
Research Article | DOI: https://doi.org/10.31579/2641-0427/013
1 Department of Orthopaedic Surgery, University of Leuven, Pellenberg, Belgium.
*Corresponding Author: Jaxon Dawson,Department of Orthopaedics, La Rabta Teaching Hospital Center, Tunis, 1007, Tunisia.
Citation: Jaxon Dawson, Drew Brody. (2018). “Zoledronate and ibandronate treatments provide a significant improvement in BMD values in osteoporosis patients”, J. Orthopaedics and Surgical Sports Medicine. 1(3); Doi:10.31579/2641-0427/013
Copyright: © 2018 Jaxon Dawson. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 October 2018 | Accepted: 26 October 2018 | Published: 13 November 2018
Keywords: osteoporosis, treatment, zoledronat, ibandronat, effectivity, side effects
Objective: In this study, we aimed to make a comparative analysis of short term clinical effectivity and side effects of intravenous zoledronate administration as single dose yearly and intravenous ibandronate administration as four doses per year.
Methods: The patients whom were included in our study had osteoporosis according to WHO criteria and were treated with either parenteral zoledronate or ibandronate. 43 patients were treated with single dose of 5mg intravenous zolendronat which was applied once in a year; whereas in 39 patients were treated with 3 mg intravenous ibandronate which was applied four times in a year in three months intervals. Biochemical tests were performed in all patients before intravenous drug infusion. Side effects during drug administration and also in the first three months of the treatment were noted for all patients. Clinical effectivity was analyzed according to changes in bone mineral density (BMD) at the end of two year after treatment.
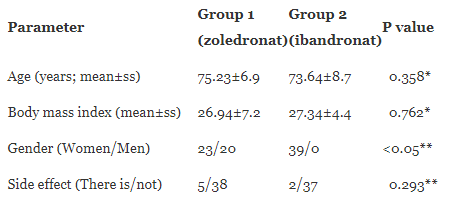
Results: Eighty-two patients who were followed-up and evaluated for the effectivity and side effects of the treatment were included in our study. The compliance of patients were 100% in both groups. Mean age was 75.23±6.9 years and mean body mass index (BMI) was 26.94±7.2. In zoledronate group in which there were 23 females and 20 males. Mean age was 73.64±8.7 years and mean BMI was 27.34±4.4. In ibandronate group in which there were 39 females. There were no statistically significant differences between the groups in terms of gender (p=0.000) Mean age, BMI and rate of diagnosed side effects were not statistically significant in between the groups. According to a one-year follow-up in both groups comparison with before application had a statistically significant increase in BMD (p<0.01). However, a one-year follow-up between the two groups in terms of mean values of bone mineral density did not differ significantly (p>0.05).
Conclusion: Choice of medical treatment is decided according to bone mineral density and personal risk factors in osteoporosis. Parenteral agents in the treatment of osteoporosis may be the preferred choice for the patients with comorbid diseases, using multiple drug therapies, or having trouble in using oral drug therapy. However, it should always be kept in mind that drug related side effects may be seen more commonly with parenteral agents. Clinicians should be aware of the probable side effects during and after application.
Osteoporosis (OP) is a systemic metabolic bone disease which is characterized by low bone mass and deterioration of bone micro-architecture, resulting in increased susceptibility to fractures [1]. The world health organization (WHO) reported that nearly 30% of women over 50 years of age have osteoporosis and increased risk of fractures, while one eighths of men carry risk of fracture [2]. Femoral neck fractures related to vertebral and distal radius fractures are most commonly observed in patients with osteoporosis [3]. Applications for prevention, diagnosis and treatment of OP may prevent fractures and its sequellae [4]. However, today, a completely safe, effective and generally accepted treatment for OP has not been defined yet [5].
Medications preventing bone resorption or increasing bone formation are used alone or in combination during the treatment [6]. Bisphosphonates (BF), which are widely used in the treatment of osteoporosis, are connected to hydroxyapatite in bone, provide resistance to the action of pyrophosphatases, reducing bone resorption [7]. In addition, they show action by changing the properties of the bone matrix responsible for the activation of osteoclasts, affecting the formation of osteoclast from progenitor cells, and by inhibiting the function of mature osteoclasts [7,8]. In the case of oral bisphosphonates, there can be upper gastrointestinal (GiS) side effects, acute phase reaction, hypocalcemia and secondary hyperparathyroidism, musculoskeletal pain, osteonecrosis of the jaw and eye complaints [5,9]. Where as in the case of intravenous bisphosphonates (zoledronic acid, etc.) used to treat osteoporosis, all of the side effects mentioned above may develop, other than upper GiS complaints. Renal toxicity, though less, may develop in the case of zoledronate [5,9].
In this study, the aim was to compare early period side effects and short-term action of a single dose per year of zoledronate administered as an intravenous infusion and ibandronate therapy which is applied 4 times per year.
82 patients admitted to our outpatient orthopedics clinic and diagnosed with osteoporosis according to WHO criteria were included in our study. The patients were asked for getting information about on their age, height, weight, number of pregnancies, smoking and alcohol use, medication use history and whether they have any additional disease or not. Ibandronate is indicated only in using of the treatment, for patients who postmenopausal Osteoporosis or Osteoporotic women in our country. Thus Male Patients were used only Zolendronate. Consequently the patients were not randomized.
Clinical evaluations, radiologic images, blood parameters and bone mineral density measurements of patients for a diagnosis of osteoporosis were recorded. The patients were divided into two groups as the group receiving parenteral zoledronate therapy (Group 1, n=43) and the group receiving ibandronate therapy (Group 2, n=39). 5 mg zoledronate was administered to the patients in Group 1 as an intravenous infusion for 15 minutes once a year, and IV ibandronate was administered to the patients in Group 2 as an intravenous infusion once every quarter of a year under hospital conditions. In order to investigate the effectiveness of treatments applied to these patients with a T-score of -2.5 and below, their bone mineral density (BMD) values were evaluated at the end of a two year follow-up period. Their values before and after drug administration were considered, and any side effects developed during and at the end of treatment were recorded.
Statistical analysis
SPSS 11.0 for Windows (SPSS Inc. Chicago, IL) statistical analysis software was used for the statistical calculations. Normal distribution of our data was evaluated using Kolmogorov-Smirnov test. Afterwards, T-test for comparison of demographic data and the test for the comparison of categorical data were used. On the other hand, Mann-Whitney U test was used for as compared to baseline vertebral and hip BMD and T scores between groups. Wilkonson Signed Rank Test for delta change before-after treatment in groups were used. P values less than 0.05 were considered statistically significant. The results are expressed as the mean±standard deviation or median (25 and 75 percentile).
A total of 82 patients who were observed and questioned about side effects during and at the end of the administration were included in the study, and the mean follow-up time was 26 months. The compliance of patients were 100% in both groups. In group 1 treated with zoledronate, mean age of 43 patients was 75.23±6.9 and their mean body mass index (BMI) was 26.94±7.2. Of these patients, 23 were women (54%) and 20 were men (46%). In group 2 treated with ibandronate, mean age of 39 patients was 73.64±8.7 and their mean BMI was 27.34±4.4. Of all these patients were women. A statistically significant difference was existed between the groups in terms of gender (p=0.000). However, there was no statistical difference in terms of age, BMI and rate of observed side effects (Table 1). In zoledronate group, gastrointestinal system (GIS) side effects were detected in 3 patients and acutephase reaction (APR) was detected in 2 patients, while in ibandronate group, GIS side effects were detected in one patient and side effects including APR were detected in another patient.
Group 1 as compared to baseline vertebral and hip BMD and T scores had improvement significantly after treatment. Likewise Group 2 as compared to baseline vertebral and hip BMD and T scores had improvement significantly after treatment ((Table 2).
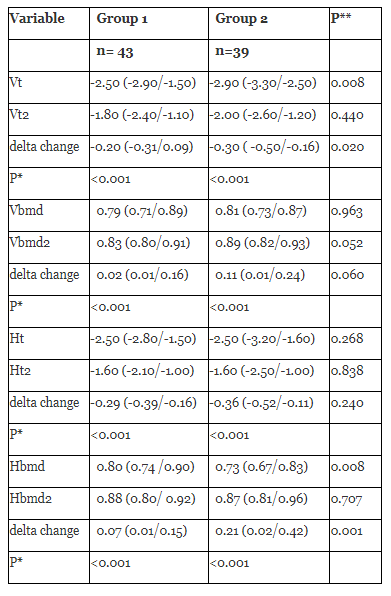
On the other hand, in both groups, as compared to baseline post-treatment vertebral& hip BMD and post-treatment vertebral & hip T scores were not significantly difference between the groups (Table 2).
There was significant difference between groups in compared of Vt delta changes and the amount of improvement was greater in group 2. Also there was significant difference between groups in compared of Hbmd delta changes and the amount of improvement was greater in group 2 (Table 2).
The most widely used method for screening and diagnosis of osteoporosis is the measurement of bone mineral density (BMD) in the hip and lumbar region by central Dual-energy X-ray absorptiometry (DXA). According to WHO diagnostic criteria, -2.5 and below cause a diagnosis of osteoporosis [10,11]. Treatment indications were established by National Osteoporosis Foundation (NOF) as a T-score of -2.5 or below in postmenopausal women and men aged 50 years and above, presence of a hip or vertebral fracture, fracture history in conjunction with low bone density (T score in the range of–1 and –2.5), presence of secondary causes increasing fracture risk related to low bone density, low bone density and a 10- year hip fracture risk of 3% or above or 10-year fracture risk of 20% or above according to FRAX scoring [12,13].
In medical treatment OP; bisphosphonates, strontium, teriparatide, selective estrogen receptor modulator (SERM) and calcitonin are used. Bisphosphonates are the antiresorptive agents which are most commonly used to treat OP and reduce the risk of hip fracture in the elderly patients mostly. Even after bisphosphonates are discontinued, their positive effects on bone are maintained and they are the best agents to prefer in senile and male OP [5,12,14,15]. Based on these, we planned this study to compare the effects and possible side effects on bone mineral density of two bisphosphonate medications used to treat osteoporosis.
Bisphosphonates are safe and well tolerated drugs used in the treatment of osteoporosis and a number of side effects may occur depending on their use. These are usually upper gastrointestinal system (GIS) and acute influenza-like symptoms. Upper gastrointestinal symptoms usually appear during oral bisphosphonate therapy, while temporary influenza-like symptoms frequently appear during IV administration of nitrogen-containing bisphosphonates (pamidronate, ibandronate, zeledronic acid) [16-18]. Eye-related side effects were also reported [19]. In a study in which risedronate was investigated, 3 years after treatment the incidence of GIS side effects was found as 27%, while this percentage was reported as 26% in the placebo group. In the case of 5-year results, it was demonstrated that the placebo group with 13.8% caused greater incidence of GIS side effects compared to the risedronate group with 12.6% [20]. Similar results were also reported for ibandronate in BONE study [21]. On the contrary, in the HORIZON study [22], patients treated with zoledronic acid were reported to suffer from GIS side effects, including nausea (8.5% and 5.2%), vomiting (4.6% and 3.2%), diarrhea (6%, 5.6%), upper abdominal pain (4.6% and 3.1%) and dyspepsia (4.3% and 4%), compared to the placebo group.
Acute phase reaction (APR) is characterized by low-grade fever, myalgia, arthralgia, and headache. This influenza like symptoms generally occur within three days of drug administration and symptoms usually resolve 2-3 days of administration and may last for 7-14 days [16,23]. Symptoms which appear at a rate of 10% after iv administrations may also be observed in oral applications if adequate dosage is reached. In the HORIZON study [24], acute phase reaction symptoms were found significantly high in zoledronic acid group, compared to the placebo group (31.6%, 6.2%, respectively). High BF blood concentrations reached during iv treatments may cause acute renal problems. This effect could not be shown in therapeutical doses of oral BFs [25]. Still, in patients with a creatinine clearance lower than 30 ml/min, it is appropriate for avoiding using either oral or parenteral BF because there isn't enough clinical experience. In studies carried out on the subject, alendronate [26], risedronate [27] and ibandronate [28] were shown to have renal side effects similar to those of placebo. It was reported that mild and transient serum creatinine level appearing on day 9 and 11, resulting from use of zoledronic acid in osteoporosis treatment, is not permanent at the end of 3 years, and that renal side effects are comparable to placebo [9,24]. In a study conducted using 5 mg zoledronate in postmenopausal osteoporosis patients, atrial fibrillation risk was found to be high, however, it was concluded in subsequent studies that such an increased risk does not exist [24,30]. Osteonecrosis of the jaw can be seen in cancer patients while they are using highly dose iv pamidronate or zoledronic acid [9].
In our study, APR-like findings were observed in 3 patients (8%) and GIS side effects were detected in 2 patients (5%) from zoledronate group. While in ibandronate group, GIS side effects were observed in one patient (2.7%) and APRlike side effects were observed in one patient (2.7%), which are less than those in the literature.
Zoledronate is the only FDA-approved agent used to prevent further fractures after an osteoporotic hip fracture. In the HORIZON-PFT study conducted to determine the effects of zoledronic acid in the case of postmenopausal osteoporosis, zoledronic acid was administered to 3881 patients at baseline, 12th and 24th months. The patients were on follow-up for 3 years and compared with placebo group. In that study, new vertebral fractures and hip fractures were considered as the primary endpoint. In zoledronic acid group, morphometric vertebral fracture risk and hip fracture risk decreased by 70% and 41%, respectively within 3 years [31]. HORIZON Recurrent Fracture Study covered patients with a mean age of 74.5 who have undergone surgery for osteoporotic hip fracture in the last 3 months, and rates of having new clinical fracture were taken into consideration as the primary target. The risk of having a new clinical fracture decreased by 35% in the group treated with zoledronic acid within an average of 19 months, compared to placebo. Zoledronic acid treatment also decreased the mortality rate by 28% [24,29]. In a study conducted on glucocorticoid-induced osteoporosis patients, it was observed that zoledronate treatment is more effective than risedronate treatment and it caused a higher increase in lumbar spine BMD after treatment than risedronate treatment. (Zoledronate 4.1%,
Risedronate 2.7%) [32]. In an osteoporosis study by Voskaridou et al., on thalassemia patients, IV 4 mg zoledronate was administered to one group once every 6 months, IV 4 mg zoledronate was administered to another group once every 3 months and placebo treatment was applied to another once every 3 months for 1 year, and the patients who received IV 4 mg zoledronate once every 3 months were found to have higher lumbar spine BMD, whereas no such change was detected in the placebo group [33]. In one study, the patients who were followed-up with daily oral ibandronate of 2.5 mg were found to have a 52% reduced vertebral fracture risk and a 6.5% increased lumbar spine BMD [34]. In a DIVA (Dosing IntraVenous Administration) study, similar increase was observed in the case of double IV ibandronate treatment (3mg once every 3 months, 2mg once every 2 months) compared to baseline lumbar BMD (5.1% and 4.8%), and an increase of 3.8% was observed in lumbar BMD with daily oral 2.5 mg ibondronate treatment compared to baseline values [35]. In our study, in both groups as compared to baseline vertebral and hip BMD and T scores had improvement significantly after treatment (Table 2), and these values are similar to those reported in the literature.
We could not find any certain knowledge on the literature and also there is no consensus about how to follow up? And especially how and/or what way to measure the affectiveness of treatment? How much change is required for clinical significance? [11,14,36-46]. In the study, patients receiving bisphosphonate treatment causing a decline in BMD have a higher for osteopotic fracture risk compared with patients whose BMD increases [36]. In another study, It is reported that causes significant changes in fracture risk, even a small difference like as -0.225 on the basis of T-score [37]. In our study, delta changes for vertebral and hip T-score were in the range between 0.20-0.36 vertebral in both groups. Also delta changes for vertebral and hip BMD were in the range between 0.02- 0.21 in both groups (Table 2).
BMD and T-score in the assessment of osteoporotic fracture risk is important. However, it is not enough. When calculating the risk of fracture not only BMD but also bone turnover, bone architecture, bone strength as well as other factors must be considered. Osteopenic patients are at risk, such as patients with osteoporosis [38-40]. Current diagnosis and treatment decisions for osteoporosis must be depended on the fracture risk calculated based on the results of comprehensive diagnostic procedures [38,41,42]. Monitoring the effectiveness of osteoporosis treatment presents a challenge in everyday clinical practice. In general, the efficacy of the therapy is evaluated by comparing pre and post treatment BMD and/ or T-score. As an alternative, BMD and T-score along with other parameters such as biochemical markers of bone turnover can be used to assess effectiveness of treatment in the osteoporotic patients [39,43-45]. In our study, we can mention reduced osteoporotic fracture risk because it's a significant improvement after treatment compared to before treatment in both groups.
It was demonstrated in this study that zoledronate and ibandronate treatments provide a significant improvement in BMD values in osteoporosis patients and there is no significant difference between their efficacies and side effects. Parenteral treatment of osteoporosis is considered as a treatment option that provides high patient compliance in elderly osteoporotic patients with comorbid diseases taking several medications, and precautions should be taken against any side effects that may occur during and after intravenous administration.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
