
Case Report | DOI: https://doi.org/10.31579/2690-8808/207
1 Department of Radiotherapy, Leuven University Hospital, Leuven, Belgium.
2Department of General Internal Medicine, Leuven University Hospital, Leuven, Belgium.
3Department of Clinical Pathology, Leuven University Hospital, Leuven, Belgium.
*Corresponding Author: Van Thielen Ine, Department of Radiotherapy, Leuven University Hospital. Herestraat 49, 3000 Leuven, Belgium.
Citation: Van Thielen Ine, Vanderschueren Steven, Piot Wout, Sciot Raf, De Meerleer Gert (2024), Whole Abdominopelvic Radiotherapy (WAPRT) for a Patient with Refractory Peritoneal Angiomatosis: A Case Report, J, Clinical Case Reports and Studies, 5(6); DOI:10.31579/2690-8808/207
Copyright: ©, 2024, Van Thielen Ine. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 July 2024 | Accepted: 09 August 2024 | Published: 22 August 2024
Keywords: angiomatosis; WAPRT; whole abdominopelvic radiotherapy; hemoperitoneum
Angiomatosis is a rare, benign condition characterized by the widespread proliferation of blood vessels with accompanying mature adipose tissue, affecting multiple tissue types or compartments. Although it is a histologically benign disease, it can cause significant morbidity due to its extensive lesions and the high recurrence rate associated with surgical removal. Given the limited clinical experience, no established consensus for the optimal treatment approach exists.
We report a case of a 60-year-old patient who was diagnosed with diffuse peritoneal angiomatosis following recurrent symptoms of abdominal pain. Despite receiving various pharmacological treatments including methylprednisolone, propranolol, thalidomide and sirolimus, the patient repeatedly developed a hemoperitoneum and infectious complications. The patient’s persistent symptoms and frequent hospitalizations prompted the use of whole abdominopelvic radiotherapy (WAPRT). This treatment resulted in significant symptomatic relief and reduction in angiomatosis. This case suggests that radiotherapy may be a viable palliative treatment for severe angiomatosis when other treatments fail.
Angiomatosis is a rare condition characterized by diffuse proliferation of blood vessels accompanied by mature adipose tissue [1]. It affects a large segment of the body in a contiguous manner either by involving multiple tissue types (e.g., skin, subcutis, muscle, bone) or by involving similar tissue types in multiple compartments (e.g., multiple muscles) [2, 3]. It primarily occurs in the lower extremities [2] but can also be localized in the abdomen, chest wall, head and neck region, back, and retroperitoneum [4]. It occurs primarily in the first two decades of life with a slight female predilection [1, 4]. Histologically, angiomatosis is defined by an irregular proliferation of vessels of varying sizes, typically accompanied by large amounts of mature fat [2, 3]. This suggests that the lesions may possibly be more generalized mesenchymal proliferations rather than exclusive vascular lesions [2]. Although it is a histologically benign disease, the lesions can be very extensive and cause substantial morbidity [5, 6]. Surgical removal of angiomatosis is difficult because of its infiltrative nature and is associated with a high recurrence rate [1]. Treatment options for managing angiomatosis include interferon alpha [6-8], thalidomide [6-8], lenalidomide [6, 7], propranolol [6, 9, 10], bevacizumab [6], aflibercept [6], cyclophosphamide [6] and octreotide [6]. We report a case of medical treatment-refractory peritoneal angiomatosis which was successfully treated with intensity-modulated whole abdominopelvic radiotherapy.
2.1 Initial presentation
A 60-year-old patient presented at the emergency department with progressive symptoms of abdominal cramp-like pain since several weeks, which had migrated to the right fossa in the days leading up to admission. Accompanying symptoms included nausea and anorexia. A CT (computed tomography) scan of the abdomen was suggestive of a appendiceal plastron but also depicted multiple small splenic noduli. The appendiceal plastron was treated with antibiotics (amoxicillin clavulanic acid 875mg/125 mg 3 times a day for 10 days) followed by an elective laparoscopic appendectomy which revealed a hemoperitoneum, as well as a splenomegaly and inflammatory adhesions in the right fossa. Additionally, small cystic lesions filled with blood were discovered. At that time, the etiology was unclear. Postoperatively, the patient developed pulmonary embolisms (PE) for which he was treated with an oral anticoagulant (rivaroxaban) [11].
One month after the surgery, the patient returned to the hospital with recurring symptoms of abdominal discomfort, prompting further investigations. A CT scan revealed the presence of a hemoperitoneum, along with diffuse omental infiltration and the previously observed splenic nodules (Figure 1). A laparoscopic exploration was carried out and evacuated 500 mL of blood. Multiple small hemorrhagic cysts were noted on the omentum. Biopsies of the spleen, omentum, and peritoneum were performed, but did not detect a malignancy. Additionally, further investigations, including bone marrow aspiration and biopsy, FDG-PET/CT scan, and screening for autoimmune (antinuclear factor, anti-cyclic citrullinated peptide antibodies, rheumatoid factor) and infectious diseases (toxoplasmosis, hepatitis, human immunodeficiency virus, cytomegalovirus, Epstein-Barr virus, and tuberculosis) all yielded negative results. Furthermore, the possibility of a clotting disorder was eliminated as well. Top of FormThe etiology of the hemoperitoneum remained unclear at this timepoint.

Figure 1: CT scan one month after the appendectomy: contrast-enhanced CT scan reveals a hemoperitoneum, along with diffuse omental infiltration (blue arrows panel B) and the spleen nodules observed previously (blue arrows panel A).
The patient developed a second hemoperitoneum, resulting in progressive abdominal pain and anemia (hemoglobin 8,1 g/dL) and requiring multiple
blood transfusions. He was referred to a tertiary center (Leuven University Hospitals, Belgium) for further investigations. A CT scan indicated a progressive hemoperitoneum and omental infiltration (Figure 2).
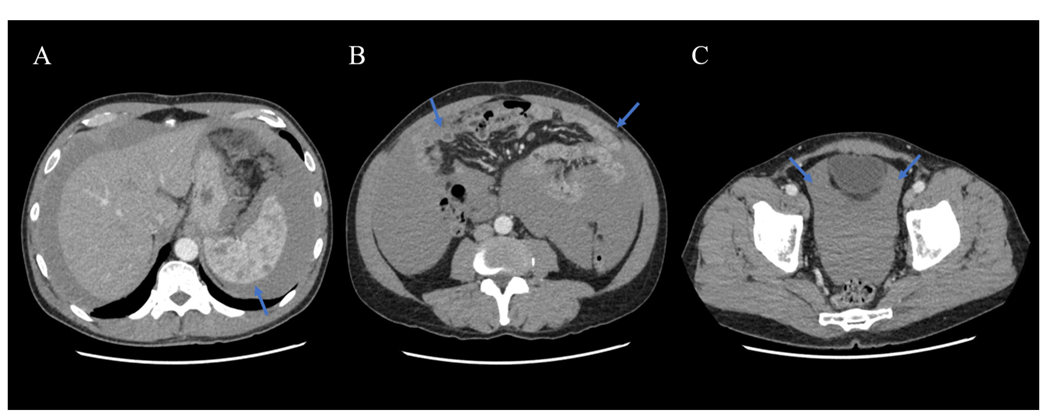
Figure 2: In January 2018, the patient developed a recurrent hemoperitoneum. A CT scan indicated a progressive hemoperitoneum (blue arrows panel A and C) and omental infiltration (blue arrows panel B).
After ruling out other conditions such as bacillary peliosis, and because of recurrent abdominal bleedings and progressive anemia, a semi-urgent splenectomy together with the removal of several omental and peritoneal hemorrhagic cysts was performed. Histological examination of the omental and peritoneal hemorrhagic cystic lesions revealed a proliferation of vessels of varying sizes. Accompanying findings included irritated mesothelium, focal foreign-body type giant cell reactions, foamy macrophages and numerous siderophages indicating hemorrhage. Microscopic examination of spleen tissue demonstrated numerous nodular vascular proliferations with vessels of varying sizes (Figure 3).
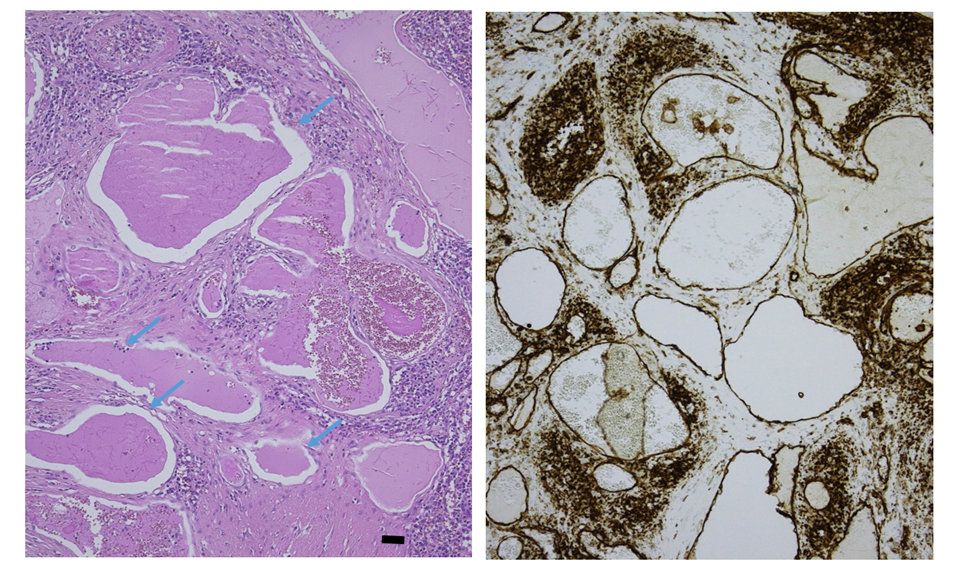
Figure 3. The splenic lesion consisted of thin-walled dilated vascular channels (blue arrows, hematoxylin & eosin stain x150, Bar=100μ). CD31 decorates the endothelium and the macrophages in between.
It was concluded that the findings were consistent with benign vascular lesions, suggestive of diffuse angiomatosis. It is possible that the lesions arose as a consequence of intraperitoneal inflammation due to appendicitis. Alternatively, the lesions may have been present long before the initial presentation but only manifested symptoms after initiation of anticoagulant therapy.
A genetic syndrome was considered less probable considering the late onset.
2.2 Treatment
Treatment of propranolol 40 mg twice daily [6, 9, 10] and tranexamic acid 1g twice daily [12] was initiated and was increased to 160 mg slow-release propranolol and methylprednisolone 32 daily due to insufficient improvement of symptoms [13]. Acetylsalicylic acid 80 mg was added to treat thrombocytosis post-splenectomy [14]. Over the following months, there was a favorable evolution with CT-graphic reduction of the hemoperitoneum and a gradual increase in hemoglobin. The dose of methylprednisolone and propranolol was gradually reduced to 4 mg and 40 mg twice daily respectively. Treatment with tranexamic acid and acetylsalicylic acid was discontinued.
Unfortunately, symptoms recurred rapidly, requiring hospital readmission due to symptomatic hemoperitoneum 9 months after start of therapy. Treatment included high doses of corticosteroids and an escalation of propranolol to 40 mg three times daily (later replaced by bisoprolol because of atrial fibrillation). Because of repeated embolic episodes such as a TIA (transient ischemic attack) caused by atrial fibrillation, anticoagulation with edoxaban was necessary [15], complicating the treatment of the angiomatosis.
Over a period of roughly 3 years after the initial diagnosis and start of treatment, the patient was hospitalized four times due to complications of peritoneal angiomatosis, being recurrent hemoperitoneum or peritonitis. During a hospitalization, the patient required admission to the intensive care unit due to E. coli bacterial peritonitis with impending sepsis, leading to two laparotomies being performed for hemoperitoneum drainage. Due to the frequent and severe complications, a treatment with thalidomide was initiated approximately 3 years after diagnosis, on top of the maintenance treatment with methylprednisolone 8 mg [6–8]. However, thalidomide proved ineffective as well, leading to initiation of sirolimus, a mTOR inhibitor [16–19].
In order to manage the side effects of chronic corticosteroid use, the patient received a proton pump inhibitor for gastric protection, calcium and vitamin D for osteoporosis prevention, and trimethoprim/sulfamethoxazole for Pneumocystis Jiroveci Pneumonia (PJP) prophylaxis during periods wherein a high dose of methylprednisolone was needed [20, 21]. Ophthalmological screening and monitoring of the HbA1c level were conducted regularly [20]. Nevertheless, over the years the patient developed cushingoid features, corticosteroid induced cataract, adrenal insufficiency and multiple compression fractures of the vertebrae necessitating treatment with alendronate [22].
When a new magnetic resonance imaging (MRI) again indicated a significant increase of the peritoneal angiomatosis (Figure 4) while under treatment with sirolimus for 3 months, it became obvious that pharmacological treatment reached its limits. Interferon was considered but, because of the limited experience and uncertain availability, it was decided not to start it. The radiation-oncology team was asked for a consult and treatment with whole abdominopelvic radiotherapy (WAPRT) was proposed [23]. After multidisciplinary agreement, the patient was referred to the department of radiation oncology.
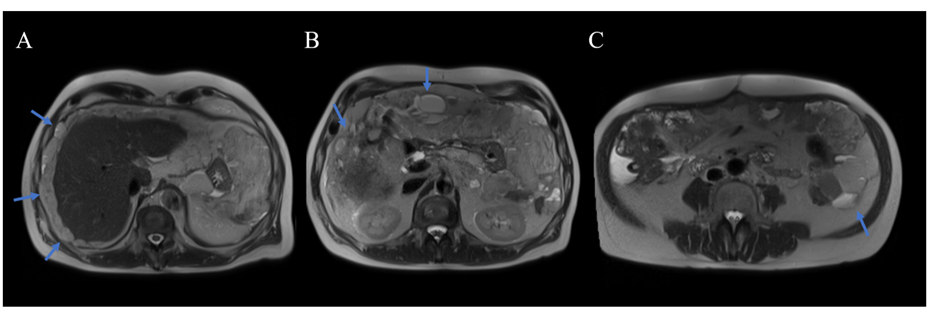
Figure 4: When treated with sirolimus, an MRI demonstrated again a significant increase of the peritoneal angiomatosis, mainly in the upper abdomen along the liver (blue arrows panel A), mesogastric region, omental (blue arrows panel B) and left paracolic area (blue arrow panel C).
2.3 Radiotherapy
At the time of the assessment by the radiation-oncology team, the patient experienced a long-standing, fluctuating pressure sensation in the meso- and epigastric areas, without the need for pain relief. The patient accepted our treatment proposal with WAPRT. The first aim was to stop the growth of the angiomatosis. Additionally aims were to decrease the volume of the angiomatosis and reduce the risk of recurrence.
The clinical target volume (CTV) encompassed the whole peritoneal cavity (Figure 5). To generate planning target volume (PTV), the CTV was expanded with an isotropic margin of 5 mm. Organs at risk (OAR) included the liver, kidneys, spinal cord, bladder, heart, lungs, stomach, small and large intestine. We prescribed a dose of 33 Gy in 22 daily fractions of 1,5 Gy to the PTV [23]. WAPRT was delivered via VMAT (Volumetric Arc Therapy) technology using 10 MV photons, incorporating 4 arcs with specifically chosen collimator rotations to optimally spare the organs at risk (Figure 6) [24]. At each fraction, a cone beam CT was performed to optimize patient setup and consequently reduce geographical misses.
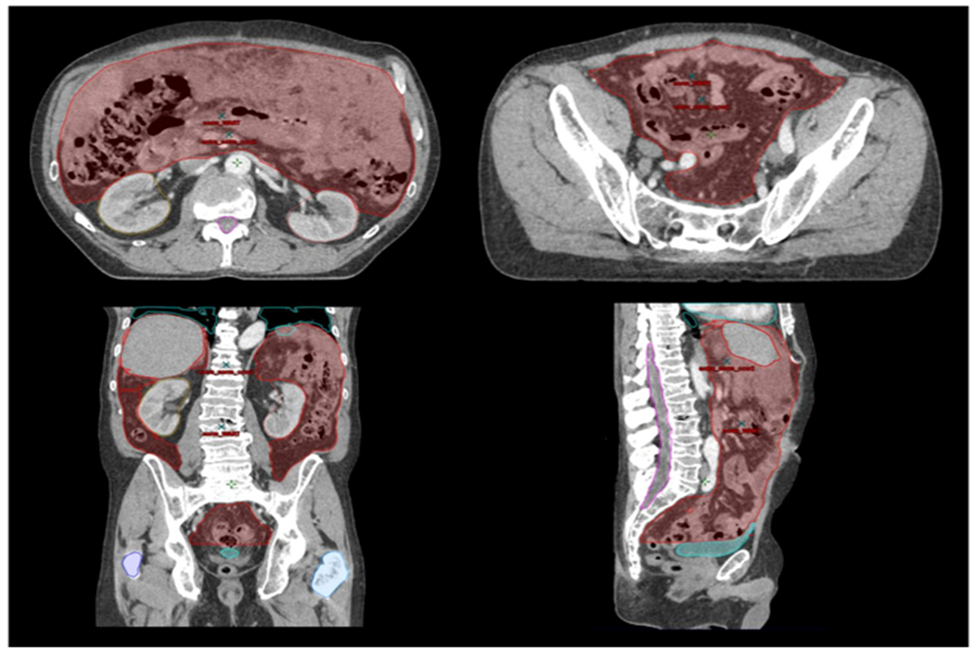
Figure 5: The clinical target volume (CTV) encompassed the whole peritoneal cavity (red). To generate planning target volume (PTV), the CTV was expanded with an isotropic margin of 5 mm. Organs at risk (OAR) included the liver, kidneys, spinal cord, bladder, heart, lungs, stomach, small and large intestine.
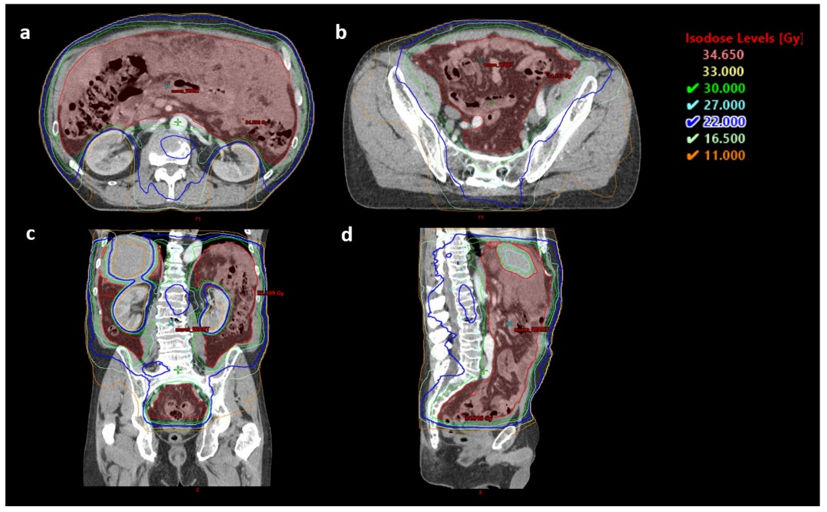
Figure 6: Axial (a,b), coronal (c) and sagittal (d) dose distributions of the patient treated with 10 MV photons using VMAT covering the whole abdominopelvic cavity (red = CTV). A dose of 33 Gy was prescribed and delivered in 22 daily fractions of 1,5 Gy.
To prevent radiation-induced nausea and vomiting, the patient took ondansetron one hour before each radiation session and received treatment on an empty stomach. Methylprednisolone was temporarily increased to 16 mg per day during treatment [25]. To prevent cumulative toxicity, sirolimus was temporarily paused, from one week before to one week after radiotherapy [26]. At that moment, it was decided to cease treatment with sirolimus definitively.
Treatment was tolerated well. The patient experienced fluctuating bowel habits (alternating between diarrhea and constipation), requiring alternating use of laxatives and loperamide [27]. Nausea remained relatively well controlled with methylprednisolone and ondansetron [25]. The abdominal pressure sensation was still present, but rather intermittently. Considering the prolonged treatment with methylprednisolone 16 mg and the development of radiotherapy-induced lymphopenia (lymphocytes <1>
After treatment, the patient described significant improvement of his abdominal complaints. Medrol was once again tapered. An MRI 11 weeks post-radiotherapy demonstrated a significant decrease of angiomatosis (Figure 7), and hemoglobin levels improved. Four months after treatment, the patient presented at the emergency department after an episode of abdominal pain in the left abdomen. Further investigations were reassuring. Eight months post-radiotherapy, a new MRI was performed. This time, there was a mixed response with mainly a reduction of the angiomas, yet also an increase of the angiomatosis in the left fossa and the pelvic mesentery. Since the patient experienced some pain in the left fossa since a few weeks, a more focal reirradiation was proposed.
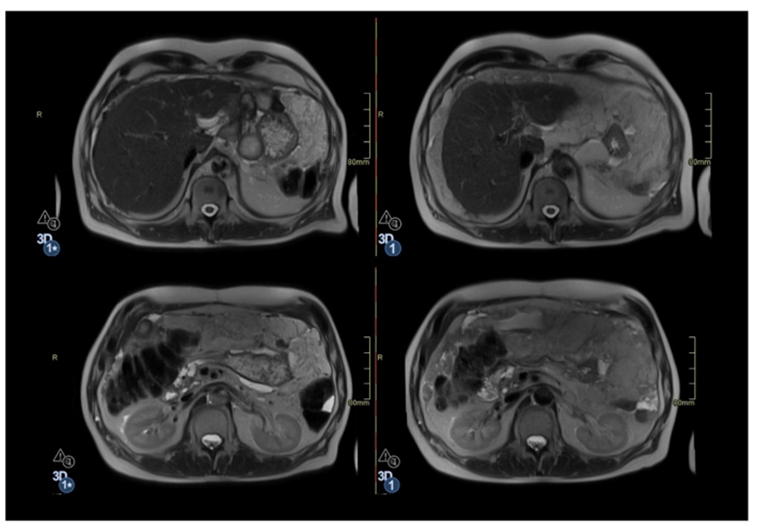
Figure 7: An MRI 11 weeks after the whole abdominopelvic radiotherapy (left) demonstrated a significant decrease of the angiomatosis, in comparison with the MRI before the start of the treatment (right), mainly in the upper abdomen along the liver, the mesogastric region, omental region and left paracolic region, as well as in both flanks and the pelvis.
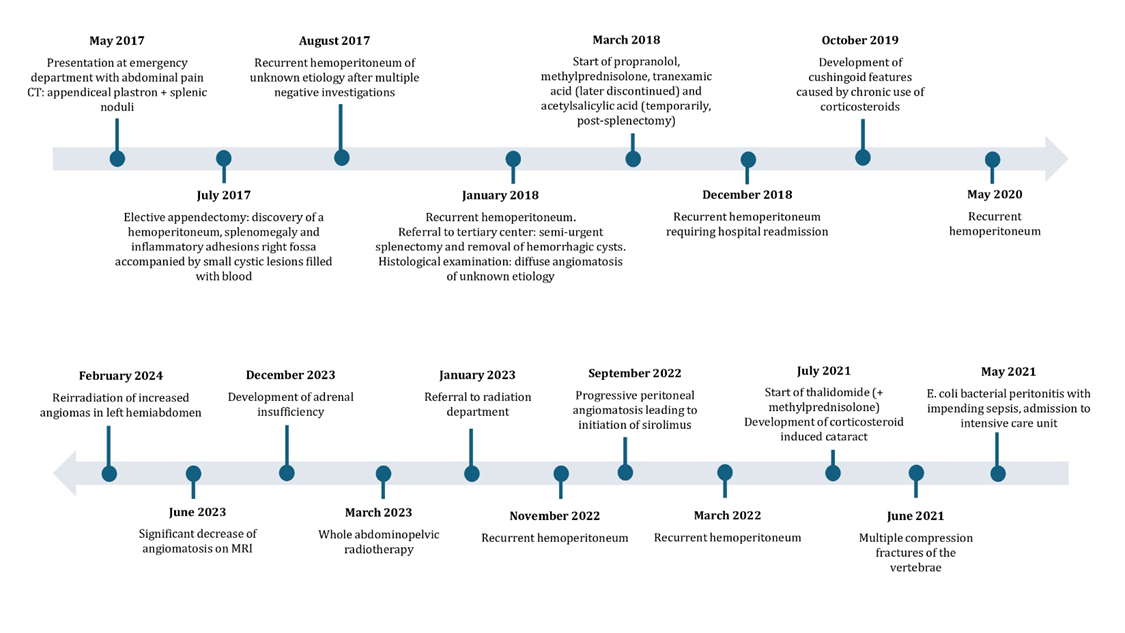
Figure 8: Timeline illustrating the keypoints in the patient’s case.
Between this follow-up appointment and the initiation of the second course of radiotherapy, the patient was admitted for a few days due to severe pain in the left lower abdomen. Investigations revealed sub-obstruction, likely caused by abdominal adhesions following multiple surgeries.
A reirradiation of the increased angiomas in the left hemiabdomen was performed, up to 33 Gy in 22 fractions of 1,5 Gy [28]. The angiomas were delineated as gross tumour volume (GTV). Around the GTV, a margin of 1 cm was used to create the PTV. Methylprednisolone was temporarily increased again from 4 mg to 8 mg twice daily. Besides a slight increase in fatigue, no acute side effects were reported. Methylprednisolone could be smoothly tapered off again after the completion of radiation treatment. Three weeks post-radiotherapy, the patient reported being completely symptom-free. One year after the WAPRT, the patient was free of symptoms.
Angiomatosis is a rare, benign disease that can manifest in multiple locations. Although benign, it can be very extensive and lead to serious complications [5, 29]. Due to limited clinical experience, there is no established consensus of the optimal treatment approach. This case of a 60-year-old male with pharmacologically refractory peritoneal angiomatosis highlights the complexities involved in diagnosing and managing angiomatosis. Despite the use of multiple pharmacological treatments, including methylprednisolone, propranolol, thalidomide, and sirolimus, the patient experienced recurrent hemoperitoneum and infectious complications. Moreover, the patient suffered from side effects due to chronic use of glucocorticoids. The persistence of symptoms and frequent hospitalizations despite multiple pharmacological treatments prompted the exploration of other options. Based on the favorable outcomes of whole abdominopelvic radiotherapy (WAPRT) in managing pseudomyxoma peritonei and ovarian cancer [23, 30], we hypothesized that WAPRT could be an effective intervention for peritoneal angiomatosis. By using VMAT, a homogenous dose distribution could be obtained, while minimizing the radiation dose to the surrounding organs at risk. This resulted in a low toxicity profile, with the patient experiencing only mild side effects. Our case demonstrated a positive clinical outcome with significant improvement in the patient's symptoms, hemoglobin levels, and angiomatosis on MRI.
In the context of other syndromes characterized by vascular proliferations, such as Sturge-Weber syndrome and Von-Hippel Lindau disease, treatment with radiotherapy has been described. Choroidal hemangiomas in Sturge-Weber syndrome are frequently treated with brachytherapy, proton therapy or radiosurgery [31–36]. Promising results have also been reported for the treatment of hemangioblastomas in Von Hippel-Lindau disease with radiotherapy [37–39]. There is limited literature available on radiotherapy as a potential treatment for angiomatosis. Adam Z. et al described a case of a patient with angiomatosis in the supraclavicular region, where radiotherapy up to 54 Gy (fractionation unknown) resulted in at least a 50% reduction in the malformation [40]. We found one other case of a patient with diffuse angiomatosis affecting the face, neck, thorax, and mediastinum, which reportedly was cured by radiotherapy (article/abstract not available) [41].
Given the limited available literature, this case report adds to the treatment armamentarium of peritoneal angiomatosis. It demonstrates that WAPRT is an effective treatment of this disease. Therefore, we suggest that WAPRT should be considered in patients with symptomatic peritoneal angiomatosis refractory to pharmacological treatment. The advantages of radiotherapy in this context include reducing the size of the lesions, reducing internal hemorrhage, alleviating symptoms, and improving quality of life. However, it is important to acknowledge that a limitation of this report is that it is based on a single patient case. Therefore, the use and interpretation of these results should be approached with caution. Continued research and clinical reporting will be essential to further establish the role of radiotherapy in managing angiomatosis and similar vascular proliferative disorders.
We present a case of diffuse peritoneal angiomatosis with recurrent complications despite surgical and pharmacological treatment. We performed a whole abdominopelvic radiotherapy using VMAT to a total dose of 33 Gy delivered in 22 daily fractions. The treatment was well tolerated and resulted in symptomatic improvement and a significant decrease of the angiomatosis. We therefore believe that WAPRT could be considered as a palliative treatment option in managing patients with recurrent angiomatosis.
CT: computed tomography
FDG-PET/CT: fluorodeoxyglucose-positron emission tomography/computed tomography
ANF: antinuclear factor
anti-CCP: anti-cyclic citrullinated peptide
RF: rheumatoid factor
HIV: human immunodeficiency virus
TIA: transient ischemic attack
E. coli: Escherichia coli
mTOR inhibitor: mammalian target of rapamycin inhibitor
PJP: Pneumocystis Jiroveci Pneumonia
HbA1c: Hemoglobin A1c
MRI: magnetic resonance imaging
WAPRT: whole abdominopelvic radiotherapy
CTV: clinical target volume
PTV: planning target volume
OAR: organs at risk
VMAT: volumetric arc therapy
The authors have no conflict of interest to report.
This case report was approved by the ethical commission of UZ Leuven (approval number: S68781). A written informed consent was obtained from the patient for publication of this case report.
Concept and initial idea: Van Thielen Ine, De Meerleer Gert
Writing and review of the article: Van Thielen Ine, De Meerleer Gert, Vanderschueren Steven, Piot Wout, Sciot Raf
Revisions and final edits: Van Thielen Ine, De Meerleer Gert, Sciot Raf
Clinical supervision of the patient and assistance with writing: Vanderschueren Steven
Radiation treatment planning: Piot Wout
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
