
Research Article | DOI: https://doi.org/10.31579/2767-7370/030
1 Nimni-Cordoba Tissue Engineering and Drug Discovery Lab, Department of Surgery, Keck School of Medicine of University of Southern California.
2 Department of Oncology, National Children Hospital of Vietnam.
3 Department of Traumatology, National Institute of Ophthalmology of Vietnam.
4 Department of Surgery, 198 Hospital of Vietnam.
5 Natural Health Medical Center.
6 Thai Minh Pharmaceutical jsc.
*Corresponding Author: Ba X Hoang, Nimni-Cordoba Tissue Engineering and Drug Discovery Lab, Department of Surgery, Keck School of Medicine of University of Southern California.
Citation: Ba X Hoang, Bo Han, Hau D Tran , Cuong Hoang, Truong N Pham, et all. (2022). Zinc Iodide-Dimethyl Sulfoxide Composition in Treatment of Chronic Respiratory Diseases. J New Medical Innovations and Research, 3(1); DOI:10.31579/2767-7370/030
Copyright: © 2022, Ba X Hoang. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 September 2022 | Accepted: 15 September 2022 | Published: 26 September 2022
Keywords: zinc; iodide; dimethyl sulfoxide; dmso; asthma; copd; pulmonary fibrosis
Zinc iodide and dimethyl sulfoxide (ZIDS) are well-characterized pharmaceutical agents that have been used in the treatment of different acute and chronic diseases. This report presents observational retrospective clinical evidence of using ZIDS for treating respiratory conditions including asthma and chronic obstructive pulmonary disease (COPD). Although our current report summarizes a series of anecdotal clinical cases, the clinical evidence suggests a possible application of ZIDS as a safe, inexpensive, and potentially effective therapy that can mitigate the symptoms and reduce the morbidity-mortality of patients with chronic respiratory diseases. Given that ZIDS comprises accepted pharmaceutical agents used in practical medicine, possible research and application of this therapeutic composition could potentially open up a new perspective avenue for the treatment of acute and chronic respiratory diseases that have been grown worldwide for the last decades.
SpO2 : peripheral capillary oxygen saturation
DMSO : Dimethyl Sulfoxide
COPD : chronic obstructive pulmonary disease
ZIDS : Zinc iodide and dimethyl sulfoxide
Chronic respiratory diseases such as chronic obstructive pulmonary disease and asthma, and interstitial lung disease are the most common non-communicable diseases worldwide [1]. Chronic respiratory diseases have received proportionately less public attention and less research funding than other diseases such as cardiovascular disease, cancer, stroke, diabetes, and Alzheimer's disease [2, 3]. COPD continues to be a significant medical problem and is the third leading cause of death in the United States. Acute bronchitis and acute exacerbations of COPD are among the most common illnesses encountered by family physicians and account for more than 14 million physician visits annually. The mortality rate of hospitalized COPD patients because of acute exacerbation is about 10% [4]. The circumstances mentioned above indicate that exploring a more effective, safe, and less expensive approach targeting the prevention and treatment of chronic respiratory diseases is crucial and imperative for global health.
Asthma, COPD, and other chronic respiratory diseases are characterized by chronic inflammation and tissue remodeling of the airways. Remodeling is resistant to pharmaceutical therapies. Our published study reported that zinc and methylsulfonylmethane (organic sulfur compounds) potentially prevent airway wall remodeling in asthma by inhibiting both the Erk1/2 and mTOR signaling pathways [5]. In our prior publication, we have also proposed a possible application of Zinc Iodide -Dimethyl Sulfoxide (ZIDS) composition to treat the respiratory symptoms and complications in patients with COVID-19 [6].
In this retrospective observational study, we have followed up, analyzed, and reported a series of anecdotal cases of patients with chronic respiratory diseases who have been treated with ZIDS composition in adjunction to the standard of care treatment.
ZIDS composition (water solution of 30% DMSO pharmaceutical grade and 0.2% of Zinc Iodide) has been developed in the Nimni-Cordoba Tissue Engineering and Drug Discovery Laboratory of the Department of Surgery, Keck School of Medicine of the University of Southern California, in cooperation with Thai Minh Pharmaceutical Company. ZIDS has been tested for acute and chronic toxicity, skin and mucosal irritation, and thyroid toxicity by the Pharmacology Department of the National Institute of Drug Quality Control of Vietnam. The testing results showed an excellent safety profile and tolerability.
Patients were asked to give their consent to participate in the trial. Patients have the right to withdraw from the study at any time and for any reason. The study is a retrospective and observational study that had no approved protocol.
Observational clinical evidence
Observation 1:
Eight moderate to severe asthmatics (5 men and 3 women) aged 28–74 years old were treated with 10 ml of ZIDS mixing with 200 ml of water, three times daily orally in 2 hours after meals for 60 days. These patients have been diagnosed with asthma and have had anti-asthmatic drugs for 6–21 years. The patients presented with episodes of dyspnea, excessive mucus expectoration, coughing, wheezing, or chest tightness more than four times a week and woke up at night with asthma symptoms more than four times a week. The patients took moderate and high doses of medications defined as at least 1,800 mcg of β2-agonists (short-acting or equivalent of long-acting) per week and inhaled corticosteroids (400–2000 µg/day) of beclomethasone dipropionate or equivalent. Their morning peak expiration flow (PEF) was less than 84% predicted as the baseline. Two patients were on oral corticosteroid in the form of prednisolone: 10 mg and 20 mg per day. Results of the treatment with ZIDS in adjunction with a standard of care are summarized and recorded in a diary card of symptoms, PEF, medication use, and quality of assessment life.
The patient’s records were analyzed retrospectively and compared with the baseline data. All patients were followed for 60 days, evaluated every week for the first month and every two weeks for the second month of therapy with oral administration ZIDS solution. The mean PEF of all patients was 72 % as the baseline.
The progression and treatment results of the patients are presented in Table 1.
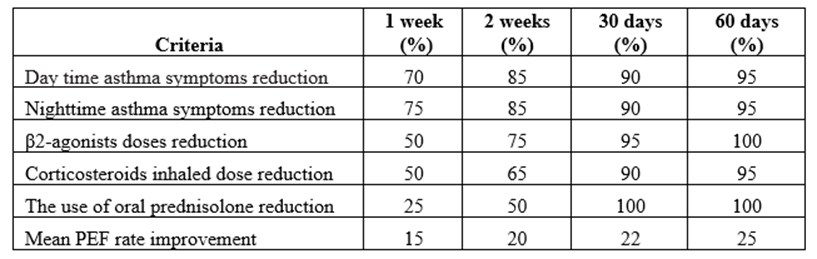
Table 1: Clinical symptoms, treatment doses, and PEF changes at four time points
After one week from the start of the ZIDS oral treatment, the patients recorded a reduction of daytime asthma symptoms by 70% and nighttime symptoms by 75%. Short and long-acting β2-agonists doses had been reduced by 50%. The corticosteroids dose inhaled was decreased by 50%. The usage of oral prednisolone was lowered to 75%. The mean PEF rate improved by 15%, and no additional side effects were recorded. The patients’ blood pressures and pulse rates were within normal ranges.
After two weeks from starting treatment, the daytime and nighttime asthma symptoms were reduced by 85%. The β2-agonist dose was reduced by 75%, the corticosteroid inhaler dose was decreased by 65%, and the usage of oral prednisolone was lowered to 50%, the mean PEF rate improved by 20%, with no side effects observed.
At the end of 30 days, both daytime and nighttime asthma symptoms were reduced by 90%. The β2-agonists use was reduced by 95%, the corticosteroid inhaler dose was reduced by 90%, and the usage of oral prednisolone was terminated. The mean PEF value increased by 22%, and no additional side effects were recorded.
After 60 days of the treatment with ZIDS, the daytime symptoms of asthma reduced by 95%, and nighttime symptoms were reduced by 95%. The β2-agonist use was terminated, and the corticosteroid inhaler was decreased by 95%. The mean PEF increased by 25 %. 6 out of 8 treated patients have reached an asymptomatic and medication-free state.
From the beginning to the end of treatment, there were no additional side effects observed in ZIDS treated patients compared to the baseline level. The mean PEF rate improved after one week, and this trend continued for two weeks, 30 days, and 60 days following the treatment. The patients’ blood pressures and pulse rates improved in 5 of 8 patients after 30 days and 6 of 8 patients after 60 days of treatment with adjunctive ZIDS solution. The general blood count test, general blood chemistry profiles, and thyroid hormone profiles were normal in 30 days and 60 days points of ZIDS treatment. All patients reported improved general health, quality of life, and sleep patterns.
Observation 2:
Seven patients (6 males and 1 female), age range from 45 to 83, with a history of chronic cough and COPD, all presented with episodes of COPD exacerbations. All patients presented with comorbidity, including asthma (2 cases), diabetes (3 cases), hypertension (5 cases), ischemic heart disease (4 cases), pneumonia (1 case), arthritis (3 cases), liver diseases (2 cases), chronic gastritis (5 cases) and stomach ulcers (2 cases).
All patients received treatment with 10 ml ZIDS solution mixed with 200 ml of water three times daily 2 hours after meals at home. The patients were allowed to take all the medications for COPD and comorbidities in the same regimen and doses before exacerbations; no additional medications were added besides the ZIDS solution.
Monitoring clinical changes and paraclinical parameters was performed at three-time points: enrolment day (day 1, baseline), 15 days of the treatment (day 15), and 30 days (day 30) of the treatment with ZIDS in addition to a baseline standard of care. Clinical parameters, including severe cough, dyspnea, sputum secretion, fever, chest tightness, capacity for exercise and activities, sleep quality, and energy levels, were scored based on the modified Medical Research Council Dyspnea Scale (mMRC) questionnaire [7, 8].
Other paraclinical parameters such as general blood count tests, general blood biochemistry profiles, and Pulmonary Function Tests (Spirometry) were recorded. (Table 2)
As shown in Table 2, the patients reported improvement in all symptoms related to COPD exacerbation after 15 and 30 days of therapy with ZIDS in addition to baseline treatment for COPD and comorbidity compared to the baseline.

Table 2: Clinical Changes at Three Time Points (Day- 1, Day-15, and Day- 30)
The mMRC dyspnea scale was used in our study to assess the effectiveness of ZIDS treatment on an individual basis. From a clinical viewpoint, the mMRC scale correlates well to such objective measures as pulmonary function tests [9, 10]. (Table 3)
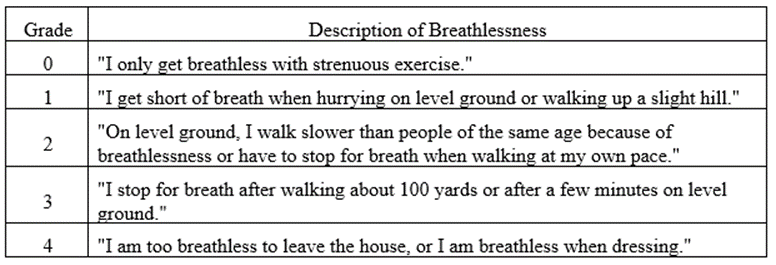
Table 3: Modified Medical Research Council scale (mMRC)
As presented in Table 4, the recorded mMRC scale showed the patients' improvement in functional activities, quality of life, and general health after 15 days and 30 days of treatment with adjunctive ZIDS to baseline treatment for COPD and comorbidity. (Table 4)
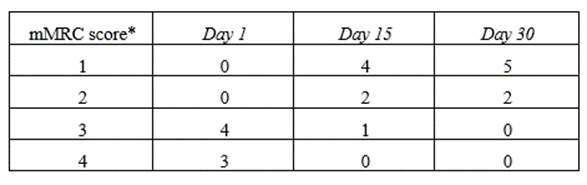
Table 4: Clinical changes at three time points by mMRC scale
The improvement of patients’ pulmonary function compared to baseline with adjunctive SIDS treatment is reported in Table 5.
(Table 5)

Table 5: Functional pulmonary test results
Retrospective analysis of the patients showed that oral ZIDS was effective as adjunctive therapy for COPD exacerbation leading to a fast reduction of the patients’ symptoms, improvement in pulmonary functional parameters, quality of life, and physical function. All these were documented in Tables 2, 4, and 5.
After 30 days of treatment, all seven patients showed an overall improvement; no additional adverse effects were reported in the treated patients compared to the baseline.
Treatments for chronic respiratory diseases are challenging and costly. Currently, none of the approved drugs or treatments can cure asthma, COPD and respiratory complications of autoimmune diseases. Treatments can reduce symptoms and prevent exacerbations; however, the need for life-long administration and severe side effects of the most common anti-inflammatory and symptomatic therapeutic agents are the challenging problems in respiratory medicine.[4, 11-13]
The clinical evidence of our current retrospective study indicated a possible implementation of old and approved pharmaceutical (nutritional) agents such as Zinc, Iodine, and organic sulfur compounds for management of asthma, COPD and other respiratory diseases.
The comprised ingredients' synergic and complex biological properties might produce viable anti-inflammatory, immunoregulatory, antioxidant, antiviral, antibacterial, antifungal, and antifibrotic therapeutic activities that resulted in favorable clinical benefits with a good safety profile of ZIDS composition [6, 14, 15]. ZIDS composes of well-characterized OTC pharmaceutical ingredients with a favorable safety profile. Therefore, it is a significant advantage for developing and applying ZIDS as a repurposed therapeutic product for acute and chronic respiratory diseases since new medications may take many years.
A future well-designed clinical trial is warranted to explore more potential therapeutic activities of ZIDS and promote a possible wider application of this potential therapeutic composition for the management of respiratory diseases.
The current observational retrospective study results demonstrate that ZIDS might effectively treat respiratory diseases. More extensive control trials will be needed to confirm the study findings.
None of the authors declares a conflict of interest regarding the data presented in this publication.
This study was investigators initiated and non-funded.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
