AUCTORES
Globalize your Research

Research
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals, Department of Pharmacy, University of Karachi-Pakistan.
Citation: Rehan Haider, Asghar Mehdi, Geetha Kumari Das, Zameer Ahmed, Sambreen Zameer, (2024), Sacroiliac Joint Pain. J Clinical Orthopaedics and Trauma Care; 6(8): DOI: 10.31579/2694-0248/113
Copyright: ©2024 Rehan Haider,this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 November 2024 | Accepted: 09 December 2024 | Published: 16 December 2024
Keywords: Sacroiliac joint pain; lower back pain; diagnosis treatment; physical therapy; inflammation; biomechanical imbalances; patient outcomes
Sacroiliac joint pain (SIJP) is a common yet often overlooked source of lower back pain, arising from dysfunction or inflammation of the sacroiliac joints, which connect the sacrum to the iliac bones. This abstract explores the plant structure's etiology, clinical presentation, diagnosis, and treatment options for SIJP. Factors contributing to SIJP include trauma, pregnancy, arthritis, and biomechanical imbalances. Patients usually report local pain in the lower back, buttocks, and upper legs, that can scatter to the legs. Diagnosis frequently includes an all-encompassing medical examination, imaging studies, and demonstrative injections to reinforce the beginning of pain. Treatment approaches surround conservative approaches such as physical therapy, chiropractic care, and antagonistic-angering medications, in addition to interventional processes like corticosteroid injections and radiofrequency extraction. In harsh cases, surgical mediation may be unavoidable. Understanding the complicatedness of sacroiliac joint pain is important for active management and revising patient consequences, emphasizing the need for increased knowledge among healthcare experts and patients alike.
ANATOMY, FUNCTION, AND INNERVATION
The sacroiliac (SI) joint complex is the largest spinal joint in the body, averaging 17.5 cm2 in size. It is most frequently classified as an auricular-shaped diarthrodial joint because it contains a fibrous joint capsule filled with synovial fluid, cartilaginous surfaces, and an intricate set of ligamentous
connections. The SI joint differs from other synovial joints in that it is not readily mobile, there is a discontinuity in the posterior capsule, and the thinner iliac articulation is composed of fibro- instead of hyaline cartilage.[1-2] The SI joint is supported by a network of myofascial structures that help promote movement, support, and stability. These structures include the gluteus maximus and
medius, biceps femoris, piriformis, latissimus dorsi via the thoracolumbar fascia, and erector spinae. The joint is primarily designed for stability and weight bearing, although small degrees of rotation (≤3 degrees) and translation (≤2 mm) occur.[3-4] Previous attempts to establish a causative
relationship between pain and motion abnormalities have been unsuccessful.[5]
The nerve supply of the SI-joint complex is very variable and a subject of great relevance for interventional pain practitioners. To summarize the literature, the last real branches of the S1 and S2 dorsal rami innervate the posterior joint and the surrounding ligaments in nearly all individuals, giving off between one and four branches.[6-7]
There is a contribution from S3 in most but not all individual dual, with again up to four branches being noted in some people.6,7 Whereas some cadaveric dissections indicate that people receive innervation from L5,7,[8] most studies have found this to be absent or infrequent.[6,9] For S4, the
literature is similarly mixed, with some studies demonstrating a neural connection in most individuals[10-11] but others find contributions rare.[6,9] Anatomic studies have also found anastomoses to be common between segmental spinal levels. Some people receive sensory input from the SI joint through the superior gluteal nerve in addition to the lateral branches.7
The innervation of the ventral SI joint is less clinically relevant but no less controversial. Whereas some cadaveric studies have reported nerve filaments stemming from the ventral rami of L4–S2,12 other experts cite contributions from levels as cephalad as [L2.13] Surprisingly, some anatomic studies have failed to find any ventral neural control button to the SI joint.[14]
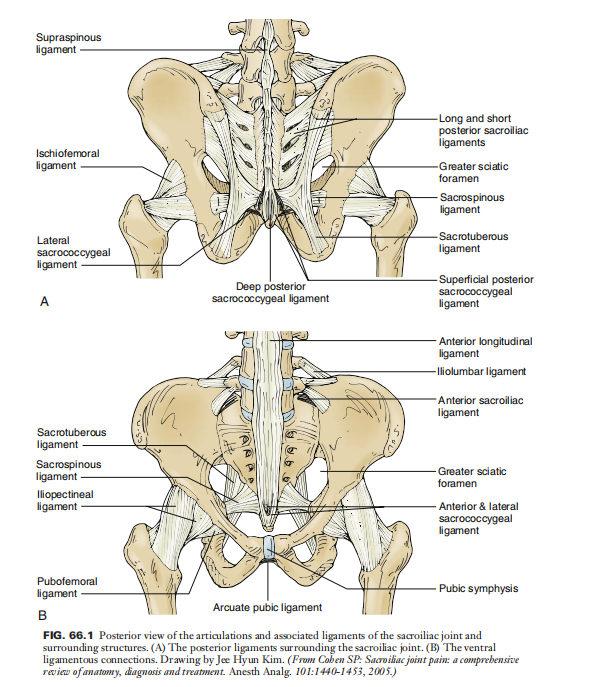
Both intraarticular and extraarticular structures can be sources of SI joint pain. Clinical studies have reported benefits from both intraarticular and extraarticular injections, with one study finding no difference in benefit between the two.[15] An electrophysiologic study performed in cats identified mechanoreceptors in both the joint capsule and adjacent muscles, with most (26/29) residing within the capsule.16 Among these receptor units, 28 were classified as nociceptive and 1 as proprioceptive. Broken down by region, [16] were found in the proximal third, 11 in the middle third, and 2 in the distal third. Immunohistochemical studies in human cadavers have also found evidence of calcitonin gene-related peptide and substance P immunoreactive nociceptors in both capsular and interosseous ligaments [17] Clinical studies have documented pain provocation in patients and asymptomatic volunteers with both capsular distention and ligamentous provocation (Figs. 66.1 and 66.2).[18–22]
EPIDEMIOLOGY
Several problems are inherent when ascertaining the prevalence of SI joint pain. These include but are not limited to the lack of any “gold standard” for diagnosis, perspective (i.e., interventional pain specialists generally attribute a greater proportion of low back pain [LBP] to SI joint pathology than surgeons do), the population studied, and method of diagnosis.
Several studies have utilized “double blocks” with lidocaine and bupivacaine to identify a painful SI joint. These studies have generally evaluated only patients without signs of radiculopathy whose predominant pain complaint was below L5. In the five studies using the reference standard of concordant pain relief with lidocaine and bupivacaine as the diagnostic criterion,23–27 the reported
prevalence rates for SI joint pain ranged between 10% and 45%, with the incidence of false-positive results varying between 0& and 43%.27 One flaw with these studies is that all based their criterion response on intraarticular injections, which likely excluded individuals with predominantly extraarticular pathology (Table 66.1). As already noted, these studies also excluded patients with radiculopathy. In one study that examined the prevalence of SI joint pain in patients with symptoms of radiculopathy and a herniated disc confirmed by magnetic resonance imaging (MRI), over two-thirds of patients had SI joint dysfunction as identified by anatomic and pain-provocation tests.31 This suggests that SI joint pain often coexists with other forms of pathology.
Studies using different diagnostic criteria have yielded similar results. Schwarzer et al.22 conducted a prevalence study in 43 consecutive patients with chronic LBP predominantly below L5 using fluoroscopically guided intraarticular SI joint injections. The authors diagnosed SI joint pain
based on three criteria: pain relief following intraarticular local anesthetic infiltration, ventral capsular tear on post-arthrography computed tomography (CT) scanning, and concordant pain provocation during capsular distension. With analgesic response as the sole criterion for diagnosis,
SECTION VIII Interventional Techniques for Pain Managementhe prevalence of SI joint pain was found to be 30%. When 75% or more pain relief combined with a ventral capsular tear was used as the diagnostic criterion, and the prevalence rate dropped to 21%. Only seven patients satisfied all three diagnostic criteria, for a lower-limit prevalence rate of 16%. Overall, SI joint pathology appears to be the primary generator in between 15% and 30% of patients with chronic axial LBP below L5, being more common in females and the elderly.[32]
ETIOLOGY
The mechanism of injury to the SI joint complex is frequently described as a combination of axial loading and abrupt rotation.1 On an anatomic level, injury or pathology involving the myriad structures comprising the SI joint can lead to nociception. These include capsular or synovial disruption, ligamentous injury, myofascial pain, hypomobility or hypermobility, extraneous compression or shearing forces, cysts, abnormal joint mechanics, microfractures or microfractures,
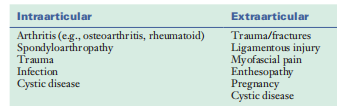
chondromalacia, soft tissue pathology, and inflammation. In patients with persistent nociceptive input, central sensitization can play a contributing role (Table 66.2).Mechanistically, there are numerous reported etiologygies for SI joint pain. These causes can be classified into
intraarticular and extraarticular sources. Arthritis and spondyloarthropathies are two examples of intraarticularlar causes of SI joint pain. Extraarticular sources include enthesopathy, fractures, ligamentous injury, and myofascial pain. The evidence in support of different etiologies
FIG. 66.2 Fluoroscopic image with drawings showing the lateral branch nerve converging on the S1 foramina. (From Yin W, Willard F, Carreiro J, et al: Sensory stimulation-guided sacroiliac joint radiofrequency neurotomy: technique based on neuroanatomy of the dorsal sacral plexus. Spine.
Involves the experience that dispassionate studies have demonstrated important pain relaxation following two together intraarticular and periarticular SI joint injections.33–36 In individual of these studies, periarticular injections were established to support benefits in patients accompanying spondyloarthropathy, suggesting that the two etiologies concede the possibility of overlap.[35]
Distinguishing the middle from two points intraarticular and extraarticular pain dynamo grant permission to be clinically appropriate in deciding on situation alternatives. A current study by Dreyfuss and others. erect that multisite lateral arm blocks were more active at obstructing pain from ligamentous acute than for the discomfort obtained during capsular distension.20 This signifies that sideways arm radiofrequency (RF) denervation grant permission be more likely to satisfy in
things accompanying extraarticular study of plants. In contrast to the intraarticular study of plants, extraarticular pain is more likely to be one-sided, to happen in more immature things, to present with more conspicuous gentleness, and expected to guide a particular inciting occurrence or biomechanics u.s. state etiologies. Numerous determinants can cause a person to expand SI joint pain. Risk determinants that conduct by growing the stress carried by the SI junctures involve corpulence, valid and apparent limb-length conflict, walk irregularities, determined strain/low-grade wound (for instance, activating), scoliosis, preg intermittently move, and incision, especially melding of the posterior of animal or human. The spine section concedes the possibility cause postprocedural SI joint pain by increasing load significance, dwindling the encircling ligaments,iatrogenic breach of the SI joint complex, and postsurgical u.s. state hypermobility.1 In one study that distinguished presurgical
and postsurgical CT scans drink inmates and doubled controls, the investigators found a nearly duple
increase in SI joint deterioration in the surgical subjects distinguished from the control issues (75% vs. 38.2%), with the best occurrence eminent with fusions that comprehensive to the posterior of animal or human.37 Studies judging the reaction to diagnostic injections following sleep-inducer mixture have stated predominance rates varying from 32% to 43%.38 Pregnancy predisposes women to SI joint pain by way of the merger of raised burden gain, exaggerated lordotic posture, the machinelike damage of childbirth, and birth control method-inferred ligamental laxity. In an individual big study
judging over 300 significant women middle from two points 12 and 18 weeks’ ripening, 62% stated LBP, accompanying 54% of these experience pelvic girdle pain located about the SI intersections, and another 29
HISTORY AND PHYSICAL EXAM
SI joint pain may be troublesome to distinguish from the added beginnings of LBP. Numerous studies have settled that no single ancient report or sign-on physical checkup can dependably pronounce an excruciating SI joint.21,22,25 Several reviews have wanted to evaluate the lawfulness of an assault of physical U.S. state test tests in establishing the SI joint as the basic pain engine converting energy. These reviews have mainly proved that flexibility and alignment tests are incompetent in recognizing insult SI joint–mediated pain.1,42 For exciting maneuvers, the results have been assorted. Whereas few reviews have driven that an alliance of aggravating maneuvers can accurately select pain from the SI joint and different beginnings of sleep-inducer pain,43,44 others have attained equivocal39,45,46 or negative47 ends. Nevertheless, dispassionate studies plan that a comprehensive record and physical exam can determine the main clues to plant structure and warn further demonstrative workup. Some of the more common judgments used to select contenders for SI joint blocks are pain mainly local below L5, pain infuriated by climbing from a cross-legged sitting, and affection coinciding with the joint. Several studies and reviews have found that when the region of maximum gentleness is located close to the posterosuperior iliac backbone, skilled is an extreme trend that the basic pain generator is the SI joint.[18-19,48-49] In contrast to additional causes of machinelike LBP, to a degree myofascial, acetogenic, and discogenic pain, SI joint pain is more inclined to be unilateral and happens following in position or time a distinguishing encouraging occurrence (Table 66.3).[22,40-41]
PAIN REFERRAL PATTERNS
Several investigators have sought to decide on pain standard of comparison patterns stemming from SI intersections. In a provocative study transported in 10 asymptomatic volunteers, Fortin and others.18 raise that all matters knowing pain in the ipsilateral buttock, that constantly scattered
into the posterolateral above femur. In a retrospective review by Slipman etal.conducted in 50 patients with
TABLE 66.1 Characteristics of Diagnostic Prevalence Studies Using Double Blocks as the Reference Standard
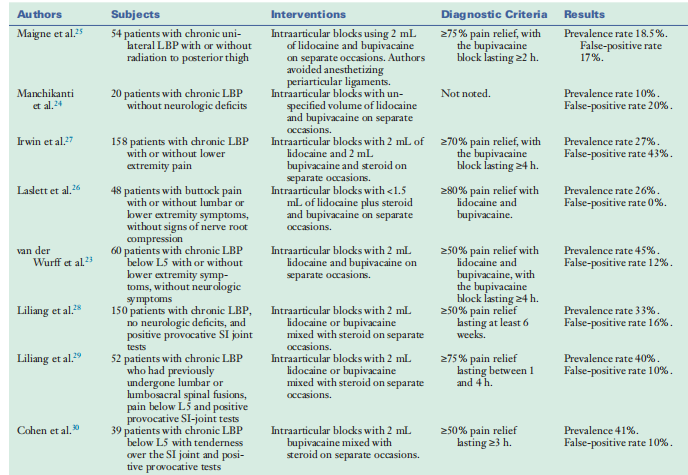
TABLE 66.2 Causes of Intraarticular and Extraarticular
Sacroiliac Joint Pain
Enter from the SI joints, vary in a wide variety and vicinity from patient to the affected person, back and forth, and from stage to level, with as many as four nerves entering the foramina at every spinal level.[97] This precludes the usage of sensory stimulation from making certain ablation of all nociceptive enter. It additionally makes capturing all afferent nerve fibers using conventional RF techniques—in which the typical lesion diameter ranges between three and four mm in a single aircraft—technically challenging. there are many methods to beautify lesion length and triumph over this impediment, consisting of fluid modulation (i.e., injecting electrolytic answers before ablation to
lessen impedance and growth strength output); heating for longer periods (>2 minutes); utilizing higher temperatures; the usage of bipolar generation or very massive, internally cooled electrodes, or “splayed” electrodes that increase the lesion’s floor place; placing prearranged tracks of electrodes (i.e., multisession probes) along the long axis of the sacrum; and replacing RF electrodes with cryoprobes.[63,101-105] The only randomized controlled trials evaluating SI-joint denervation each used cooled RF technology, demonstrating giant pain comfort and purposeful development lasting between 6 months and 1 year in over half of the dealt with people.[63,106] however, the huge,
competitive lesions effected using cooled RF and different lesionenhancing techniques may also increase the charge of postprocedural neuritis, which one look at found took place in near
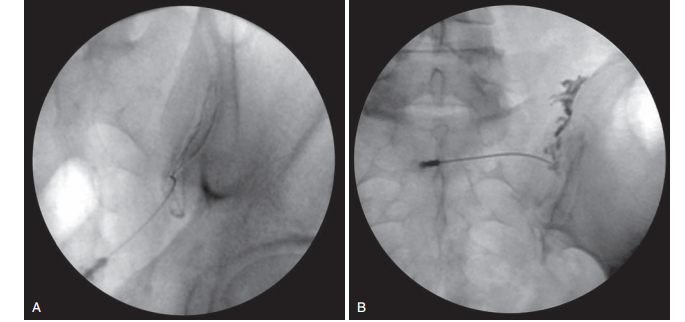
FIG. 66.4 Anteroposterior fluoroscopic images demonstrating (A) intraarticular and (B) extraarticular sacroiliac joint injections.
10% of individuals.[107] For cryoanalgesia, which preserves extra of nerve architecture than heat ablation, the primary the drawback is the shorter period of advantage.102 RF denervation won't be an amazing remedy choice for all and sundry. Focused on the posterior nerve deliver does not cope with ache emanating from the ventral thing of the joint, and Dreyfuss et al.,[20] in their observe, discovered that lateral department
blocks have been greater powerful at preventing ache secondary to extraarticular (i.e., ligamentous) stimulation than from capsular distension, suggesting that such treatment can be less powerful in sufferers with arthritis. To perceive the patients at the highest likelihood of responding to SI joint RF denervation, Cohen et al.[41]performed a multicenter examination evaluating demographic and clinical factors affecting outcomes in 77 sufferers. Typical, 52% of the seventy-seven patients continued to enjoy 50% or extra ache remedy 6 months postprocedure. Not incredibly, sufferers 65 years of age or older (possibly due to the fact aged patients are more likely to have intraarticular pathology) had better preprocedural pain ratings, opioid utilization, and ache to extend under the knee; these elements had been associated with remedy failure.
Although this study determined an association between positive final results and using cooled RF probes, some other examine did not discover a distinction between using cooled and traditional RF ablation (Fig. 66.5).108
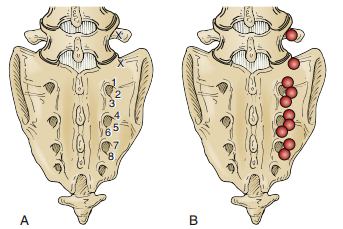
FIG. 66.5 Schematic diagram illustrating (A) target points for rightsided conventional (L4 and L5) and cooled (S1–S3) radiofrequency denervation at the junction of the L5 superior articular and transverse
processes (L4 primary dorsal ramus), the sacral ala (L5 primary dorsal ramus), and S1–S3 foramina (lateral branches). (B) Anticipated lesions at each of the target points. (From Cohen SP, Hurley RW, Buckenmaier CC III, et al: Randomized, placebo-controlled study evaluating lateral branch
radiofrequency denervation for sacroiliac joint pain. Anesthesiology. 109: 279-288, 2008.)
SURGICAL STABILIZATION
SI joint arthrodesis has been used for many years to deal with fractures, instability/dislocations, and pain secondary to degenerative changes. Among those indications, SI joint arthropathy is one of the most debatable, with the available studies being confounded using terrible choice criteria and numerous final results measures. Till lately, the consequences of those studies were confined to small, typically retrospective studies that have yielded combined consequences.109,110 but, in the past few years new minimally invasive the era has yielded extra promising consequences, inclusive of a comparative effectiveness look at that demonstrated superiority over open SI-joint fusion and a large, multicenter a study that discovered fusion to be more powerful than nonstandardized conservative care in patients with both degenerative sacroiliitis or SI joint disruption.[111–113] The reason behind this technology within the context of arthropathy is that it can lessen stress on the joint in people with intraarticular pathology at the same time as minimizing the large tissue trauma related to previous hardware placement.
KEY points
! SI joint ache is a common cause of persistent axial LBP, accounting for between 15% and 30% of instances. It typically provides a unilateral ache situated under L5 that regularly radiates into the posterolateral thigh and occasionally underneath the knee.
l there is susceptible tremendous evidence that a battery of seasoned vocative maneuvers can become aware of a painful SI joint; the reference fashionable for diagnosis remains diagnostic
blocks. but, control blocks are associated
l When a specific, remediable cause of SI joint pain can be identified (e.g., leg-length discrepancy or muscle weakness), treatment should be based on correcting the underlying pathology.
L Both intraarticular and periarticular corticosteroid injections may provide intermediate-term relief in well-selected patients, but the evidence for long-term benefit is mainly anecdotal.
l There is moderate evidence supporting the lateral branch RF denervation to treat SI pain, particularly in individuals with extraarticular pathology.
l In individuals with intraarticular pathology who respond to diagnostic intraarticular injections, there is a growing body of evidence to support minimally invasive arthrodesis.With a full-size fake-advantageous fee.
l SI joint pain is a heterogeneous situation that can be categorized into intraarticular and extraarticular reasons. For both therapy represents an extensive venture.
Treatment of psychotic states with electrical shock for Sacroiliac Joint Dysfunction
CRANIAL SHEAR TEST
With the patient likely and the stomach disabled through the modern, pressure is used to the coccygeal end of the posterior of an animal or human. This test grants permission to make known clearly or officially in cases with SI joint pain.
EXTENSION TEST
The patient is established in the liable position, accompanying the individual of the tester’s hands on the groin of the afflicted side and the difference over the opposite iliac ridge. As the tester brings to bear earthward pressure on the iliac ridge while attracting marginallyon the beginning groin, the incident of SI joint pain indicates study of plants.
FLAMINGO TEST
The patient is requested to be contingent on the complicated stage and spring. Pain in the SI domain is an exhibit of SI joint dysfunction.
GAENSLEN TEST
The patient lies inactive on the checking table accompanying two together knees tense to until the breast. He or she is before requested to shift over to the edge of the table because the part being
proven hovers mentally deranged. The tester therefore pressesabhor the troubled side, hyperextending the cool. Gener associate thought out a sign of SI joint pain, and a helpful Gaenslen
test granted permission to display a trendy study of plants also.
GILLET TEST
With the patient standing accompanying extremities nearly 12 inches separate, the tester sits behind the patient and palpates the S2 thorny process accompanying individual touch and the posterior superior iliac backbone accompanying the additional. As if attractive a big advancing step, the patient therefore flexes the patella, and stylish of the side is proven. If the posterosuperior iliac backbone abandons to move posteroinferiorly concerning S2, the test is certain. A helpful Gillet test displays SI joint dysfunction.
PELVIC COMPRESSION TEST
This test compresses the stomach for one request of sideways pressure to the chief iliac symbol supervised toward the opposite iliac emblem. It is trusted to stretch the posterior SI ligaments and compact the beginning few the joints.
PELVIC DISTRACTION TEST
For this test, the tester applies pressure supervised poste poorly and alongside two together anterosuperior iliac spines. This is asserted to stretch the beginning SI ligaments.
PELVIC ROCK TEST
With the patient dishonest inactive, the tester cups two together hands about the iliac crests for fear that the thumbs act as the prior superior iliac backbone and the palms on the iliac tubercles. He or she before against one's will compresses the stomach toward the midline of the physique. Complaints of pain concede the possibility of display study of plants in the SI joint.
PATRICK TEST
The patient is located inactive accompanying the foundation of the complicated side against the opposite body part. The SI joint is therefore emphasized by urgent together against the flexed patella and contralateral anterosuperior iliac inactive. Although this process is chiefly used to test for SI joint dysfunction, pain in the inguinal or new extent concedes the possibility of cate cool study of plants also. Since this test includes flexion,abduction and extrinsic turn of the cool, it is otherwise known as
the FABER test.
SACROILIAC SHEAR TEST
With the patient dishonest likely, the tester crosses two togethergiving back the posterior of an animal or human. The overlying help transfers a location of mail service teroanterior thrust, while the fundamental help is used to discover motion in the joint.
THIGH THRUST TEST
This test applies a posterior shearing stress to the sacroiliac joint through the femur.
Research Method
Recent studies have used differing diagnostic tests to judge SIJ pain, including the femur thrust test and condensation test, which have proved few discriminating capacities for diagnosis. Systematic reviews have more happened administered to determine the efficacy of various clinical intervention, in the way that sacroiliac joint fusion and cooled radiofrequency neurotomy, are deliberate with the top alternatives for pain reli
The verdicts display that demonstrative veracity for SIJ pain remains a challenge, with medical examination methods providing restricted predictive volume. The orderly review emphasizes that while sure interventions like SIJ melding and radiofrequency situations rank extreme for reconstructing pain intensity and kind of growth, the overall evidence is still uncertain on account of variability in study designs and methods.
Additionally, the dishonest-definite rate for sacroiliac joint injections is around 20%, signifying a need for a cautious understanding of demonstrative results.
The complexity of diagnosing SIJ pain is complicated for one imbricate with other reduced back pain beginnings. The lack of patterned demonstrative criteria and the instability in situation answers make a tailored approach for each patient.
Current non-surgical remedies, containing drugs and physical therapy, show restricted enduring benefits, suggesting that more authoritative interventions can be proper for never-ending cases.
In conclusion, while skilled are promising mediations for sacroiliac joint pain, the demonstrative process debris deficient, and treatment efficiency changes widely between things. Future research should devote effort to something cleansing demonstrative tests and exploring new healing alternatives to embellish patient effects in managing SIJ pain.
Acknowledgment
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project
We would also like to thank My Mentor [. Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout the research. Their insights and expertise were instrumental in shaping the direction of this project
Declaration of Interest
I at this moment declare that:
I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Financial support and sponsorship
No Funding was received to assist with the preparation of this manuscript
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
