AUCTORES
Globalize your Research

Research Article
*Corresponding Author: Lara-Vargas Jorge A, Department of cardiac rehabilitation, Centro Médico Nacional 20 de Noviembre Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado Facultad Mexicana de Medicina Universidad La Salle.
Citation: Diaz-Zepeda Jennifer S, Lara-Vargas Jorge A, Cárdenas-Beltrán Luis C, Machuca-Loeza Maricruz G, Pineda-Juárez Juan A., et al, (2024), Evaluation of the Effects of a Cardiac Rehabilitation program with Combined Training on Left Ventricular mass in Patients with Heart Failure, J Clinical Cardiology and Cardiovascular Interventions, 17(13); DOI: 10.31579/2641-0419/428
Copyright: © 2024, Lara-Vargas Jorge A. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 November 2024 | Accepted: 06 December 2024 | Published: 13 December 2024
Keywords: cardiac rehabilitation; combined training; left ventricular mass; heart failure
Background and Aim: Heart failure (HF) is a chronic, multisystemic, heterogeneous, and progressive syndrome where sustained activation of compensatory neurohormonal mechanisms leads to maladaptive left ventricular remodeling. There is evidence that regular exercise stimulates physiological cardiac growth, increases mitochondrial biogenesis, mitophagy, and improves mitochondrial dynamics in healthy hearts. However, its effects on left ventricular mass and the relationship with peak VO2 gains, specifically with combined training in HF patients, have not been elucidated. Therefore, the aim of the study is to assess whether a cardiac rehabilitation program (CRP) with combined training can increase left ventricular mass and thereby peak oxygen consumption (VO2p) in patients with HF.
Materials and Methods: A quasi-experimental, non-controlled study was conducted in chronic HF patients who completed the supervised phase 2 of the CRP. Participants underwent transthoracic echocardiography and a cardiopulmonary exercise test with gas analysis (CPET) where echocardiographic variables such as mass, end-diastolic volume, posterior wall thickness and interventricular septal thickness of the left ventricle were measured, as well as cardiopulmonary exercise variables such as VO2p, VT1, VAT, VT2, FATmax and crossover, at admission and discharge.
Results: A total of 50 patients diagnosed with HF were included, 70% men, with a mean age of 63.9 ± 11.7 years. In the inferential analysis between baseline parameters and after completing the CRP, significant differences were found in LVEF (p <0.001), end diastolic volume (p <0.001), left ventricular mass indexed to total body surface area (p <0.001), oxygen pulse (p <0.001), Mets-C (p <0.001), VT1 (p = 0.013), VAT (p = 0.002), VT2 (p <0.001), FATmax (p = 0.003), and crossover (p <0.001). VO2 peak behavior was analyzed in patients who had an increase in ventricular mass (n=17) compared to those who had a decrease in ventricular mass (n=33), finding both groups had statistically significant changes in VO2 peak (p = 0.04).
Conclusions: CRPs based on combined physical training are effective and safe in patients with chronic HF, improving peak VO2 in clinically stable patients regardless of changes in left ventricular geometry measured through left ventricular mass. While the most frequently presented adaptation at the end of the intervention was reverse remodeling, this condition does not contravene the gains in cardiorespiratory fitness, as this ventricular mass could generate greater fitness and aerobic power.
Chronic heart failure is one of the most common cardiovascular disorders in the world, with an annual incidence of 0.1-0.5% and a prevalence of 1-3% [1,2]. This heterogeneous and progressive clinical syndrome initially activates various compensatory mechanisms that modulate ventricular function within physiological limits, which later become deleterious [3]. Among the most important adaptations are the generalized increase in sympathetic nervous tone, attenuation of parasympathetic tone and activation of the renin-angiotensin-aldosterone system, leading to loss of heart rate variability and increased peripheral vascular resistance [3]. As HF progresses, sustained activation of neurohormonal systems generates hypertrophy, fibrosis, stiffness, and structural and geometric alterations known as left ventricular remodeling [4].
Evidence demonstrates that regular exercise induces structural and molecular changes, specifically through signaling pathways that stimulate physiological cardiac growth in healthy hearts and hypertrophy of skeletal muscle [4,5,6,7]. Exercise also increases mitochondrial biogenesis, mitophagy, and improves mitochondrial dynamics by activating the AMPK protein and upregulating sirtuins 1/3, factors that promote the synthesis of new mitochondrial proteins and muscle growth [4,8]. Cardiac rehabilitation based on aerobic training (AT) can increase maximal oxygen consumption (VO2max) and decrease left ventricular mass in hypertensive patients (9). In patients with reduced left ventricular ejection fraction (LVEF), this training modality increases LVEF, decreases end diastolic dimensions of the left ventricle, and improves motion abnormalities [10,11,12,13,14]. Additionally, this has been developed in a diverse manner with varying frequencies of strength training (ST) intended to promote muscle expression and mitochondrial biogenesis [15].
Multiple studies and meta-analyses, such as HF-ACTION [42], CROS-HF [16], and the most recent meta-analysis by Taylor et al. [17] have clearly demonstrated that exercise is safe, improves exercise tolerance, ventricular remodeling, endothelial function, health-related quality of life, and reduces hospital readmissions in patients with HF, both with reduced and preserved ejection fraction [18]. However, its effects on left ventricular mass and the relationship with peak VO2 gains, specifically with combined training, have not been elucidated. Our hypothesis is based on evidence of the ability of ST (peripheral and inspiratory) combined with ET to activate physiological pathways of cardiac muscle growth in a pathological environment which will generate an increase in left ventricular mass with a possible increase in VO2max in patients with HF. Therefore, the objective of the study is to evaluate the effect of a combined CRP on left ventricular mass in patients with HF.
Materials And Methods
A quasi-experimental, non-controlled study was conducted with a convenience sampling of patients who completed phase II of the supervised CRP. Among the inclusion criteria were patients of any gender older than 18 years known to have HF with reduced and preserved LVEF due to any ischemic etiology, infiltrative cardiomyopathies, cardiotoxic agents, arrhythmias, and mild to moderate repaired or unrepaired valve disease. They were required to have a transthoracic echocardiogram and a cardiopulmonary exercise test with gas analysis (CPET) at the beginning of the program and within 6 months after discharge. The exclusion criteria included pregnant patients, those with decompensated HF, coexisting orthopedic disease that prevented participation in a physical training program, missed over 80% of sessions, had aortic dissection, symptomatic severe aortic stenosis, acute pulmonary embolism, recent myocardial infarction (less than 2 days), uncontrolled cardiac arrhythmias with evidence of low output, uncontrolled hypertension (greater than 200/100), high-grade atrioventricular block, presence of intracardiac thrombus, acute pericarditis or myocarditis, hypertrophic cardiomyopathy, or advanced HF on a transplant protocol, with or without intracardiac devices and complex congenital heart disease.
Measurement of Echocardiographic and Cardiopulmonary Variables
Left ventricular measurements were performed using a Phillips EPIQ1, 4, and CVx ultrasound system. Linear measurements were taken from the left parasternal long axis for interventricular septal and left ventricular posterior wall thickness. The end diastolic volume of the left ventricle was obtained from apical four- and two-chamber views, considering the upper limits of the corresponding normal range: 74ml/m² for men and 61 ml/m² for women, values indexed to total body surface area (19). LVEF was calculated using the biplane modified Simpson method, with a threshold of abnormality <52 xss=removed>
At admission and discharge from the supervised phase II of the CRP, all patients underwent a symptom-limited CPET for assessment of dyspnea, angina, nausea, vomiting, muscle fatigue, and/or patient request. After calibrating volumes and gases (O2 and CO2) and fasting for at least 4 hours before the test, a standardized protocol was executed, either a modified Bruce Ramp or a modified Naughton Ramp protocol depending on the patient's DASI greater or less than 5 METs, performed with incremental loading. Oxygen consumption (VO2), carbon dioxide production (VCO2), and ventilation per minute were continuously evaluated using expired gas analysis, indirect calorimetry, and continuous cardiopulmonary variables. The test was deemed maximal if one of the following two criteria was met: RER ≥1.15 and/or ≥85% of the predicted maximum heart rate for age. As part of the CPET, all patients underwent baseline spirometry in a standing position. Once the test was completed, a physical quality assessment was conducted, including strength, balance, flexibility, and coordination, as well as a cardiovascular risk stratification consultation by a specialist.
Cardiac Rehabilitation Program Protocol
Combined physical training was carried out through 3 weekly sessions for 4 or 6 weeks depending on the cardiorespiratory fitness level obtained from the initial exercise test. Each session lasted 60 minutes, alternating aerobic training (AT) on a cycle ergometer or treadmill, which included a 5-minute warm-up at 40-50% of the heart rate reserve (HRR) and/or Borg scale 10-11, followed by a moderate intensity phase at least 70% of the HRR and/or Borg scale 12-13 for 20 minutes, and finally a 5-minute cool-down, with progression of 2.5-5% per session based on patient tolerance. The ST consisted of a warm-up, an active phase with 3 sets of 10, 12, and 15 repetitions per muscle group (starting with 30% of maximum repetition in upper limbs and 40% in lower limbs), and finally cooling down with relaxation exercises. Blood pressure and heart rate were measured at rest before both types of exercise, at maximum effort, and during recovery. All sessions were carried out in the designated area for cardiac rehabilitation and/or gym under the supervision of a cardiologist, physical rehabilitation physician, physiotherapist and nurse.
Patients also received virtual sessions of diaphragmatic re-education and online classes on various topics for managing cardiovascular risk factors, such as medication adherence, transition to phase III of the program, anxiety and stress management, depression and sleep disorder management, and finally, heart-healthy dietary habits, twice a week. Participants were also evaluated and given nutritional counseling at the beginning and end of phase II, where body composition was assessed using bioimpedance and skinfold measurements, and a dietary plan was established according to their needs.
Based on the results of the study by Edelman et al. in 2011 [18], which reported an increase of 0.7 in left ventricular mass following an AT exercise program and taking into account the characteristics of the population, a 95% confidence interval was considered, with 80% statistical power and a 10% margin of error, resulting in a sample size of 21 patients. The distribution of quantitative variables was analyzed for normality using the Kolmogorov-Smirnov test, those with a parametric distribution were reported as means ± standard deviation, while qualitative variables were presented as percentages. The descriptive analysis of demographic characteristics, comorbidities, and HF etiology was carried out using measures of central tendency (means) ± standard deviation, absolute values (n) and percentages. Echocardiographic characteristics were established as qualitative and quantitative variables. Qualitative variables were studied with absolute values (n) and percentages. Quantitative variables were analyzed using means ± standard deviation and percentage change. For inferential analysis and comparison of quantitative variables, the paired Student’s t-test was used, and for categorical variables, the McNemar test. Statistical significance was defined with a p-value of less than 0.05. Data analysis was performed using SPSS statistical software version V23 (IBM 2020).
A total of 50 patients with a diagnosis of heart failure were analyzed, with a predominance of male sex at 70% and an average age of 63.9 ± 11.7 years. Among the patients, 15 had a body mass index in the overweight range and 12 were obese; 58% of patients were diabetic and 66% were hypertensive (Table 1).

Table 1. Characteristics of the Study Population.
Data are presented as means ± standard deviation and in number (n) and percentage (%). CABG: coronary artery bypass grafting. PCI: percutaneous coronary intervention. TAVI: transcatheter aortic valve implantation.
Among the etiologies of HF 56% was ischemic, 14% valve disease, 8% dilated cardiomyopathy, 4% amyloidosis, 10% congenital heart disease, 8% pulmonary arterial hypertension, 4% arrhythmias, 2% viral myocarditis, and 2% atrial myxoma (Table 1).
LVEF was analyzed initially and at the end of the program and was classified as reduced <40>p = 0.68). Basally, 32 patients had left ventricular mass indexed to total body surface area (BSA) within normal limits, while 18 had increased ventricular mass (Table 2).
| Parameter | n = 50 | |
| Pre intervention n (%) | Post-intervention n (%) | |
| LVEF | ||
| Preserved | 20 (40) | 24 (48) |
| Intermediate | 11 (22) | 13 (26) |
| Reduced | 19 (38) | 12 (26) |
| LV dimension | ||
| LV dilatation | 14 (28) | 11 (22) |
| Left ventricular mass | ||
| Normal | 32 (64) | 34 (68) |
| Hypertrophic | 18 (36) | 16 (32) |
Table 2. Morphological and Functional Characteristics of the Left Ventricle Before and After the CRP Program
Data are presented in absolute values (n) and percentages (%). LVEF: left ventricular ejection fraction. LV: left ventricle. LVEF reduced <40>74ml/m² for men and >61 ml/m² for women. Normal ventricular mass: <95g>
In the inferential analysis between baseline parameters and following the completion of the CRP, significant differences were found in LVEF (p <0>p <0>p <0>p=0.14 and p=0.17, respectively), there was a 10.8% change in the thickness of the LV posterior wall, which is clinically significant (Table 3).
The variables assessing maximum cardiorespiratory fitness included peak oxygen consumption (VO2p) measured through gas analysis and expressed in metabolic equivalents (METs), METs obtained from estimated treadmill load (METs-c), and oxygen pulse (PO2). All three variables exhibited statistically significant differences with percentage changes greater than 10%, rendering them clinically significant (Table 4). VO2p increased by 17%, from a baseline of 4.7 ± 1.3 to 5.5 ± 1.5 at the end of the program, with p<0>p<0>p<0>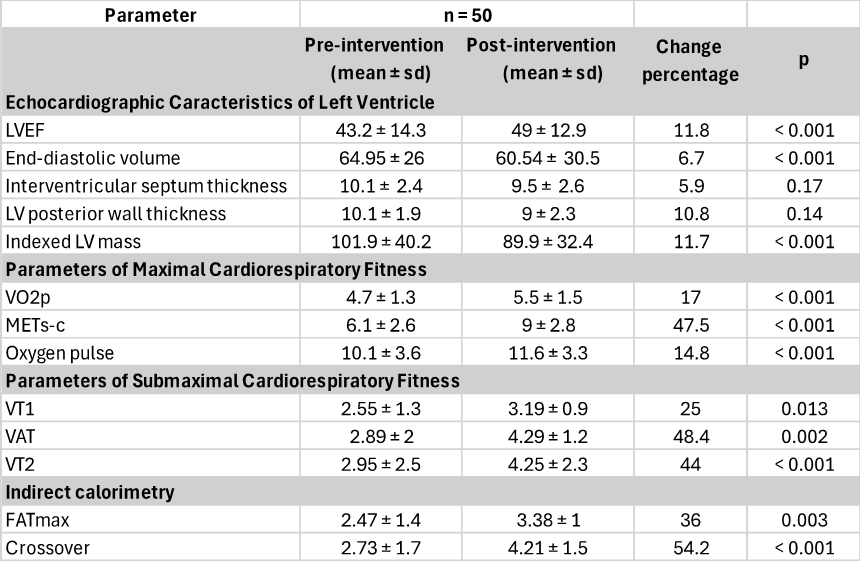
Table 3. Echocardiographic Characteristics of the Left Ventricle, Cardiorespiratory Fitness Parameters and Indirect Calorimetry Before and After the Cardiac Rehabilitation Program
Data are presented as means ± standard deviation and percentage change. LVEF: left ventricular ejection fraction. LV: left ventricle. VO2p: peak oxygen consumption expressed in METs. METs: metabolic equivalents. METs-c: estimated treadmill load. VT1: first ventilatory threshold or aerobic threshold. VAT: respiratory exchange ratio equal to 1. VT2: second ventilatory threshold or anaerobic threshold. FATmax: maximal fat oxidation point. Crossover: exercise intensity at which the energy supplied by carbohydrates exceeds that provided by fats.
The submaximal cardiorespiratory fitness variables analyzed included ventilatory thresholds from the cardiopulmonary exercise test, which showed significant increases: VT1 had a 25% increase, from a baseline of 2.55 ± 1.3 to 3.19 ± 0.9 at the end of the program, with p=0.013. VAT shifted from a baseline of 2.89 ± 2 to 2.29 ± 1.2, with an increase of 48.4% and p=0.002. VT2 showed a significant increase (p<0>
Indirect calorimetry assessed FATmax and crossover (point of interchange between fat and carbohydrate oxidation rates), both showing significant differences. The initial FATmax was reported at a mean of 2.47 ± 1.4 and improved to 3.38 ± 1 post-program, with a percentage change of 36% and p=0.003. Crossover also showed an increase of 54.2%, with a baseline mean of 2.73 ± 1.7 and ending at 4.21 ± 1.5, p <0>
The behavior of left ventricular mass was analyzed (Table 4), revealing that patients with an increase in ventricular mass (n=17) had an 18.2% increase, from a baseline of 92.3 ± 33.3 to 109.1 ± 33.6, p<0 n=33)>
Table 4. Left Ventricular Mass Behavior
Data are presented as means ± standard deviation and change percentage. LV: left ventricle.
The behavior of VO2p, expressed in METs, was studied in patients who increased their ventricular mass compared to those who decreased it. Patients with an increase in LV mass achieved a mean gain of 4.9 ± 1.5
MET and the ones that decreased LV mass 5.9±1.4 METs. Both groups showed significant increases in METs ( p = 0.04), however, the group in which LV mass decreased presented greater gains (graph 1).
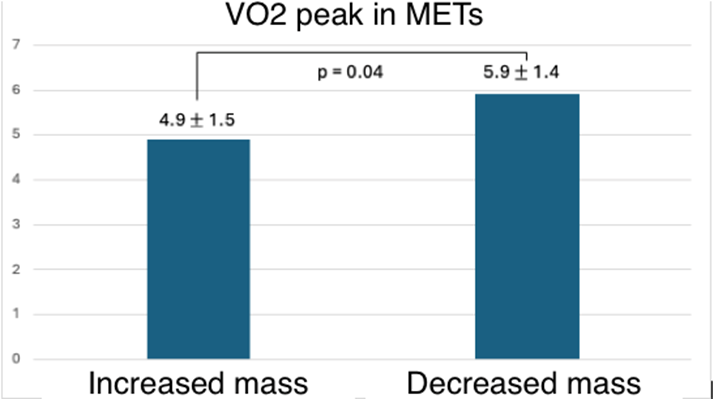
Graph 1. Peak Oxygen Consumption (VO2p) Expressed in Metabolic Equivalents (METs) in the Group of Patients Who Increased Left Ventricular Mass and in the Group Who Decreased Left Ventricular Mass
Data are presented as means ± standard deviation. LV: left ventricle. In the group that increased LV mass, the mean gain was 4.9 ± 1.5 METs (VO2p measured in METs), while the group that experienced a decrease in mass achieved an increase of 5.9 ± 1.4 METs (VO2p measured in METs). Both groups showed significant increases in METs (p = 0.04).
The geometry of the LV was assessed at the beginning and end of the program, and the changes observed are detailed in Table 5.
| Geometry | n = 50 | |
| Pre-intervention n (%) | Post-intervention n (%) | |
| Normal | 15 (30) | 15 (30) |
| Concentric remodeling | 14 (28) | 11 (22) |
| Concenric hypertrophy | 4 (8) | 6 (12) |
| Eccentric hypertrophy | 5 (10) | 8 (16) |
| Physiological hypertrophy | 3 (6) | 4 (8) |
| Dilated hypertrophy | 6 (12) | 1 (2) |
| Eccentric remodeling | 2 (4) | 4 (8) |
| Mixed hypertrophy | 1 (2) | 1 (2) |
Table 5. Pre-Intervention and Post-Intervention Left Ventricular Geometry
Data are presented as absolute values (n) and percentages.
Patients underwent supervised training with an overall mean training volume of 329.26 METs/week and 395.56 Kcal/week. The group that exhibited an increase in ventricular mass had a mean training volume of 319.41 compared to 334.33 in the group that experienced a decrease in LV mass. Kcal/week in the group that increased ventricular mass was 381.11 vs. 403 Kcal/week in the group that decreased LV mass. There were no reported adverse events during any of the exercise training sessions.
This research is the first specifically designed to investigate the effects of combined training on left ventricular mass in patients with HF of varying pathogenesis and independent of LV systolic function. Our findings demonstrate that combined training induces a reverse remodeling effect, leading to a decrease in end-diastolic volumes, an increase in LVEF and changes in left ventricular mass, primarily reductions, which are associated with greater oxidative potential (evidenced by the indirect calorimetry and ventilatory threshold variables), VO2p, METs-c, and PO2 significantly.
Exercise offers multiple physical and health benefits to individuals with chronic HF. Training modality, frequency, duration, and intensity are key factors that influence the degree of adaptations achieved. Aerobic training (AT) has been the primary exercise modality in cardiac rehabilitation programs (CRPs), with predominant evidence in the literature; however, strength training (ST) provides additional and complementary benefits to ET [25].
AT characterized by sustained increases in cardiac output with reduced peripheral vascular resistance induces morphological and functional adaptations, both central and peripheral. Centrally, it generally increases stroke volume and improves cardiac contractility, coupled with cardiac remodeling, specifically eccentric hypertrophy, enables greater venous return, ventricular filling, and cardiac output. Peripherally, it enhances vascular capacitance, permeability, and capillary density, which in turn improves muscle perfusion and contributes to an increased oxygen supply [27,28]. ST characterized by an increase in peripheral vascular resistance and slightly in cardiac output, during short episodes, produces concentric hypertrophy, increases lean mass and muscle strength [21,22,23,24]. Both training types achieve morphological and functional gains that collectively yield greater cardiovascular and musculoskeletal benefits; however, their effects on left ventricular mass have not yet been fully elucidated, particularly considering the interference effect on combined adaptations [44,45,46].
Training volume, a byproduct of frequency, duration, and intensity, as well as program length, will influence the gains achieved, but this volume quantifies the ET-dependent effects [30]. In our study, we implemented a program lasting 4 to 6 weeks, as regular training over at least six weeks is minimally sufficient for developing central and peripheral adaptations, as evidenced in our results [31,33]. Additionally, we improved patient adherence to the program due to its hybrid constitution.
Various international guidelines recommend exercise-based CRPs for patients with HF, whether with preserved or reduced LVEF, with a class I indication and level of evidence A [20]. Generally, the recommendation is to perform 30 minutes of moderate-intensity AT (starting with 40 and progressing up to 80% VO2p) at least 5 days per week, along with strength training, performing 10-15 repetitions for each muscle group, 2 to 3 times a week at 30-60% of 1RM, totaling 500 METs/week or 1500 Kcal/week, which is quite similar to the prescription we carried out in our study, except for the weekly METs and Kcal, which were lower in our sample. However, it is important to note that only supervised AT was quantified, as the contribution of ST is not feasible to quantify using the method employed by Kaminski [43]. This recommendation is derived from numerous trials, systematic reviews, and meta-analyses that have documented gains in exercise tolerance, quality of life, and reduced hospital readmissions, without adverse effects in patients with HF [15,16,17,26,27,28,31].
We know that regular exercise can restore autonomic, neurohormonal, and abnormal hemodynamic function, but several studies have demonstrated that it can reverse or attenuate LV remodeling [17,33,37]. The importance of this lies in the fact that left ventricular remodeling plays a key role in the progression of HF and is associated with increased morbidity and mortality. Moderate-intensity AT is capable of decreasing end-diastolic volumes, improving ejection fraction and increasing VO2peak by approximately 2.98 ml/kg/min or between 12% and 31% in patients with HF by enhancing contractility, preload, and vascular reserve [27,28,29,30,33,37]. However, combined training has not been conclusive in improving EF or reducing end-diastolic volumes [27,38,39,40,41] but has shown improvements in VO2peak [38,39,40]. Nevertheless, our study found significant gains in EF and VO2peak, as well as a reduction in end-diastolic volume with combined training.
Although the complex changes occurring in the heart during remodeling have traditionally been described in relation to anatomy, the remodeling process also affects cardiac myocyte biology and energy systems. In HF the concentrations of ATP and myocardial phosphocreatine are decreased, which, along with mitochondrial dynamics anomalies, compromises ATP generation. It has been shown that AT in patients with HF leads to improvements in VO2max by increasing the number of mitochondria and enzyme activity, thereby enhancing energy substrate utilization [12,25,28]. In our study, we hypothesize that the increase in mitochondrial biogenesis, along with greater capillary supply, led to improved cardiorespiratory fitness measured by submaximal variables and VO2p [12], meaning that training was able to enhance oxidative systems by generating metabolically active myocardial mass, which resulted in higher VO2p independent of changes in ventricular geometry. Indirect calorimetry supports these findings by showing a shift in the loading rates of FATmax and crossover to a higher VO2 at the final exercise test compared to the initial, suggesting a more developed oxidative base, despite the predominant reduction in ventricular mass.
At the same time, this increase in mitochondrial biogenesis is likely to result in lower lactate production during submaximal exercises and stricter control of the acid-base state, which is related to a positive impact on performance in daily living activities. This adaptation can be observed in the ventilatory thresholds (VT1, VAT, and VT2), which appeared at a higher VO2 at the end of the program, indicating a better submaximal cardiorespiratory fitness that directly impacts quality of life in this population [27,29,32]. Unfortunately, we could not perform histopathological studies of the myocardium to corroborate these intracellular findings.
It is important to mention that peripheral adaptations in circulation and skeletal muscle caused by exercise may also contribute to VO2p modifications [34]. Maximum cardiorespiratory fitness expressed as VO2max or VO2peak reflects the integrated capacity to transport oxygen from the atmosphere to the mitochondria to obtain the energy necessary for living [2]. Therefore, by quantifying an individual's functional capacity, it depends on a linked chain of processes that include ventilation and pulmonary diffusion, biventricular function, the ability of the vasculature to transport blood, and the competence of muscle cells to receive and utilize oxygen for ATP generation, it is considered a reflection of overall health. VO2max is determined by many factors, including the heart [2]. A change in cardiac geometry could modify the ability to increase ventricular volume and thus VO2peak, but we deem it necessary to clarify whether it was the increase or decrease in ventricular mass that was responsible for functional adaptation during exertion.
The primary objective of this study was to evaluate whether a cardiac rehabilitation program with combined training could increase left ventricular mass and thus peak VO2 in patients with HF. We know that cardiac hypertrophy is essential for maintaining pump function in HF; however, as it progresses, cellular organization breaks down, fibrosis occurs, contractile elements are lost, and energy metabolism is altered, leading to pathological hypertrophy. Within our results, we observed that the majority of the participants showed a significant decrease in left ventricular mass, likely due to the reduction in cardiac fibrosis. Conversely, one third of participants showed a significant increase in left ventricular mass, which may be secondary to the activation of signaling pathways promoting cardiac growth in a pathological environment and likely involves mass capable of generating significant VO2p gains.
Campos et al. demonstrated that 8 weeks of moderate-intensity AT improved left ventricular function associated with gains in mitochondrial oxidative capacity and reduced cardiac fibrosis in rodents with HF [5]. Schaible et al. found that an 8 to 10 weeks swimming program reversed pathological hypertrophy in rodents [35]. Based on these findings, we deduce that combined training can decrease left ventricular mass by reducing cardiac fibrosis, lowering afterload, triggering a sympathovagal balance and decreasing vasoconstrictive neurohormones that ultimately ended reducing the imposed hemodynamic load.
However, the most relevant result shows that the increases in peak oxygen consumption (VO2peak) after cardiac rehabilitation program (CRP) were independent of changes in left ventricular mass. We believe that this discordant effect between left ventricular mass and its ambiguous gain in cardiorespiratory fitness variables largely depends on the diversity of the pathophysiology of heart failure and that this reverse remodeling is independent of the increase in mitochondrial oxidative capacity, generating a metabolically active ventricular mass that leads to gains in VO2p and other variables associated with cardiorespiratory fitness, in which we can also notice an increase in oxygen pulse (PO2) which is recognized to be its main cardiac component measured by cardiopulmonary exercise test.
In our study, we established a multidisciplinary CRP with combined exercise and inspiratory diaphragmatic re-education sessions due to the evidence showing significant gains in health-related quality of life, VO2peak, and cardiac remodeling. Additionally, by including specialists in nutrition, psychology, nursing, physiotherapy, and physical rehabilitation, we contributed to managing associated cardiovascular risk factors that also improve the afore mentioned outcomes.
During the study there were no significant complications. Evidence has shown that the incidence of major cardiovascular complications during outpatient CRPs is 1 in every 60,000 hours [42]; however, the incidence is lower in supervised programs, as was the case in our study.
Many limitations and methodological biases exist. Most participants were men with heart diseases of various etiologies, and their pathophysiological heterogeneity influenced the results. Due to the sample size, it was not possible to assess whether specific changes in ventricular geometry were significant after the intervention, nor to conduct sub-analyses only on ventricular mass. It was not possible to study the morphological changes induced by combined training at a histological level because myocardial biopsies were not performed. This was a quasi-experimental study, as it was uncontrolled and unblinded, and the definition of the intervention largely had to be according to the characteristics of the patients due to the high risk of the population. Although adherence to the program was over 80%, the exercise frequency was one supervised session per muscle group per week, so we do not know if patients complied with the recommendations of two sessions per week per muscle group in a non-supervised manner, nor if increasing exercise sessions would generate greater gains in ventricular mass. Lastly, the transthoracic echocardiograms performed before and after the program depended on the operator's experience for the accuracy of the measurements, alongside inter-observer and intra-observer variability, as well as patient characteristics to allow for high-quality imaging. Despite this and the limitations of the population studied, the results were significant enough to draw conclusions.
CRPs based on combined physical training are effective and safe in patients with heart failure, improving VO2p in clinically stable patients independently of changes in left ventricular geometry measured through left ventricular mass. Although the most frequently presented adaptation at the end of the intervention was reverse remodeling, this condition does not contradict gains in cardiorespiratory fitness, as this ventricular mass can generate greater resistance and aerobic power.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
