AUCTORES
Globalize your Research

Research
*Corresponding Author: SenDasgupta Chaitali, Professor, Departments Cardiac Anaesthesia, Institute of Post Graduate Medical Education and Research, Kolkata.
Citation: Chaudhuri S, SenDasgupta C, Goswami A, Sinha S (2021). Comparison of Effects of Prophylactic Amiodarone versus Lignocaine and Magnesium Sulphate versus Placebo in Prevention of Arrhythmias in Patients Undergoing Valve Replacement Surgery. Clinical and Interventional Cardiology. 1(1); DOI: 10.31579/cic-2021/004
Copyright: © 2021 SenDasgupta Chaitali. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 July 2021 | Accepted: 19 August 2021 | Published: 28 August 2021
Keywords: postoperative arrhythmias; lignocaine; magnesium sulphate; amiodarone; open heart surgery; acute atrial enlargement; cardioplegia; ventricular tachyarrhythmias
Background- Postoperative arrhythmias are a serious but frequent complication of open heart surgery. The incidence of postoperative supraventricular arrhythmias has been reported to be 11-54%, and the incidence of ventricular arrhythmias to be 1.8-13% [1]. Various drugs have been tried prophylactically to prevent postoperative arrhythmias including amiodarone, lignocaine and magnesium sulphate.
This study compares the efficacy of amiodarone, lignocaine and magnesium sulphate to placebo in prevention of postoperative arrhythmias in patients undergoing valve replacement surgery under cardiopulmonary bypass.
Materials and methods- This prospective, double blind, parallel group randomized study was carried out in the Cardiothoracic & Vascular Surgery OT and postoperative ICU of IPGME&R and SSKM Hospital, Kolkata in 60 subjects of either sex, 15-65years of age undergoing elective valve replacement surgery. The patients were allocated in three groups comprising 20 patients in each group. Group 1 received normal saline; Group 2 received 3mg/kg of amiodarone; Group 3 received 1.5mg/kg of lignocaine and 40mg/kg of magnesium sulphate just before the release of aortic cross clamp. The frequency of occurrence of supraventricular or ventricular arrhythmias in the 24 hour postoperative period was determined in all groups. Observed data was compiled and analysed using appropriate statistical methods.
Results- There was no significant difference between the 3 groups in the incidence of supraventricular or ventricular arrhythmias in the 24 hour postoperative period.
Conclusion- Single dose of amiodarone, lignocaine and magnesium sulphate have no advantage over placebo in prevention of postoperative arrhythmias.
Running Title:
Prophylaxis of Postoperative Arrythmia
Postoperative arrhythmias are a serious but frequent complication of open heart surgery. The incidence of postoperative supraventricular arrhythmias has been reported to be 11-54%, and the incidence of ventricular arrhythmias to be 1.8-13% [1].
These significantly increase the morbidity of the patients and adversely affect their prognosis. These arrhythmias are multifactorial in origin and thus, their prevention is a challenge requiring knowledge of the predisposing factors which lead to the development of arrhythmias in the postoperative period.
Atrial fibrillation is the most common arrhythmia encountered postoperatively, the incidence varying with the type of cardiac surgery undertaken and the different ascertainment methods used. It prolongs hospital stay, adds to the cost burden, disturbs the patient’s comfort and increases the risk of stroke.
Risk factors for atrial fibrillation include acute atrial changes occurring at the time of surgery, such as acute atrial enlargement, ischaemia and infarction, hypertension, trauma from cannulation, hypomagnesaemia, inflammation caused by pericarditis, cardiopulmonary bypass and cross-clamp times, pulmonary vein venting and beta blocker withdrawal. Other reported risk factors include pre-existing COPD, cardiomegaly, left atrial enlargement, type of cardioplegia, right coronary artery stenosis and sinus nodal or AV nodal artery disease [2].
Ventricular arrhythmias following cardiac surgery include the more common benign isolated ectopic beats or non-sustained ventricular arrhythmias and the dangerous but fortunately less frequent ventricular tachycardia or ventricular fibrillation [3].
Conditions associated with ventricular arrhythmias after cardiac surgery include haemodynamic instability, electrolyte abnormalities, hypoxia, hypovolaemia, ischaemia and infarction, acute graft closure, reperfusion after cessation of cardiopulmonary bypass, and pro-arrhythmia caused by inotropic and anti-arrhythmic drugs [2].
Numerous preventive as well as therapeutic strategies have been studied and used to combat post cardiac surgery arrhythmias.
Many drugs have been used prophylactically in order to prevent postoperative atrial fibrillation (POAF). Amiodarone, which blocks potassium and calcium channels, and has both alpha and beta blocking properties, has been assessed in multiple trials. It can reduce POAF by 50-70% and evidence suggests that ventricular arrhythmias are also reduced. However, there is concern about possible complications including pro-arrhythmia, sudden respiratory distress or bradycardia requiring pacing. Therefore close monitoring is required [3].
Various approaches have been used to prevent or treat post cardiopulmonary bypass (CPB) reperfusion induced ventricular fibrillation. Lignocaine, an amide local anaesthetic, has been shown to increase the threshold for VF by binding to sodium channels, decreasing the slope of phase 4 depolarization and increasing the threshold potential in Purkinje fibres. The administration of lignocaine two minutes before the release of aortic cross clamp not only decreased the incidence of reperfusion ventricular fibrillation, but also increased the cardiac output. Another approach to prevent VF has been the use of magnesium sulphate. The prophylactic use of magnesium after cardiac surgery was better than placebo in reducing the risk of atrial fibrillation, supraventricular and ventricular arrhythmias. The cardiac protective effects of magnesium are induced by the activation of the Na+ K+ ATPase, which stabilizes the membrane potential, and thereby raises the ventricular fibrillation threshold [3].
The aim of this study is to compare the effect of a single prophylactic dose of amiodarone to a dose of lignocaine and magnesium sulphate to placebo on the overall incidence of arrhythmias in patients undergoing valve replacement surgery following the release of aortic cross clamp.
After getting approval from institutional ethics committee and obtaining written informed consent from each of the patients, this prospective, double blind, parallel group, randomized study was conducted in the CTVS OT and postoperative ICU in IPGME&R/SSKM Hospital, Kolkata in 60 patients of either sex, 15-65years of age undergoing elective valve replacement surgery.
Sixty (60) patients aged between 15 to 65 years of either sex were included in the study .The patients were divided into 3 groups: Group 1, 2 and 3 by a computer generated randomization chart. Patients who refused, had any contraindication or allergy to the study drugs, patients taking any of the study drugs in the previous 4 months or taking any drugs known to have significant interactions with the study drugs (e.g. phenytoin, cyclosporine or cholestyramine) were excluded from the study. Group1 (n= 20) received normal saline; Group 2 (n=20) received 3mg/kg of amiodarone; Group 3 (n=20) received 1.5mg/kg of lignocaine and 40mg/kg of magnesium sulphate just before the release of aortic cross clamp in the venous reservoir of the pump.
Written informed consent was obtained from all the patients prior to including them in the study during the pre-anaesthetic visit. Complete pre-anaesthetic evaluation was performed in each patient including detailed history taking, thorough physical examination, airway examination and routine preoperative investigation.
The preoperative left atrial size was measured using M-mode transthoracic echocardiography in parasternal long axis view. Beta blockers and calcium channel blockers and digoxin, if prescribed for rate control, were continued on the day of surgery. All the patients were premedicated with 0.1mg/kg of midazolam intravenously prior to induction.
In the operation theatre electrocardiography, pulse oximetry and non-invasive blood pressure monitoring were commenced. After establishing intravenous cannula and arterial line, general anesthesia was induced by the following drugs intravenously- 5μg/kg of fentanyl, 5mg/kg of thiopentone, 1.2mg/kg of rocuronium. Trachea was intubated with an endotracheal tube of appropiate size. Anaesthesia was maintained with incremental doses of fentanyl, midazolam, isoflurane and vecuronium. The right internal jugular vein was cannulated with a triple lumen central venous catheter. The pulmonary artery pressure was measured directly before going on pump with the help of the surgeon.
Heparin 4mg/kg was administered intravenously to achieve adequate anticoagulation with activated clotted time ≥ 480 seconds. The valve replacement surgery was performed under CPB with mild hypothermia. The CPB circuit was primed with Ringer’s lactate solution, sodium bicarbonate, mannitol and heparin. Haematocrit was maintained between 21 and 28% during CPB. Myocardial protection was achieved by antegrade cold cardioplegia (at 4⁰C, St. Thomas’ solution based crystalloid) after aortic cross clamping and cardioplegia was repeated every 20 minutes. As per Institutional protocol, nitroglycerine 0.5μg/kg/min and dopamine 5μg/kg/min were started at the onset of rewarming. Serum potassium levels were optimized to 4-4.5 mEq/L to minimize arrhythmias induced by hypo/hyper- kalemia. Group 1 patients received normal saline, group 2 received 3mg/kg of amiodarone and group 3 received 1.5mg/kg of lignocaine and 40 mg/kg of magnesium sulphate just before the release of the aortic cross clamp. The drug was prepared according to a computer generated randomization sheet by an anaesthesiologist not involved in the study for the sake of blinding. All the study drugs or placebo were added to the reservoir.
Initial rhythm after the release of aortic cross clamp was noted. When AF was detected cardioversion was attempted with internal paddles with stepwise increase in energy output. When the heart rate was less than 60/min atrial pacing (epicardial) was initiated. If the patient had VF/VT, it was treated with internal defibrillation with stepwise increase in energy upto 50J. If the patient had atrio-ventricular block, AV sequential pacing was initiated. Adrenaline was added for inotropic support to treat persistent hypotension despite 10μg/kg/min of dopamine infusion. Aorta was decannulated after reversal of residual action of heparin by administration of protamine sulphate intravenously. After surgical closure the patients were transferred to the postoperative ICU and monitored for the occurrence of any arrhythmias for a 24 hour period. Arrhythmias were treated as and when they occurred. The study ended after 24 hours of postoperative period.
Statistical Analysis
The software used for statistical analysis was Statistica version 6 [Tulsa, Oklahoma: StatSoft Inc., 2001]. Sample size was calculated on the anticipated incidence of spontaneous return to normal sinus rhythm following release of aortic cross clamp. Assuming, based on published literature7 that 46% of patients in the placebo group will not demonstrate spontaneous return to normal sinus rhythm it was calculated that 19 subjects would be required per group for a 20% reduction in proportion of patients not returning to sinus rhythm with 80% power and 5% probability of type I error.
The numerical variables which were normally distributed were : age, body weight, pre- and post-operative LA size, pre-operative pulmonary artery pressure, duration of CPB, aortic cross clamp time, total duration of surgery, pO2, pCO2, K+ and all other lab parameters (Hb%, FBS, urea, creatinine) and they were compared between the three groups using one way ANOVA. The numerical variables which were not normally distributed included: ejection fraction, drug doses, defibrillation energy required, duration of pacing, duration of intubation, ICU stay and they were compared between the three groups using Kruskal-Wallis ANOVA. The categorical variables were compared using the Chi- Square test.All statistical analyses were two-tailed and p <0>
The three groups were comparable with respect to all baseline variables including age, body weight, sex, NYHA class, haemoglobin, fasting blood glucose, blood urea and serum creatinine, pre- and post-operative LA size, pre-operative pulmonary artery pressure and ejection fraction. (Table-1)
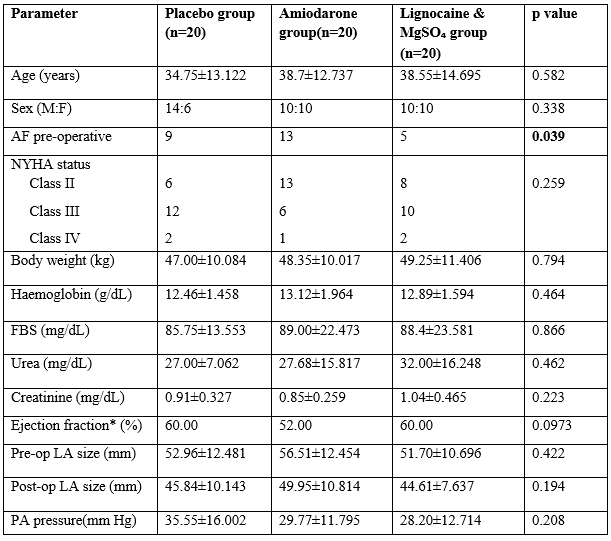
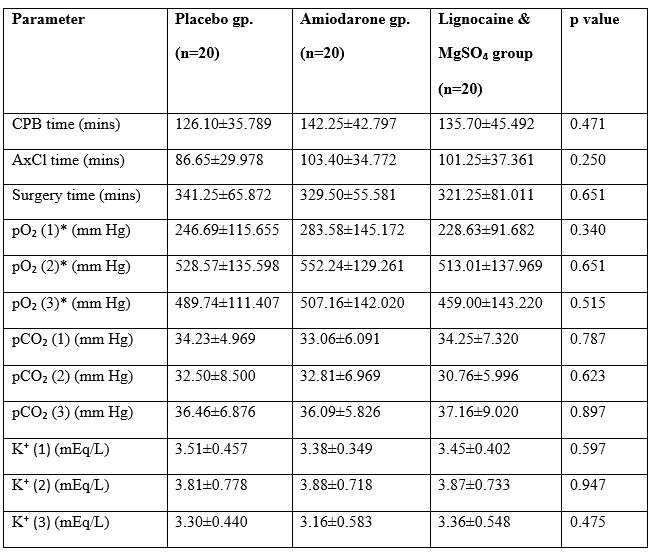
The groups were also comparable with respect to intraoperative factors which might have affected outcome including CPB, aortic cross clamp and surgical durations, pO₂, pCO₂ and K⁺ concentrations just after induction, after weaning from CPB and just after surgery (Table-2).
However, statistically significant differences (p value = 0.039) were noted between the three groups in the presence of pre-operative atrial fibrillation which may have affected the outcome (Table-1).
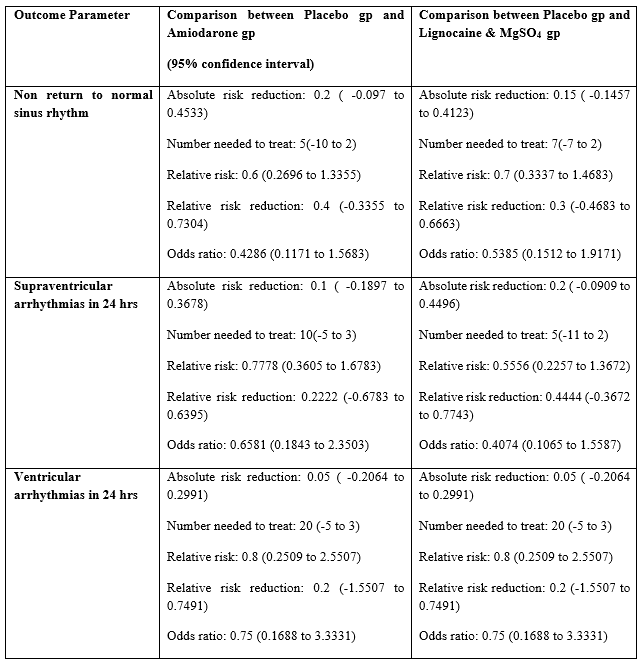
Spontaneous return to normal sinus rhythm after removal of the aortic cross clamp, without the need for pacing or defibrillation was seen in 10[0.5{95% C.I- 0.2993 to 0.7007}] out of 20 patients of the placebo group, 14 patients [0.7{95% C.I- 0.4810 to 0.8545}] of the amiodarone group and 13 patients [0.65{95% C.I- 0.4329 to 0.8188}] of the lignocaine and magnesium sulphate group. However, these differences were not statistically significant (p value = 0.399) (Table-3).
The incidence of supraventricular arrhythmias within 24 hours in the three groups were- 9 patients [0.45{95% C.I- 0.2582 to 0.6579}] of the placebo group, 7 patients [0.35{95% C.I- 0.1812 to 0.5671}] of the amiodarone group, 5 patients [0.25{95% C.I- 0.1119 to 0.4687}] of the lignocaine and magnesium sulphate group. These differences were statistically insignificant (p value =0.415) (Table-3). The incidence of ventricular arrhythmias within 24 hours of surgery was 5 patients [0.25{95% C.I- 0.1119 to 0.4687}] in the placebo group, and 4 patients [0.2{95% C.I- 0.0807 to 0.4160}] each in the amiodarone group and lignocaine and magnesium sulphate group. These differences were also statistically insignificant (p value =0.906) (Table-3).
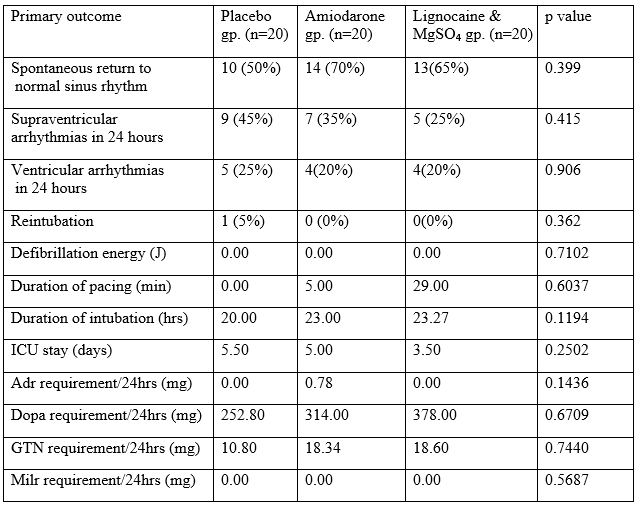
No statistically significant differences were also found between the three groups with respect to defibrillation energy requirement, pacing duration, duration of intubation and ICU stay (Table-3). Reintubation was required in only one patient in the placebo group (Table-4).
Atrial fibrillation is the most common arrhythmia encountered postoperatively following cardiac surgeries under cardiopulmonary bypass. Ventricular tachyarrhythmias after reperfusion following CPB, though fortunately less common are more dangerous. Amiodarone, lignocaine and magnesium sulphate have all been individually shown to be effective in the prevention of postoperative arrhythmias. While amiodarone and magnesium sulphate have been proved to be effective against both supraventricular and ventricular arrhythmias, lignocaine is primarily effective against ventricular arrhythmias [1].
There have been many trials to demonstrate the efficacy of amiodarone in preventing postoperative atrial fibrillation as well as ventricular tachyarrhythmias. Mitchell et al in the PAPABEAR trial compared oral amiodarone (10mg/kg/day) for 6 days prior to surgery to placebo. Amiodarone significantly reduced (p<0>
MT Moeen Vaziri et al, studied 76 patients undergoing CABG, comparing the effect of prophylactic lignocaine to magnesium sulphate and normal saline in preventing ventricular fibrillation. They found that both lignocaine and magnesium sulphate decreased the incidence of ventricular fibrillation, magnesium sulphate more than lignocaine [6].
O. Tiryakioglu et al studied 192 patients undergoing CABG surgery. They compared magnesium sulphate given intravenously 12 hours prior to operation, immediately following the operation, and on postoperative days 1, 2 and 3 to a preoperative infusion of amiodarone (1200 mg) on first postoperative day followed by oral amiodarone (600mg/day), to normal saline inthe control group during the same time periods. This study found that prophylactic amiodarone for total (both ventricular and supraventricular) arrhythmias was significantly more effective than magnesium sulphate (p=0.015). There was no difference between the two drugs in preventing supraventricular arrhythmia (p=0.026) [1].
S.Kar et al studied 56 patients undergoing valve replacement surgery and compared the prophylactic efficacy of a single preoperative dose of amiodarone to placebo. They found that amiodarone significantly decreased the incidence of atrial fibrillation (p=0.035), ventricular fibrillation (p=0.089) and increased the incidence of spontaneous reversion to normal sinus rhythm after cross clamp release (p=0.002) [7].
Ayoub CM et al compared amiodarone to lignocaine and placebo, given 2 minutes before cross clamp release for prevention of ventricular fibrillation in 120 patients undergoing CABG.The study showed no difference between amiodarone and placebo in prevention of ventricular fibrillation after release of aortic cross clamp. In addition, the use of lignocaine was able to reduce the incidence of ventricular fibrillation as compared to both amiodarone and placebo [8].
In a similar study comparing amiodarone, lignocaine and placebo William J. Hauermann et al found that neither amiodarone nor lignocaine reduced the incidence of ventricular fibrillation in patients undergoing a variety of cardiac surgeries. However, amiodarone was shown to reduce the number of shocks required to terminate a ventricular fibrillation [9].
Another study by A A Ghavidel et al comparing amiodarone, lignocaine and placebo on 150 patients showed no significant difference in the incidence of VF after aortic cross clamp release between groups [10].
In our study however, there was no significant difference in the rate of spontaneous reversion to sinus rhythm between the placebo, amiodarone, lignocaine and magnesium sulphate groups. Neither was any difference seen in the incidence of atrial fibrillation or ventricular arrhythmias within 24 hours. Amiodarone and lignocaine and magnesium sulphate also failed to show any significant advantage over placebo in terms of decreasing the defibrillation energy requirement, duration of pacing, intubation and hospital stay in our study. Though similar findings were reported by William J Hauermann et al and A A Ghavidel et al, majority of the studies show amiodarone, lignocaine and magnesium sulphate to be effective against postoperative arrhythmias. However, in our study we have used a single dose of the agents just before the release of cross clamp, whereas most studies have used different regimens of the study drugs. Another fallacy of our study was that despite randomization, a significant difference in the incidence of pre-existing atrial fibrillation crept between the groups which may have affected the outcome.
A single prophylactic dose of amiodarone or lignocaine and magnesium sulphate did not decrease the incidence of atrial fibrillation or ventricular arrhythmias or increase the rate of spontaneous reversion to normal sinus rhythm in patients undergoing valve replacement surgery.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.

Clinical Cardiology and Cardiovascular Interventions, we deeply appreciate the interest shown in our work and its publication. It has been a true pleasure to collaborate with you. The peer review process, as well as the support provided by the editorial office, have been exceptional, and the quality of the journal is very high, which was a determining factor in our decision to publish with you.

The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews journal clinically in the future time.

Clinical Cardiology and Cardiovascular Interventions, I would like to express my sincerest gratitude for the trust placed in our team for the publication in your journal. It has been a true pleasure to collaborate with you on this project. I am pleased to inform you that both the peer review process and the attention from the editorial coordination have been excellent. Your team has worked with dedication and professionalism to ensure that your publication meets the highest standards of quality. We are confident that this collaboration will result in mutual success, and we are eager to see the fruits of this shared effort.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, I hope this message finds you well. I want to express my utmost gratitude for your excellent work and for the dedication and speed in the publication process of my article titled "Navigating Innovation: Qualitative Insights on Using Technology for Health Education in Acute Coronary Syndrome Patients." I am very satisfied with the peer review process, the support from the editorial office, and the quality of the journal. I hope we can maintain our scientific relationship in the long term.

Dear Monica Gissare, - Editorial Coordinator of Nutrition and Food Processing. ¨My testimony with you is truly professional, with a positive response regarding the follow-up of the article and its review, you took into account my qualities and the importance of the topic¨.

Dear Dr. Jessica Magne, Editorial Coordinator 0f Clinical Cardiology and Cardiovascular Interventions, The review process for the article “The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery” was extremely rigorous and detailed. From the initial submission to the final acceptance, the editorial team at the “Journal of Clinical Cardiology and Cardiovascular Interventions” demonstrated a high level of professionalism and dedication. The reviewers provided constructive and detailed feedback, which was essential for improving the quality of our work. Communication was always clear and efficient, ensuring that all our questions were promptly addressed. The quality of the “Journal of Clinical Cardiology and Cardiovascular Interventions” is undeniable. It is a peer-reviewed, open-access publication dedicated exclusively to disseminating high-quality research in the field of clinical cardiology and cardiovascular interventions. The journal's impact factor is currently under evaluation, and it is indexed in reputable databases, which further reinforces its credibility and relevance in the scientific field. I highly recommend this journal to researchers looking for a reputable platform to publish their studies.

Dear Editorial Coordinator of the Journal of Nutrition and Food Processing! "I would like to thank the Journal of Nutrition and Food Processing for including and publishing my article. The peer review process was very quick, movement and precise. The Editorial Board has done an extremely conscientious job with much help, valuable comments and advices. I find the journal very valuable from a professional point of view, thank you very much for allowing me to be part of it and I would like to participate in the future!”

Dealing with The Journal of Neurology and Neurological Surgery was very smooth and comprehensive. The office staff took time to address my needs and the response from editors and the office was prompt and fair. I certainly hope to publish with this journal again.Their professionalism is apparent and more than satisfactory. Susan Weiner

My Testimonial Covering as fellowing: Lin-Show Chin. The peer reviewers process is quick and effective, the supports from editorial office is excellent, the quality of journal is high. I would like to collabroate with Internatioanl journal of Clinical Case Reports and Reviews.

My experience publishing in Psychology and Mental Health Care was exceptional. The peer review process was rigorous and constructive, with reviewers providing valuable insights that helped enhance the quality of our work. The editorial team was highly supportive and responsive, making the submission process smooth and efficient. The journal's commitment to high standards and academic rigor makes it a respected platform for quality research. I am grateful for the opportunity to publish in such a reputable journal.

My experience publishing in International Journal of Clinical Case Reports and Reviews was exceptional. I Come forth to Provide a Testimonial Covering the Peer Review Process and the editorial office for the Professional and Impartial Evaluation of the Manuscript.
