child Age (In Months) | 236.131* | 338.382* | 149.025* |
| 0-5 | 247 (9.3) | 212 (7.5) | 177 (14.7) |
| 6-11 | 514 (19.9) | 541 (17.8) | 372 (30.2) |
| 12-23 | 938 (20.9) | 996 (18.4) | 757 (31.8) |
| 24-35 | 743 (18.0) | 702 (14.3) | 582 (26.6) |
| 36-47 | 625 (14.3) | 575 (11.3) | 547 (25.0) |
| 48-59 | 523 (13.3) | 457 (9.5) | 490 (22.4) |
| Maternal Age | 10.013 | 8.509 | 9.537 |
| 15-19 | 221 (18.7) | 180 (14.5) | 127 (28.2) |
| 20-24 | 701 (16.5) | 699 (14.0) | 561 (27.8) |
| 25-29 | 981 (15.4) | 985 (13.5) | 809 (24.9) |
| 30-34 | 759 (15.9) | 739 (12.8) | 652 (24.5) |
| 35-39 | 547 (16.6) | 513 (12.5) | 504 (26.0) |
| 40-44 | 262 (16.5) | 261 (13.4) | 201 (26.0) |
| 45-49 | 119 (17.1) | 106 (14.6) | 71 (24.1) |
| Maternal Education | 3.41 | 5.552 | 156.361* |
| No Education | 1747 (16.3) | 1659 (13.4) | 1379 (31.4) |
| Primary | 859 (16.5) | 749 (13.9) | 503 (26.6) |
| Secondary | 822 (16.1) | 899 (13.2) | 864 (21.3) |
| Higher | 162 (14.3) | 176 (11.6) | 179 (17.1) |
| Source of Drinking Water | 19.767* | 4.590* | 10.145* |
| Improved | 1717 (15.1) | 2004 (13.0) | 1717 (24.7) |
| Unimproved | 1873 (17.3) | 1479 (13.9) | 1208 (27.4) |
| Cooking Fuel Type | 7.640* | 65.805* | 151.739* |
| Clean | 461 (14.5) | 399 (9.5) | 358 (15.7) |
| Unclean | 3129 (16.5) | 3084 (14.1) | 2567 (28.2) |
| Toilet Facility | 6.048* | 0.778 | 55.942* |
| Improved | 1651 (15.6) | 1677 (13.1) | 1378 (22.8) |
| Unimproved | 1939 (16.8) | 1806 (13.5) | 1547 (29.0) |
| Housing Quality Material | 16.895* | 56.614* | 197.277* |
| Poor | 1737 (17.3) | 1671 (15.2) | 946 (33.7) |
| Average | 477 (15.5) | 512 (12.3) | 596 (30.6) |
| Good | 1376 (15.2) | 1300 (11.9) | 1383 (20.9) |
| Place of Residence | 42.322* | 4.232* | 86.975* |
| Urban | 847 (13.6) | 1080 (12.7) | 929 (20.9) |
| Rural | 2743 (17.2) | 2403 (13.6) | 1996 (28.8) |
| Wealth Index | 31.415* | 64.975* | 261.618* |
| Poorest | 957 (17.4) | 861 (14.5) | 811 (35.8) |
| Poorer | 886 (16.9) | 883 (14.5) | 668 (29.4) |
| Middle | 721 (16.6) | 773 (14.4) | 634 (25.2) |
| Richer | 603 (15.5) | 580 (11.9) | 503 (21.2) |
| Richest | 423 (13.2) | 386 (10.0) | 309 (15.8) |
| Region | 487.378* | 740.839* | 380.292* |
| North Central | 396 (9.4) | 300 (7.6) | 412 (20.5) |
| North East | 1079 (20.5) | 1205 (22.0) | 737 (36.1) |
| North West | 847 (15.4) | 848 (10.2) | 885 (31.7) |
| South East | 514 (25.8) | 479 (20.4) | 371 (23.1) |
| South South | 498 (20.7) | 442 (14.3) | 329 (26.2) |
| South West | 256 (9.2) | 209 (7.1) | 191 (11.4) |
Table 2: Prevalence of Fever by Selected Demographic Characteristics of the Children, per Survey Year
*Chi-square value significant at 95% Confidence Interval
Distribution of Short Rapid Breaths
The prevalence of short rapid breath (SRB) among under-five children across the three survey rounds was presented in Table 3. The prevalence of SRB was highest in 2008 (41.7%) and least in 2018 (6.5%). There was a consistently high prevalence of SRB among under-five children living in households where unimproved sources of drinking water were used – the prevalence of SRB was 47.3%, 48.9%, and 7.4% in 2003, 2013, and 2018 respectively compared to households with improved sources of drinking water. SRB prevalence in under-five children was consistently higher in rural areas than in urban. In 2008 and 2013 data for instance, compared to under-five children living in the urban areas where the prevalence of SRB was 36.1% and 32.9%, about 44.0% and 47.6% were found in the rural areas respectively.
| 2008 | 2013 | 2018 | |
|---|---|---|---|
| (N=2620) | (N=2605) | (N=11376) | |
| n (%) | n (%) | n (%) | |
| Total | 1092 (41.7) | 1106 (42.5) | 741 (6.5) |
| Characteristics | |||
| Sex of Child | 0.042 | 0.06 | 0.858 |
| Male | 544 (41.9) | 572 (42.7) | 363 (6.3) |
| Female | 548 (41.5) | 534 (42.2) | 378 (6.7) |
| Child Age (In Months) | 7.212 | 12.832* | 55.812* |
| 0-5 | 107 (42.5) | 86 (42.2) | 67 (5.6) |
| 6-11 | 165 (42.3) | 190 (44.7) | 107 (8.7) |
| 12-23 | 299 (44.6) | 334 (44.3) | 206 (8.6) |
| 24-35 | 202 (37.2) | 233 (45.6) | 138 (6.3) |
| 36-47 | 177 (42.4) | 147 (36.4) | 140 (6.4) |
| 48-59 | 142 (40.8) | 116 (37.8) | 83 (3.8) |
| Maternal Age | 20.680* | 19.719* | 7.356 |
| 15-19 | 72 (47.4) | 63 (45.3) | 28 (6.2) |
| 20-24 | 254 (49.1) | 267 (47.7) | 156 (7.7) |
| 25-29 | 315 (40.8) | 290 (41.0) | 212 (6.5) |
| 30-34 | 216 (37.4) | 230 (39.2) | 169 (6.4) |
| 35-39 | 138 (38.0) | 141 (37.2) | 113 (5.8) |
| 40-44 | 69 (40.1) | 78 (47.3) | 47 (6.1) |
| 45-49 | 28 (42.4) | 37 (54.4) | 16 (5.4) |
| Maternal Education | 129.945* | 91.417* | 22.122* |
| No Education | 558 (54.0) | 495 (53.4) | 311 (7.1) |
| Primary | 272 (39.4) | 265 (43.3) | 153 (8.1) |
| Secondary | 235 (31.2) | 295 (33.5) | 231 (5.7) |
| Higher | 27 (19.0) | 51 (27.6) | 46 (4.4) |
| Source of Drinking Water | 32.737* | 29.953* | 10.361* |
| Improved | 488 (36.3) | 589 (38.1) | 412 (5.9) |
| Unimproved | 604 (47.3) | 517 (48.9) | 329 (7.4) |
| Cooking Fuel Type | 77.870* | 113.769* | 28.153* |
| Clean | 107 (23.3) | 89 (19.8) | 93 (4.1) |
| Unclean | 985 (45.6) | 1017 (47.2) | 648 (7.1) |
| Toilet Facility | 17.827* | 15.629* | 0.723 |
| Improved | 474 (37.5) | 483 (38.5) | 382 (6.3) |
| Unimproved | 618 (45.6) | 623 (46.1) | 359 (6.7) |
| Housing Quality Material | 123.180* | 111.767* | 56.336* |
| Poor | 560 (52.6) | 557 (51.8) | 255 (9.1) |
| Average | 173 (47.5) | 196 (50.8) | 149 (7.6) |
| Good | 359 (30.1) | 353 (30.9) | 337 (5.1) |
| Place of Residence | 13.815* | 52.518* | 13.447* |
| Urban | 277 (36.1) | 300 (32.9) | 242 (5.5) |
| Rural | 815 (44.0) | 806 (47.6) | 499 (7.2) |
| Wealth Index | 141.450* | 143.625* | 57.612* |
| Poorest | 305 (52.2) | 263 (53.0) | 218 (9.6) |
| Poorer | 296 (54.0) | 321 (53.1) | 150 (6.6) |
| Middle | 226 (42.5) | 276 (46.1) | 163 (6.5) |
| Richer | 160 (30.5) | 144 (29.6) | 127 (5.4) |
| Richest | 105 (24.4) | 102 (24.3) | 83 (4.2) |
| Region | 228.194* | 270.902* | 421.444* |
| North Central | 143 (41.4) | 149 (46.6) | 78 (3.9) |
| North East | 469 (58.7) | 553 (61.2) | 323 (15.8) |
| North West | 176 (52.9) | 128 (35.9) | 104 (3.7) |
| South East | 112 (27.7) | 132 (36.5) | 102 (6.4) |
| South South | 141 (30.0) | 117 (26.2) | 106 (8.4) |
| South West | 51 (19.0) | 27 (12.5) | 28 (1.7) |
Table 3: Prevalence of Short Rapid Breaths by Selected Demographic Characteristics, per Year
*Chi-square values significant at 95% Confidence Interval
Optimized Hotspot Analysis of Prevalence of Pneumonia Symptoms
Figures 2-4 show the spatial and temporal distribution of states in Nigeria with a significantly high prevalence of pneumonia symptoms. For Cough, Figure 2 indicates a decrease in states with a significantly high prevalence of cough over time. In 2008, only Gombe has a significantly high prevalence at 90% CI while the other years has no states with significantly high prevalence. Figure 3 indicates an overall decrease in prevalence and states with a significantly high prevalence of fever over time. In 2008, Bayelsa, Rivers, Akwa Ibom, Edo, Anambra, Enugu, Ebonyi and Imo states had significantly high prevalence at 90% CI while in 2013, the south-south states had less significant prevalence which include Delta, Bayelsa and Rivers only at 90% CI. There was no state with a significantly high prevalence of fever in 2018. Figure 4 shows a decrease in the number of states with significantly high prevalence from 2008 to 2018. In 2008, Kaduna, Kano and Jigawa were the states with a significantly high prevalence of short rapid breath. In 2013 and 2018, only Yobe and Taraba has a significantly high prevalence of pneumonia symptoms respectively.

Figure 2: Significance of High Prevalence of Cough in under-five children in Nigeria, 2008-2018

Figure 3: Significance of High Prevalence of Fever in under-five children in Nigeria, 2008-2018

Figure 4: Significance of High Prevalence of Short, Rapid Breaths in under-five children in Nigeria, 2008-2018
Factors Associated with Cough, Fever and Short Rapid Breath
Table 4 presents the results of the adjusted MCMC models fitted for each of the symptoms. It is worthy of note that the factors included in these models were put through bivariate analysis to determine their independent association with the respective symptoms before they were seeded into the multiple models. The adjusted odds (while other factors are kept constant) of cough reduced by 20% (adjusted odds ratio (aOR) =0.80, 95% Credible Interval (CrI): 0.76-0.85) in 2013 but rose by 52% (aOR =1.52, 95% CrI: 1.40, 1.63) in 2018 compared with the likelihood in 2008. Similarly, the adjusted odds of fever reduced by 24% (aOR =0.76, 95% CrI: 0.72, 0.80) in 2013 and nearly doubled (aOR =1.93, 95% CrI: 1.82, 2.05) in 2018. Whereas the adjusted odds of short rapid breaths were insignificant in 2013, but reduced by 91% (aOR =0.09, 95% CrI: 0.08, 0.11) in 2018 compared with 2008.
| Cough | Fever | Short, Rapid Breaths | |
| Adjusted OR (95% CrI) | Adjusted OR (95% CrI) | Adjusted OR (95% CrI) | |
| Variables | |||
| Year | |||
| 2008 | Reference | ||
| 2013 | 0.80(0.76-0.85)* | 0.76(0.72-0.80)* | 0.96(0.84-1.11) |
| 2018 | 1.52(1.40-1.63)* | 1.93(1.82-2.05)* | 0.09(0.08-0.11)* |
| Sex of Child | |||
| Male | Reference | ||
| Female | 1.02(0.96-1.07) | 0.94(0.90-0.99)* | 1.01(0.91-1.11) |
| Child Age (months) | |||
| 0-5 | Reference | ||
| 6-11 | 1.95(1.77-2.18)* | 2.66(2.44-2.97)* | 1.35(1.11-1.67)* |
| 12-23 | 1.92(1.73-2.12)* | 2.86(2.61-3.16)* | 1.34(1.12-1.63)* |
| 24-35 | 1.45(1.31-1.62)* | 2.23(2.01-2.44)* | 1.11(0.90-1.34) |
| 36-47 | 1.15(1.03-1.27)* | 1.75(1.58-1.93)* | 1.00(0.82-1.22) |
| 48-59 | 0.93(0.84-1.04) | 1.51(1.36-1.67)* | 0.79(0.64-0.98)* |
| Mother’s Age (years) | |||
| 15-19 | Reference | ||
| 20-24 | 1.11(0.98-1.27) | 1.04(0.93-1.16) | 1.42(1.12-1.80)* |
| 25-29 | 1.02(0.90-1.15) | 1.01(0.90-1.13) | 1.16(0.92-1.46) |
| 30-34 | 1.00(0.88-1.15) | 1.02(0.91-1.15) | 1.15(0.91-1.46) |
| 35-39 | 0.95(0.84-1.08) | 1.03(0.92-1.16) | 1.05(0.82-1.36) |
| 40-44 | 0.95(0.82-1.11) | 1.07(0.93-1.22) | 1.25(0.93-1.65) |
| 45-49 | 1.06(0.87-1.30) | 1.08(0.90-1.28) | 1.19(0.82-1.72) |
| Mother’s Education | |||
| No Education | Reference | ||
| Primary | 1.39(1.28-1.52)* | 1.13(1.05-1.22)* | 1.13(0.98-1.31) |
| Secondary | 1.35(1.23-1.48)* | 1.08(1.00-1.17) | 1.01(0.87-1.20) |
| Higher | 1.32(1.15-1.51)* | 1.06(0.94-1.21) | 0.93(0.71-1.22) |
| Source of Drinking Water | |||
| Improved | Reference | ||
| Unimproved | 0.99(0.92-1.06) | 0.99(0.94-1.05) | 1.06(0.95-1.20) |
| Cooking Fuel Type | |||
| Clean | Reference | ||
| Unclean | 0.90(0.80-1.00) | 0.95(0.86-1.06) | 1.12(0.90-1.40) |
| Toilet Type | |||
| Improved | Reference | ||
| Unimproved | 0.98(0.91-1.04) | 1.02(0.96-1.08) | 0.99(0.88-1.13) |
| Housing Material Quality | |||
| Poor | Reference | ||
| Average | 0.99(0.90-1.08) | 0.97(0.90-1.05) | 0.98(0.82-1.16) |
| Good | 0.89(0.80-0.99)* | 1.01(0.92-1.11) | 0.76(0.62-0.92)* |
| Type of Place of Residence | |||
| Urban | Reference | ||
| Rural | 1.03(0.95-1.12) | 1.13(1.05-1.21)* | 0.98(0.84-1.14) |
| Wealth Index | |||
| Poorest | Reference | ||
| Poorer | 1.06(0.97-1.16) | 1.04(0.97-1.13) | 1.12(0.94-1.31) |
| Middle | 1.14(1.01-1.30)* | 1.03(0.93-1.15) | 1.14(0.91-1.42) |
| Richer | 1.14(0.99-1.31) | 0.93(0.82-1.06) | 0.90(0.68-1.19) |
| Richest | 1.09(0.91-1.31) | 0.80(0.68-0.95)* | 0.92(0.66-1.28) |
| Region | |||
| North Central | Reference | ||
| North East | 2.64(1.62-4.10)* | 2.80(1.80-4.53)* | 3.16(2.12-4.81)* |
| North West | 0.76(0.49-1.22) | 1.63(1.06-2.51)* | 1.05(0.70-1.62) |
| South East | 1.93(1.17-3.16)* | 2.20(1.35-3.53)* | 1.22(0.77-1.92) |
| South South | 1.97(1.25-3.19)* | 1.73(1.09-2.75)* | 1.13(0.73-1.77) |
| South West | 0.85(0.52-1.35) | 0.83(0.51-1.31) | 0.43(0.27-0.67)* |
| Random Effects (Intercepts) | |||
| Neighbourhood Level | |||
| Variance (CrI 95%) | 0.23(0.43-0.52)* | 0.21(0.42-0.50)* | 0.37(0.53-0.69)* |
| % Variation Explained (CrI 95%) | 0.06(0.03-0.10)* | 0.04(0.02-0.07)* | 0.03(-0.01-0.06)* |
| State Level | |||
| Variance (CrI 95%) | 0.17(0.31-0.55)* | 0.16(0.31-0.53)* | 0.10(0.22-0.47)* |
| % Variation Explained (CrI 95%) | 0.03(-0.09-0.14)* | 0.03(-0.06-0.13)* | 0.01(-0.06-0.08)* |
Table 4: Results of the Monte Carlo Markov Chain Models for each Symptom of Pneumonia.
OR: Odds Ratio, CrI: Credible Interval
The results of this study indicated that the odds of the under-five children having the cough and fever symptoms reduced between 2008 and 2013 but the odds rose by 52% and 93% respectively in 2018. In sharp contrast, the adjusted odds of short rapid breaths were reduced by 91% in 2018 compared with 2013. The temporal pattern observed in the current study corroborates findings from similar studies conducted elsewhere [43,44].
The in-depth spatial hotspot analysis indicated a significant reduction in the prevalence of the symptoms of pneumonia from 2008 to 2018. This decrease may not be unconnected with the various interventional programme and efforts of the government of Nigeria in conjunction with the United Nations and other international partners. For instance, the introduction of the National Pneumonia Control Strategy and Implementation Plan (NPCSIP) by the Nigerian government in the year 2019 towards reducing the high number of childhood mortality due to pneumonia and the menace of pneumonia-related morbidities/deaths in under-five children [45] can explain the reason for our finding. The impact of the government’ interventions may be responsible for the statistically significant reduction of these symptoms over the years. In our study, the gender of the child was found to be related to fever. Gender has been said to be a significant epidemiological factor for most diseases [46]. It is important to note that the males also had a higher prevalence of fever as a symptom of pneumonia for all the years under study. Similarly, Victoria et al. found gender to be significantly related to pneumonia but was expressed as the males having a higher odd of experiencing pneumonia, though the odds of a male having pneumonia than a female in this study was lower [47]. The role of sex hormones in the immunity of individuals may have been responsible for this difference [46].
Children aged 6 to 47 months had higher odds of experiencing cough, fever, or short rapid breaths as symptoms of pneumonia relative to 0 to 5 months children. Previous studies also reported that the odds of contracting pneumonia were higher among children aged 6 to 48 months and lower among children aged 48 to 59 months [31]. This confirms the assertion that younger age corresponds to higher odds of contracting pneumonia in children [7]. Maternal age was significant only for short rapid breaths in mothers aged 20 to 24 where they had higher odds of bringing about short rapid breaths as a pneumonia symptom in their children. This may be due to inexperience in child care or their lack of knowledge or perception of pneumonia. Another study that examined how age affects mothers’ perception and knowledge of pneumonia in children found that women aged 18-24 were grossly lacking in knowledge [48]. This poor knowledge may have accounted for mothers aged 20-24 ability to prevent the occurrence of pneumonia (short rapid breaths) in under-five children. Maternal education goes to a large extent in affecting their knowledge of pneumonia and its preventive measures. It is expected higher education among mothers would correspond to lower odds of the occurrence of pneumonia symptoms in their children. However, this may not necessarily be the case, as there may be a difference between knowledge and practice, particularly regarding health outcomes [49].
The sources of drinking water were not found to be significant for the three symptoms of pneumonia in this study contrary to earlier findings [50,51] despite a large-scale lack of quality water in Nigeria [52,53]. Unclean cooking fuel was found not to be significantly associated with cough, fever, and short rapid breaths as symptoms of pneumonia. This is against the expectation of the effect of pollution caused by unclean solid fuels. The findings were corroborated in a study of the household environment and symptoms of childhood acute respiratory tract infections in Nigeria [54].
The role that housing plays in the state of the health of the people cannot be overlooked and overemphasized [55]. Homes that are healthy with enough quality ventilation and insulation guarantees the health of the members of such households, free from pests and contaminant [56]. Findings from this study showed that the odds of cough and short rapid breaths as symptoms of pneumonia were lower among children residing in buildings with good housing material quality. Overcrowding, poor sleeping arrangements, and poor ventilation dominate most housing with poor quality in Nigeria, but findings on toilet facility contrasts previous literature that sanitation and hygiene is a major contribution to childhood pneumonia [57]. A possible basis for the disparity in the odds of the symptoms across the geopolitical regions can be attributed to variations in social and economic development in these regions [54,58,59].
The use of secondary data for this study limits the choice of variables we explored. The data might have suffered recall bias as this study was a cross-sectional study wherein respondents were made to recall past events without any means of verification by the data collectors. Notwithstanding, the data collection procedures and methods adopted by DHS minimized the effect of such bias. In this study, it was not possible to indicate the presence of pneumonia per child as the number of symptoms examined (as available in the DHS dataset) were not exhaustive to serve as a basis for diagnosis of pneumonia. The symptoms, as examined individually, only serves as pointers to the possibility of the presence of pneumonia. The DHS is well-known for its high quality as a result of the data collection approach used by the data originators. The data used is also nationally representative data covering nearly two decades. Also, the pneumonia symptoms available in the DHS dataset are not exhaustive and prevented the measurement of pneumonia from a diagnostic perspective which would have enabled us to have a variable measuring pneumonia as a disease. The use of Bayesian models in place of frequentist models in understanding the associated risk factors helped to avoid the problems of the inconsistency of results associated with the frequentist approach.
This study provided evidence that variations exist in the prevalence of symptoms of pneumonia among under-five children across the states in Nigeria. The northern states were more characterized by short, rapid breaths while the southern states were more characterized by fever but both regions have a fair share of cough among under-five children.
For the cough and fever symptoms, the increased prevalence between 2013 and 2018 indicates that the symptoms need more attention. Although care should be taken in interpreting the significance of a factor to at least one of the symptoms of pneumonia as significance to pneumonia, our findings supported positive change in pneumonia prevention by providing evidence of risk factors influencing the symptoms of pneumonia. Child’s age and region of residence were significant determinants of all pneumonia symptoms considered in the study. While place of residence was a significant predictor of fever, wealth and mother’s education was significant for cough and fever.
Government and other relevant stakeholders should do more in the area of providing good housing conditions to its population as this will alleviate the prevalence of pneumonia symptoms in Nigeria. The interventions for pneumonia control towards the United Nation’s Sustainable Development Goal (SDG-3) of reducing child mortality by two-thirds should be sustained and improved upon since these strategies have yielded good results. In the Northern part of the country where the results showed that short rapid beaths were more prevalent, the government should design programs to enlighten mothers on the need to properly breastfeed their babies and ensure they get more water to avoid dehydration and provision for more mosquito nets and further enlightenment on ensuring a clean environment should be done as preventive measures. The high prevalence of symptoms of pneumonia in Nigeria as evidenced in this study points to the need for government to improve on the existing sensitization frameworks on home prevention of these symptoms of pneumonia in under-five children in Nigeria.
Ethics approval and consent to participate
The owners of the secondary data used in this analysis obtained the necessary ethical approval and consent prior to data collection. There was no need for further approvals on our part as open-source secondary data.
Competing interests
The authors declared no conflict of interest, financial or non-financial.
Funding
Authors received no funding for this study
Authors’ contributions
AKA, LTV and FAF conceptualized and designed the study. AKA and LTV analyzed and interpreted the data while FAF and AAS were senior authors overseeing the analysis and interpretation of the results. AKA and LTV drafted the manuscript FAF and AAS reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Availability of data and materials
The dataset(s) supporting the conclusions of this article is(are) included within the article (and its additional file(s))
Acknowledgements
The authors are grateful to ICF Macro, USA, for granting the authors the request to use the Demographic and Health Survey data.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.

I would like to offer my testimony in the support. I have received through the peer review process and support the editorial office where they are to support young authors like me, encourage them to publish their work in your esteemed journals, and globalize and share knowledge globally. I really appreciate your journal, peer review, and editorial office.

Dear Agrippa Hilda- Editorial Coordinator of Journal of Neuroscience and Neurological Surgery, "The peer review process was very quick and of high quality, which can also be seen in the articles in the journal. The collaboration with the editorial office was very good."

We found the peer review process quick and positive in its input. The support from the editorial officer has been very agile, always with the intention of improving the article and taking into account our subsequent corrections.
