
Case Report | DOI: https://doi.org/10.31579/2690-8808/142
1 Corneal Surgery and External Eye Disease
2 General Practitioner: Airlangga University
*Corresponding Author: Ucok P. Pasaribu, Corneal Surgery and External Eye Disease (Singapore National Eye Center, Singapore).
Citation: Ucok P. Pasaribu, Kukuh Prasety. (2022) Clinical features of systemic lupus erythematosus-related interstitial lung disease-a clinical retrospective study J. Clinical Case Reports and Studies 3(10); DOI: 10.31579/2690-8808/142
Copyright: © 2022 Ucok P. Pasaribu, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 August 2022 | Accepted: 22 October 2022 | Published: 26 November 2022
Keywords: yamane scleral fixation; single pass four throw; aphakia; secondary IOL; pupilloplasty
Purpose: This is a report of an aphakia case without posterior capsular support and iris support. We did a Yamane scleral fixation combined with single pass four throw pupilloplasty.
Case report: A-56 year-old male with a history of complicated phacoemulsification and glaucoma came with a diagnosed of aphakia and angle closure glaucoma. There were no posterior capsular support and iris support so that in this case iris claw secondary IOL cannot be done. We performed Yamane scleral fixation secondary IOL in this case followed by single pass four throw technique pupilloplasty. Post operative uncorrected visual acuity was 0.5 without any complain of quality of vision including glare. Intraocular pressure was within normal limit with topical medication.
Conclusion: Yamane scleralfixation secondary IOL implantation combinedwith single pass four throw pupillopasty can be considered on aphakia patient without both posterior capsular support and iris support.
Implantation of intra-ocular lenses (IOL) following cataract surgery has become standard for achieving optimal vision after surgery. The success of IOL implantation is determined by the integrity of the capsules during cataract surgery. Posterior capsule tear is one of intra-operative complications that makes operator impossible to put IOL in the right place. From the literature, it was found that the incidence of posterior capsule tears varied from 0.18% to 23.3%. [1,2] The absence of support from posterior capsule integrity made IOL implantation is rather difficult. Several techniques are currently being developed to overcome this problem. It was started with the use of open loop posterior IOL which was sutured on the iris and on sclera whose efficacywas reviewed by AAO in 2007 [3]. Onthe same year, Agarwal et al [4] introduced the technique of open loop posterior
IOL fixation using fibrin glue on sclera that closed by conjungtiva. Though the advent of the scleral-sutured IOL dramatically improved rates of corneal endothelial cell loss and uveitis-glaucoma-hyphema syndrome compared to anterior chamber intra-ocular and iris-fixated lenses, the glued IOL technique provided further advantages over suture fixation [5]. Previous study showed that postoperative inflammation and postoperative glaucoma found to be less in glued technique compared to scleral sutured technique.5 Although the glued IOL technique is a promising method of scleral fixation, it is not immune to s ignificant postoperative complications; specifically, haptic extrusion can result from factors including poor scleral tunnel construction, slipping of the IOL haptic from the scleral tunnel, inadequate scleral flap formation, insufficient scleral flap adherence, or fragility of the scleral wall secondary to the patient's history (e.g., Ehlers-Danlos syndrome, scleritis, ocular trauma, surgeries, or exposure to mitomycin-C) and like suture exposure, haptic exposure poses a risk of infection/ endophthalmitis [6].
Dr. Shin Yamane introduced new technique of scleral fixation of IOL with trans- conjungtival approach withoutusing any suture or glue on 2016: The flanged IOL fixation with a double-needle technique. Two needles are bent in line with the bevel to a length approximately the distance from the sulcus to the pupil center. A three-piece IOL is inserted into the anterior chamber using an injector, making sure the trailing haptic is kept external to the incision. An angled sclerotomy is then made through the conjunctiva using a thin- walled 30-gauge needle 90° from the incision where the lens is inserted, 2 mm posterior from the limbus. When it enters the sulcus, the needle is directed toward the leading haptic, which is threaded into the needle using an intraocular forceps. With the haptic secure, a second sclerotomy is made with the second thin-walled 30-gauge needle 180° from the first sclerotomy. The trailing haptic is threaded into the lumen of the second needle. Once both haptics are docked and the lens is found to be centered, both haptics are externalized onto the conjunctiva. Haptics then cauterized to create a triangular flange with a diameter of 0.3 mm. The flange of each haptic is tucked through the conjunctiva and fixedinto the scleraltunnels [7]. Though IOL tilt and decentration are potential complications of the Yamane technique, review of the literature did not reveal any cases of haptic extrusion. One reasonable explanation for this is that thereis very littlehaptic exposed in the flange, making extrusion less likely. Though considering the relatively recent birth of this technique for IOL scleral fixation, we are lacking in the long-term data [8]. Single pass four throw techniqueis a pupilloplasty technique wherein the suture forms a hellical structure of thread that pressed across itself and holds the damaged iris tissue firmly. This technique firstly described by Agarwal as a modification of Siepsier methods. n this technique, a 10-0 or a 9-0 polypropylene suture attached to a long arm needle is passed through the proximal iris tissue that is to be involved in the pupil reconstruction. A 26 G needle is introduced from the paracentesis in the opposite direction, where it engages the distal iris tissue to be approximated. The 10-0 needle is then passed in to the barrel of the 26 G needle, before it is withdrawn from the eye. A Sinskey’s hook withdraws the loop of the suture and the suture end is passed from the loop four times, thereby taking four throws. Both the sutureends are pulled, and the loop slides inside the eye, thereby approximating the pupillary edges together. A micro-scissor is introduced inside the eye and the suture ends are cut. The helicalstructure created due to the loop approximation forms a self-locking and a self-retaining knot inside the eye [9].
In this paper, we described our experience in using both Yamane scleral fixation technique and single pass four throw technique of pupilloplasty on our aphakic and irregular pupil case.
This case of male 56 year-old male with a history of glaucoma and underwent phacoemulsification procedure. He was diagnosed with aphakic that planned for secondary IOL implantation procedure without adequate support of lens capsule and irregular pupil.
First we thought about putting an iris claw IOL in this case but we could not do due to irregularity of the pupil. We decided to do the IOL implantation using Yamane technique first as presented at figure1. We put a marker 2 mm posterior from limbus 180 degress apart for haptic placement. Main incision was made using keratome and three piece non foldable IOL is prepared. A pocket dedicated for haptic is made using 90 degress angled of needle at the marker. IOL then implanted with leading haptic presented firsat at anterior chamber and being catch by
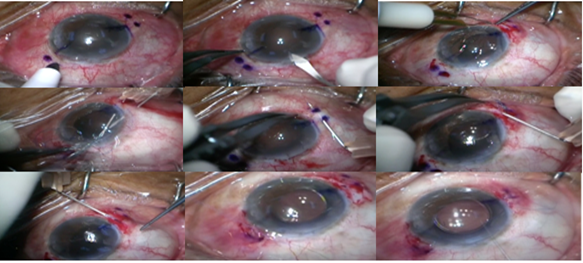
Figure 1: Yamane scleral fixation procedure
the needle and at this point, it is important to make sure that the trailing haptic is outside the eye. A pocket was made using 30G needle after we open the conjungtiva. Using 30G needle guidance, haptic was placed safely inside the pocket. Haptic was then being cauterized using low temperature cauterized to ensure that the position would not change and then closed by the conjungtiva. The same procedure was done to trailing haptic exactly 180 degrees from leading haptic position. The next step was performing single pass four throw pupiloplasty as shown at figure 2.
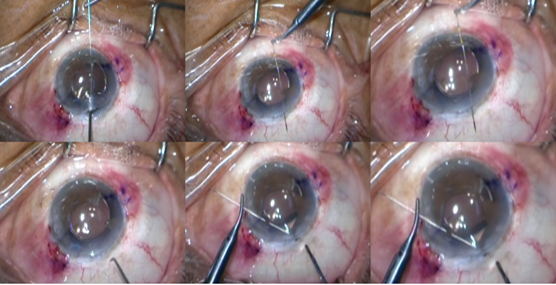
Figure 2: Single pass four throw pupilloplasty
It was started with putting viscoelastic device into the anterior chamber. Forceps was holding the distal part of damaged iris through main incision while 10.0 polyprophylene suture with long needle was passing through the distal part of damaged iris, Introduced the forceps from anotherpart to grasp the proximal part of the damaged iris and presented it to the long needle. Using a sinskey, we grasped the distal part of the suture to make a loop at anterior chamber and then externalized the loop using micrograsper. The knot was the made. The same procedure was done in the other part of the damaged iris. Patient achieved uncorrected visual acuity postoperative 0.5 and not complaining about glare (picture 3). There also no complication was found during the post operative visit. Visual acuity stabil during 2 years post operative visit. He also received glaucoma medication routinely so that post operative intraocular pressure stabil
We decided to perform Yamane Scleral Fixation technique on this patient because this patient had no capsular support. On this case, Yamane scleral fixation IOL secondary implantation went second after iris claw
secondary IOL. Since the iris on this patient also damaged, we went with the second option. Previous study showed that the indications for Yamane Scleral Fixationsecondary IOL are for aphakia follow aphakia following complicated cataract surgery in ten eyes (32%), along with lensectomy for subluxated/dislocated cataract in six eyes (19%) and along with IOL explantation for subluxated/dislocated IOL in 15 eyes (48%). Overall, 13 eyes (42%) underwent anterior vitrectomy at the time of SFIOL placement and the remaining 18 eyes (58%) underwent pars plana vitrectomy [10]. The advantage of this technique are i t s applicabillity and practicality, it is also still currently the fastest scleral fixated secondary IOL implantation method available. The disadvantage of this technique are the method still challenging even for experienced surgeon in implanting scleral fixated IOL, it requires vitrectomy pars plana, the surgeon view is obstructed during the Instrascleral passes, need an exact 2 mm posterior limbus scleral poscket in order to minimize the possibility of IOL position changes, and limited International experience [11]. Previous studies had reported various complications such as IOL elevation, h y p h e m a , vitreoushemorrage , I O L decentration, and Cystoid macular edema [12].Such complications were not found on our patient.
Indications for single pass four throw technique varied widely including congenital iris abnormalities, traumatic iris tear or dialysis, and pupil abnormalities due to surgical procedure. Othe rindication had been added curreently for example: urrets Zavalia syndrome and angle closure glaucoma [9,13]. We consider the damagediris on this patient so that we decide to repair the pupil using single pass four throw technique. In order to make the procedure easier, we perform the single pass four throw technique right after we implant IOL.
There are no consensus whether beginner surgeon should try both of this techniques, but it is known that both technique had a relatively long learning curve. Yamane said that the most difficult step of the technique was Shen making sure that the scleral pocket was made exact 2 mm examinedusing OCT [14]. Too short of scleral tunnel will lead to IOL dislocation and too long scleral tunnel will lead to intraoperative distortion of the corneaduring the procedure. This difficulty also can be cause by too small angle of 30 G needle.
Combination technique of Yamane scleral fixated secondary IOL secondary implantation and single pass four throw technique can be considered as treatment choice on patient without adequate capsular support and irregular pupil in order to achieve better visual acuity post operative
Authors have no financial interest
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
